
Abstract
Introduction
Behçet disease is a chronic vasculitis that generally affects young adults in the most productive period of their life. The purpose of this study is to evaluate patients’ work productivity and daily activity impairment, and their relationship with disease activity and quality of life.
Method
In this study, 55 patients with Behçet disease who are currently working and 50 healthy controls were included. To evaluate quality of life, a 36-item short form health survey was used. For the evaluation of Behçet disease activity and work productivity, the Behçet Disease Current Activity Form and Work Productivity and Activity Impairment questionnaire were used, respectively. Quality of life and work productivity between patients and healthy controls were compared.
Results
Scores of all domains of the health survey were significantly worse in patients with Behçet disease (range, p = 0.006 to p < 0.001). The mean Work Productivity and Activity Impairment absenteeism, presenteeism and activity impairment scores were higher in patients with Behçet disease (p = 0.005, p < 0.001 and p < 0.001, respectively). There was a significant correlation between Behçet Disease Current Activity Form score and absenteeism (r = 0.32, p = 0.016). Moreover, there was significant correlation between Work Productivity and Activity Impairment and most domains of the health survey (range, r = −0.27 to –0.64, range, p = 0.047 to p < 0.001).
Conclusion
Our results showed remarkable impairment in work productivity and health-related quality of life in Behçet disease. There is a strong correlation between work productivity and quality of life. To improve work productivity, more effective therapeutic approaches and improvements in working conditions should be provided.
Introduction
Behçet disease (BD) is a chronic, multi-system, vasculitic disorder characterized by recurrent oral aphthous ulcers and numerous potential systemic manifestations, such as ocular, neurologic, gastrointestinal and vascular disease (Tursen et al., 2003). Although major organ involvements are associated with morbidity and mortality, other manifestations of the disease reduce quality of life (QoL) (Hatemi et al., 2014). Treatment of BD depends on disease severity and organ involvement. The main treatment goals are persistent disease remission, to prevent organ damage and to improve patients’ QoL and working conditions (Hatemi et al., 2014; Oliveira et al., 2011).
BD is slightly more common in men than women and males are affected more seriously. BD activity is higher in the early stages of the disease, and its onset is usually around age 30–40 years, in the most work-productive stage of life (Wang et al., 2010). Working is a significant part of life. It provides a social role and affects standards of living. So, the ability to meet job demands and sustain employment are important aspects for an individual and must be considered in treatment decisions (Gignac et al., 2004). Work impairment is also an important factor for insurers and employers to consider. In addition, BD causes considerable economic burden for the health care system (Sut et al., 2007).
There are many studies evaluating work productivity in inflammatory disorders such as rheumatoid arthritis and ankylosing spondylitis (Burton et al., 2006; Haglund et al., 2013; Tran-Duy et al., 2015; Verstappen, 2015). Although BD is also an inflammatory disorder with a lower prevalence, only a few small studies have evaluated work productivity in patients with BD and these studies had important limitations, for example lack of comparison with healthy subjects (Mehta et al., 2014; Mumcu et al., 2017). Moreover, no study investigated associations between QoL, BD activity and work productivity. The working life of patients may be affected negatively due to acute and chronic complications of BD. Identifying problems related to working life will contribute to the development of effective therapeutic interventions that may improve the work performance and health-related quality of life of patients. The aim of this study is to investigate work productivity and activity impairment (WPAI) in BD patients and possible underlying factors.
Method
Patients and study design
In this cross-sectional study, 55 currently working BD patients who attended the outpatient rheumatology clinic of Gazi University Hospitals and 50 healthy controls were included. The study was conducted between May and September 2018. The control group consisted of patient companions, who had no known systemic disease. The diagnosis of BD was made according to the International Study Group (ISG) criteria (1990). Inclusion criteria were being ≥18 years of age and currently working in a paid job. Exclusion criteria were pregnancy, psychiatric disorders, severe systemic disorders, having other inflammatory diseases and not working in a paid job. Demographic characteristics, educational status, body mass index (BMI), duration of delay in diagnosis (defined as the time between onset of symptoms and diagnosis) and duration of disease, and clinical manifestations (eye, mucocutaneous, musculoskeletal, vascular, neurologic and alimentary) were recorded. The dominant organ involvement was defined as the type of involvement that primarily led to the treatment decision. Income level was defined as low (minimum wage), moderate (one to three times the minimum wage) or high (more than three times the minimum wage). Minimum wage is considered to be at the poverty threshold in Turkey (www.resmigazete.gov.tr/eskiler/2017/12/20171230-10.pdf). The stress level of their work was also classified by patients as low, moderate or high according to the perceived emotional stress of the patients. Participants were asked if their work had changed at any time due to BD (yes or no). The study was approved by the Gazi University Research Ethics Committee in accordance with the Helsinki Declaration of 1975. Informed consent was obtained from all participants.
Evaluation of quality of life, disease activity and work productivity
We used the 36-Item Short Form Health Survey (SF-36) to evaluate the QoL in patients and healthy controls (HC) (Ware and Sherbourne, 1992). The SF-36 health survey is a subjective measure of health-related quality of life and consists of 36 questions relating to eight domains: physical functioning, social functioning, physical role functioning, emotional role functioning, vitality, mental health, pain and general health. Each domain scores from 0 to 100 points. A higher score shows a better quality of life. A Turkish version of the SF-36 has been validated (Kocyigit et al., 1999)
For the assessment of disease activity, the Behçet Disease Current Activity Form (BDCAF) (Bhakta et al., 1999), which scores clinical features of patients in the last four weeks, was used. The BDCAF has 12 components: headache, oral ulcer, genital ulcer, erythema, skin pustule, arthritis, arthralgia, nausea/vomiting/abdominal pain, diarrhea or frank blood in the stool, or new symptoms in the eye, nervous or vascular systems. Each component is scored as absent (0) or present (1) and the final BDCAF score is the sum of all components. Patient and physician perception of disease activity is based on a seven-point Likert scale (1=feel very good, 7=feel very bad) and is also evaluated with this form. A Turkish version of the BDCAF has been validated (Hamuryudan et al., 1999).
We used the Work Productivity and Activity Impairment Specific Health Problem v2.0 (WPAI:SHP) questionnaire to evaluate work productivity. The WPAI can be adapted to a specific disease/condition (Reilly et al., 1993). There are six questions, which evaluate the last seven days: current employment status (Q1); number of hours missed from work due to disease/health condition (Q2); number of hours missed from work due to other reasons, such as vacation, holiday (Q3); the number of actual working hours (Q4); the impact of the disease/health condition on the patient’s productivity at work (Q5) and the impact of the disease/health condition on daily activities other than work (Q6). For Q5 and Q6, a 10-mm visual analog scale (VAS) (0: no interference, 10: complete interference) was used. We calculated absenteeism, defined as missed work hours due to health problems, as [Q2/(Q2 + Q4)]×100, presenteeism, defined as reduction of productivity while at work (Q5/10) and daily activity impairment (DAI) other than work (Q6/10). We multiplied presenteeism and daily activity impairment by 10.
Statistical analysis
All statistical analyses were performed using SPSS (Statistical Package for Social Sciences) Version 15.0 (SPSS, Inc, Chicago, IL, USA). Continuous variables were presented as mean and standard deviation (SD), and categorical variables as frequencies and percentages. Differences between categorical variables were evaluated with a chi-square test. Normality distribution of continuous variables was determined by using the Kolmogorov–Smirnov test. The differences between two independent groups were compared by using an independent sample t-test for normal distributions or the Mann–Whitney U test for non-normal distributions. The differences between three or more independent groups were compared by using the Kruskal–Wallis H test with a Bonferroni adjusted Mann–Whitney U test. Correlation coefficients were calculated using the Spearman’s rank test. A two-sided p-value of <0.05 was considered statistically significant for all analyses.
Results
In this study, 55 patients with BD (12 females and 43 males, mean age: 36.76 ± 10.06 years) and 50 healthy controls (13 females and 37 males, mean age: 35.82 ± 6.79) were included. The mean BMIs for BD patients and HC were 26.2 ± 4.16 and 25.1 ± 3.47 kg/m2, respectively. There was no significant statistical difference between the two groups in terms of age, sex and BMI (p>0.05, see Table 1). The median duration of BD and delay in diagnosis was 7 (range 0–36) and 4 (range 0–25) years, respectively.
Demographic variables of patients and control group (healthy individuals).

Data were presented frequency (percentage) for categorical variables or mean ± standard deviation for continuous variables.
BMI: body mass index
%: we calculated the percentage of demographic variables among themselves; for example 43/(43+37)=53.8/100. 53.8% of male subjects was in patient group.
The frequency of clinical manifestations of patients with BD were as follows: oral ulcers 100% (n=55), genital ulcers 67% (n=37), ocular involvement 64% (n=35), arthritis 27% (n=15), vascular involvement 27% (n=15), neurological involvement 18% (n=10) and no gastrointestinal involvement. The most common dominant organ involvement was eye 40% (n=22), followed by mucocutaneous–musculoskeletal 29% (n=16), neurologic 16% (n=9) and vascular disease 15% (n=8).
Scores of all domains of the SF-36 were significantly lower in patients with BD compared to healthy controls (range, p = 0.006 to p < 0.001, Table 2). The ratios of absenteeism (32.7%, n=18 vs 10%, n=5, p = 0.005), presenteeism (87.3%, n=48 vs 38%, n=19, p < 0.001) and DAI (80%, n=44 vs 38%, n=19, p < 0.001) were strikingly worse in patients with BD compared to the control group. There was no difference in mean total working hours and lost working hours due to non-disease causes (Q3) between the two groups (Table 2). There was a low negative correlation between absenteeism and vitality (r = –0.28, p = 0.042) and a moderate negative correlation with social function (r = –0.32, p = 0.016), physical role function (r = –0.46, p < 0.001), emotional role function (r = –0.33, p = 0.015) and pain (r = –0.32, p = 0.019). Presenteeism was negatively moderately correlated with social function (r = –0.31, p = 0.016), physical role function (r = –0.46, p < 0.001), mental health (r = –0.32, p = 0.018), pain (r = –0.31, p = 0.020) and general health (r = –0.46, p < 0.001). Lastly, there was a moderate to strong negative correlation between DAI and all domains of SF-36, except pain domain (range, r = –0.27 to –0.64, range, p = 0.047 to p < 0.001) (Table 3).
Comparison of SF-36 and WPAI between Behçet disease patients and control group (healthy individuals).
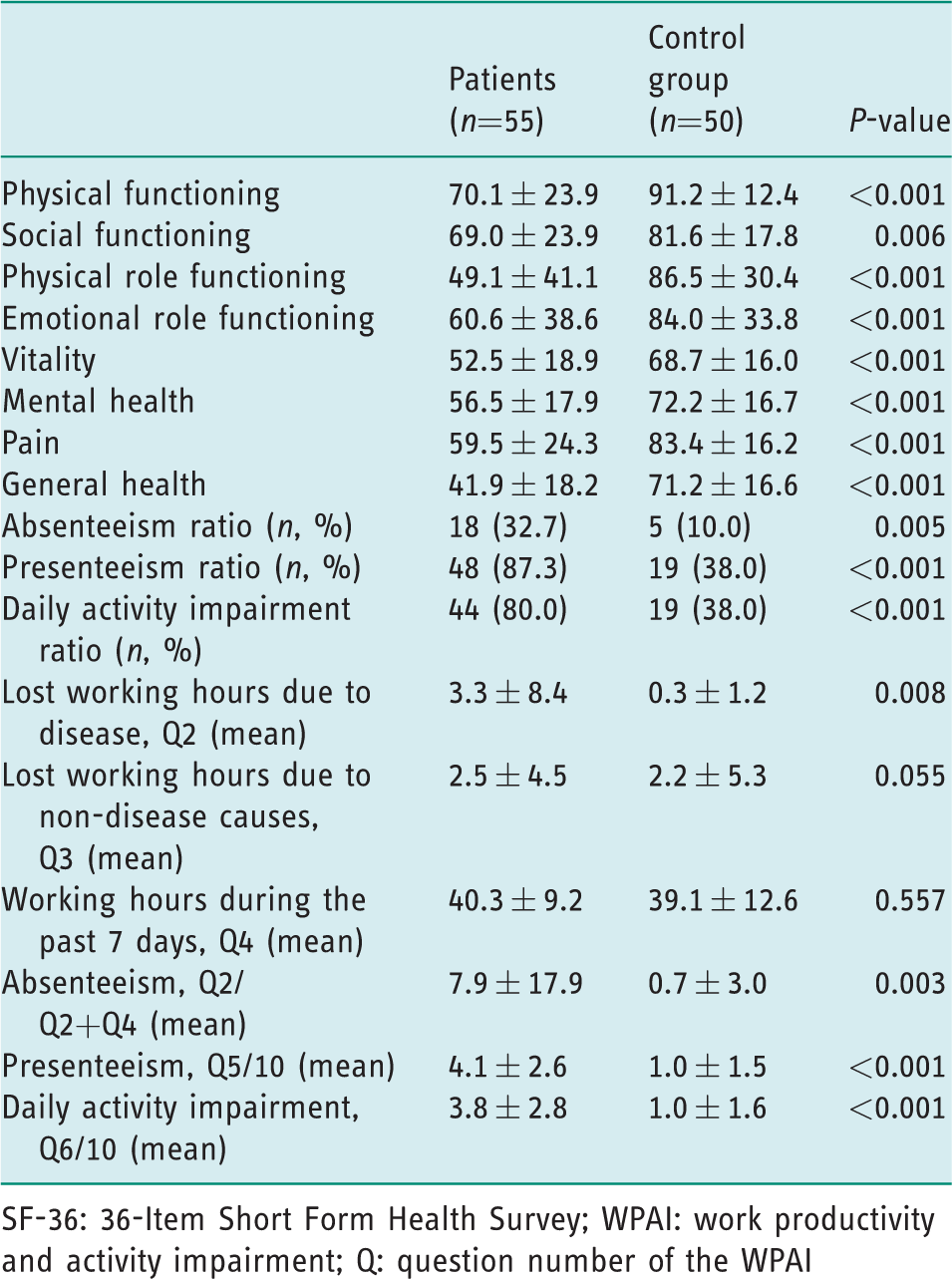
SF-36: 36-Item Short Form Health Survey; WPAI: work productivity and activity impairment; Q: question number of the WPAI
Correlation of SF-36 domains and BDCAF score with mean WPAI absenteeism, presenteeism and daily activity impairment.
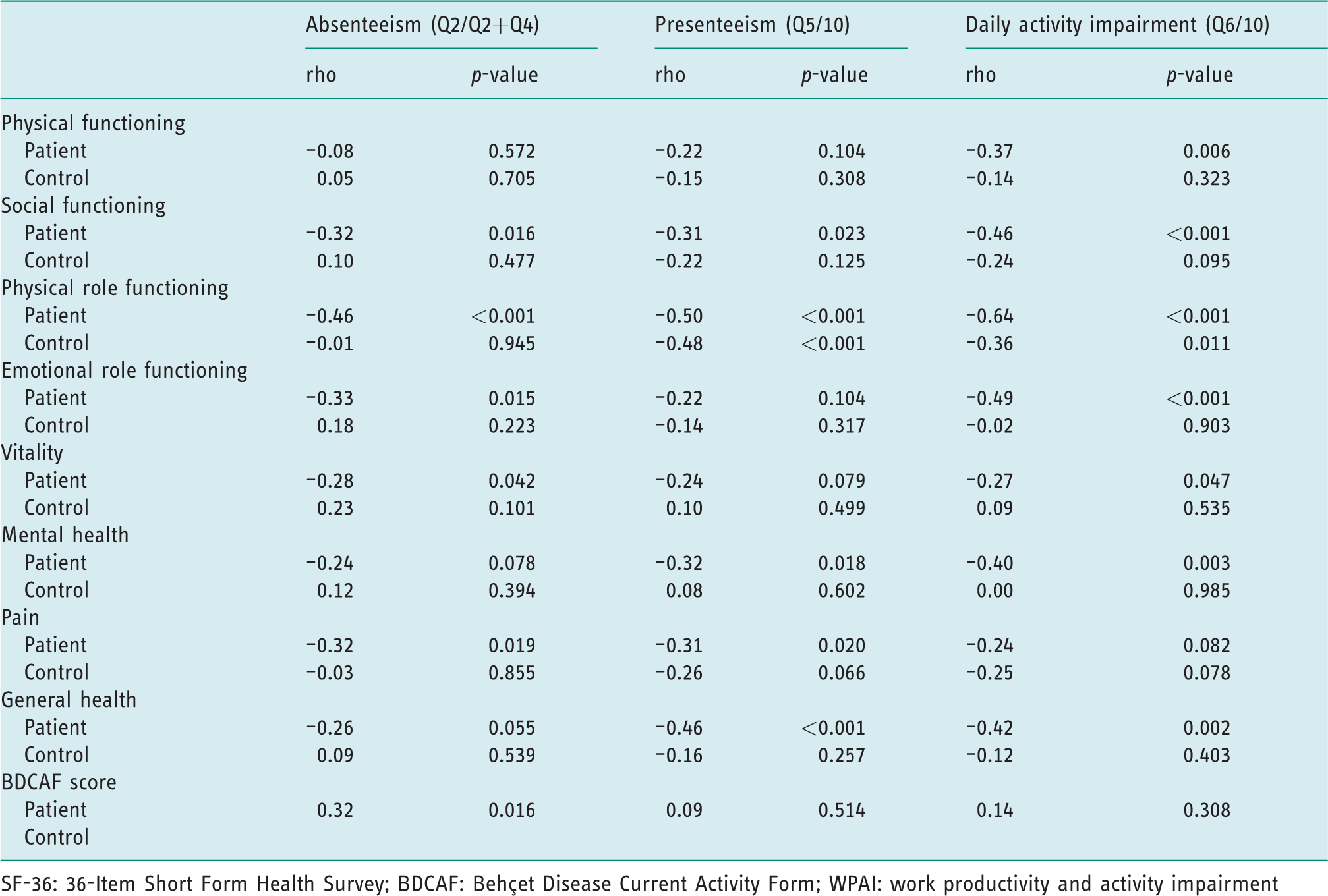
SF-36: 36-Item Short Form Health Survey; BDCAF: Behçet Disease Current Activity Form; WPAI: work productivity and activity impairment
The mean BDCAF score was 2.4 ± 1.4. The mean patient and physician perceptions of disease activity based on a seven-point Likert scale were 3.2 ± 1.2 and 3.0 ± 1.1, respectively. The most scored components of BDCAF were: arthralgia 67% (n=37), oral ulcer 55% (n=30) and headache 51% (n=28). There was a moderate correlation between BDCAF score and mean absenteeism (r = 0.32, p = 0.016) and no correlation with mean presenteeism (r = 0.09, p = 0.514) and DAI (r = 0.14, p = 0.301). The patient Likert scale was moderately correlated with mean presenteeism (r = 0.446, p = 0.001) and DAI (r = 0.447, p = 001), while the physician Likert scale was moderately correlated with mean absenteeism (r = 0.301, p = 0.025) and presenteeism (r = 0.305, p = 023).
The work change due to BD was evident in 18 (33%) of patients. The highest absenteeism was observed in dominant vascular involvement (37.5%, n=3) and the highest presenteeism was in those with mucocutaneous–musculoskeletal symptoms (94%, n=15). DAI was highest in BD patients with dominant eye involvement (86.4%, n=19). There was no effect of sex, BMI, duration of disease and delay in diagnosis, history of work change or educational status on mean absenteeism, presenteeism and DAI. No association was observed between WPAI and stress level at work (Table 4).
Relation of patient characteristics with WPAI absenteeism, presenteeism and daily activity impairment.

WPAI: work productivity and activity impairment; SD: standard deviation, BD: Behçet disease
Discussion
BD is generally observed in young males in their most productive ages and both treatment expenditure and loss of work labor causes considerable economic burden for the health care system (Sut et al., 2007). In this study we evaluated the presence of absenteeism, work productivity and daily activity impairment and their relations with QoL and disease activity in patients with BD.
In our study, presenteeism, absenteeism and DAI were significantly higher in patients with BD than in the healthy control group. These results were comparable with recent studies (Mehta et al., 2014; Mumcu et al., 2017). Mehta et al. (2014) reported that 54% of patients changed their jobs due to BD. The mean VAS assessment (a 0–10 scale) for the effect of BD on work productivity was 7/10, the effect on daily activity impairment was 4/10. Work hour loss was higher in mucocutaneous disease. Mumcu et al. (2017) reported that 30.41% had missed work during the last week and the decrease in working hours was higher in patients with eye involvement. The DAI was higher in patients with musculoskeletal involvement. In our study, 33% of patients changed their job due to BD. The ratio of absenteeism was also 33% in BD patients. By using the mean VAS assessment, the effect of BD on work productivity was (4.1 ± 2.6)/10 and the effect on daily activity impairment was (3.8 ± 2.8)/10. Absenteeism, presenteeism and DAI were higher in the disease group. The highest ratio of work change due to BD was in neurologic involvement. Interestingly, the highest presenteeism ratio was in the mucocutaneous–musculoskeletal group, a less severe presentation of BD. This may be due to the effect of oral ulcers on speech and the effect of musculoskeletal pain on moving.
The duration of disease had no impact on WPAI. Therefore, it is necessary to make working conditions better for BD patients regardless of disease duration. Although BMI was not related to mean absenteeism, presenteeism or DAI, because of the high risk of metabolic syndrome in BD, lifestyle changes like exercise and diet should be suggested to patients with a high BMI (Yalcin et al., 2013).
There was a moderate correlation between BDCAF score and absenteeism, but no relation between presenteeism and DAI. Interestingly, this was in contrast to ankylosing spondylitis and rheumatoid arthritis patients, in whom an important association was shown between disease activity and work productivity and daily activity (Boonen et al., 2010; Salazar-Mejia et al., 2018). There was a meaningful association of mean presenteeism and DAI with the patient Likert scale. In addition, significant relations between physician Likert scale and mean absenteeism and presenteeism were observed. Because of this, on each visit patients should be asked how they feel. If a poor feeling of disease perception is defined, in addition to medication, psychological support should also be provided to increase work productivity and decrease DAI.
In our study, all subscales of SF-36 were significantly impaired in BD patients when compared with healthy controls because, like other chronic diseases, BD also has negative impacts on the patient’s health. There are many studies showing impairment of QoL in BD (Bernabe et al., 2010; Bodur et al., 2006; Melikoglu and Melikoglu, 2014). In this study, there was a negative correlation between the subscales of the SF-36 and WPAI. Interestingly, the association between WPAI and QoL was more potent than the association with disease activity. This shows us that even if the disease is clinically silent, there are problems caused by the chronic nature of the disease that have negative impacts on working conditions and physical, social and mental health. So, irrespective of whether the patient is in remission, all patients with BD should be supported with extra care, both mentally and physically.
There were some limitations to our study. First, our cohort is lacking certain involvement types, such as alimentary involvement. Second, patients answered questions at a single time, so temporal changes were not evaluated. Prospective, longitudinal studies should be performed to evaluate changes with treatment.
Conclusion
BD affects actively working young adults. Our study revealed high work- and health-related quality of life impairment in BD patients. This results in a high economic burden for society. In addition, this situation may have effects on the social, mental and daily life of patients. To improve work productivity and health-related quality of life, a comprehensive management of patients with BD should be done, including lifestyle changes, medical treatment, psychological and social support and the improvement of working conditions.
Key findings
Work productivity is impaired in patients with Behçet disease. Work productivity is associated with quality of life. Health-related quality of life is impaired in patients with Behçet disease.
What the study has added
This study evaluated work productivity and underlying factors in patients with Behçet disease and showed impairment in work productivity and health-related quality of life. Further studies are necessary in order to understand and effect the comprehensive management of this disease and improve the working conditions, working life and health-related quality of life for this group of patients.
Footnotes
Research ethics
Ethical approval was obtained from Gazi University Research Ethics Committee (2018, reference number 318).
Consent
All participants provided written informed consent.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Contributorship
Nuh Atas designed the study, researched literature, applied for ethical approval and wrote the initial draft of the manuscript. All authors contributed to the methodology of the project, the collection and interpretation of data and the statistical analysis plan. Bulent Celik carried out the statistical analysis, and all authors interpreted the data. All authors reviewed and edited the manuscript and approved the final version.