
Abstract
Introduction
This study describes the self-initiated pretend play abilities of children who had sustained an acquired brain injury.
Method
A non-experimental study was conducted with 26 children with acquired brain injury (15 females, mean age 5.08 years, SD 1.58 years), who were out of post-traumatic amnesia, able to sit independently and engage in a play session. The children were assessed individually on one occasion using the Child-Initiated Pretend Play Assessment.
Findings
All children in the study presented with pretend play deficits, particularly in symbolic play. Inattention, distractibility and limited concentration were common behaviours of the children. Three quarters of the sample (76.48%) were unable to complete the time of the assessment. For many of the children the cessation of their play was sudden and abrupt, even for those who showed complex play ability.
Conclusion
Cognitive fatigue is argued to have impacted on the children’s play ability due to the considerable amount of cognitive effort required to engage in pretend play. Implications for intervention are to offer short sessions for children with acquired brain injury and pay particular attention to a child’s symbolic play within pretend play ability.
Introduction
Of all types of injury, those to the brain are among the most likely to result in death or permanent disability (Centers for Disease Control and Prevention, 2017). Within Australia, paediatric brain injury is a leading cause of acquired long-term disability, resulting in a variety of ongoing, motor and cognitive deficits (Galvin et al., 2010a). According to Brain Injury Australia, ‘Acquired brain injury (ABI) refers to the multiple disabilities arising from any damage to the brain that occurs after birth’ (Rushworth, 2008: 2) and traumatic brain injury (TBI) is ‘an ABI caused by a traumatic event, from an external force to the brain such as a motor vehicle accident, a fall or a blow to the head’ (Rushworth, 2008: 2). Globally, TBI is the leading cause of mortality in young adults (Johnson and Griswold, 2017), and is a leading cause of death and disability across the lifespan (Maas et al., 2017). It is estimated that approximately half the world’s population will have one or more TBIs over their lifetime (Johnson and Griswold, 2017). The Australian government Bureau of Statistics’ 2003 Survey of Disability, Ageing and Carers reported that 1 in 12 Australian children had a disability, of whom 22,800 were diagnosed with an ABI (Rushworth, 2008). Of the children identified as having an ABI, 90% were recognised as having ‘severe or profound core activity limitations’ (Rushworth, 2008: 3). That is, children identified as having an ABI experience a wide range of disabilities, including fine motor, gross motor, self-care, social skills and cognitive deficits (Galvin et al., 2010b; McKinlay et al., 2016).
The impact of ABI on function, and the retention and re-acquisition of skills, varies significantly among individuals (Ewing-Cobbs et al., 2003). The long-term recovery from an ABI for children has been debated, with evidence to support an ‘early plasticity’ theory (that is, flexibility in the immature brain associated with good recovery) or ‘early vulnerability’ theory (that is, the vulnerability of the immature brain and poor recovery) (Anderson et al., 2011). Anderson et al. (2011) argue in their review that these opposing points of view are ‘extremes of a continuum of recovery’ (2199), depending on the child’s age, predisposition, environment and type of injury. While physical impairments, including changes in muscle tone, impaired balance and sensation, and reduced strength, endurance and coordination, may persist over time, researchers suggest that recovery of motor skills is faster and less complex than cognitive recovery (Galvin et al., 2010a). In the past two decades, considerable research has accrued in an attempt to appreciate the full cognitive ramifications of paediatric ABI (Ewing-Cobbs et al., 2003). The wide range of cognitive consequences includes, but is not limited to, changes in executive functions (Galvin and Mandalis, 2009), behaviour and personality (Chapman et al., 2010), attentional and processing skills (Anderson et al., 2005), and academic ability (Catroppa et al., 2009). Significantly greater cognitive fatigue has also been found in children with TBI, compared to typically developing children (Ryan et al., 2016). Cognitive fatigue is defined as a ‘decreased capacity for mental activity due to an imbalance in the availability, utilization, and/or restoration of resources needed to perform the activity’ (Ryan et al., 2016: 2). Cognitive fatigue is associated with reduced quality of life and is regarded among the most debilitating sequelae of paediatric TBI (Ryan et al., 2016). These cognitive consequences can limit participation in life activities.
Participation, defined as involvement in life situations (World Health Organization, 2001), is an important outcome of rehabilitation intervention as it plays a vital role in children’s development, learning and wellbeing (Anaby et al., 2012). Participation in occupations is directly related to positive long-term functional outcomes (Law, 2002). Studies aimed primarily at describing the participation patterns of children and youth with an ABI have determined that children, even with mild injuries, participate less than their peers across a variety of activities in the home, school and community (Anaby et al., 2012; Galvin Froude et al., 2010b).
Play is regarded as a child’s primary occupation (Parham and Primeau, 2008), and as a means through which children participate with their peers. Pretend play is a unique type of play that involves three key cognitive skills: the ability to substitute an object as something else; attribute properties to objects; and refer to absent objects (Stagnitti, 2007). To pretend in play a child is required to impose meaning on objects and play scenes and think beyond the literal (Stagnitti, 2007). Neuro-imagining studies have identified that when children engage in pretend play, activation occurs in the limbic system and cortex (Stagnitti, 2017). There is a growing body of evidence supporting the many connections between cognitive competence and pretend play (Lillard et al., 2010).
Fink et al. (2012) conducted the first study that directly measured the pretend play abilities of children with an ABI. They utilised an exploratory cross sectional design to measure the pretend play abilities of three children with an ABI using the Child-Initiated Pretend Play Assessment (ChIPPA) (Stagnitti, 2007). Children with an ABI demonstrated a range of pretend play abilities; however, none of the participants were able to complete the total time of the ChIPPA play session, and all had difficulties maintaining attention and engagement (Fink et al., 2012). This paper builds on Fink et al. by including a larger sample to further investigate the pretend play ability of children with an ABI.
The study aims were to investigate (1) if a larger sample of children with ABI displayed pretend play deficits; if so, (2) what are the pretend play deficits of children with an ABI; (3) do children with TBI perform differently to those with ABI; (4) does time since injury and age influence pretend play ability in children with ABI. It was hypothesised that: (1 and 2) children with ABI have pretend play deficits; (3) there will be no difference between children with TBI and ABI; (4) time since injury and age will influence pretend play ability.
Method
Research design
A non-experimental cross-sectional design was used to address the study aims. Ethical approval for this study was granted by Deakin University and The Royal Children’s Hospital. Written informed consent was obtained from all participants’ parents for their child’s participation in the study and for the publication of results.
Participants
Twenty-six children aged between 3 years 1 month and 7 years 11 months participated in this study. Participants were all receiving either inpatient or outpatient rehabilitation from the Royal Children’s Hospital (RCH) in Melbourne, Australia. The ABI stream coordinator approached parents of eligible children to offer a brief overview of the study and invite their child to participate. Voluntary participation was emphasised. To participate, children were required to be typically developing before their brain injury was acquired, out of post-traumatic amnesia as determined by a neuropsychologist, able to sit independently on the floor and able to tolerate either an 18-minute or 30-minute play assessment depending on age. Exclusion criteria were a previous history of developmental delay, non-accidental injury and medical or orthopaedic restrictions that limited the child’s ability to participate in a play session.
Instrument
The ChIPPA is a standardised, norm-referenced assessment of the quality of a child’s ability to self-initiate pretend play over a set time period (Stagnitti, 2007). The assessment is for children aged 3 to 7 years. Children aged 3 years are assessed for 18 minutes while children aged 4 to 7 years are assessed for 30 minutes.
The ChIPPA measures both conventional-imaginative and symbolic play by offering two sets of play materials sequentially. The ChIPPA measures and scores three aspects of children’s pretend play: the elaborateness of play (the ability to logically sequence play actions, which includes attribution of objects and reference to absent objects); use of symbols in play (the ability to substitute objects); and if the child requires a model on which to base play ideas (the child imitates the assessor’s modelled actions). These three items are accordingly titled ‘percentage of elaborate play actions’ (PEPA), ‘number of object substitutions’ (NOS) and ‘number of imitated actions’ (NIA). Each item is scored separately in the conventional-imaginative and symbolic play sessions, and then combined to create a combined score (see Table 1).
The ChIPPA items (abbreviation and description).

ChIPPA: Child-Initiated Pretend Play Assessment; PEPA: percentage of elaborate play actions; NOS: number of object substitutions; NIA: number of imitated actions.
The ChIPPA includes a clinical observations form where typical indicators and play deficit indicators are recorded for each child. For example, if the child creates a narrative in the play, if characters in the play are played with as if they are alive and if children use all of the toys. The ChIPPA has proven reliability and validity. Inter-rater reliability has been shown to be κ=.7 or above across two studies (Stagnitti et al., 2000; Swindells and Stagnitti, 2006). Test–retest reliability was also shown to be stable for elaborate actions and imitated actions, and moderate for object substitution scores (Stagnitti and Unsworth, 2004). In terms of validity, the ChIPPA has been shown to discriminate between typically developing preschool children and preschool children with suspected pre-academic problems (Stagnitti et al., 2000). Language and social competence can be inferred from ChIPPA scores (Stagnitti and Lewis, 2015). The norm sample for 4- to 7-year-old children is over 400 children (Stagnitti, 2007). Standard scores can be recorded as z scores with –1 to +1 being within the expected range for age. Scores below –1 are below that expected for age. Children scoring +1 or higher are showing ability to play at complex levels above that expected for their age.
Data collection
Prior to administration of the ChIPPA, demographic information was recorded for each participant via parent report and medical records. This information included injury/diagnosis, child’s age and time post injury at assessment. The first and second authors administered and scored the ChIPPA sessions. The first author was trained in the administration and scoring of the ChIPPA by the second author.
Each child was individually assessed once using the ChIPPA. The assessments were completed in a quiet room at RCH with parents given the option to remain in the room or wait nearby. All assessment sessions were scheduled with the child’s family for a time that ensured that the children were rested and able to participate. All children were assessed before two o’clock in the afternoon to reduce the fatigue that commonly occurs in young children following midday. Following the assessment, parents were given a verbal description of how their child played, and were asked if this was typical of their child’s play ability at home. The play assessment reflected the child’s play at home, with all parents confirming the verbal description. Parents were provided with a one-page feedback summary at the completion of data collection.
Data analysis
The Statistical Package for Social Science (SPSS) for Windows software version 22 was used in analysis. The children’s PEPA, NOS and NIA raw scores were compared to the ChIPPA normative scores. For aims (1) and (2), descriptive statistics were used as well as comparison with norms. The normative scores (z scores) were used to categorise the participants across four levels of performance for 4- to 7-year-olds. These were: (a) good performance (a z-score above the range, that is > +1); (b) performance expected for age (a z-score within the range, that is between –1 and +1); (c) delay for age (a z-score below the norm range, between –1.01 and –1.99); and (d) significant delay (a z-score < −2). For 3-year-olds, there are cut-points for delay and significant delay. T-tests were used to compare the time in minutes of assessment completed between those who completed the assessment and those who did not, unless group sizes were too uneven, then a Mann Whitney U test was used based on assumption of normality (Daniel, 2005). Clinical observations and notes of play behaviours were reviewed to add rich data to each of the aims.
For aim (3), a Mann Whitney U test was used and children were divided into groups, with one group being children with TBI and the other group being children with ABI. For this aim, raw scores were used as standard scores were not available for 3-year-olds. For aim (4) a generalised linear model was used as this model is suitable for samples under 100 (Agresti, 2015).
Results
All of the 26 children invited to participate completed the study. No parents declined for their child to participate or later withdrew. The sample size of 26 was calculated based on a two-tailed independent t-test with power of .70 and an effect size (using Cohen’s d) of .70 (Portney and Watkins, 2000). The effect size was an estimation based on the study by Fink et al. (2012). The mean age of the participants was 5.08 years (SD 1.58). The sample included 11 boys and 15 girls. There were 10 children with a diagnosis of TBI and 16 children with a diagnosis of ABI, stemming from various causes including meningitis, encephalitis, stroke and various other infectious and inflammatory disorders. At the time of assessment, time post injury ranged from 2 weeks to 208 weeks (43.5 weeks, SD 54.6). Just over a quarter of the sample (26.2%) were 4 weeks post injury and 69.2% were within 52 weeks post injury at the time of the study. Children with TBI were between 8 and 118 weeks post injury and children with ABI were between 2 and 8 weeks and 100 and 208 weeks post injury. The participants resided in suburban, regional and rural living environments and were from a broad range of socio-economic locations.
Aim 1 and 2 – pretend play ability of children with ABI
The children’s raw scores on the ChIPPA were compared to the norms and categorised to indicate performance across four levels of expectation (see Table 2 for 3-year-olds and Table 3 for 4- to 7-year-olds).
Comparison of sample raw scores to ChIPPA cut-point scores for 3-year-old children (n = 10).
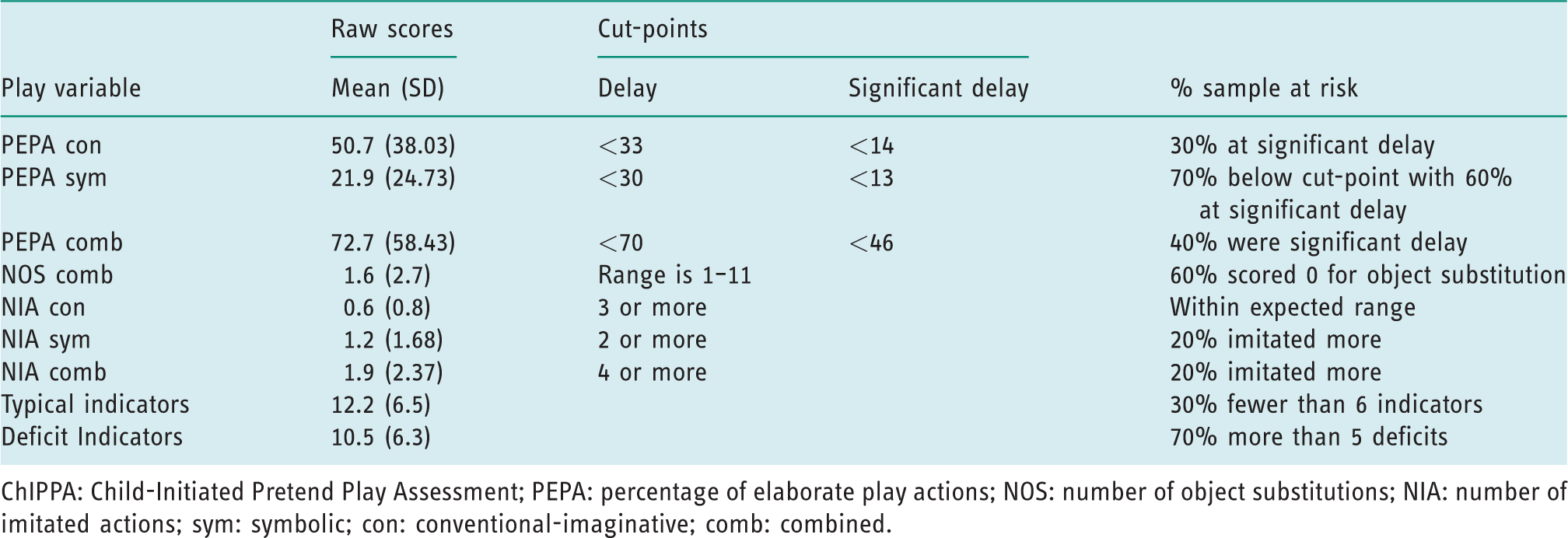
ChIPPA: Child-Initiated Pretend Play Assessment; PEPA: percentage of elaborate play actions; NOS: number of object substitutions; NIA: number of imitated actions; sym: symbolic; con: conventional-imaginative; comb: combined.
Performance of the sample aged 4 to 7 years compared with ChIPPA norms (n = 16).

ChIPPA: Child-Initiated Pretend Play Assessment; PEPA: percentage of elaborate play actions; NOS: number of object substitutions; NIA: number of imitated actions; comb: combined; con: conventional-imaginative; sym: symbolic.
Tables 2 and 3 show that children with an ABI display a wide range of pretend play ability and that there were more than twice as many children (17 of 26 children) who performed below expectations for their elaborateness in symbolic play compared with their elaborateness in conventional-imaginative play (9 of 26 children). Three-year-olds were less able to use symbols in play (M=1.6, SD=2.8) compared to 4–7-year-olds (M=7.88, SD=9.2) and three-year-olds imitated more frequently (M=1.9, SD=2.37) than the 4–7-year-olds (M=0.43, SD=0.89). This would be expected for age. On the clinical observations form, scores for pretend play deficits ranged from 1–19 out of a possible 23.
As seen in Table 4, nearly three quarters of the children could not complete the time of the assessment (73%). Of this 73%, two 3-year-olds and two 4-year-olds finished within three minutes of the total time, with all other children ending the assessment much earlier than expected for their age. The majority of children who were unable to complete the time did so because they had either run of out of play ideas or could no longer sustain the play story that they were working on. Children indicated that they wanted to finish playing by packing toys away or verbal notification that they had finished or didn’t want to continue. Children were often unable to incorporate an ending into their play narrative and frequently finished by killing the dolls and animals or abruptly stopping the story. For many of the children the cessation of their play was sudden and abrupt, even for those who showed complex play ability. When this occurred, no amount of encouragement was successful in re-engaging the children.
Children who did not complete the time (n = 26).

Children were observed to change play ideas regularly, thus not following through in a sequence of play actions, or working slowly with frequent pauses in the play. Some children could set up a play scene, and then stopped playing without developing a narrative in the play. Many participants were noted to ‘lose track’ of their ideas, which was recorded as an inability to logically sequence play actions. Inattention, distractibility, disengagement and limited concentration were observed in this sample of children. Organisation of the play space and materials was generally poor, and this was exhibited as an inability to use all of the play materials, with play materials scattered across the play space or left in a pile. Repetition of play actions indicates difficulty with elaboration of play and for many children this amplified as the assessment time progressed.
No significant differences in performance were found between participants who were not able to complete the assessment time. This means that an ability to complete the total time of the ChIPPA did not indicate elaborate pretend play. The hypotheses were supported that children with ABI show difficulty in pretend play ability.
Aim 3 – play ability of children with TBI and children with ABI
A Mann Whitney U test was used to analyse differences between groups. No significant differences were found for raw scores across all play variables between children with ABI and children with TBI. The TBI group raw scores were lower in elaborate play, object substitution and typical play indicators, and they played for less time compared to children with ABI. The hypothesis was partially supported.
Aim 4 – time since injury and age influence on pretend play ability in children with ABI
A generalised linear model was completed to determine if time post injury and age were predictive of PEPA combined scores as an indicator of quality of play. Time post injury and age were the predictors, and play quality (PEPA combined raw score) was the dependent variable. The factor was diagnosis. Time post injury was not associated with quality of play (B = .221, p = .15; CI (95%) –0.08–.5). Age was not associated with quality of play (B = 7.46, p = .17; CI (95%) –3.23–18.1). The same analysis was repeated with PEPA symbolic as the dependent variable. Time post injury was not associated with quality of play (B = −.079, p = .83; CI (95%) –.8–.65), and age was not associated with quality of play (B = −.15, p = .22; CI (95%) –.38–.09).
The sample was further divided into those with a time post injury less than 52 weeks, and those with a time post injury 52 weeks or greater. As there were unequal group sizes (17 in the group less than 52 weeks) a Mann Whitney U test was carried out and no significant difference was found between time post injury less than 52 weeks (82.4 SD 39.4) and time post injury 52 weeks or more (80.2 SD 56.1) for PEPA combined. Further analysis showed no significant difference between groups for object substitution ability. Further analysis also showed non-significant weak relationships between time post injury and quality of play (r = .12, p = .37 for PEPA combined and r = −.01, p = .96 for object substitution). The hypothesis was not supported.
Discussion
The ChIPPA scores reflect children’s complexity in the quality of their ability to self-initiate elaborate pretend play and use symbols in play. In this study, 17 of the 26 children were delayed in their ability to elaborate in symbolic play and 16 were very delayed in their ability to use symbols in play. Low elaborate symbolic play scores and object substitution ability indicate low organisation and coherence in play, difficulties playing in unstructured play situations, difficulties socially connecting with peers, and thinking more literally (Stagnitti and Lewis, 2015). Object substitutions in play are strongly linked to language and learning, and their absence is a diagnostic marker of language delay (Smith and Jones, 2011). It was not surprising that the older children in the sample had significantly more object substitutions in their play because there is a large developmental change in this ability from 4.5 years (Stagnitti, 2007). However, the ability to elaborate with only unstructured objects is a demanding cognitive ability, with 12 children being significantly delayed in this ability compared to five children being significantly delayed in conventional-imaginative play (elaborate play with toys).
While the range of imitated action scores placed the majority of the sample within that expected for their age, the pattern of play scores gives a more nuanced understanding of a child’s function. No imitated actions together with poor elaborate play and low object substitution scores indicate a deficit play style (Stagnitti, 2007). The majority of children in this sample had a deficit play style. Low elaborate play ability and low object substitutions were also found to be play abilities that discriminated children with suspected pre-academic problems compared to peers where teachers and parents had no concerns (Stagnitti et al., 2000).
Time post injury was not predictive of play ability. This was unexpected as it was hypothesised that time post injury would be a factor. Children who had injuries more than one year prior to the study did not perform above those children who had more recently experienced injury.
Pretend play and cognitive fatigue in children with ABI
For children to act ‘as if’ when existing within a hypothetical scenario necessitates a considerable amount of cognitive ability for abstract and flexible thought. Bergen (2002) asserts that pretend play engages many, if not all, areas of the brain because it involves emotion, cognition, language and sensorimotor actions. Perry (2006), based on his work with children who had experienced trauma, developed the neurosequential model, and within this model play at the limbic and cortical level encourages storytelling and drama. Pretend play involves storytelling as children develop stories in their play and carry out roles (Stagnitti, 2017). Whitebread and O’Sullivan (2012) argue that pretend play is intellectually demanding, with demands increased when children engage in social pretend play. Metacognition and representational thought, creativity and narrative understanding are essential for children to engage in complex pretend play (Hughes and Leekam, 2004; Nicolopoulou and Ilgaz, 2013).
This study concurs with the findings of Fink et al. (2012) in that children had difficulty engaging in pretend play for the time of the ChIPPA. The time of the ChIPPA is 30 minutes for 4- to 7-year-old children and 18 minutes for 3-year-old children. Children who are typically developing in their play have no difficulty playing for this length of time, with 4- to 7-year-old children, who are immature, finishing between 26 and 30 minutes (Stagnitti, 2007). Children in this study had difficulty playing for the time of the assessment (see Table 4), with the added observation that children who were competent players abruptly stopped play before the time was up. This latter observation has not been noted in any other clinical group to date with the ChIPPA (for example, see Lin et al., 2017; Pfeifer et al., 2011).
With the cognitive demand that is required for children to engage in pretend play, it is argued that cognitive fatigue impacted on the ability of children to complete the time of the assessment and is a possible explanation for why there was abrupt cessation of play even for children who showed complex play ability. Ryan et al. (2016) identified cortical-striatal correlates of cognitive fatigue in a paediatric brain injury study with children with TBI. For adults with an ABI compared to their healthy, age-matched peers, Kohl et al. (2009) established by the use of functional magnetic resonance imaging that more cerebral effort was required to complete tasks. Given the knowledge about the considerable amount of cognitive effort engaging in pretend play demands (Fink et al., 2012; German et al., 2004; Whitehead et al., 2009), it is argued that for the children in this study, engaging in pretend play generated a substantial physiological toll that resulted in them becoming cognitively fatigued. Children found it difficult to sustain a long sequence of play actions and exhibited behaviours such as distractibility, losing lines of thought and stopping play abruptly. Cognitive fatigue is considered one of the most challenging symptoms following paediatric brain injury (Ryan et al., 2016).
Limitations
The generalisability of these findings is limited due to the small sample size, although a sample size of 26 was estimated to give acceptable levels of power. While the sample was heterogeneous, it did not reflect the prevalence rate of ABI for boys and girls in Australia as there was a higher proportion of girls in this study. The activities that the children in this study participated in prior to their assessment were unable to be controlled. All children were assessed before 2 o’clock in the afternoon to account for fatigue during the latter part of the day.
Summary and conclusions
Children with ABI present with a range of abilities in pretend play. With such a variance in skill, this study highlights the need to ensure interventions are individualised for each child with an ABI. A pattern emerging from this study was that nearly three quarters (73%) of the children were unable to complete the total assessment time and that symbolic play ability, in particular, was delayed for these children. It is argued that cognitive fatigue, and the demands of engagement in a complex occupation such as pretend play, impact on ability to engage in pretend play for long periods of time for children with ABI. This has profound implications for the delivery of effective service to these children, with therapy sessions to be in short bursts and to focus on the more abstract play ability of using symbols in play. Future research that explores length of time in intervention and outcome would be valuable, as well as the long-term outcomes of interventions that focus on building symbolic play capacity in this group of children.
Play is an important occupation of childhood, and when children engage in pretend play they impose meaning on their play that goes beyond the literal meaning of the objects or play scene. Occupational therapists including an assessment of pretend play in their work with children with ABI will inform practice by giving insight into the child’s functioning and level of cognitive fatigue. This study emphasises that, given the complex cognitive ramifications of cerebral insult in children and the emerging knowledge about cognitive fatigue and play and the brain, understanding the pretend play ability of children with ABI will give insight into that child’s ability to participate in daily life.
Key findings
Children with ABI have difficulty playing symbolically and for periods of time expected for their age. Cognitive fatigue was observed when children abruptly ended their play session.
What the study had added
Understanding the pretend play ability of children with ABI informs occupational therapy practice as it impacts on a child’s ability to participate.
Footnotes
Research ethics
Ethical approval was obtained from Deakin University Human Research Ethics Committee, Ref no: 2011-213, Year: 2011 and the Royal Children’s Hospital Research Ethics Committee, Ref no: 31158, Year: 2011.
Consent
All participants’ parents provided written informed consent for their children to participate in the study.
Declaration of conflicting interests
The authors declared the following potential conflict of interest with respect to the research: author two is the author of the Child-Initiated Pretend Play Assessment used to measure the participants’ pretend play abilities in this study. Author two was not involved in data collection and participants’ scores on the ChIPPA were peer-checked to ensure reliable scoring by the principal researcher.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Contributorship
Bridget Dooley, Karen Stagnitti and Jane Galvin researched the literature, applied for ethical approval, and contributed to the development of the data. All authors contributed to the methodology of the project and the statistical analysis plan. Bridget Dooley and Karen Stagnitti carried out the statistical analysis, and all authors interpreted the data. Bridget Dooley wrote the first draft of the manuscript, which was edited by Karen Stagnitti. All authors reviewed the edited manuscript and approved the final version.