
Abstract
Occupational therapists promote meaningful engagement in occupations and associated role continuity, and encourage agency and citizenship. A lack of engagement can be understood as occupational deprivation, alienation and marginalisation, which are concepts associated with occupational injustice. However, occupational injustices associated with collectives, such as residential aged care settings, receive little professional attention. This article encourages the occupational therapy profession to research and develop practice addressing occupational injustice within collectives, specifically in residential aged care settings. Proposed key considerations include environmental adaptations, creating occupational spaces and upskilling staff to promote citizenship, agency and self-determination for residents.
Keywords
Fuelled by our profession’s ambitious attempts to enable access to meaningful occupation for all, keynote addresses by Ramugondo (2018) and Hammel (2018) at the World Federation of Occupational Therapists Congress 2018 highlighted the importance of occupational justice and a focus on collective engagement in various settings. McGrath (2017: 558) warns that ‘despite growing professional interest in occupational justice and participation, daily occupational therapy practice often fails to confront issues of occupational justice’. This opinion piece proposes mechanisms for promoting a more engaged life for aged residents as members of collective settings.
Stadnyk et al. (2010: 331) describe occupational justice as ‘meaningful and purposeful occupations (tasks and activities) that people want to do, need to do, and can do considering their personal and situational circumstances’. For residents, barriers to occupational justice may lead to a lack of occupational engagement that creates a loss in personal purpose and meaning; a loss of roles, identity and sense of continuity; and exacerbates a loss of agency, contribution and citizenship. These highlighted occupational justice issues can be framed as occupational deprivation when aged residents spend their days sleeping and unengaged. In association with the deprivation experienced by residents, staff are prone to experience occupational marginalisation due to the busy, highly regimented routines (see, for example, Thomas et al., 2014). Residential care contexts are therefore complex and pose occupational justice issues for various groups, whether due to having too little (deprivation) or too much (marginalisation) to do, within this collective.
The role of the occupational therapist in aged residential care
The traditional practice of occupational therapy focuses on the individual, and discipline-specific literature predominantly reports on individual, rather than collective, outcomes (see, for example, Adams and Casteleijn, 2014). Most assessment tools, outcome measures and profession-specific models of practice available to guide occupational therapists are focused on the person, creating a confined scope of individualised practice that emphasises functional outcomes.
In residential care contexts, our profession lacks an approach that distinguishes us from less expensive and, in many cases, equally effective colleagues. Occupational therapy for individuals in residential care is perceived as an expensive intervention in comparison to that of an activity therapist or nursing aide. Additionally, funding structures often dictate the occupational therapy role within aged residential care to focus on pain management or issuing assistive devices. When considering the associated cost of having a group-based leisure programme run by volunteers, it is hardly surprising that group interventions are not viewed as an occupational therapy domain in this care context.
Besides the ability to enable meaningful engagement for residents despite their level of ability, the occupational therapy profession could address other occupation-specific issues affecting staff that cause them to experience disenfranchisement and disempowerment (Thomas et al., 2014). To date we have limited data to document how occupational therapy could add significant value to existing residential care services.
Changing our game
While there will always be the need for skilled occupational therapy services for individuals, we recommend that our profession adopt a more strategic and comprehensive approach to residential populations. Pereira and Whiteford (2013) recommend changing our focus to the collective to promote social and environmental change that will influence social policy. In this opinion piece, we reinforce these ideas. We recommend that residential facilities are viewed as micro-communities (Du Toit et al., 2018) and strive towards a shared vision and intentionality to collectively achieve outcomes that are mutually beneficial (Adams and Casteleijn, 2014). A shared vision by staff, families and residents will lead to the increased belonging and meaningful engagement of all parties. However, this process of participating collectively does not come automatically and requires expert facilitation.
We propose that an occupational therapy focus on collective participation within aged care settings would greatly contribute towards health and wellbeing. The right to active and engaged ageing for older adults is supported by our profession. Policies acknowledging older people’s right to self-fulfilment through meaningful engagement are complemented by a large body of multi-disciplinary research evidence documenting the adverse impacts that inactivity, lack of connection/loneliness and boredom have on institutionalised people (see, for example, Brownie et al., 2014). Moreover, by addressing meaningful engagement for both residents and staff, staff burnout could be prevented when purpose and meaning are incorporated into caregiving. Meaningful engagement can also support occupational identity (Thomas et al., 2014).
At the beginning of the new millennium, Ilott et al. (2006: 40) urged for ‘an openness to new ways of thinking and doing; and a commitment to offer services of proven effectiveness’ to promote the agenda for evidence-based practice in occupational therapy. Our next step should be to incorporate collectives into this agenda through the combined effort of national associations, occupational therapy services and individual practitioners. Research initiatives to build empirical evidence are needed to address our deficiency in authoritative research on collective settings, without which the profession’s comments remain devoid of expert status.
Residential care as a collective context
Aged residential care settings contain neighbourhoods within a finite geographical setting, creating a contrived micro-community (Du Toit et al., 2018). Paradoxically, current residential care settings typically foster a lack of belonging and exclusion from collective intentions, which leads to feelings of isolation, anxiety and dissatisfaction among staff, residents and families (Thomas et al., 2014). These micro-communities are the ideal settings to investigate and research the social impact of creating collective occupations such as group participation and the involvement of external communities. The need for belonging within a micro-community could address social cohesion while simultaneously advancing a common good (Ramugondo and Kronenberg, 2015). Furthermore, the unique occupational science perspective on how settings affect function, integration and engagement in everyday occupations (see, for example, Morgan-Brown and Chard, 2014) can be utilised to explore and explain how the routines and habits of daily life within micro-community settings positively promote collective occupations.
Townsend and Polatajko (2007) identify four features that provide a way to conceptualise the whole setting, namely (a) accessibility and access to everyday objects (physical environment); (b) access to relationships and social engagement, and the use of language (social environment); (c) ethnicity and spiritual preferences (cultural environment) and (d) an organisation’s care culture (institutional environment). These features could support identifying potential barriers or enablers to collective engagement within a residential care facility micro-community.
Substantiating a whole-setting perspective
Addressing the collective needs of a residential care facility as a micro-community and identifying sources of occupational injustices requires a whole-setting perspective. At present, there is very little occupational science-specific research and our values and outcomes for enhancing meaningful engagement rely mostly on measures developed by other professions, such as such as dementia care mapping (Brooker and Surr, 2005). Other important multi-disciplinary research focuses on the impact of settings on occupational and social engagement (see, for example, de Boer et al., 2017) and on the factors that make it most likely that individuals will engage in occupations (see, for example, Cohen-Mansfield et al., 2017). To add to the body of evidence, interventions and contributions should be assessed with valid and reliable measures, such as the Assessment Tool for Occupational and Social Engagement (Morgan-Brown and Chard, 2014) and the Residential Environmental Impact Scale (Fisher et al., 2014), which evaluate and compare collective occupational engagement within a whole setting from an occupational perspective.
Collaborative engagement in everyday occupations in a residential care setting would enable an older adult to build a sense of belonging, personal identity and interdependence with others (Ramugondo and Kronenberg, 2015), promoting occupational justice. Thriving micro-communities, which foster citizenship for older adults living in residential care, depend on the meaningful engagement of both residents (Du Toit et al., 2018) and staff (Thomas et al., 2014). An essential component of meaningful and mutual engagement is an objective analysis of institutional contexts that impact on staff occupations and consequent engagement with residents. Research is required to understand how to translate real life contexts into settings that support a shared collective vision, with collective actions amongst staff that promote engagement with one another and with residents.
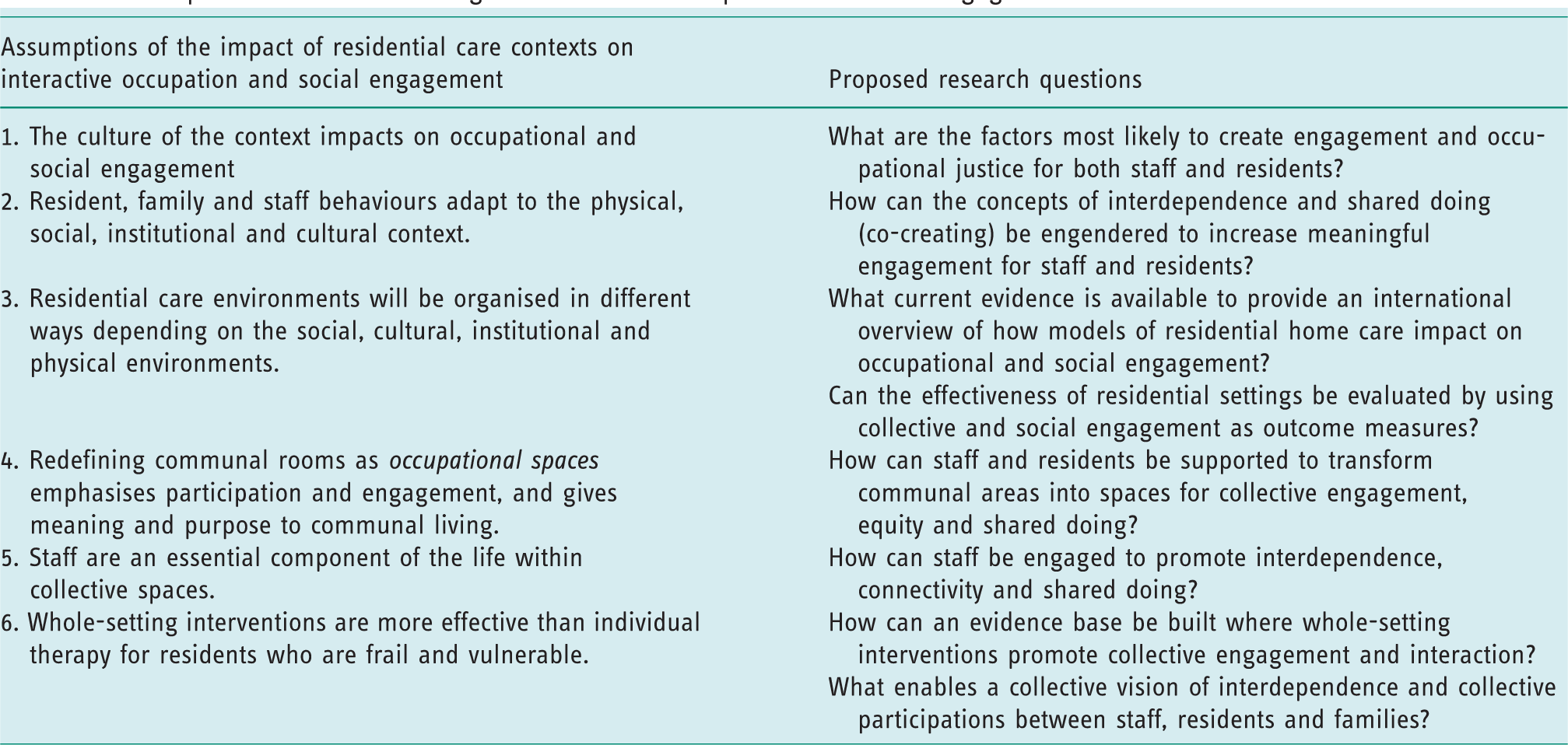
Understanding meaningful engagement within a collective requires all factors within the whole setting to be considered. Only then would the collective increases in social and occupational encounters reflect the belonging and meaningful engagement of everyone in that setting (Du Toit et al., 2014). Morgan-Brown and Du Toit (2018) propose six assumptions about residential settings that impact on levels of interactive occupation and social engagement (see Table 1). They recommend that these assumptions need to be investigated in order to build a solid data base that will underpin the occupational therapy profession as it seeks to better the lives of those living in residential care. Table 1 proposes how assumptions about residential contexts could be explored to develop collective-specific theories, recommendations and interventions.
The impact of residential settings on interactive occupation and social engagement.
Summary
This article challenges occupational therapists to consider how they could influence meaningful engagement for an aged residential care setting and to widen our focus from an individual to a collective approach. This redirection needs the support of national and international associations to develop strategies for prioritising research and accessing funding in order to create a substantial evidence base for evaluating and strengthening environmental interventions (physical, social, organisational and cultural) and to support evidence-based occupational therapy roles that will achieve greater occupational engagement in collective settings.
Key message
The occupational therapy profession needs a holistic, evidence-based approach to promote occupational justice in the collective context of residential care.
Footnotes
Research ethics
Research ethics is not relevant to this opinion piece.
Consent
Consent is not relevant to this opinion piece.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Contributorship
Sanetta du Toit and Daleen Casteleijn planned the initial focus of the article. Sanetta du Toit and Mark Morgan-Brown wrote the first draft of the manuscript. All authors reviewed and edited the manuscript and approved the final version.