
Abstract
Introduction
Individuals with visual impairment may choose to use a mobility scooter for meaningful community mobility. This study investigated what self-regulation strategies older adults with visual impairment employed to ensure effective mobility scooter use.
Method
This interpretive description study used multiple methods, including participant observation and semi-structured interviews. Among the 15 participants, a variety of visual impairments was represented.
Results
Participants described the various reasons for getting a scooter. They also detailed risks and barriers that warranted self-regulation strategies including the environment, the visual impairment and the attitudinal approaches.
Conclusion
Barriers to community participation are common for people with visual impairment. This study adds detailed accounts of strategies for the competent management of such barriers using self-regulation practices. These practices can be applied in the community to maintain/improve infrastructure accessibility, address public understanding of scooter use and educate individuals with visual impairment of strategies to improve their scooter use.
Keywords
Introduction
Community mobility, the ability to travel beyond one’s home, is a key concern for any occupational therapist when supporting a client to live with meaning and purpose. Community mobility allows a sense of connection to place and people, and influences individuals’ health and wellbeing (di Stefano et al., 2012).
Mobility scooters (scooters) are popular community transport choices for individuals with limited mobility (Australian Competition and Consumer Commission, 2012). Scooters are a powered mobility device with 3–4 wheels that travel at low speeds (typically 5 km/h–15 km/h) on the footpath. They differ from powered wheelchairs as their speed and steering controls sit in a console in front of the user and they have a larger turning circle. However, overall scooters are a similar weight and power to powered wheelchairs. Townsend and Watson (2013) suggest that necessary prerequisite skills to use a scooter include ‘coordination, strength, balance, endurance, visual acuity and visual fields, depth perception, reaction time, memory, concentration, insight, divided attention and judgement’ (455). They also suggest that occupational therapists have the necessary skills for comprehensive scooter assessment considering the range of suggested prerequisite skills (Townsend and Watson, 2013), and undoubtedly such a role is a natural progression from well-established roles in assessment of vehicle driving and wheelchair prescription. Occupational therapists are researching scooter use, as shown by studies from Australia (Maywald and Stanley, 2015), Canada (Mortenson et al., 2015) and the Netherlands (Cordes et al., 2018). As occupational therapists develop their role regarding scooters, evidence-based practice is essential to ensure decision-making is supported and consistent, especially for novice occupational therapists working in scooter prescription (Maywald and Stanley, 2015).
As scooters become more prevalent on footpaths, they are increasingly scrutinised for their potential to disrupt footpaths and harm others. At present there is no regulation of scooters in New Zealand (NZ) policy, but any increase in the negative reporting in the media, as found by Stowe and Mulley (2010), may create a demand for regulation and there is particular concern that individuals with visual impairment (IVI) will be a target of such policies.
This study looked at the NZ context; however, it is useful to consider worldwide approaches to scooter regulation. In Queensland scooter use must be approved by a general practitioner, whereas throughout the rest of Australia scooter assessment is only required in the case of public funding applications, and all scooter use is restricted to 10 km/h (Townsend and Watson, 2013). In the United Kingdom, scooters are only permitted to be used by people with a mobility impairment and scooter speed is restricted to 12 km/h on the road and 6 km/h on footpaths (Department for Transport, 2015). In the Netherlands, scooters can travel up to 45 km/h on the road, 30 km/h in cycle lanes and 6 km/h on the footpath.
Within the NZ health system, a health professional (often an occupational therapist) may provide scooter training when the scooter is needed due to an accident; otherwise, training (if any) is provided by family, friends, retailers or community organisations. In some cases, when public funding is requested for a scooter, the applicant may require pre-assessment by a health professional; otherwise, a scooter user qualifies purely if they can privately fund it. The NZ Transport Agency (2015) provides written guidelines for scooter users and, although rarely used, the NZ police do have the jurisdiction to charge scooter users with disorderly driving.
Scooter use is therefore largely self-regulated, rather than regulated by legislation. Self-regulation is a concept typically used with older drivers, and is not usually applied to scooter use. Laliberte Rudman (2006) describes driving self-regulation as an ongoing process of achieving mobility goals within the context of an acceptable level of comfort. Donorfio et al. (2008) portray driving self-regulation as an active calculation that involves weighing up ‘the meaning of driving for the individual, what alternatives are available (if any) and how attractive they are, as well as age, health, and lifestyle concerns’ (331).
Although self-regulation is not usually applied to scooter use, it can be seen that common strategies occur across both driving and scooter use. For example, both drivers and scooter users may choose a quieter time of day to go out, they may increase levels of concentration, and restrict travel to familiar routes (Donorfio et al., 2008; Fomiatti et al., 2014; May et al., 2010; Mortenson et al., 2015).
Some specific populations are known to have lower rates of community mobility due to their experience of disability or environmental limitations, including individuals with visual impairment (IVI) (Blaylock et al., 2015). Barriers to community mobility for IVI include the inability to drive or access public transport, a lack of confidence and difficulty navigating poorly designed or maintained footpaths (Brouwer et al., 2008; Wilton and Davey, 2007). To facilitate their mobility, IVI report self-regulation strategies as pedestrians that relate to driving self-regulation strategies, such as carefully planning routes and travelling at a slower pace (Brouwer et al., 2008; Gallagher et al., 2011; Laliberte Rudman and Durdle, 2008; McGrath et al., 2017; Montarzino et al., 2007). However, IVI have a higher rate of physical impairments than their non-sight-impaired peers, compromising their ability to walk as a means of transport (Crews et al., 2006). For all these reasons, some IVI choose to use scooters for managing community mobility.
There are few studies of scooter use among IVI and there might be an assumption that visual impairment precludes the use of scooters. For example, in Australasia some professionals reported actively discouraging IVI from using scooters simply due to being clients of visual impairment services (Deverell, 2011). However, in the Netherlands, Cordes et al. (2018) measured the scooter performance of participants with a range of visual impairments and found that the visual impairment was not a predictor of capacity to use the scooter. In addition, a small NZ study found that scooter use contributed to the IVIs’ wellbeing and autonomy, with participants suggesting a range of self-regulation practices (McMullan and Butler, 2018).
This study set out to add to the small literature on self-regulation by scooter users, by investigating how IVI self-regulate their scooter use. The study aimed to gain an understanding of barriers to participation, individual strategies for managing visual limitations and the promotion of ongoing community mobility for older adults with visual impairment and mobility needs.
Method
Research design
An interpretive description approach was used because of the intention to ensure clinical application of the results (Thorne et al., 1997). The interpretive description methodology provides health professionals with a non-categorical, generic methodology that allows integration of clinical context and practitioner knowledge rather than a sole focus on creating theory from the data set (Thorne et al., 1997).
Data collection included a combination of ‘go-along’ participant observation, interviews and optometry reports.
The study was granted ethical approval and all participants provided written informed consent. Participants chose or were given pseudonyms to preserve anonymity. Participant information and informed consent documents were provided in large text, and an audio file of these documents was available.
Participants
The study was undertaken at several sites in NZ, deliberately including a variety of terrains and town sizes. Purposive sampling was used to recruit participants through advertisements, word of mouth and by asking key contacts to pass on information about the study. In this way, contact was made with scooter retailers, a low vision rehabilitation clinic and retirement villages. Respondents contacted the researchers if they were interested in volunteering for the study.
The inclusion criteria were that all participants had to have a diagnosed uncorrectable visual impairment, be aged over 60 years and use a scooter regularly. In total, 15 participants were recruited and agreed to take part (Table 1). Eight of the participants came from retirement villages and all the participants identified as pākehā (European/New Zealand European). Due to a variety of comorbidities, all of the participants reported they were unable to walk the distance of the journeys that they undertook on their scooter. One participant was unable to walk unaided, whereas other participants could walk some distance but could not, for example, carry groceries.
Participant descriptions.

ARMD: age-related macular degeneration; F: female; M: male; L): left eye; R): right eye; VA: visual acuity; VFI: visual field index.
Procedures
Part 1
After an initial introduction, the participants were asked to go on a short scooter journey along a familiar route: the ‘go-along’ method. During the go-along, the participant demonstrated their individual scooter techniques while the researcher recorded the conversation and took notes (Kusenbach, 2003). The researcher avoided distracting the participant by letting the participant direct the conversation and being conscious of giving the scooter priority on the footpath. As this interview was participant-led, a question schedule was not used; participants tended to discuss difficult and/or meaningful areas, and their scooter techniques. The go-along was optional and three participants declined this data collection method. The go-along offered observation of the participants’ speed, interactions with environmental features, their unique strategies, and more. As Kusenbach (2003) explains, a go-along provides an opportunity to ‘render visible some of the filters that shape individual environmental perception’ (478).
Part 2
The go-along was followed by a sit-down interview in a quiet location of the
participant’s choice (unanimously the participant’s own home), which was
recorded and allowed for robust discussion following a question schedule and
revisiting any important details from the go-along. Questions included:
reasons for having a scooter (including
comorbidities); visual impairment and how it affected scooter
use; a typical outing on a scooter; experience of using a scooter over time; what makes the IVI feel comfortable/discomfort on their
scooter; when the IVI chooses not to use a scooter; why scooter use may cease; opinions of scooter regulation including assessment and
training.
Participants were also asked to provide a recent optometry or ophthalmology report to describe each participant’s level of visual impairment. Based on experience from a previous study (McMullan and Butler, 2018), it was assumed participants would have optometry/ophthalmology reports available, eliminating the need to make further vision measurements. Unfortunately, it was found that the vision reports provided inconsistent information, most including only visual acuity and visual field, but not contrast sensitivity, glare sensitivity, useful field of view or any comparative measures of functional vision. In spite of these inconsistencies, it was clear that all participants had a diagnosed visual impairment and met the inclusion criteria. Participants were welcome to have a support person present during any stage of the data collection.
Data collection
The lead researcher carried out the data collection during 2017, meeting participants on one occasion in their own homes. Each interview took between 40 and 90 minutes.
Data analysis
Data analysis followed the Qualitative Analysis Guide of Leuven (QUAGOL) and was coded using the Quirkos software (Dierckx de Casterle et al., 2012). The go-along and sit-down interviews were transcribed verbatim, with observation notes embedded into the text. The transcriptions were then summarised into a report giving a narrative of each interview. These interview reports were analysed by both authors for preliminary codes before testing codes against the original transcript and then against other interviews. A list of concepts related to the preliminary codes was applied to the transcripts, exploring the definition of these concepts in order to determine an essential structure across the data set and come to the final themes. This process of data analysis was non-linear and iterative, with regular meetings between the two authors to arrive at the final findings.
Trustworthiness
Participants were provided with a verbatim transcript of the interview and a narrative interview report to view the information that would be included in the study and make any amendments or additional comments for member-checking (Shenton, 2004). Peer-reflexivity was enhanced through presentations to and discussion with occupational therapists and other stakeholders (Shenton, 2004). Both this study and the previous study (McMullan and Butler, 2018) were introduced in online presentations, at visual impairment consumer group meetings and at conferences, welcoming scrutiny from peers including practising NZ occupational therapists and others interested in visual impairment, accessibility and disability rights. The use of participant observation (the go-along) and interview provided a form of triangulation with all but the three participants who declined the go-along (Shenton, 2004).
Results
The findings fall into the three themes of ‘reasons for getting a scooter’, ‘risks and barriers associated with using a scooter’ and lastly ‘strategies used by scooter users’, with the three subthemes of ‘taking the environment into account’, ‘taking the visual impairment into account’ and ‘attitudinal strategies for managing scooter risks’ (see Table 2).
Themes layout.

Reasons for getting a scooter
Participants’ self-regulation began with the decision to acquire a scooter, with participants detailing their individual reasons for getting a scooter.
Alternative transport was generally limited to lifts from family members. Five participants could use a bus, and most would use a taxi. However, buses or taxis were often non-existent, irrelevant, unaffordable and/or inaccessible. Three participants lacked any alternative modes of transport, as May explained: ‘What else would I do apart from scooter? I can’t walk, I can’t hop, I can’t skip. It’s a really strange question… I grow wings and fly? So you suggest another way I can get from A to B’.
Scooter use also served to maintain connections with the neighbourhood or to enhance their overall wellbeing. Una stated, ‘that’s the big thing about scooters, you’re out in the fresh air, you’re not inside. You don’t get bedsores and things like that’. Scooter use also supported emotional self-regulation, as Mouse explained: ‘[when I get upset] it makes me feel like I want to get on the [scooter] and go for a ride’.
Poppy and Clint both used their scooter to access safe spaces for walking. For
example, they went to large stores because these offered warmth, adequate clear,
flat space and good lighting. The scooter appeals to individual values of
independent travel, allowing expressions of freedom, autonomous community
engagement and doing so with privacy. May particularly used her scooter to
support her social needs: ‘[my grandson] came down and did the rail trail with
me last year, he was only nine’. Scooters could also contribute to the feelings
of adventure and freedom: I love it. I need it. It just gives me independence. My daughter and my
family would do my grocery shopping for me, but I don’t want to lose
that. I want to still be able to choose what I want.
(Chiconne) I do know some of the people here say, ‘Oh, I couldn’t drive a scooter’,
and they won’t even try. So, I suppose it’s a matter of having a bit of
confidence. And yet they’ve all driven cars. They’re just silly, they
won’t try. (Matilda)
Social supports also played a role in the decision to get a scooter. Some participants felt supported in their decisions, while others felt discouraged but still went ahead: ‘I know that the Blind Foundation are not happy with having people with low vision on them… my GP was just a little bit concerned’ (Arthur).
May had a choice between a wheelchair and a scooter, and felt that the scooter was less stigmatising: ‘you’re a lot more patronised in the wheelchair, and they usually talk to the person pushing. But when you’re on a scooter, they must think that you can do something’.
Risks and barriers associated with using a scooter
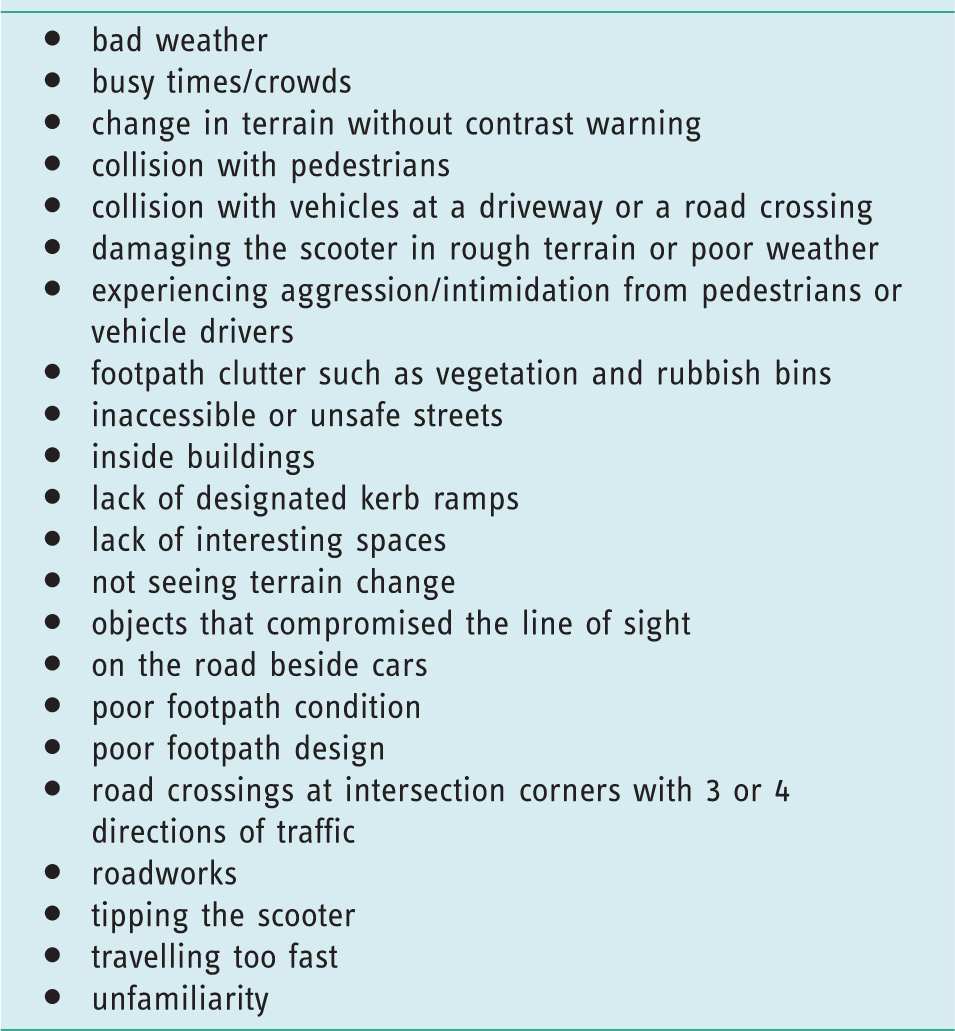
Self-regulation is only necessary in response to risk of harm, so before discussing self-regulation techniques, the risk of harm and barriers to participation need to be introduced. Participants described many physical features, personal limitations and social environmental factors that posed as risks and barriers to effective scooter use. These risks and barriers are compiled in Table 3 to allow a quick reference to the variety of issues that participants reported. Across the sample, the degree of concern about each item varied according to the individual’s personal circumstances, discussed further in ‘Strategies used by scooter users’.
Risks and barriers associated with using a scooter.
Strategies used by scooter users
Consequently, the third theme and its subthemes present specific details of self-regulation tactics used in response to the described risks and barriers.
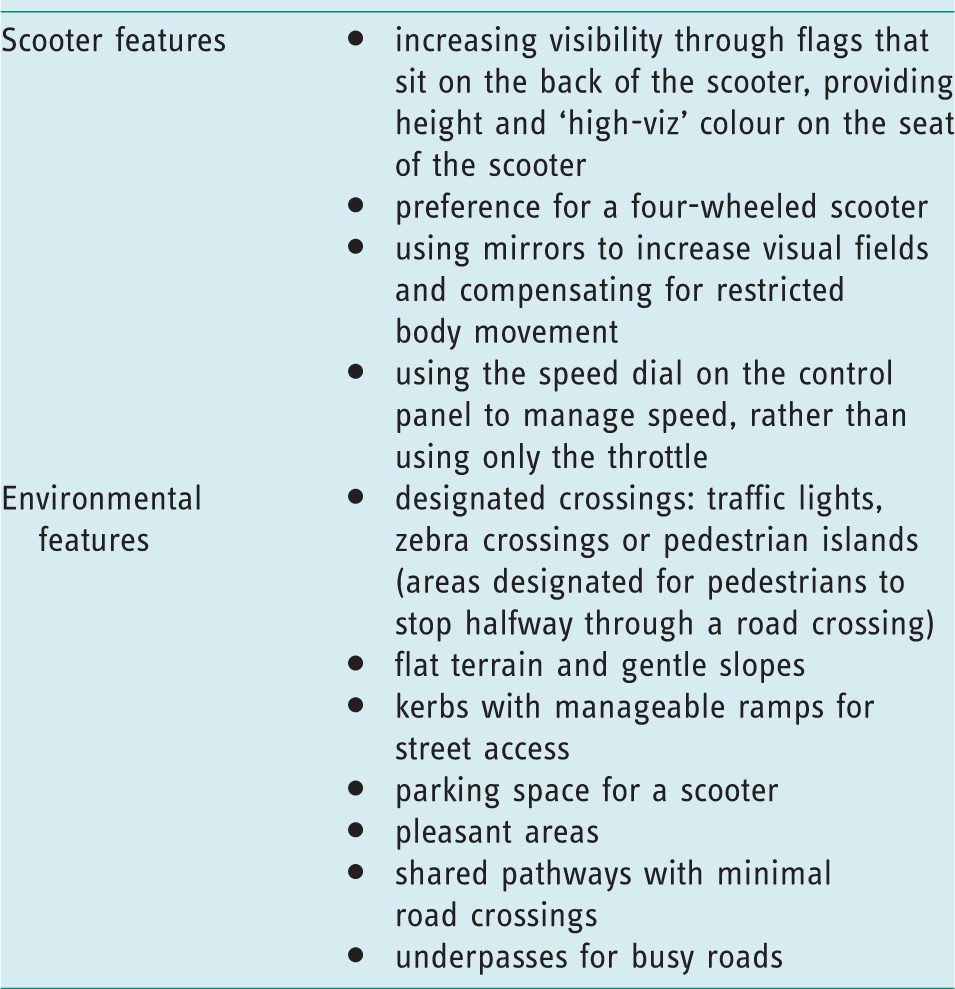
The participants indicated that the presenting risks and barriers described above could be managed through maximising available safety features either with the scooter itself or environmental features. These features are presented in Table 4.
Features for promoting effective scooter use.
In addition, participants described planning their routes and preparing for anticipated disruptions by carrying a mobile phone, wet weather gear and walking aides.
Taking the environment into account
All participants lived in flat neighbourhoods, but there were other
environmental differences across the sample. Some preferred a specific time
of day considering crowd or traffic flow, temperatures and better lighting.
Of the few participants who made outings at night, only Susan used her
scooter, whereas the Poppy and Flo arranged alternative transport. Poor
weather posed a risk due to discomfort, inability to see or hear adequately,
damage to the scooter, fear of an accident and risking illness: I don’t use it when it’s a very dark day. The dark days don’t like me
and I don’t like them. And always sunglasses, because the glare’s
always bad. Because [this region is] known for the glare, strong
sunshine. (Una) Even if this side stops and the other side is still coming, I stop. I
just wait. And this person usually gets angry with me, but then I
think they realise that, oh, it’s because of the other car that I
haven’t gone. (Susan)
Strategies varied across the sample. Some would not use their scooters inside shops, whereas others were comfortable doing so; Leonard was happy to cross the road without a designated crossing, which others avoided; Poppy assessed that a poorly maintained footpath was riskier than travelling on the road.
Taking the visual impairment into account
When asked about their vision and scooter use, most participants felt capable. Eight participants felt either their vision did not affect their scooter use or struggled to articulate the effect. The following examples demonstrate how vision loss could influence scooter use.
Clint and Evelyn had the most obvious strategy for managing vision loss.
Evelyn, the sighted partner, drove her scooter ahead of Clint to guide him
as he could see as far as her scooter in front. William, who could only see
about five metres ahead, memorised his route, listened for traffic and
pedestrians, and then drove blindly through an underpass. Thomas, who could
see about four metres ahead, restricted his scooter use to where he was
confident. Frances, with hemianopia, identified the lack of vision on her left: One of the things I’ve got to watch is people coming out of drives,
and it depends which side of the road I’m on. If I’m next to the
houses [on the right], that’s no problem, but if I’m on this side of
the road and I’m not seeing the drive, I’ve got to watch carefully.
(Frances) Everything is what I would call two-dimensional, so I knew there was
gutters and things like that, but everything was dead flat to me…
But my brain could work out that when you saw a change of colour or
a change of texture, you knew that there was probably going to be a
drop there, so it’s just a matter of getting used to that. And a lot
of the footpaths are in very, very bad repair, so it does put some
streets out altogether. (Poppy)
Attitudinal strategies for managing associated risks
As risks and barriers occurred within the social environment, participants described how they managed such risks through their personal attitudes toward other footpath users and in how they drove their scooter.
Generally, participants described a simple courtesy or a patient attitude to others. However, Poppy recognised that this was not common to all: ‘I do know some scooter users that I would consider a risk to other people. That is because of their aggressive attitude when they’re driving’. Participants demonstrated etiquette by slowing down near pedestrians and either not overtaking or calling out beforehand. However, etiquette was not always reciprocated and participants spoke of the difficulty of sharing a footpath with pedestrians who were distracted by their mobile phones, not looking, wearing headphones or exiting shops too quickly.
May, who was acutely aware of discrimination toward scooter users, explained
her approach was to normalise the use of her scooter: I don’t want to [have a flag]. I want to blend in and be nothing. I
would hate to see cycle helmets come in. That’s me personally. I
just like to be anonymous on my scooter and just blend, so I don’t
like things that make you stand out. But I’m aware of those things.
(May)
Discussion
Key results
Insights provided by the participants reveal how self-regulation allows effective mobility and key areas for further investigation and action.
The self-regulation practices described in this study fit with Donorfio et al.’s (2008) and Laliberte Rudman et al.’s (2006) theories of driving self-regulation. This involves ongoing decision-making process accounting for risks, barriers and needs, while adjusting behaviour to suit the particular situation.
When looking at the need for self-regulation by IVI who use scooters, many of the barriers are similar to those experienced by IVI as pedestrians. These barriers include poorly maintained footpath infrastructure, difficult road crossings and the threat of embarrassment (Blaylock et al., 2015; Brouwer et al., 2008; Gallagher et al., 2011; Laliberte Rudman et al., 2016; McGrath et al., 2017; Montarzino et al., 2007). The need to improve community mobility conditions seems obvious, and is also supported by a range of other studies into the experiences of pedestrians with visual impairment, powered mobility device users and older pedestrians (Blaylock et al., 2015; Brouwer et al., 2008; Fomiatti et al., 2014; Gallagher et al., 2011; Laliberte Rudman et al., 2016; McGrath et al., 2017; May et al., 2010; Montarzino et al., 2007; Mortenson et al., 2015; Wilton and Davey, 2007).
At a personal level, IVI can be affected by decreased motivation, and a loss of confidence and resilience (Laliberte Rudman et al., 2016). In addition, overall mobility for IVI can be affected by perceived risk and the need to ask for assistance (Brouwer et al., 2008; Laliberte Rudman and Durdle, 2008; McGrath et al., 2017). Participants in this study responded to all these issues in ways that demonstrated initiative and resilience.
A common experience for the participants was difficulty with the urban physical environment. The environmental production of disability is a key area for occupational therapy intervention through advocating for physical and social changes at a societal level, not focusing solely on individual remedial approaches to intervention (McGrath et al., 2016). For example, footpath maintenance and design improvements can mitigate the physical access issues listed in Table 3 and, when employed with universal design principles, improve access for a wide range of people, not just IVI who use scooters.
In this study, identified barriers in the environment included both social and physical elements. The social environmental barriers include attitudes, poor consideration of other footpath users and institutional systems that do not consider diverse mobility needs (Hamraie, 2013). Scooter users can feel judged when they have invisible mobility impairments and onlookers may not understand the use of a scooter for energy conservation, pain or the inability to walk independently (Fomiatti et al., 2014). Ripat et al. (2018) found that wheelchair users experience negative social attitudes and any campaign to label the scooter as a disability tool carries the risk of similar stereotyping. As Stowe and Mulley (2010) suggested, media can play a role in improving attitudes toward scooters users by reporting the positive elements of scooter use, and occupational therapists can provide such positive stories.
Cordes et al. (2018) indicate there are many factors that need to be considered when determining competent scooter use. The participants in this study represented a wide range of functioning, both visual and in terms of other disabilities such as hearing and overall capacity. A key finding is that personal awareness of the impact of the visual impairment allows for better self-regulation. For example, two participants with low depth perception had very different management strategies. Poppy took the impairment into account and travelled defensively, whereas Chiconne learned gradually through making mistakes.
An important contribution made by this study is the documentation of specific self-regulation strategies of scooter users. Tables 3 and 4 describe both risks and features for promoting effective scooter use, along with detailed strategies, and these can be used to influence infrastructural design and encourage public campaigns. They could also be incorporated into scooter training programmes and support evidence-based practice for any clinician who works with an IVI who uses a scooter, empowering the client with self-awareness and practical approaches to managing hazards.
Limitations and further research
The sample for this study consists of participants from geographically similar locations, which affects the study’s generalisability to other locations and a larger population. However, many of the findings describe ubiquitous risks and barriers, and practical strategies that could be trialled in many locations or with many scooter users, meaning that application of the findings is at the reader’s discretion. As with an interpretivist viewpoint, the findings are presented as details but with an understanding of multiple realities. Therefore, the findings are not presented as definitive; rather, they encourage an ongoing conversation and suggest further research into effective scooter use by IVI.
One limitation of the study was the lack of measurement of whether self-management strategies used by these participants actually improved overall safety. However, such an evaluation is a challenge that other studies detailing driving self-regulation strategies also struggle to measure (Molnar et al., 2015). Until such a study is undertaken, it must be assumed that scooter users (along with other road users) have enough insight to know how and whether self-regulation strategies improve their safety.
Further research evaluating the risks associated with scooter use are needed. Currently, scooter injury statistics are inconsistently recorded and so there is a lack of baseline measures such as how many scooter users/journeys there are in NZ (Lieswyn et al., 2017). A comprehensive risk evaluation would also compare the risk of scooter-related injury to risk of social isolation, poverty or other harmful states for which the scooter can compensate. Such an evaluation can support further research that assesses whether self-regulation is satisfactory or at what point formal interventions are warranted for promoting safer environments.
Implications for practice
This study provides a small, but significant, addition to the growing literature from occupational therapists involved in scooter research.
Occupational therapists have a role in promoting community mobility by advocating at institutional levels, such as central and local government, for the built environment to be accessible (di Stefano et al., 2012). This study provides valuable descriptions of footpath infrastructure that promotes or reduces accessibility for IVI who use scooters.
Current scooter training is often ad-hoc and community initiated. Occupational therapists can have a role advocating for and/or advising community-led scooter training and scooter clubs. The occupational therapy perspective of the interaction between the person’s capability, the occupation’s features and the environmental demands is valuable for community groups wanting to promote effective community mobility training. This study specifically highlights barriers and risks of scooter use by IVI and the self-management strategies to be incorporated into scooter education.
While scooter assessment and provision are yet to be established as a common scope of practice for occupational therapists, any research detailing scooter use supports the emerging practice. This study’s insights can support an occupational therapist working in any capacity with a client who has a visual impairment and uses a scooter. As Deverell (2011) found, some professionals working with IVI actively deter clients from using a scooter. This study provides a more positive approach, with evidence of proficient scooter use by IVI and self-regulation practice. Risk-averse perspectives are clearly apparent in research on visual impairment, and this study presents a pragmatic view of how to manage risk without unnecessarily limiting an individual’s agency. Such evidence is needed for practitioners to promote an activity that is perceived as risky (Laliberte Rudman et al., 2016).
Occupational therapists can empower their clients by ensuring they are aware of the influence of their visual impairment on general function. They can also facilitate appropriate scooter use by highlighting both the value and the known risks. It is important to provide education about management strategies in order to support and foster the client’s own capacity for self-regulation. In any adult learning situation, it is important to start where the person is. In the case of scooter users, there is obviously a huge variety of starting places.
Conclusion
Compiling the self-regulatory practices of IVI who use scooters for mobility allows understanding of personal capabilities and needs. Such understanding can empower current and future scooter users by raising awareness of risks and barriers, and by providing knowledge of various approaches that can overcome the apparent hazards. The identification of environmental demands also allows for better infrastructure planning and provides roles for occupational therapists to advocate for those planning to use scooters and to provide factual information about the barriers. Occupational therapists can also support community organisations who provide non-mandatory scooter training.
Mobility is an intricate practice, and the nuances of a seemingly simple trip to the shop is actually a multifaceted experience with many invisible elements to consider. This study provided the unique perspectives of IVI who use scooters.
Key findings
Many features pose barriers or risks for IVI when they use their scooter.
It is important to promote the maintenance and adaptation of the environment to meet the mobility needs of diverse communities. IVI can undertake many strategies to ensure effective community mobility.
Occupational therapists have a role in advocating for accessible environments, consulting on scooter training programmes and educating their clients with visual impairment who use a scooter.
What the study has added
This study has provided a detailed compilation of barriers and risks as perceived by IVI who use scooters, and their corresponding self-regulation strategies for managing these barriers and risks.
Footnotes
Research ethics
Ethical approval was obtained from the Otago Polytechnic Ethics Committee reference number 718 on 12th April 2017.
Consent
All participants provided written informed consent to be interviewed for the study.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research project: a grant from Lighthouse Vision Trust, New Zealand.
Contributorship
Keri McMullan was the lead researcher on this project, with close supervision and contributing analysis from Mary Butler across all aspects of the research. Keri McMullan wrote the first draft of the manuscript. Both authors reviewed and edited the manuscript and approved the final version.