
Abstract
Introduction
Cognitive stimulation therapy is an evidence-based group intervention for promoting cognition and quality of life in people with dementia. This New Zealand study aimed to describe and measure the ‘switch-on’ effect, a recently reported benefit involving enhanced participation.
Method
A convergent parallel mixed methods design was implemented. Interviews guided by qualitative descriptive methodology were conducted with four community-dwelling men with mild dementia and their wives, before, during and after cognitive stimulation therapy. Concomitantly, participants with dementia were scored on the Volitional Questionnaire following a single-subject A–B design. Qualitative and quantitative data were analysed using NVivo-assisted thematic analysis and descriptive statistics respectively and conjointly.
Findings
‘Switch-on’ was found to be multi-dimensional in nature, with increased engagement and expanded scope in Doing, Feeling, Relating, and Thinking and Reflecting. ‘Switch-on’ occurred with a noticeable onset within 3 weeks, which was sustained and consolidated towards completion of cognitive stimulation therapy in both group and home environments. Three men showed concurrent improvements on the achievement sub-scale of the Volitional Questionnaire. However, the measure did not effectively capture ‘switch-on’ due to its ceiling effect.
Conclusion
Findings about ‘switch-on’ suggest broader, under-researched benefits of cognitive stimulation therapy that merit further exploration from an occupational therapy perspective.
Keywords
Introduction
Occupational therapists are making valuable contributions to the research, training, promotion and delivery of cognitive stimulation therapy (CST) (Murray et al., 2016; Streater et al., 2017; Yuill and Hollis, 2011), which is an activity-based social group for people with mild to moderate dementia. The embedded principles of CST, ‘respectfulness of individuality, recognition of capacity for self-determination, encouragement of participation in meaningful activities, and optimization of overall well-being’ (Yuill and Hollis, 2011: 168), are congruent with the philosophy, values and practice of occupational therapy. While there is mounting evidence that it improves cognitive function, no study has satisfactorily investigated the occupational benefits of CST. That knowledge gap puts occupational therapists’ involvement into question. However, the recently reported ‘switch-on’ effect of CST is described in occupational terms, including enhanced capabilities and social participation (Cheung and Peri, 2014; Spector et al., 2011). A fuller explanation of the effect will be provided in the Background. This paper reports an exploratory mixed methods study of ‘switch-on’ and how it might be measured.
Background
CST is one of the few evidence-based, non-pharmacological interventions for people with mild to moderate dementia (Spector et al., 2003; Woods et al., 2012). CST falls into the category of cognitive stimulation for people with dementia that aims at ‘general enhancement of cognitive and social functioning’ through engagement with a variety of activities and discussions, usually in a small group setting (Woods et al., 2012: 3). CST has potential for use alongside a reablement approach that aims to alleviate the functional impact of dementia on people’s lives. Indeed, Poulos et al. (2017: 452) state, ‘interventions providing opportunities for social interaction, general stimulation, or other pleasurable activities can be applied alongside reablement’.
CST offers a manualized, 7-week, twice-weekly group programme of themed, enjoyable activities and discussions, the contents including physical, number and word games, ‘childhood’, ‘sounds’, ‘food’, ‘current events’, ‘being creative’, ‘using memory’ and so on (Spector et al., 2005: 5). CST is delivered in a supportive environment designed to optimize cognitive and social performance. Originally developed in the United Kingdom, CST has been applied and researched worldwide, including in New Zealand (Cheung and Peri, 2014).
CST targets global stimulation of cognition and was primarily devised based on two precedent psychosocial interventions for people with dementia (Spector et al., 2001), Reality Orientation (Spector et al., 2000), and a French version of cognitive stimulation (Breuil et al., 1994). CST developers extracted the technique of repeatedly presenting orientation information to enhance memory from Reality Orientation; they then transformed its rigid and insensitive style into a person-centred programme (Spector et al., 2001). Following Breuil et al.’s (1994) cognitive stimulation, CST taps into implicit memory and implicit learning, relatively well-preserved realms of cognitive function in people with dementia (American Psychiatric Association, 2013); however, it was adapted into a light-hearted, non-threatening delivery from its original clinical approach (Spector et al., 2001).
A wealth of quantitative studies, including randomized controlled trials, have examined specific cognitive domains and discrete outcome areas for people who attended CST (Hall et al., 2013; Piras et al., 2017; Spector et al., 2003, 2010). The evidence generated demonstrates that CST promotes cognitive function, particularly language, memory and orientation, and self-rated quality of life for people with mild to moderate dementia (Hall et al., 2013; Piras et al., 2017; Spector et al., 2003; Woods et al., 2012). An earlier study found that improved subjective quality of life following CST was mediated by improved cognition and reduced depression (Woods et al., 2006). However, no further research has explored the therapeutic effects on cognition, mood and quality of life using a more dynamic or holistic approach.
Only five qualitative and mixed methods studies have hitherto explored the broader benefits of CST, two of which described ‘switch-on’ as a favourable outcome (Cheung and Peri, 2014; Spector et al., 2011). ‘Switch-on’ comprised a cluster of positive behavioural changes noted in some CST attendees that were consistent with the confirmed benefits of CST in quantitative research (Spector et al., 2010; Woods et al., 2012). Changes included ‘a sense of being more switched on or wanting to attend to things more’ (Spector et al., 2011: 948), and having ‘new-found confidence, capabilities and vastly improved communication skills’ (Cheung and Peri, 2014: 7).
Of note, the term ‘switch-on’ seems to reflect an observer’s standpoint in representing the changes, which may not be viewed as dementia friendly. An equivalent, more subjective label for the effect used by participants with dementia in Cheung and Peri’s (2014) study was ‘stimulation’ or ‘feeling stimulated’ (21).
Spector et al. (2011) associated ‘switch-on’ with improved concentration and alertness, which are commonly reported cognitive benefits of CST, whereas Cheung and Peri (2014) regarded it as a more satisfying outcome of social engagement, a non-specific therapeutic element of participation in CST. While the nature and scope of the effect have not yet been clearly delineated, three further studies using a qualitative or mixed methods design have described similar positive changes (Bailey et al., 2017; Kelly et al., 2017; Murray et al., 2016). This suggests that ‘switch-on’ might be a common but less recognized benefit of CST.
The observed behavioural change of ‘wanting to’ pay more attention to things and having enhanced confidence and capabilities suggests a volitional component to the ‘switch-on’ effect. This is an important possibility to explore because apathy or lack of motivation is the most prevalent behavioural symptom in people with Alzheimer’s type dementia (Dyer et al., 2018). Recent research in cognitive neuroscience, psychology and ageing has also found some evidence of interactions between motivation and cognition (Braver et al., 2014). Despite that, no study has yet explored the impact of CST, a cognitive intervention, on the person’s motivation or volition, as indicated in the existing knowledge of ‘switch-on’.
That research gap indicated the need for a more complete understanding of the therapeutic outcomes of CST, including the ‘switch-on’ effect, from a holistic, occupational perspective (Law et al., 1996; Taylor, 2017; Townsend and Polatajko, 2007). The limited knowledge about ‘switch-on’ required an inductive qualitative research approach to obtain a ‘thick’ description about the effect. To examine the hypothetical correlation between volition and ‘switch-on’, an occupation-focused measure of volition, the Volitional Questionnaire (VQ) (de las Heras et al., 2007), was selected. Three research questions were formulated:
What is the nature of the ‘switch-on’ effect as described by people attending CST and their family or caregivers? At what time-points during and after the group is the ‘switch-on’ effect reported? Are the changes described as the ‘switch-on’ effect measurable using the VQ?
Method
Study design
A convergent parallel mixed methods design (Creswell, 2014) merging qualitative descriptive methodology (Stanley, 2015) and a single-subject A–B design (Carter and Lubinsky, 2015) was implemented. Driven by the single-subject design, qualitative and quantitative data were collected concomitantly at participants’ homes at three time-points: before commencement of CST (time 1); during the third week of CST (time 2) and within a week after completion of CST (time 3). Quantitative and qualitative data were analysed using their respective analytic methods separately and then conjointly. Considering the scant knowledge about ‘switch-on’, more weight was placed on the qualitative component of the study.
Ethics approval was obtained for the study from the Auckland University of Technology Ethics Committee in 2016 (reference number 16/396).
Measures
The Volitional Questionnaire (de las Heras et al., 2007) was selected as a possible measure of ‘switch-on’ because of its theoretical foundation in the Model of Human Occupation (Taylor, 2017) and the alignment observed between most items in the measure and the descriptions about ‘switch-on’ in CST literature. The instrument has good construct validity, internal validity and intra-rater reliability (Chern et al., 1996; Li and Kielhofner, 2004).
The Addenbrooke’s Cognitive Examination – III (ACE-III) is a commonly used neuropsychological test with sound psychometric properties for screening cognitive impairment and dementia diagnosis (Hsieh et al., 2013). The ACE-III was used in this study for estimating cognitive function and severity of dementia of the participants with dementia.
Service delivery context of the study
CST is a best-practice example in the national Framework for Dementia Care in New Zealand (Ministry of Health, 2013). CST is delivered in a variety of settings, including the public health system, non-government community organizations, dementia day care centres and aged care residential facilities. Like most health and disability services in New Zealand, CST is government-funded and accessible for people with dementia free of charge.
CST group and participant recruitment
Research participants were people with mild to moderate dementia who attended a standard CST programme and/or their associated family member or caregiver. Dementia Auckland, a non-government community organization that offers CST to people with dementia in the greater Auckland area, was identified and approached as a suitable CST provider for the study. The staff involved in delivering CST were provided with a full briefing about the study design and aims prior to recruiting four men with mild dementia and their wives from a CST group run between 27 March 2017 and 11 May 2017. The staff explained the research project to people with dementia and their family who met the inclusion criteria. Their verbal consent was obtained to forward contact details to the researcher. Six people with dementia and five family members expressed interest and four couples were finally recruited to the study. Facilitation of the programme closely followed the CST manual (Spector et al., 2005), which allows some flexibility in the choice of activities in response to the specific programme participants. All participants provided written informed consent for participating in the research. None of the study authors were involved in running the CST group.
Data collection
All data were gathered by the first author. The demographic information of participants with dementia, including age, ethnicity, education, past occupations and relationship with their caregiver, was collected at first contact. Qualitative data collection involved conducting semi-structured interviews of the eight participants at the three time-points, using the same set of open-ended questions. These explored the men’s engagement with daily activities, including their interests, routines, feelings, concentration and communication with others. For example, ‘What are some of the things you have been doing over the last month?’ ‘How do you spend your time on a typical day?’ and ‘Have you noticed any changes?’ Questions to family members were framed in relation to their observation of their spouse. Participant recall was supported by conducting interviews in their own homes, where there were familiar objects to prompt memories of activities. Most interviews were conducted separately, to encourage those with dementia to express their views fully rather than deferring to their spouse. However, there were a few interviews involving both husband and wife, who supported recall. In these cases, focus on the intended interviewees was maintained. All 24 interviews were digitally audiotaped and transcribed verbatim by professional transcribers.
Quantitative data collection consisted of administering the ACE-III at time 1 and the VQ at the three time-points. Following the single-subject A–B design (Carter and Lubinsky, 2015), each participant with dementia was observed while carrying out two daily activities of their choice at home and rated on the VQ before, during and after the CST programme, with time 1 being baseline (phase A) and times 2 and 3 being post-intervention measures (phases B1 and B2).
Data analysis
The qualitative data analysis was primarily conducted by the first author, with the second and third authors involved in peer review of analytic decisions. Data were analysed using open coding and thematic analysis (Stanley, 2015) manually and electronically in NVivo 11 Pro (QSR International, 2015). The outcome of the qualitative analysis was a coding matrix, with three ‘columns’ representing the three time-points and four ‘rows’ categorizing four thematic areas, Doing, Feeling, Relating, and Thinking and Reflecting. Similar codes were grouped and collapsed and eventually merged into three sub-themes for each matrix cell. Descriptive statistics and visual analysis (Vogt, 2014) were applied to calculate and present the VQ measurement results over the three time-points. Qualitative and quantitative data were further converged and analysed together in relation to the three research questions (Creswell, 2014).
Rigour
A main strength of the study design was the repeated interviews with both people with dementia and their family caregivers. Extended engagement and triangulation of the men’s and their wives’ perspectives enhance the credibility and confirmability of the study outcomes (Guba and Lincoln, 1982).
The VQ is a technical, interactive, observational measure that can be administered easily in any setting (de las Heras et al., 2007). These features make the measure suitable for use in a single-subject design as a consideration of rigour (Carter and Lubinsky, 2015).
The convergent parallel mixed methods design of the study aimed to optimize rigour and trustworthiness of its qualitative and quantitative components. The rich qualitative data compensated for the limitations of the A–B design, such as lacking repeated baseline measurements and not addressing confounding factors following treatment. Measurements using the VQ served as a triangulation strategy to strengthen the credibility and objectivity of the qualitative findings.
Findings
Table 1 shows the demographic information and the ACE-III scores of the participants with dementia, using pseudonyms. They were males aged 69 to 82 years and had backgrounds in engineering and construction.
Demographics of participants with dementia and the Addenbrooke’s Cognitive Examination – III (ACE-III) scores.

Nature of ‘switch-on’
Table 2 displays the sub-themes that were identified from thematic analysis of the interview data in a coding matrix.
The coding matrix and sub-themes for describing ‘switch-on’.
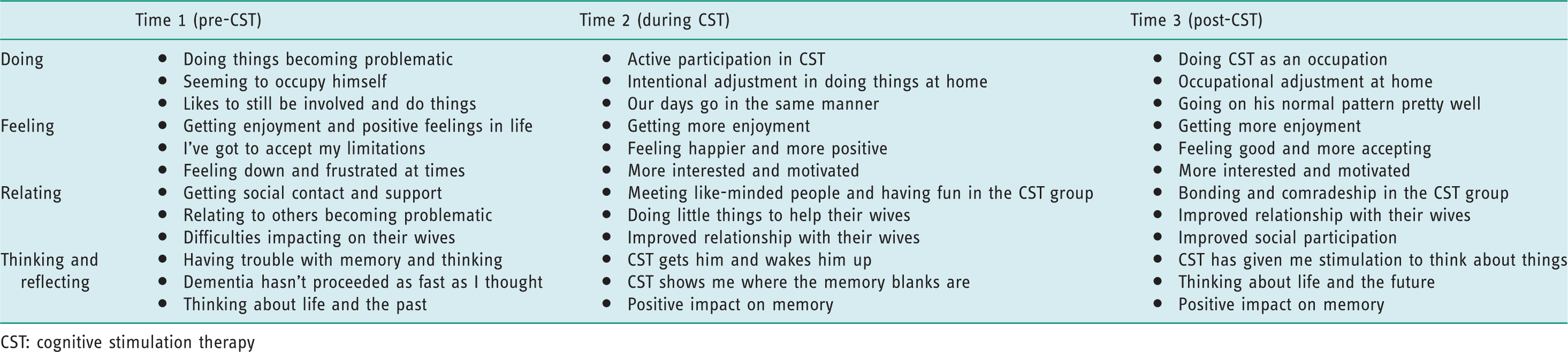
CST: cognitive stimulation therapy
Doing
A marked common change in Doing at times 2 and 3 was that all participants with dementia were ‘keen’ to attend CST and engaged with the programme actively and enthusiastically. They also started ‘talking more about stuff’, including CST, at home. The main thing that stands out is he’s so happy to go to this course and talk about it afterwards. (Frank’s wife, time 2) When he goes to these sessions, he gets goals, like things to do, and he busies himself with that. He gets stuck in and spends hours like doing the last one he did and that was on current events and he went into it with great guns, and to present his little speech! (John’s wife, time 2) I’m taking less responsibility [for our finances] because Ann [wife] is doing so much more. … But I actually probably do a little bit more around the house. … if she [wife] wanted any help, she’d ask for it. Now she doesn’t have to, I just go and do it. (Frank, time 3)
Feeling
Changes in feelings were similarly reported at times 2 and 3 by all participants with dementia, characterized by increased experience and expression of positive emotions. These positive emotions included getting more enjoyment from, and feeling more interested in and motivated to participate in, occupations, having a sense of achievement and satisfaction from participation, becoming more positive, confident and accepting of living with dementia, and showing more appreciation and consideration towards their wives. When I come away, I always feel good, had a good time. I look forward to going to it. (Frank, time 2) I am enjoying life, I am really enjoying, even liking watching that … making a 3D pack. I’ve done three 3D puzzles, and they are quite stimulating. They’re not very hard to do but I get a bit of enjoyment out of it. (Peter, time 3) He is accepting things better and understanding things better, not to be selfish … and demanding. (Mark’s wife, time 3)
Relating
All participants with dementia developed a sense of ‘comradeship’ and bonding with the ‘like-minded’ peers in the CST group, which was apparent at time 2 and strengthened towards time 3. We accept it [dementia]. We try [to] sort of improve on it, it doesn’t worry us. It’s been interesting being with a group of like-minded people, because that’s what we are. (Frank, time 2) The stimulation really comes from the group, and it’s what they bring to and from each other that does the stimulating. … You can’t make things stimulating if the people aren’t stimulated within themselves and get the comradeship that you feel for one another. … You feel for each other ’cos you know you’re in the same boat. (John, time 3) I feel sorry for my wife ’cos [she] only do it for me. And I said, ‘that’s my job, I was told to do it, so I have to do it myself’. (Mark, time 3) I’ve noticed that there’s still that being very self-centred, but since I think he’s done this course, it has expanded it and that if he sees I’m struggling, he’ll get up and do something whereas before he wouldn’t. (Peter’s wife, time 3) [He] gave me a hug and that’s unusual. Sometimes I’ve tried to hug him and there was this rigid thing there, like hugging a lamp post, he was not willing to give. But he had a lovely hug! (Frank’s wife, time 3) What did the girls say the other day? ‘He did something that was like the old Dad’. His personality is changing a little back to [his old self], he’s getting more [involved], he’s making jokes about things. (John’s wife, time 3)
Thinking and reflecting
An altered, more lively presentation was noted in three men at time 2, characterized as ‘waking up’ and becoming more aware of ‘what’s going on around him’. It [attending CST] didn’t excite him exactly, but it sort of gets him and it wakes him up. (John’s wife, time 2) He’s more alert in other things that he used to be slow at, like … I said to him ‘in the morning when you get up, you can go and open all our curtain[s]’ and sometimes he forgets, but lately he will remember. (Mark’s wife, time 2) So for stimulation, I’ve found it has helped because if we’ve been given a subject, it is for the next time we go. I’d have to dig into something and have a think about it. (John, time 3) Just this morning he said, … ‘when we’re settled there [retirement village], let’s just go away for a couple of days’. It’s always been me who’s suggested that, not him. Quite a few things have changed. (Frank’s wife, time 3) I start to think about some other part. I don’t know what happened, which one of us [him and his wife] gonna go, ’cos that’s life. … We die, we go to heaven and that’s the only place you go, gonna meet again. (Mark, time 3) I had a bad blank [in the CST group] in catching the ball and say name, one of your grandchildren, and absolutely nothing there at all. … I can name most of them now. … Instead of saying ‘woo, I’ve lost it’, ‘let’s find it again’. So, I went back and wrote out my family tree. (Peter, time 3)
Occurrence of ‘switch-on’
The qualitative data indicated that all participants with dementia experienced the ‘switch-on’ changes, which occurred in a gradual, advancing fashion towards completion of CST in both CST and home environments. However, each man appeared to have his own trajectory of ‘switch-on’ with varied onset, presentation and timing. Three wives were able to report a specific time range for noticing the ‘switch-on’ changes at home. It happened as soon as he started the group, right from day one. He was picking up an interest and looking for things and looking to go to the group. (Peter’s wife, time 2) Not the first week, the first week is much the same as usual but he just, quite quickly started changing really. Well he’s only been to five [sessions]. Yeah especially the last two. (John’s wife, time 2) Probably the last two weeks [of CST] I’d say, it’s been gradual, up to then there was no noticeable change. (Frank’s wife, time 3)
Measurement of ‘switch-on’
Table 3 presents means of the overall VQ scores and three sub-scores for each participant with dementia at the three time-points. Rated on a four-point scale, mean scores of the VQ and its sub-scales range from 1 to 4, with higher scores suggesting higher volition. Given the small number of participants and the single pre- and post-test assessment points, the statistical significance of the change was not calculated. The data are visually depicted using line charts in Figures 1 and 2, as recommended in a single-subject research design (Carter and Lubinsky, 2015).
Means of overall Volitional Questionnaire (VQ) scores and sub-scores for each participant at three time-points.
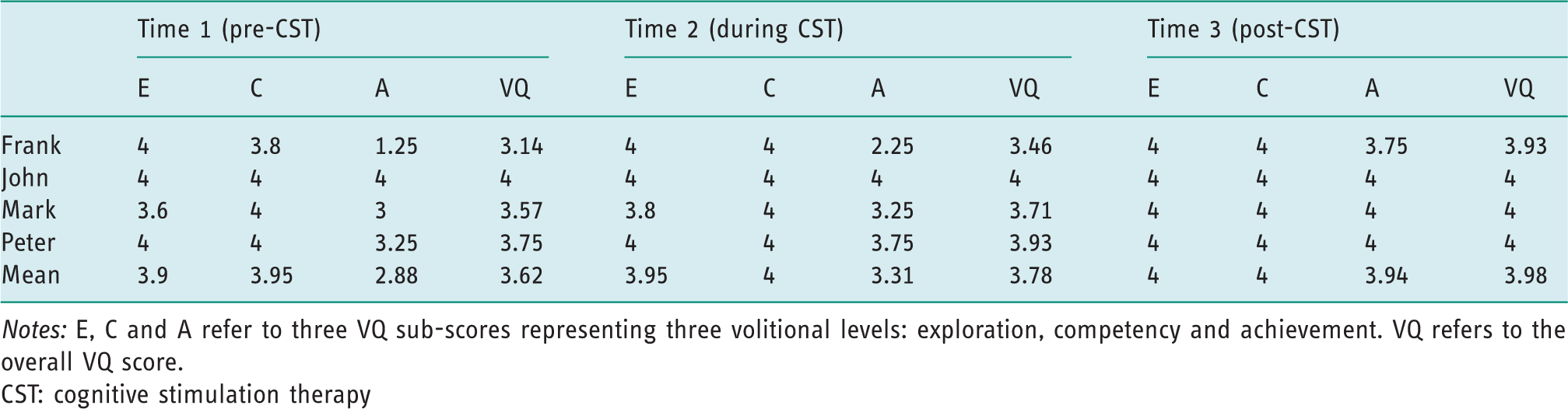
Notes: E, C and A refer to three VQ sub-scores representing three volitional levels: exploration, competency and achievement. VQ refers to the overall VQ score.
CST: cognitive stimulation therapy
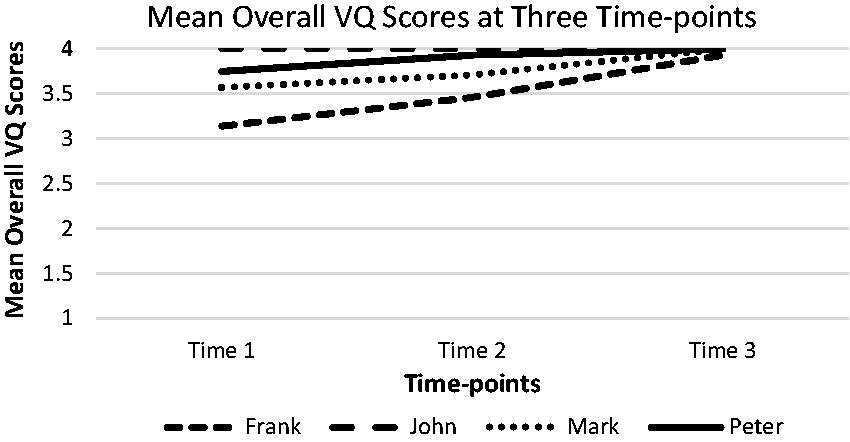
Mean overall VQ scores for each participant at three time-points.
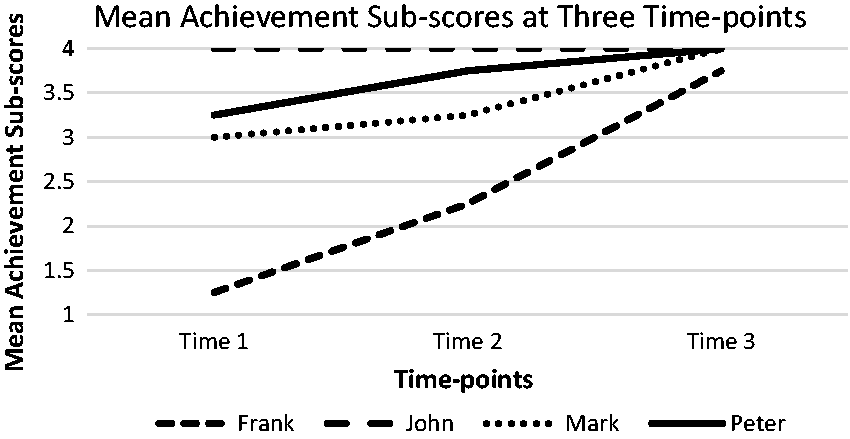
Mean achievement sub-scores for each participant at three time-points.
Figure 1 shows that all the men obtained high overall VQ scores, even at baseline. While John stayed at the maximum consistently, there was an increasing trend towards the maximal score over time for the other three participants. Figure 2 demonstrates the relatively low achievement sub-scores at baseline for three men, with a similar improving pattern after engaging in CST. This indicates that the improved overall VQ scores in three men were attributable to their improved achievement level of volition, the highest level of volition on the volitional continuum (de las Heras et al., 2007).
Discussion
The nature of ‘switch-on’ revealed in this study comprised of simultaneously enhanced activity and strength in multiple areas of Doing, Feeling, Relating, and Thinking and Reflecting. These changes were across environments, deliberate, with intentional goals, driven by positive feelings, and manifested in social and occupational contexts. Although there was individual variation, ‘switch-on’ occurred in a gradual, progressive fashion towards completion of CST in all participants with dementia. Corresponding to the qualitative data, the VQ measurements, particularly the achievement sub-scores, showed similar improvement in three men. However, the instrument failed to detect the ‘switch-on’ changes in John due to its ceiling effect (Salkind, 2010), which confines its usefulness for measuring the ‘switch-on’ effect.
These findings suggest that volitional changes were part of the ‘switch-on’ effect from participation in CST as an occupation. Volition is theorised as patterns of thoughts and feelings that inspire, propel and energize a person to participate in an occupation (Taylor, 2017). Volition consists of three relatively stable components: personal causation, values and interests, with a dynamic and cyclic volitional process of the person anticipating, choosing, experiencing and interpreting the occupations they engage in. The ‘pervasive influence’ of volition (Taylor, 2017: 52) was evident in the multi-dimensional nature of ‘switch-on’ discovered in this study, involving synchronized activation of and mutual enhancement between the four areas (Doing, Feeling, Relating, and Thinking and Reflecting) of the person. Volition was also reflected in the spatial and temporal features of the occurrence of ‘switch-on’, characterized by spontaneous transfer of the effect across environments and the gradually improving pattern of ‘switch-on’ over time. The VQ measurement data further verified the ‘switch-on’ of the higher achievement level of volition in three men, which motivated them to strive towards goals and attain internal satisfaction (de las Heras et al., 2007).
Although no previous study has explicitly examined the volitional benefits of CST, the ‘generalized’ effects of this cognition-oriented therapy for improving self-rated quality of life have been confirmed and discussed in quantitative studies (Spector et al., 2003, 2010; Woods et al., 2006). Further, all the earlier qualitative and mixed methods studies described expanded positive changes outside the CST environment (Bailey et al., 2017; Cheung and Peri, 2014; Kelly et al., 2017; Murray et al., 2016; Spector et al., 2011).
These findings in CST literature align with the ‘pervasiveness’ of volition and the ‘switch-on’ changes noted in this study, which signalled two implications for future research. First, more general investigations on the volitional outcomes and mechanisms of CST are needed, especially from an occupation-based theoretical perspective. Second, given the ceiling effect of the VQ and its partial measurement of the broader ‘switch-on’ effect, it would be beneficial for further study to either develop a new, specific measure for ‘switch-on’ or apply a more holistic and sensitive instrument for measuring the effect, such as the Engagement in Meaningful Activities Survey (Goldberg et al., 2002).
Woods et al. (2006) found some evidence that the cognitive focus of CST promoted quality of life and wellbeing. In contrast, Cheung and Peri (2014), who first named ‘the switch-on phenomenon’, emphasized the therapeutic value of the non-specific aspect of social engagement in CST groups. The present study, using occupational frameworks (Law et al., 1996; Townsend and Polatajko, 2007), suggests that ‘switch-on’ is an outcome of the transactional dynamics occurring between the person, environments and occupations throughout the course of CST. An example was the reciprocal ‘stimulation’ that attendees brought ‘to and from each other’ through engagement with CST in the group setting. Further, some qualitative data in Relating, such as meeting the ‘like-minded’ people, being ‘in the same boat’ and developing bonds and ‘comradeship’ in CST, suggested the sub-culture in CST was a therapeutic element. This has not been explicitly identified in CST literature previously, although Dugmore et al. (2015: 964) recognized ‘peer identification, support and membership’ as one of five common ‘active mechanisms’ that could make a psychosocial intervention ‘work’.
The sub-cultural element of CST and its contribution to the positive outcomes of the intervention, including ‘switch-on’, may require further exploration. A possible implication could be placing more emphasis on the social and cultural connections between CST group members in maintenance CST programmes and even working towards building an ongoing post-CST community for people with dementia.
Limitations
This was a small-scale study that involved only four community-dwelling couples from the same CST group. The four participants with dementia had several commonalities, including being male, married, living with a wife who was the main caregiver, and having a similar interest or background in engineering, technology or construction. Demographic information about their wives was not collected, but it may have influenced their perceptions of their husbands’ experiences. The lack of variety in participant characteristics in this study limits the transferability of the findings.
Further, the current study rendered a ‘thick’ description about ‘switch-on’ with ‘low-inference’ interpretation (Sandelowski, 2000: 335). However, it was not designed to explore deep meaning or lived experience of ‘switch-on’ for participants with dementia. Neither did the study intend to examine the active mechanisms that underlie ‘switch-on’, the internal dynamic relations between the ‘switched-on’ areas, or the exact timing of its occurrence.
In addition, there were several limitations related to the VQ measurement. The VQ was administered by the researcher rather than an independent rater, which might have resulted in observer bias, affecting the rigour of the study. Due to its opportunistic recruitment, the study did not achieve multiple baseline measurements as recommended for a single-subject A–B design (Carter and Lubinsky, 2015). The measure showed a ceiling effect due to its psychometric weakness in differentiating higher levels of volition (Chern et al., 1996).
Conclusion
This was the first study that explored the ‘switch-on’ effect of CST using a parallel convergent mixed methods design and incorporating an occupation-based perspective. The findings of the study indicated that ‘switch-on’ was multi-dimensional in nature, consisting of simultaneous positive changes in the areas of Doing, Feeling, Relating, and Thinking and Reflecting. The ‘switch-on’ changes occurred synchronously in both CST and home environments, with incremental improvement towards completion of CST. Concurrent with the ‘switch-on’ descriptions were the improving trend of the VQ scores, particularly on the achievement sub-scale, in three of the participants with dementia. Although the instrument was deemed to not effectively capture ‘switch-on’, this was the first study that measured the impact of CST on volition. The evidence from the present study suggests that the ‘switch-on’ effect could be a desirable outcome of occupational participation in CST, which warrants further investigation. Other indicated areas that deserve more research in the future are the volitional benefits and the therapeutic value of CST for a sub-cultural group for people with dementia.
Key findings
‘Switch-on’ involved enhanced engagement in Doing, Feeling, Relating, and Thinking and Reflecting, which occurred in an incremental fashion. Three participants with dementia showed improvement on the achievement sub-scale of the VQ.
What the study has added
This study provided a more comprehensive understanding of the ‘switch-on’ effect, a positive and little-known outcome of CST from an occupation-based theoretical perspective.
Footnotes
Acknowledgements
The authors thank Rhonda Preston-Jones, Barbara Fox, Nicola Brenton, Zhi Chen, Lynn Hubbert and Maria Co from Dementia Auckland, who provided the cognitive stimulation therapy programme and assisted with recruitment of the research participants. Dr Gary Cheung is acknowledged for mentoring the research project in guiding the ethics approval application and selection of the cognitive screening tool for the study.
Research ethics
Ethical approval was obtained from the Auckland University of Technology Ethics Committee in 2016 (reference number 16/396).
Consent
All participants provided written informed consent to be interviewed for the study. All participants with dementia provided written informed consent to complete the selected measures for the study.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The first author disclosed receipt of the Occupational Therapy Innovation, Learning and Development Fund for post-graduate study from her employer, Auckland District Health Board, towards completion of this research, which was undertaken in partial fulfilment of the requirements of a Master of Health Science degree from Auckland University of Technology.
Contributorship
All authors contributed to development of the research proposal, methodology, design and application for ethical approval. Qi Liu, under the supervision of Margaret Jones and Clare Hocking, researched the literature and collected the data. All authors contributed to interpretation of the data. Qi Liu drafted the manuscript. All authors reviewed and edited the manuscript and approved the final version.