
Abstract
Introduction
This study explored the impact of HIV on the functional recovery of personal activities of daily living of stroke survivors. This assisted in identifying possible implications for the rehabilitation of stroke survivors who are also HIV-positive.
Method
A quantitative, descriptive, longitudinal comparative research design was used to determine the change in personal activities of daily living scores of HIV-negative and HIV-positive stroke survivors from admission to 1 month after discharge. Data were collected at a rehabilitation unit using the South African Database Functional Measure.
Results
There was no difference in the rate and nature of functional recovery of personal activities of daily living between the two groups between admission and discharge. A difference was noticed during the period from admission to 1 month after discharge, during which the HIV-negative group continued to show improvement, while the HIV-positive group showed little improvement or a decline in personal activities of daily living scores.
Conclusions
While the rate and nature of functional recovery related to personal activities of daily living for HIV-positive and HIV-negative stroke survivors is similar during inpatient care, discharge planning for the HIV-positive group needs to consider the decline in personal activities of daily living functioning post discharge. Regular follow-ups and the inclusion of the stroke survivors in an outpatient treatment programme is recommended.
Introduction
Stroke is the second leading cause of death worldwide, and the leading cause of acquired disability, with up to 50% of survivors being chronically disabled (Donkor, 2018). Low to middle income countries (LMIC), such as South Africa, account for higher stroke mortality (85%) and higher Disability-Adjusted Life Year (DALY) (80%) (Donkor, 2018; Sajjad et al., 2013).
Although the burden of stroke in younger adults is increasing globally, a disproportionate burden is seen in LMIC countries. In South Africa the average age of stroke survivors is between 45 and 49 years for both men and woman, while in developed countries the average age of stroke survivors is 70 years in men and 75 years in women (Maredza et al., 2015). An investigation into the aetiology of stroke in patients younger than 45 years found that in Africa, stroke in this group is usually associated with Human Immunodeficiency Virus (HIV) infection (Singer et al., 2013). This risk for stroke in individuals living with HIV is increased both by the condition and the antiretroviral therapy (ART) used to treat the condition (Bogorodskaya et al., 2019).
South Africa has a high prevalence of HIV, resulting in 7.7 million of the population and 20.4% of adults (15–49 years) living with HIV (UNAIDS, 2018). Thus, occupational therapists working in South Africa and other LMIC countries with high HIV prevalence rates should take cognisance of the implications of differences in aetiology, age, illness progression and prognosis in stroke survivors (Wolf et al., 2009). They should also critically review the focus of occupational therapy on improving a stroke survivor’s independence. In addition, the patient’s ability to participate in personal activities of daily living (pADL) in relation to the recovery that can be expected in terms of these factors should be considerd (American Association of Occupational Therapy, 2014; Hartman-Maeir et al., 2007). This is especially important as hospital admissions in these countries are reported to be short. The average hospital stay is between 6 and 10 days, with inconsistent follow-up and outpatient treatment (Mudzi et al., 2012; Parekh and Rhoda, 2013).
Empirical evidence is needed to understand the interactive impact of HIV status and stroke on a stroke survivor’s rate of recovery and participation in pADL in order to ensure appropriate and cost-effective service delivery. This study aimed to provide evidence for the rate and nature of recovery of pADL in HIV-positive and HIV-negative stroke survivors at a South African hospital with a small rehabilitation unit, catering for patients funded by the private and public health care sectors. The structure of this unit enabled occupational therapists to request an extended hospital stay of 4–6 weeks, until patients achieved optimal pADL outcomes. This further assisted the provision of appropriate treatment to these patients through appropriate goal-setting, caregiver training and support.
Literature review
The incidence of non-communicable diseases including hypertension, cardiovascular diseases and diabetes is a predisposing factor for stroke. These conditions have reached epidemic proportions in both rural and urban areas in LMIC countries, with an associated increase in stroke (Nojilana et al., 2016). South Africa, as an LMIC country, has a high annual incidence for stroke with a crude stroke rate of 300 per 100,000 person-years and 1070 DALYs lost owing to stroke (Connor et al., 2007; Maredza et al., 2015).
Part of these statistics also account for stroke associated with HIV, which is also endemic in South Africa. Early studies on ART-naive patients reported young adults who were HIV-positive and presenting with stroke had no cardiovascular disease or other known predisposing factors. Stroke in this population was found to be due to vasculopathy causing occlusion of arteries (Bhagavati and Choi, 2008) and aneurysmal arteriopathy (Singer et al., 2013). HIV was thus reported as an independent predictor of stroke, after controlling for demographics and traditional stroke risk factors (Owolabi and Ibrahim, 2012; Singer et al., 2013).
Although the introduction of ART reduced the incidence of opportunistic brain infections, the rate of ischaemic and haemorrhagic stroke has increased (Subsai et al., 2006) due to atherosclerotic side effects of the medication (Atadzhanov et al., 2012). Thus, while immunosuppression with ART increases the risk of stroke across all ages, the more traditional risk factors are also found in the population with HIV. It has been noted that early onset atherosclerosis may develop after 2 years of continual use of ART, with an increase in both myocardial infarctions and strokes (Singer et al., 2013).
Thus, risk factors for stroke among the HIV-positive population may differ from the unaffected population, and the effects of HIV and ARV medication must always be considered (Benjamin et al., 2012; Chow et al., 2012). It is important to understand the extent to which HIV infection contributes to the increased risk for stroke, especially in regions with high HIV prevalence, such as South Africa.
In developed countries, the median age of HIV-positive stroke survivors is 42 years, whereas the median age of HIV-positive stroke survivors in LMIC countries is 39 years. One hypothesis to explain the difference in median age of HIV-positive stroke survivors is the earlier identification of the illness and ART initiation in developed countries (Benjamin et al., 2012).
Some research suggests that there is also a relationship between the CD4 count and stroke, particularly a CD4 count that has dropped below 200 (Hogan and Wilkins, 2011) as a result of opportunistic infections such as meningitis, hepatitis C, varicella zoster virus or tuberculosis (Bertram et al., 2013; Bogorodskaya et al., 2019). Low CD4 counts and high opportunistic infection rates are commonly seen in South Africa due to late initiation of ART, as only 85% of those living with HIV know their status and of these only 71% are receiving ART (Huerga et al., 2018). While South African research is predicting a marked reduction in new HIV infections over the next 30 years, particularly in the 15–49 years age groups (Taylor and Ntusi, 2019), those living with HIV and receiving ART remain at risk of stroke. It is estimated that in the age group 50 years and older the prevalence of stroke will increase from 9% to 17% due to increased life expectancy associated with the introduction of ART (Atadzhanov et al., 2012).
While the clinical descriptions and neurological deficits of stroke survivors who are HIV-positive and HIV-negative are reported to be similar, HIV-positive stroke survivors often have atypical symptoms such as acute confusion and acute loss of consciousness (Benjamin et al., 2012). These symptoms may be associated with HIV-neurocognitive disorders (HAND), which present with varying severity in many individuals with HIV. Mild neurocognitive disorder (MND) has been linked to a decline in activities of daily living (ADL) including pADL, while HIV-associated dementia (HAD) is linked to dependence in ADL (Woods et al., 2009). HIV-neurocognitive disorders are more prevalent due to increased life expectancy (Nath et al., 2008).
The incidence of ischaemic strokes in the HIV-positive population is higher at 5.27 per 1000 people compared to 3.75 in the HIV-negative population (Singer et al., 2013). The subtypes of stroke common in the HIV-positive population include lacunar strokes, partial anterior circulation strokes and total anterior circulation strokes (Benjamin et al., 2012). While the site of lesion has been associated with recovery after stroke (Kwakkel et al., 2003), the progress in pADL over the first 6 months post stroke can be predicted from the initial results of standardised ADL assessments irrespective of site, vascular territory, comorbidities or hemisphere of the stroke (Kwakkel and Kollen, 2013; Saposnik et al., 2011).
Literature indicates that 60% of HIV-negative stroke survivors are permanently dependent in some pADL, including eating, grooming, dressing, bathing, toileting and mobility, 1 year after suffering a stroke (Hartman-Maeir et al., 2007). Although there is considerable research on change in the pADL of stroke survivors, very little information is available on the impact of HIV on the stroke survivor’s ability to achieve independence in pADL. Identifying the impact of HIV on the rate and nature of stroke recovery during inpatient rehabilitation and post discharge can assist occupational therapists to direct their goal-setting and the rehabilitation process for pADL.
Method
A quantitative, descriptive longitudinal comparative study design was used. The study determined the relationship between the rate and nature of recovery of the stroke survivors, with and without HIV.
Participants
The study population consisted of all first stroke survivors referred to occupational therapy after admission. Data were collected at the small 15-bed physical rehabilitation unit at the research site. Total population sampling was used. Of the 42 stroke survivors who were admitted to the unit over the period of 6 months, 32 agreed to participate in the study. These patients met the inclusion criteria of a first stroke and were over the age of 18 years. The stroke diagnosis was confirmed by a medical doctor at the referring hospital. The participants’ HIV status was confirmed in accordance with the national guidelines for HIV testing, including supported counselling (Department of Health, 2016) routinely provided by HIV counsellors in the unit. Stroke survivors who refused HIV testing or who had any secondary diagnosis (such as spinal cord injuries, head injuries, tumours, dementia and encephalopathy) were excluded from the study. Ethical clearance for the study was obtained from the Human Research Ethics Committee at the University of the Witwatersrand (M130934). All participants were informed of the purpose and the nature of their participation in the study and signed informed consent if they were willing to participate in the study. Confidentiality and anonymity of the participants was ensured through the use of numerical codes.
Research instruments
Data were collected using a demographic questionnaire, which included age in ranges of 10 years, gender, and employment status. Medical information was collected from the medical records including the type of stroke and any comorbidities. The information on the HIV status of the stroke survivors was accessed from the confidential section of their files with their permission.
The South African Database for Functional Measures (SADFM) BETA® scale was used to collect data relating to the stroke survivor’s ability to participate in pADL. The SADFM is an evidence-based reporting tool developed by Loubser, based on the International Classification of Functioning, Disability and Health Framework (ICF). The assessment tool was developed as a nursing measure, and is validated for use in South Africa. The tool can be used to convert patients’ functional abilities into quantifiable data, making it possible for occupational therapists to measure the improvement of patients in the sub-acute phase (Loubser et al., 2015). The BETA® scale consists of 18 items, 13 that consider physical function and five cognitive function, although the latter were not included in this study. The pADL domains assessed included eating, grooming, upper limb and lower limb dressing, washing and toileting. The assessment is scored on an ordinal seven-point scale with 1 indicating the patient is completely dependent. Scores of 2, 3 and 4 indicate the patient completes 25%, 50% or 75% of the task. A score of 5 is given if the patient requires supervision, cueing and/or setting up to complete the task, while 6 indicates they are independent with extra time or an assistive device. A score of 7 indicates that they are fully independent. The internal consistency of the BETA® scale is high at α = 0.96. The Rasch analysis confirmed significant person reliability and item reliability values on the BETA® scale. The BETA® subscales are reported to have good levels of accuracy and predictability (Loubser et al., 2015).
Research procedure
A research assistant, who was also part of the rehabilitation team, completed the demographic questionnaire with patients on admission to ensure that the researcher remained blinded to the HIV status of the stroke survivor. The researcher completed the compulsory training and was qualified to administer the BETA® scale. Data using the BETA® scale were collected at three points in time, namely on admission, at discharge and 1 month after discharge. The last assessment was completed during the stroke survivor’s routine 1-month follow-up appointment.
All the stroke survivors who participated in the study received therapy from the multi-professional team as per the hospital policy, including occupational therapy where participation in pADL was emphasised. Although treatment was individualised for each patient, hospital policy provides guidelines for therapists in terms of rehabilitation outcomes. On discharge, the caregivers of the stroke survivors routinely received training on the facilitation of independence and assistance required by the stroke survivor during pADL activities. Information on precautions to be observed was also stressed.
Data analysis
Descriptive statistics were used to analyse the demographic and BETA® scale data. The results of the HIV-negative and HIV-positive groups were compared using nonparametric statistics to accommodate the small sample size, lack of normally distributed data and the ordinal nature of the data. The change in the pADL scores within the two groups over the three assessment periods was analysed using Wilcoxon sign rank tests as well as effect sizes (Cohen’s r). A between-group analysis was completed on the difference in the scores from admission to discharge and from discharge to 1 month later using the Mann–Whitney U test and effect sizes (Cohen’s r). Change from admission to 1 month after discharge was also determined.
Results
The study sample consisted of 32 stroke survivors, who were divided into two groups: 63% (20) HIV-negative and 37% (12) HIV-positive stroke survivors.
Demographics
The HIV-negative group (age band mode 50–59 years) was significantly older than the HIV-positive group (p = 0.001) (age band mode 40–49 years). There were significantly more males (p = 0.014) in the HIV-negative group, with an equal distribution between males and females in the HIV-positive group (Table 1).
Demographics of the of the HIV-positive group and HIV-negative group.
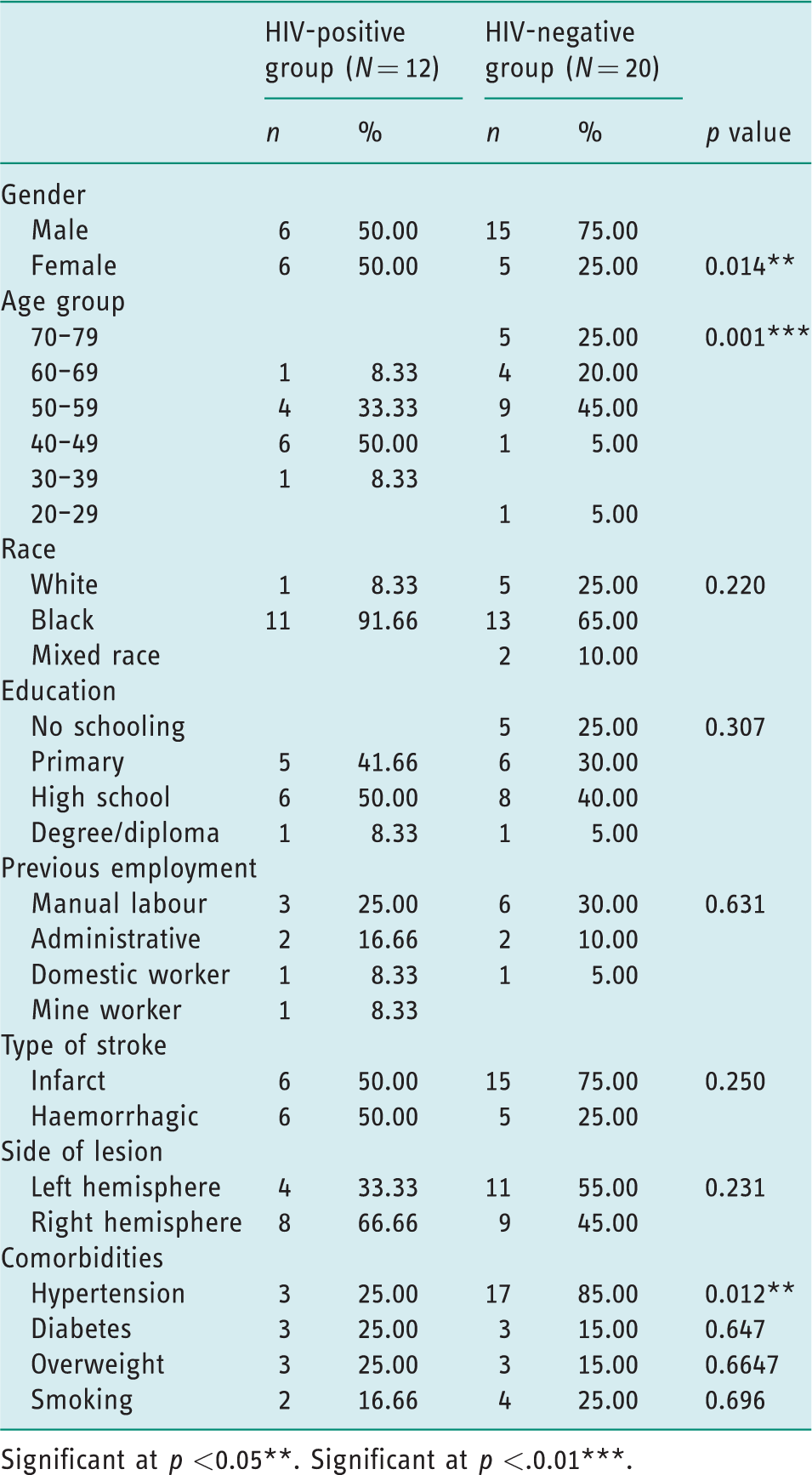
Significant at p <0.05**. Significant at p <.0.01***.
There was no statistical difference in racial distribution, education and previous types of employment between the HIV-negative and HIV-positive groups. In both groups, the majority of stroke survivors were unemployed.
Although more participants in the HIV-positive group had haemorrhagic strokes and a higher prevalence of right hemispheric lesions than the HIV-negative group, there was no significant difference between the groups. However, as suggested by Saposnik et al. (2011) and Kwakkel and Kollen (2013), this study did not consider the site of the lesion of the stroke but rather clinical information using a standardised test in determining the outcomes for pADL. All participants had been initiated on ART either prior to admission or while hospitalised.
No statistically significant differences between the two groups for comorbidities such as diabetes, obesity and smoking were found. The HIV-negative group had a significantly higher prevalence of hypertension, which was the most common comorbidity in the majority (85%) of participants in this group.
Personal activities of daily living scores for participants who were HIV-positive and HIV-negative over the three assessment periods
On admission both groups showed limited independence in pADL, especially washing, lower limb dressing and toileting. Both groups were found to have a statistically significant improvement in all domains of pADL during their inpatient rehabilitation (Table 2).
Total median personal activities of daily living scores of the HIV-positive and HIV-negative group over the three assessment periods.
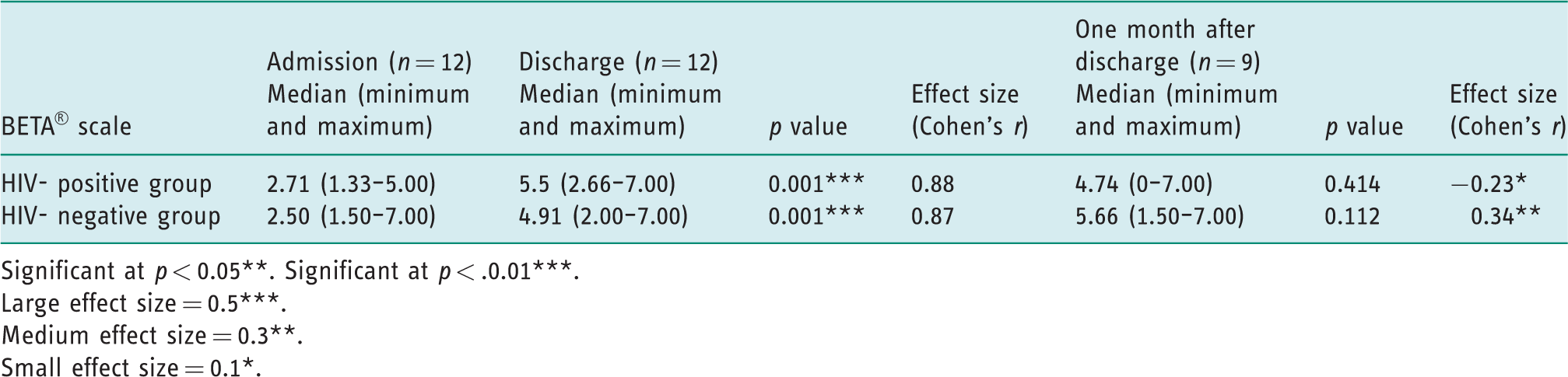
Significant at p < 0.05**. Significant at p < .0.01***.Large effect size = 0.5***.Medium effect size = 0.3**.Small effect size = 0.1*.
On discharge, the HIV-positive group achieved a statistically significant improvement and large effect sizes in all domains of pADL with the exception of washing, where participants scored 4 out of 7. The HIV-negative group scored 4 for both washing and toileting tasks but achieved a statistically significant improvement in all other domains of pADL, with large effect sizes indicating a clinically meaningful change in pADL. However, only 19% of the participants in the HIV-negative group achieved full independence in all domains of pADL on discharge compared to 39% in the HIV-positive group.
One month after discharge the HIV-positive group had no significant change in any of the pADL domains, with effect sizes indicting no or a small clinical improvement and a deterioration in their washing scores to a median score of 3.5. Median scores indicated most of the participants in this group now required set-up or cueing for grooming. At this stage the HIV-negative group continued to improve in all domains of pADL, although only grooming showed a statistically significant improvement (p = −0.020). An overall continued clinically meaningful improvement was supported by a medium effect size. These participants were independent or required minimal assistance with pADL tasks with the exception of washing, which scored 4.5.
Change in personal activities of daily living scores for participants that were HIV-positive and HIV-negative
The change in the BETA® scale scores between admission and discharge and from discharge to 1 month later were compared for the two groups to determine if one group improved more than the other during and after inpatient rehabilitation (Table 3).
Change in personal activities of daily living scores for HIV-positive and HIV-negative groups from admission to discharge and discharge to 1 month after discharge.
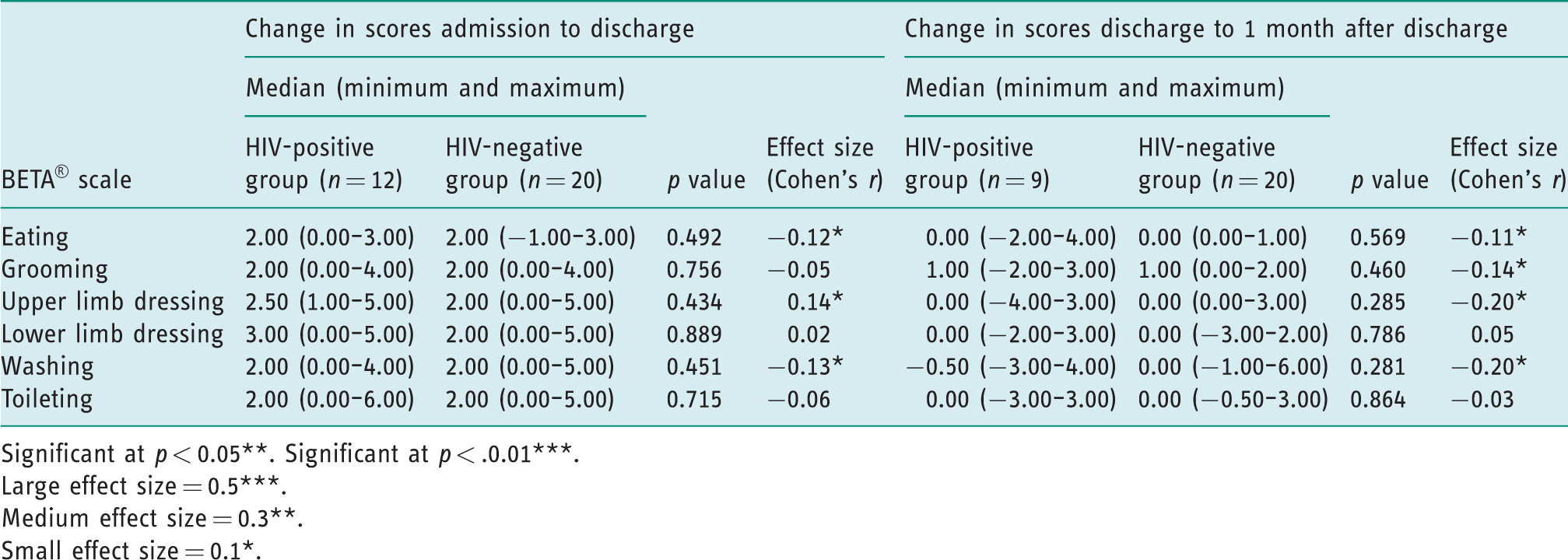
Significant at p < 0.05**. Significant at p < .0.01***.Large effect size = 0.5***.Medium effect size = 0.3**.Small effect size = 0.1*.
Although there were no significant differences between the groups in the scores from admission to discharge, the participants in both groups had median improvements of 2 to 3 points on their pADL scores. The younger participants in the HIV-positive group achieved a small clinically meaningful improvement in upper limb dressing compared to the HIV-negative group. The small negative effect sizes indicated greater clinically meaningful change in the HIV-negative group compared to the HIV-positive group for eating and washing.
Once the HIV-positive participants were discharged the median pADL scores showed no further change except for washing, which deteriorated. In this group 43% showed no change in their scores, while 29% had scores that were lower 1 month after discharge. This indicates the majority of participants achieved no further independence at 1 month post discharge. Although no statistical significance was found between the two groups after discharge, the small negative effect sizes indicate that that HIV-negative group had clinically meaningful improvement in eating, grooming, upper limb dressing and washing as compared to the HIV-positive group. In the HIV-positive group, only 32% of participants showed no change at 1 month after discharge, while 11% had lower pADL scores.
The lack of improvement in pADL in the HIV-positive group was confirmed when change from admission to 1 month after discharge was analysed. The HIV-negative group achieved statistically significant change (p = 0.000 to p = 0.015) and large effect sizes, indicating clinically meaningful change in all domains of pADL from admission to 1 month after discharge. The change in pADL scores for the HIV-positive group was not statistically significant when the change from admission to 1 month after discharge was analysed, indicating a return to levels of function similar to those seen on admission. This group did achieve limited clinical improvement for eating, grooming, lower limb dressing and washing as indicated by small effect sizes (Table 4).
Change in personal activities of daily living scores from admission to 1 month after discharge.
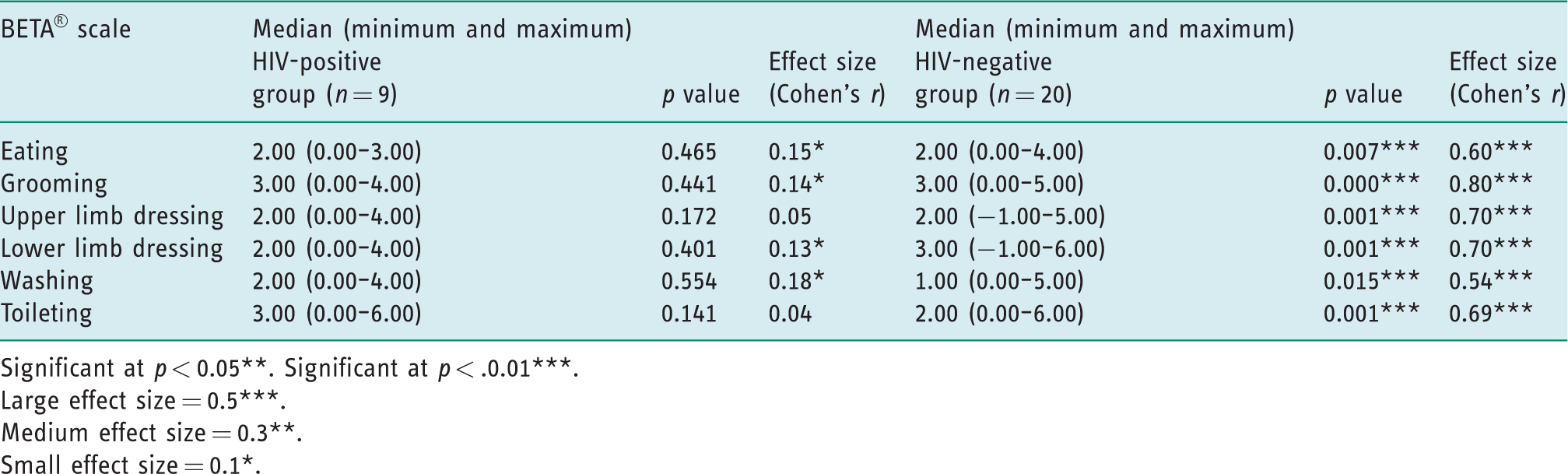
Significant at p < 0.05**. Significant at p < .0.01***.Large effect size = 0.5***.Medium effect size = 0.3**.Small effect size = 0.1*.
Discussion
The high percentage (37%) of participants admitted to the unit with stroke who were HIV-positive confirms the risk for stroke amongst adults with this condition in South Africa. This is similar to figures reported in Malawi (Heikinheimo et al., 2012) and is supported by the odds ratio of 2.46 (95% CI: 1.59–3.81) for stroke reported for HIV-positive individuals in sub-Saharan Africa (Namale et al., 2018). The greater percentage of male participants in this study was, however, contrary to the higher incidence of stroke (Connor et al., 2007) and HIV infection rate previously reported amongst women in South Africa (UNAIDS, 2018). The 10 year age difference between the HIV-positive group and the HIV-negative group is supported in the literature (Singer et al., 2013).
Hypertension is a significant risk factor for stroke in South Africa, where only 13.5% of those with hypertension receive treatment (Berry et al., 2017). This comorbidity was significantly more prevalent in the HIV-negative group, where the incidence of haemorrhagic strokes was similar to the 34% reported for African countries (Donkor, 2018). The high incidence of haemorrhagic strokes in the HIV-positive group is not consistent with the literature (O’Donnell et al., 2010) but has been associated with inflammation-induced vasculitis changes in cerebral arteries associated with other viruses and infections (Hatleberg et al., 2019). Thus, participants in this study may have been exposed to other infections prior to initiation of ART due to late diagnosis of HIV and limited access to ART in South Africa (Huerga et al., 2018). The higher incidence of right-sided stroke in the HIV-positive group does not appear to have affected the change in pADL, which is supported by research that indicates hemispheric lateralisation is not a predictor of functional outcome (Fink et al., 2008).
When the within-group scores of pADL were considered on admission, both HIV-positive and HIV-negative participants had marked dependence for all domains, requiring at least 25% assistance with activities such as eating and 100% assistance with lower limb dressing, washing and toileting. During the inpatient hospital stay, participants in both groups were found to have statistically significant improvement in all the pADL domains. These results are consistent with other South African studies (Joseph and Rhoda, 2013; Mamabolo et al., 2009), which show improvement in pADL after multi-disciplinary team rehabilitation in acute and sub-acute units. The findings are also supported by a 2014 Cochrane review (Pollock et al., 2014), which found that occupational therapy was significantly beneficial for independence in pADL in stroke survivors as compared with no intervention.
When the change in the pADL scores over time were compared there was no statistically significant difference between the scores of the two groups over the period of admission to discharge. This is supported by van Rensburg et al. (2018), who confirmed similar improvement in HIV-positive and HIV-negative patients with stroke during inpatient rehabilitation. However, 1 month after discharge the stroke survivors in the younger HIV-positive group showed a decreased ability to perform their pADL. It had been expected that the pADL of both groups would continue to improve in the month after discharge as this falls within time frame in which most patients are still expected to have further recovery (Jørgensen et al., 1995).
The decreased ability of the participants with HIV to perform their pADL after discharge may have been due to a number of factors. HIV is a chronic illness and will continue to affect the participants’ overall health, while the long term use of ART may also play a role in ongoing physical and mental deterioration and disability (Hama et al., 2007). Use of ART is associated with renal failure, peripheral neuropathy, hypersensitivity, bone marrow suppression, hyperglycaemia and gastro-intestinal disorders resulting in apathy and fatigue, which may also play a role (Dudgeon et al., 2004). Hanass-Hancock et al. (2015) also identified decreased participation in activities, including pADL, in over 40% of South Africans with HIV, due to mental health issues, particularly depression irrespective of time on ART. This was associated with mobility and cognitive limitations, both of which may apply to the participants with HIV in this study.
Although participants diagnosed with HAD were excluded from this study, asymptomatic neurocognitive impairment (ANI) and MND are estimated to affect 30–50% of HIV-positive individuals (Vally, 2011; Woods et al., 2009). Cognitive functioning was not assessed in the HIV-positive participants and deficits may have impacted their ability to maintain their independence in pADL after discharge. Therefore, over time HIV may be seen as an independent indicator for a poor prognosis in pADL function following stroke.
Limitations of the study
The sample size of the study was small and therefore generalisation of the results of the study is limited. The study was also limited to one hospital. While differences between the two groups were noticed, limited research is available regarding the effect of HIV on the rate and nature of stroke recovery, thus further investigation is necessary.
The relationship between site of lesion, CD4 count, HAND and pADL performance was also not included in the study. These aspects might have had an influence on the rate and nature of recovery of the HIV-positive stroke survivors. These aspects need further investigation.
Conclusion
This study confirms that there is no difference between the improvement of pADL between HIV-positive and HIV-negative stroke survivors during inpatient rehabilitation. This indicates that similar intervention programmes can be offered to HIV-positive and HIV-negative stroke survivors. A difference did exist between the groups after discharge. While discharge planning is important for all patients with stroke, additional attention to mitigate possible deterioration in patients who are HIV-positive must be considered. Follow-ups that are more regular might be needed for these stroke survivors. It is recommended that they be included in outpatient treatment programmes or are referred for further community-based rehabilitation at a facility close to their homes. Family training should include the possibility of deterioration in the pADL function of stroke survivors who are HIV-positive after discharge; therefore, additional measures to improve or to maintain their current functioning need to be included in the intervention.
Key findings
Confirmation of stroke at a younger age in HIV-positive patients. Both HIV-positive and HIV-negative patients benefit from inpatient rehabilitation in terms of personal activities of daily living (pADL). Only HIV-negative patients sustained improvements in pADL achieved during inpatient rehabilitation.
What the study has added
Occupational therapists should be aware that improvement in pADL made during inpatient rehabilitation may not be sustained in HIV-positive patients at 1 month post discharge and there is a need to plan for continuation of therapy and support accordingly.
Footnotes
Research ethics
Ethical approval was obtained from the Faculty of Health Sciences Human Research Ethics Committee of the University of Witwatersrand (M130934) in 2014. Permission was obtained from the North West Department of Health to conduct the study.
Consent
All participants provided signed informed consent for demographic and medical data access and for completion of the (SADFM) BETA® scale assessments. An individual information session was held with each participant and the implications of participation in the study were explained in their language of choice prior to the request for informed consent.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Contributorship
Hymeri Augustyn was the researcher and main contributor to the study in partial fulfilment of her master’s degree in occupational therapy in the School of Therapeutic Sciences, Faculty of Health Sciences at the University of Witwatersrand.
Patricia de Witt, the postgraduate supervisor, contributed substantially to the research process by advising, revising and editing the research proposal and research report.
Denise Franzsen advised on and completed the statistical analysis. Data was interpreted by Hymeri Augustyn and Denise Franzsen.
All authors reviewed, edited and contributed to the manuscript and approved the final version for submission and publication.