
Abstract
Introduction
Fatigue is a pervasive symptom of chronic disease that often interferes with occupational performance. Our objective was to describe what is known about energy management education and occupation-related outcomes in adults with chronic diseases.
Methods
Seven electronic databases were searched for relevant literature published before August 2019. Eligible articles were full-text, available in English, and studied energy management education in adults with a chronic disease. The first author assessed article eligibility with validation from a second reviewer, extracted characteristics of included studies, and described them using descriptive statistics. A narrative synthesis of findings was conducted for each chronic disease population.
Results
Forty-four studies addressed eight different chronic disease populations. The most common program delivery format was face-to-face in a group setting (42%), 39% of programs were informed by a learning theory, and their median cumulative length was 8 hours. Positive outcomes were associated with a specific, group-based energy management program in people with multiple sclerosis. The evidence on other energy management programs and in other chronic disease populations was more limited and inconclusive.
Conclusions
Further research is needed to understand the impact of energy management education in chronic disease populations beyond multiple sclerosis, and its impact on occupational performance.
Keywords
Introduction
Fatigue is one of the most common symptoms of illness; an estimated 5–7% of people who visit a primary healthcare provider present with fatigue as their primary complaint (Hamilton et al., 2010). Fatigue is defined as “an uncommon, abnormal or extreme whole bodily tiredness, disproportionate or unrelated to activity or exertion” (Piper, 1993: 285). It is a particularly prevalent symptom among populations with chronic or long-term illnesses. For example, 59–100% of people with cancer (Weis, 2011), 29–77% of post-stroke survivors (Acciarresi et al., 2014), 75% of people with multiple sclerosis (MS) (Braley and Chervin, 2010), 70% of people with advanced kidney disease (Murtagh et al., 2007), and 69–88% of people with heart failure (Fini and de Almeida Lopes Monteiro da Cruz, 2009) experience persistent and disabling fatigue. Across chronic disease populations, fatigue is a complex, nonspecific symptom that can have an array of multidimensional contributing factors (Chaudhuri and Behan, 2004). Effective pharmacological or medical treatments to alleviate fatigue are limited (Yancey et al., 2012). Of concern to occupational therapists, fatigue is often reported by patients as interfering with their occupational performance (Jones et al., 2016; Mandliya et al., 2016), which is “the ability to perceive, desire, recall, plan and carry out roles, routines, tasks and sub-tasks for the purpose of self-maintenance, productivity, leisure and rest in response to demands of the internal and/or external environment” (Ranka and Chapparo, 1997: 59). As the prevalence of chronic illness continues to increase globally (World Health Oganization, n.d.), identifying approaches to help people with fatigue optimize their occupational performance should be a high priority for occupational therapists.
Energy management education (EME) (also known as energy conservation or adaptive pacing) is an approach to fatigue management that teaches people to use occupation-focused strategies, such as prioritizing activities, pacing oneself, adopting energy-efficient body postures, or using energy-saving tools (Matuska et al., 2007), to reduce fatigue and improve occupational performance. Mathiowetz and colleagues (2001) assert that energy management education is specifically indicated when “fatigue interferes with occupational and/or role performance” (Mathiowetz et al., 2001: 450). The research that exists about EME and its effects on occupation or related outcomes in adults with chronic diseases has, however, not been comprehensively explored, apart from one systematic review in MS that has not been updated since 2013 (Blikman et al., 2013). Identifying and describing the literature on EME and occupational performance and related outcomes in adults with chronic diseases will help to identify research gaps, and inform occupational therapists seeking to engage in evidence-based practice with clients experiencing chronic fatigue. Accordingly, the purpose of this scoping review was to identify and describe the literature on energy management education and occupational performance or related outcomes in adults with chronic diseases.
Methods
We followed scoping review methodology as described by Arksey and O’Malley (2005) for this review. Scoping review methodology is used to summarize the extent, range, and nature of research activity in a research area, for the purpose of collating knowledge and/or identifying evidence gaps (Arksey and O’Malley, 2005). Arksey and O’Malley’s (2005) five iterative scoping review stages were implemented and are used to structure this paper. The Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) extension for scoping reviews (PRISMA-ScR) (Tricco et al., 2018) was also followed to ensure optimal reporting (Appendix 1 online materials). PRISMA was chosen as it is a widely accepted international gold standard for reporting systematic reviews and meta-analysis.
Stage 1: identify the research question(s)
The primary research question of this review was: what is known about the impact of EME on occupational performance or related outcomes in adults with chronic diseases? Specifically, we sought to identify the chronic disease populations in which EME has been investigated; describe the characteristics of existing studies; identify the key characteristics of existing EME programs; and describe the reported findings on EME.
Stage 2: identify relevant studies
The primary author developed the search strategy with an experienced rehabilitation information specialist. The following list of search terms was used to identify literature pertaining to energy management education: energy management, energy conservation, fatigue management, energy saving, adaptive pacing, work simplification, and energy envelope. Search terms were also used to narrow the results to education-related intervention studies: education, training, program, course, and treatment. Where available, database-specific search limiters were also used to further narrow the results to intervention studies (for example comparative study, evaluation studies, multicenter study, and clinical trial for Medline). No search terms were applied to narrow the review population; rather, we kept the scope of the search broad at this stage to ensure relevant literature was not missed. A detailed example of the search strategy for Medline is included in Appendix 2.
All search terms were entered into the subject heading, title, abstract, and keyword fields in seven electronic literature databases (Medline, Embase, Pubmed, Cochrane database of systematic reviews, CENTRAL, CINAHL, and PsycInfo), to identify literature published up to August 2019. Search limits were placed on study population (adult only) and publication language (English only). The primary author also reviewed reference lists of seminal articles to ensure literature was not missed in the electronic search.
Stage 3: select studies
The information specialist imported the results from the electronic search into Endnote reference management software and removed duplicate articles. Filters were applied to eliminate extraneous articles that were captured due to conceptual overlap (such as environmental energy management). Two screeners (the first author and an MSc student, who first underwent training in applying the study eligibility criteria) independently reviewed a random sample (10%) of the results according to the study inclusion/exclusion criteria, to validate the screening process and refine study eligibility criteria. Any disagreements about study eligibility were resolved through discussion to reach consensus. The primary author then screened the remaining titles/abstracts and full-text articles to determine their eligibility. We used the following inclusion/exclusion criteria to select articles:
Inclusion criteria
Study participants were aged ≥18 years. Study participants had a chronic disease (defined as a disease lasting >3 months, in accordance with the U.S. National Center for Health Statistics definition). The primary focus of the intervention was energy management education (teaching strategies to manage energy expenditure during everyday activities). The study sought to understand the impact of EME on occupational performance or related outcomes, including fatigue, fatigue impact, quality of life, and self-efficacy. The article was available in English.
Exclusion criteria
The fatigue intervention included one or more other fatigue management approaches (for example cognitive-behavioral therapy, exercise) in addition to energy management education. The article was not peer-reviewed. The result was an abstract, conference proceeding, or review article.
Stage 4: chart the data
The authors collaboratively developed a Microsoft Excel data sheet to document and organize the study data from the eligible articles. The first author then independently extracted and charted the data. Data extracted were:
Publication characteristics (title, authors, year, journal); Study characteristics (location, research question, research design, sample size, outcome measures); Sample characteristics (clinical condition, mean age, gender; additional unique characteristics of the sample such as clinical setting, recruitment methods, age restrictions, functional status); EME program characteristics (content, length, mode, format); Major findings (quantitative or qualitative) relating to occupational performance or related outcomes (consistent with scoping review methodology (Arksey and O’Malley, 2005), no critical appraisal was undertaken).
Stage 5: collate, summarize, and report results
We described the characteristics of included articles, studies, and samples, using frequencies and percentages or means, where appropriate. We used a narrative synthesis approach (Popay et al., 2006) to summarize reported findings on EME and its effects on occupational performance-related outcomes within each chronic disease population. As the literature was particularly extensive on the MS population, findings in MS were further grouped according to EME program.
Results
The search strategy generated 8654 possible items. After we removed duplicates and screened articles for eligibility (Figure 1), we identified 44 primary articles that were eligible for the review.

PRISMA flow diagram of study selection process.
Description of the literature
Eighteen of the 44 articles (41%) were published within the last 5 years (2014–2019) (Table 1). Just over half (n = 24) focused exclusively or primarily on the MS population. The remaining 20 articles focused on chronic fatigue syndrome (five studies), cancer (five studies), cardiac disease (three studies), arthritis (three studies), acquired brain injury (two studies), fibromyalgia (one study), and post-polio syndrome (one study). Of the 44 eligible studies, 28 measured the effects of EME on occupational performance or related outcomes (Table 2). The remaining studies described specific occupation-related goals and energy management strategies used in EME programs; evaluated the impact of EME design components on outcomes; identified client characteristics that moderate outcomes after EME; and captured client experiences of EME. Among the 28 efficacy studies, 11 were randomized controlled trials, 10 were pilot/feasibility studies, five were pre–post studies, two were single-case studies, and one was a secondary analysis. Thirteen assessed the impact of EME on occupational performance; other related outcomes that were investigated included fatigue (21 studies), mental health (16 studies), and fatigue impact (14 studies).
Characteristics of articles included in the review.
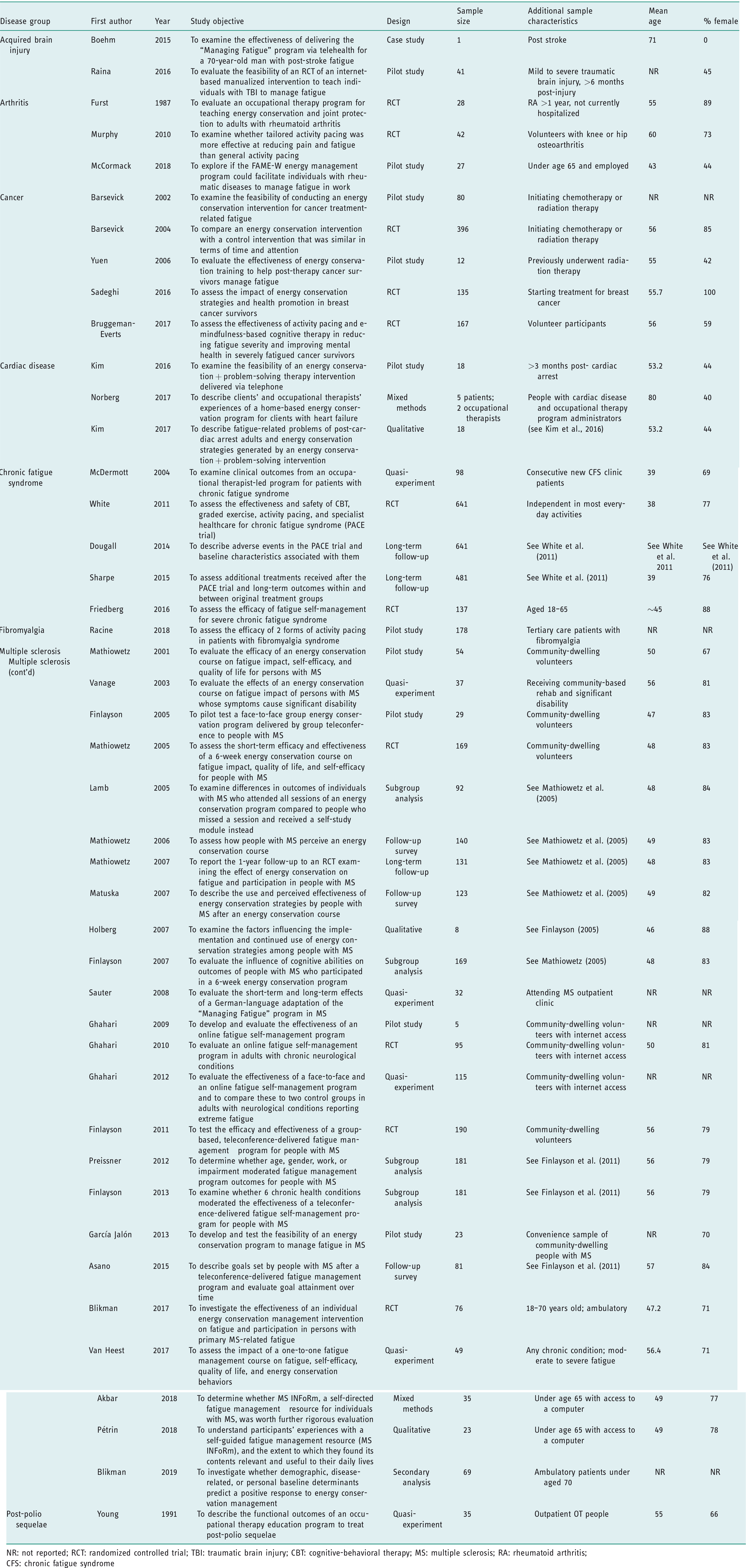
NR: not reported; RCT: randomized controlled trial; TBI: traumatic brain injury; CBT: cognitive-behavioral therapy; MS: multiple sclerosis; RA: rheumatoid arthritis;CFS: chronic fatigue syndrome
Reported findings on occupation and related outcomes associated with energy management education (EME).

+: favors EME; –: no difference between EME and control; M: mixed evidence; blank: not assessed
Characteristics of energy management education programs
Twenty-six different EME programs were identified in the 44 studies (Table 3). The group-based “Managing Fatigue: A Six-Week Course in Energy Conservation” (Packer et al., 1995) was used in eight (18%) studies, while adaptations of the program including a teleconference-based program, an internet-based program, a program for individuals with higher levels of disability, and 1:1-based programs were used in 14 studies (32%). Across the 22 remaining studies, 18 different EME programs were identified. The median cumulative length of the programs was 8 hours (range 1–27). Half of the programs relied predominantly on a face-to-face delivery model, while the remaining half used telephone delivery (three programs), computer delivery (two programs), and mixed modalities (four programs). Eight programs were delivered by a provider on a 1:1 basis, while seven were delivered in groups, and three used a self-guided model. In total, 42% of the EME programs mentioned a theoretical framework used to inform program design, and 26% incorporated a goal-focused approach to EME.
Design characteristics of energy management education programs described in the literature.
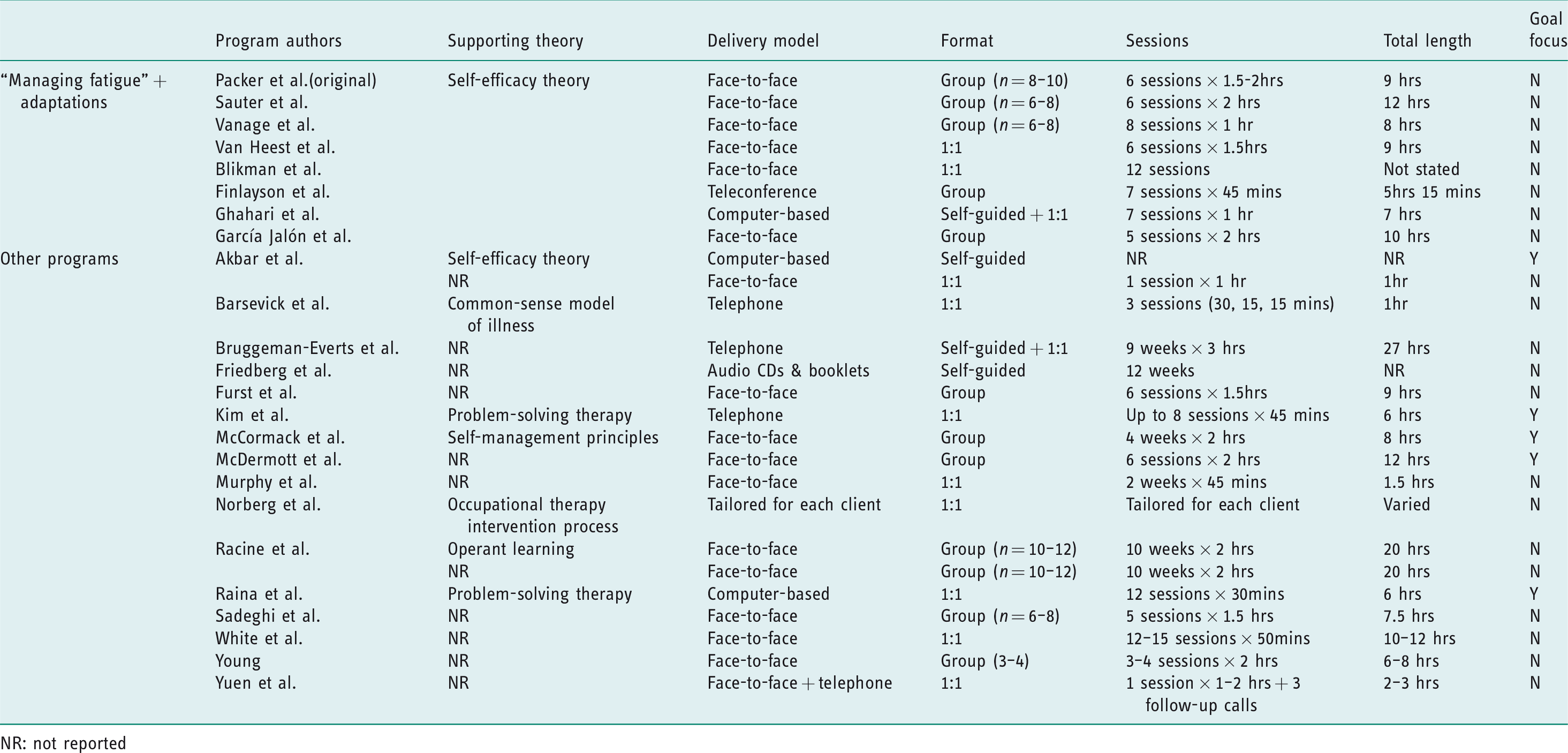
NR: not reported
Findings regarding occupational performance and related outcomes
Multiple sclerosis
The “Managing Fatigue” program
Reported findings on the “Managing Fatigue” program in people with MS have been generally positive. A pilot randomized controlled trial (RCT) found that the program was associated with improvements in fatigue, fatigue impact, and some quality of life domains (Mathiowetz et al., 2001) (Table 3). A large RCT confirmed these findings, and also found that the program was associated with improvements in self-efficacy. The improvements associated with EME were maintained at 6 weeks (Mathiowetz et al., 2005) and 1 year post intervention (Mathiowetz et al., 2007). Participants’ baseline cognitive status was not found to influence fatigue outcomes (Finlayson et al., 2007), and participants who missed ≥1 treatment session and received self-study modules instead experienced comparable outcomes to people who attended all sessions (Lamb et al., 2005). The most useful EME strategies taught in the program according to participants were taking rest breaks, delegating tasks, and modifying priorities; however, all 14 strategies covered in the program were newly adopted by more than half of the participants (Matuska et al., 2007). Overall, the most valued components of the program were concepts such as budgeting and banking energy and the social aspect of the group-based format, while less-valued components were completing homework assignments, and topics such as activity stations and ergonomics (Mathiowetz and Busch, 2006).
Teleconference-based adaptation
Reported findings on a teleconference-based version of the “Managing Fatigue” program have been mixed. A pilot study found that the program was associated with significant improvements in fatigue impact, fatigue severity, and some domains of quality of life (Finlayson, 2005). An RCT confirmed the improvements observed in fatigue impact, which were found to be maintained at 6 months post-intervention. However, the RCT found no changes in self-efficacy, fatigue severity, or quality of life associated with the teleconference-based program (Finlayson et al., 2011). Participants were found to achieve approximately half of the occupational performance goals they set at the beginning of the study, with short-term goals more frequently being achieved than mid-term or long-term goals (Asano et al., 2015). Older adults were found to experience less improvement in fatigue impact or self-efficacy after the program, and those with a lower baseline functional status experienced less improvement in mental health (Finlayson et al., 2012). Comorbidities such as diabetes and rheumatoid arthritis also moderated outcomes (Finlayson et al., 2013). In qualitative interviews, participants reported that the program had changed their perspective on fatigue and enabled them to feel more in control of their lives (Holberg and Finlayson, 2007); however, they reported that factors such as disease progression, level of disability, and predictability of fatigue affected their use of EME strategies.
Internet-based adaptation
Reported findings on an internet-based version of the “Managing Fatigue” program have been largely negative. A small pilot study found the program was associated with improvements in occupational performance, fatigue impact, and quality of life (Ghahari et al., 2009). However, an RCT involving participants who had various progressive neurological conditions found that the internet-based adaptation had no effect on occupational performance, fatigue impact, or quality of life (Ghahari et al., 2010). When the data on the online adaptation was compared post-hoc to a non-equivalent group who received the original “Managing Fatigue” program, the original program was associated with greater improvements in fatigue impact (Ghahari and Packer, 2012).
One-to-one adaptations
Reported findings on 1:1 adaptations of the “Managing Fatigue” program have been mixed. A pre–post study involving participants who predominantly had MS found that a 1:1 “Managing Fatigue” program adaptation was associated with improvements in fatigue and self-efficacy (Van Heest et al., 2017). However, an RCT of a different 1:1 “Managing Fatigue” adaptation found no effect on occupational participation or fatigue (Blikman et al., 2017). Participants who had a less negative perception of fatigue, perceived fewer disease benefits, and perceived a higher discrepancy in social support were more likely to respond to the EME intervention in the RCT (Blikman et al., 2019).
Other adaptations
An RCT of the “Managing Fatigue” program adapted for people with a lower functional status found the program was associated with improvements in fatigue impact, and gains were maintained at 8 weeks post-intervention (Vanage et al., 2003). Meanwhile, a pre–post study that examined a German-language adaptation of the “Managing Fatigue” program found that it was associated with improvements in fatigue impact at 3 months and 9 months post-intervention, but fatigue was unaffected (Sauter et al., 2008).
Other EME programs in MS
Findings on other EME programs beyond “Managing Fatigue” in MS have been mixed. A mixed-methods study found that a self-guided, computer-based EME program (MSInform) was associated with improved fatigue impact and self-efficacy (Akbar et al., 2018). In qualitative interviews, participants reported experiencing a shift in their knowledge, expectations, and behaviors related to fatigue management after completing the program, which led to increased self-confidence and improved quality of life (Pétrin et al., 2018). However, a pilot RCT examining a different six-session, group-based EME program that was informed by the “Managing Fatigue” program and several other EME programs reported no effect on fatigue, self-efficacy, or depression symptoms (García Jalón et al., 2013).
Chronic fatigue syndrome
Reported findings on EME in people with chronic fatigue syndrome have been mixed. A large RCT comparing an extensive 1:1 EME program administered by an occupational therapist with cognitive-behavioral therapy (CBT), graded exercise (GET), and usual care (UC) reported that EME had no effect on occupational performance, fatigue, physical performance, or mental health (White et al., 2011). In a follow-up study, people allocated to EME or standard care were reportedly more likely to experience a decline in physical functioning compared to the CBT and GET participants (Dougall et al., 2014). However, a pre–post study of a six-session, group-based EME program in 98 people with chronic fatigue syndrome (CFS) reported that 56% of program participants underwent work training or acquired new full-time, part-time, or volunteer work at 18 months post-intervention, while 19% continued with their previous employment (McDermott et al., 2004). Another RCT conducted with participants who had extensive disability at baseline found that two versions of a self-guided EME program (a “high tech” and “low-tech” version) were both associated with reductions in fatigue and depression symptoms; however, self-care independence, activity levels, and anxiety were unaffected (Friedberg et al., 2016).
Cancer
Findings on EME in people with cancer have been mixed. Two RCTs that examined extensive EME programs both reported improvements in fatigue associated with EME (Bruggeman-Everts et al., 2017; Sadeghi et al., 2016). The first program used a partially self-guided format that was administered over 9 weeks with support from a physiotherapist (Bruggeman-Everts et al., 2017), while the second used a group-based format that took place over five 90-minute sessions (Sadeghi et al., 2016). A pilot study on another EME program administered over three brief telephone sessions similarly reported positive effects on fatigue (Barsevick et al., 2002). However, a large RCT examining the same program did not find it to be associated with clinically meaningful improvements in fatigue or occupational performance (Barsevick et al., 2004), while another pilot study that examined a brief, home-based EME program with cancer survivors similarly reported that the majority of fatigue domains were unaffected by EME (Yuen et al., 2006).
Cardiac disease
Few studies have investigated EME in people with cardiac diseases. A small pilot study of an EME program that used an individualized, telephone-based, goal-focused, problem-solving approach found that it was associated with improvements in fatigue impact, fatigue, and occupational performance in cardiac arrest survivors (Kim et al., 2016). Planning ahead, pacing oneself, and delegating activities were the most common energy management strategies used by participants, while the most common goal activities were household tasks, leisure activities, and grocery shopping (Kim et al., 2017). Meanwhile, a small pilot study of a different, 1:1 EME program found that both fatigue and mental health outcomes were mixed (Norberg, 2017).
Acquired brain injury
Few studies have investigated EME in people with acquired brain injury. A case study of a 1:1, teleconference-based adaptation of the “Managing Fatigue” program in a participant living post stroke found the program was associated with a decrease in multiple domains of fatigue impact, but did not improve occupational performance (Boehm et al., 2015). Meanwhile, a pilot RCT of an internet-based EME program that used a problem-solving therapy approach found the program was associated with improvements in fatigue and fatigue impact in people with an acquired brain injury (Raina et al., 2016).
Arthritis
Few studies have investigated EME in people with arthritis. A pilot study that compared a group-based EME program to usual occupational therapy care reported that the EME program was associated with increases in physical activity levels, and balance between rest and activity, at 3 months post-intervention. However, no differences were reported in other study outcomes such as pain, fatigue, psychosocial adjustment to illness, knowledge, or independence in activities of daily living (Furst et al., 1987). A pre–post study of a group-based program focused on energy management at work in individuals with rheumatoid arthritis (RA) found that participants were more able to meet work demands and had reduced symptoms (for example fatigue, pain, depression) at 3 months post-intervention (McCormack et al., 2018). An RCT with 32 osteoarthritis patients that compared a tailored EME program to a generalized EME program found the tailored intervention to be associated with less fatigue interference at a 10-week follow-up assessment (Murphy et al., 2010).
Fibromyalgia
One study investigated EME in people with fibromyalgia. An RCT compared a traditional energy management approach and an approach that used learning principles that were operant to each other and to a control condition. Neither program was associated with reduced fatigue or pain compared to the control group, but both programs were found to improved sleep quality, physical function, and pacing activity (Racine et al., 2018). The operant learning condition was reportedly associated with greater improvements in fatigue interference and psychological function (Racine et al., 2018).
Post-polio syndrome
One study investigated EME in people with post-polio syndrome. A pre–post study investigated the effects of a group-based EME program in 35 people with post-polio syndrome, and reported improvements in fatigue associated with the program (Young, 1991).
Discussion and implications
Our study is the first to comprehensively identify and describe the literature on EME and occupational performance or related outcomes in adults with chronic diseases. EME has been studied in eight different chronic disease populations, including MS, cancer, CFS, cardiac disease, arthritis, acquired brain injury, fibromyalgia, and post-polio syndrome. The literature was most extensive on the six-session, group-based “Managing Fatigue” program (Packer et al., 1995) in MS, where studies including RCTs suggested positive impacts on outcomes related to occupational performance, such as fatigue impact and self-efficacy (Finlayson et al., 2011; Mathiowetz et al., 2005). Participants of this program reported that the energy management strategies they learned were novel and effective (Mathiowetz and Busch, 2006; Matuska et al., 2007), and that other aspects of the program, such as making social connections, were valuable (Mathiowetz and Busch, 2006). However, the evidence on EME for other programs and chronic disease populations was found to be more limited, and often described mixed or inconclusive findings. There were also few studies that directly investigated the effects of EME on occupational performance.
The lack of robust research on EME outside of MS is surprising, given the prevalence of fatigue in many chronic diseases populations (Acciarresi et al., 2014; Fini and de Almeida Lopes Monteiro da Cruz, 2009; Weis, 2011) and the need for evidence-based interventions to improve fatigue management. In some populations (for example arthritis, post-polio, cardiac disease), although preliminary findings appeared to be promising, a lack of RCTs limits the conclusions that can be drawn about the efficacy of the approach. In other populations (for example cancer and CFS), although large RCTs have been conducted, they had potential methodological limitations that might minimize their validity. For example, in cancer, an RCT that reported EME had limited effects on fatigue and physical function (Barsevick et al., 2004) used a very brief EME program, which might have provided insufficient education to achieve positive outcomes. In CFS, a large RCT showed no effect of an extensive, individually delivered EME program on occupational performance, fatigue, physical performance, or mental health (White et al., 2011), but the validity of this trial and its conclusions have been questioned due to several methodological concerns since its publication (Jason, 2017; Wilshire et al., 2017), including concerns with the activity pacing intervention (Jason, 2017). We also found no studies (preliminary or other) on EME in other chronic disease populations known to have a high burden of fatigue, such as chronic kidney disease (Murtagh et al., 2007) and chronic obstructive pulmonary disease (Baltzan et al., 2011). Collectively, this review highlights the need for more well-designed primary studies about EME in adults with chronic diseases, to support occupational therapists seeking to engage in evidence-based practice in this area.
The limited evidence addressing the impact of EME on occupational performance was surprising, given that EME has been described as an intervention with a specific focus on occupation and role participation (Mathiowetz et al., 2001). While changes in occupational performance components such as fatigue might translate to improved occupational performance, reduced fatigue might not affect occupational performance if the fatigue management strategies learned are not applicable to the patient’s top-priority occupations. We therefore recommend that more studies are conducted to examine the impact of EME on occupational performance. We also found that available evidence on EME and occupational performance was mixed, with more studies reporting negative than positive findings. We question, as others have (Asano et al., 2015; Kim et al., 2017; Raina et al., 2016), whether a goal-focused approach to EME might maximize its impact on occupational performance. In the broader rehabilitation literature, goal-based, problem-solving interventions are used to improve occupational performance in diverse clinical populations (Dawson et al., 2009; Polatajko et al., 2012; Smits-Engelsman et al., 2013). It is suggested they are effective in part due to their individualized, client-centered approach, and use of techniques that promote self-management and independence (Dawson et al., 2017). However, we found that less than one-third of the EME programs identified in this review used a goal-based or problem-solving approach. Such approaches to EME might be optimal for providing individualized energy management strategies that address idiosyncratic occupations and contexts, and for providing methods for problem-solving around future goals. We therefore recommend that future EME research continues to explore the potential of goal-based, problem-solving approaches, and investigate their impact on occupational performance relative to traditional approaches.
Overall, there was extensive variability in the 26 EME programs used across the 44 studies, which complicates interpretation of the evidence across studies and populations. Some program differences, such as formats or delivery modes, could reflect population-specific needs and contexts, and there does not appear to be a consensus about which format or modality is generally most effective in the general health education literature (Hoddinott et al., 2010; Wilson, 1997). Rather, specific formats can each have strengths and weaknesses. For example, 1:1 formats more readily allow for intervention tailoring (Noar et al., 2007), while group formats provide an opportunity for social interaction and learning (Hoddinott et al., 2010). Similarly, while face-to-face programs can enable participants to receive direct social support, tele-based formats and e-formats can be more accessible and convenient for patients (Polinski et al., 2016). However, across formats and modalities, behavior-based interventions should always be based on sound learning and design theory, since those lacking a theoretical framework may omit components and processes that are central to behavior change, and therefore fail to optimize their effectiveness (Michie and Abraham, 2004). In total, we found that only 39% of the EME programs in this review identified a theory that guided intervention development, which suggests this as an area for future improvement in EME research that could help to maximize its efficacy. We also observed a wide range of cumulative program lengths, ranging from 1 hour to 27 hours, which could reflect the lack of theory-based design leading to wide differences in dosing between studies. While inadequate dosing might mean missing or incomplete elements of education and skills training, excessive dosing might limit feasibility and result in the overuse of resources. We therefore recommend that future EME studies carefully consider learning and design theory to identify the essential components of an EME intervention, in order to maximize efficacy and efficiency.
The strengths of this review include the comprehensive literature search that was conducted by trained professionals; the broad examination of the evidence on EME across clinical populations; and the systematic approach used to locate, select, and synthesize the literature. Its limitations include the exclusion of non-English studies, which may limit the generalizability of the findings; limitations inherent to a scoping review (for example the lack of a systematic evaluation of evidence quality), which may mean that quality-based gaps in the evidence were not identified; and the use of only one data extractor, which may increase the likelihood of data extraction errors.
Conclusions
Multiple studies support the “Managing Fatigue” group EME program as an effective intervention for improving outcomes related to occupation in the MS population. Preliminary evidence on EME is also promising in acquired brain injury, post-polio syndrome, and cardiac disease, but further robust research is needed to confirm these findings. Evidence on EME is conflicting in cancer and CFS, signifying a need for further, well-designed studies. Investigation into EME in other chronic disease populations with a high burden of fatigue, such as COPD and kidney disease, is also warranted. Future EME studies should aim to understand its impact on occupational performance, and should use programs that are theory-based.
Key findings
Energy management education has been found to improve outcomes in several studies in multiple sclerosis. Beyond multiple sclerosis, the evidence on energy management is more limited and inconclusive. There is currently limited evidence demonstrating the effects of energy management education on occupational performance.
What this study has added
This study has comprehensively synthesized the evidence on energy management education in adults with chronic diseases, and has identified the need for more robust primary research studies in populations beyond multiple sclerosis.
Supplemental Material
BJO904327 Supplemental Material1 - Supplemental material for Energy management education and occupation-related outcomes in adults with chronic diseases: A scoping review
Supplemental material, BJO904327 Supplemental Material1 for Energy management education and occupation-related outcomes in adults with chronic diseases: A scoping review by Janine F Farragher, Sarbjit V Jassal, Sara McEwen and Helene J Polatajko in British Journal of Occupational Therapy
Supplemental Material
BJO904327 Supplemental Material2 - Supplemental material for Energy management education and occupation-related outcomes in adults with chronic diseases: A scoping review
Supplemental material, BJO904327 Supplemental Material2 for Energy management education and occupation-related outcomes in adults with chronic diseases: A scoping review by Janine F Farragher, Sarbjit V Jassal, Sara McEwen and Helene J Polatajko in British Journal of Occupational Therapy
Footnotes
Research ethics
Ethics approval was not required for this study as it is a scoping review that involves no participants.
Consent
Informed consent was not relevant as this is a scoping review that involves no participants.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and publication of this article: Janine F Farragher received financial support via a Vanier Canada Graduate Scholarship and a Kidney Foundation of Canada Allied Health Doctoral Fellowship. No other authors received financial support for the research, authorship, or publication of this article.
Contributorship
All authors contributed to formulating the research question and designing the methodology for the project. Janine F Farragher carried out the literature search, article selection, data extraction, and synthesis of results. All authors contributed to interpreting the data. Janine F Farragher wrote the first draft of the manuscript. All authors reviewed and edited the manuscript and approved the final version.
Supplementary material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.