
Abstract
Introduction
This study investigated whether listening and communication skills are predictive of occupational therapy students’ resilience.
Method
135 third- and fourth-year undergraduate occupational therapy students (74% response rate) completed the Active-Empathetic Listening Scale, Listening Styles Profile – Revised, Interpersonal Communication Competence Scale, Resilience at University and Resilience Scale for Adults instruments. Linear regressions were completed with the Resilience at University and Resilience Scale for Adults subscales as the dependent variables and the Active-Empathetic Listening Scale, Listening Styles Profile – Revised and Interpersonal Communication Competence Scale subscales as the independent variables.
Results
Regression analysis identified significant predictors of students’ resilience. The Active-Empathetic Listening Scale: Sensing Listening accounted for 5% (p = .009) and 4.3% (p = .011) of the unique variance of Resilience at University: Find Your Calling and Living Authentically. Listening Styles Profile – Revised: Analytical Listening accounted for 4.4% (p = .022) and 2.7% (p = .038) of the unique variance of Resilience at University: Managing Stress and Maintaining Perspective. Interpersonal Communication Competence Scale: Self-Disclosure accounted for 6.7% (p = .003), 3.6% (p = .035) and 3.4% (p = .047) of the unique variance of Resilience Scale for Adults: Social Resources, Resilience at University: Maintaining Perspective and Resilience Scale for Adults: Planned Future. Interpersonal Communication Competence Scale: Social Relaxation accounted for 8.5% (p = .001) of the unique variance of Resilience Scale for Adults: Social Competence.
Conclusion
Components of listening and interpersonal communication were found to be significant predictors of resilience in occupational therapy students. Further investigation in this area of research is recommended.
Introduction
Within the allied health professions, highly attuned listening and communication skills are fundamental components of client-centred practice, establishing therapeutic rapport with patients and beneficial working relationships with colleagues. Resilience comprises the positive resources an individual possesses that can be activated during stressful life events to prevent the development of negative mental health outcomes (Herrman et al., 2011). As such, resilience is considered a key capability for graduates that enables them to overcome adversity by drawing on personal, social and organisational resources to achieve personal growth and transformation (Sanderson and Brewer, 2017). The purpose of this study is to examine the association between components of listening and interpersonal communication and factors that facilitate resilience in a sample of occupational therapy students.
Background literature
Listening skills
The ability to listen actively and effectively has been shown to exert a positive influence on the development of provider–patient relationships by fostering improved patient understanding, adherence to treatment plans and increased patient satisfaction levels (Bennett and Lyons, 2011; Pope et al., 2008). It is regarded as a core competency for occupational therapists and assists in the demonstration and application of professional behaviours, values and attitudes (Aguilar et al., 2012).
Active listening requires the empathic and emotional involvement of a listener and consists of sensing the emotional needs of a patient, processing what has been said, understanding and responding by using verbal and non-verbal responses, and asking questions to indicate active attention (Bodie et al., 2013). The art of active listening is not simply the practice of individual skills such as maintaining eye contact or an open posture but concerns a state of being and connectedness with others whereby real depth and meaning are added to interactions (Ellis and Abbott, 2018). In therapeutic and clinical settings, illness, pain and treatment are often ‘triggers’ for feelings of fear and distress in patients, which may present personal and professional challenges for the health professional (Maunder and Hunter, 2012). By listening with all the senses, validating the speaker’s emotions and using reflective questioning, empathic listening builds the necessary trust for patients to follow medical and therapeutic advice. Research demonstrates that active-empathic listening is associated with the maintenance of positive health behaviours and higher patient and practitioner satisfaction rates (Hojat et al., 2011; Menendez et al., 2015).
Interpersonal communication skills
Interpersonal communication is a broad term that encompasses a spectrum of attributes considered essential for beneficial interactions between individuals, ranging from openness, empathy and sociability through to supportiveness, expressiveness and immediacy (Gilligan et al., 2016). In interactions with clients and colleagues, transparency and engagement foster interpersonal relationships that are contextually appropriate to both the person and situation. This is reflected in research investigating supportiveness and immediacy in paramedic students that highlights the importance of these attributes in demonstrating the empathic behaviours required for treating and reassuring concerned and often distressed patients (Ross et al., 2014). For allied health students in training, the practice education setting provides opportunities for them to develop their interpersonal skills and apply them appropriately to facilitate team functioning, collaboration and the management of conflict and negotiations. The different healthcare and community settings also support students in learning the importance of adapting interpersonal communication accordingly within multi-disciplinary team environments and during the course of interacting with patients drawn from diverse cultural backgrounds and presenting with variable therapeutic needs and cognitive abilities (Maloney and Griffith, 2013).
Resilience
At a practical level, resilience is the ability to bounce back and the ‘process of adapting well in the face of adversity, trauma, tragedy, threats or significant sources of stress’ (American Psychological Association, 2014). The literature indicates that working in the helping and caring professions, including occupational therapy, is rewarding but emotionally demanding and stressful (Ashby et al., 2013; McCann et al., 2013). Resilience levels among undergraduates across a range of health professions including occupational therapy, physiotherapy, medicine, midwifery and paramedicine are reported as being unsatisfactory, with factors such as time pressure, workload, multiple roles and emotional issues having a deleterious effect on students’ stress-coping abilities (de Witt et al., 2019; McCann et al., 2013; Tambag and Can, 2018). These challenges are particularly acute when students are required to undertake practice placements where they are confronted with the reality of clinical practice following classroom learning, resulting in students feeling isolated and unsupported. This highlights the importance of developing resilience strategies in health science students prior to their professional training when they are likely to experience heavy workloads, mental and physical exhaustion and new working environments (Bar et al., 2018).
Employment-related stressors reported across a range of health professions including physiotherapy, social work, pharmacy and nutrition provide evidence of a spectrum of resilience indicators including job satisfaction, emotional competence, empathy and tenacity (Da Silva Sousa and De Araujo, 2015). Studies of medical students suggest that opportunities to discuss difficult clinical events and levels of self-awareness can also impact the professional preparation of students (Houpy et al., 2017). Research in the nursing arena has identified three broad categories of resilience – wellbeing, social support and self-care – reporting that students who feel supported and demonstrate strong personal and professional identities possess better coping strategies and are positively associated with reduced instances of burnout in the workplace environment, improved work–life balance and lower anxiety levels (Bar et al., 2018).
Resilience is therefore a multifaceted concept that draws on the notions of support, wellbeing and empowerment. There is also a view that resilience can be based on internal traits (personality, values, thinking style, beliefs, social supports) but also an ecological perspective that views resilience in the context of person–environmental transactions varying across dimensions, time periods and social networks/organisations (Stokols et al., 2013). Ungar (2011) refers to this perspective as the social ecology of resilience and has four key principles as its basis: decentrality, complexity, atypicality and cultural relativity. It focuses on the ‘design of interventions that promote well-being among populations who experience environments that inhibit resilience-promoting processes’ (1). Therefore, based on the ecological resilience view, universities and practice education providers could put external programmes in place and create external practice environments that promote the internal resilience of health professional students.
As health professional students transition through placement into the professional workplace, they draw on these resources in developing coping strategies that assist them to overcome challenges and mitigate the effect of stressors
The relationship between listening and interpersonal communication skills and resilience in health professions students has to date not been formally investigated. The findings will assist academic and fieldwork educators in identifying core focal areas to inform the design of evidence-based curricula and learning environments that promote resilience in occupational therapy students.
Method
Design
A self-report survey design was used to collect data for the project. A convenience sampling method was used to recruit participants.
Participants
The participants comprised 135 third- and fourth-year occupational therapy students enrolled in the 4-year Bachelor of Occupational Therapy (Honours) course at Monash University – Peninsula Campus, Frankston, Victoria, Australia.
Instrumentation
Demographic data were collected via a paper-based self-report questionnaire, and data on students’ listening and interpersonal communication skills and their levels of resilience were generated from five standardised self-report measures: the Listening Styles Profile – Revised (LSP-R) (Bodie et al., 2013), Active-Empathetic Listening Scale (AELS) (Bodie, 2011), Interpersonal Communication Competence Scale (ICCS) (Rubin and Martin, 1994), Resilience at University (RAU) scale (Turner et al., 2017) and the Resilience Scale in Adults (RSA) (Friborg et al., 2005).
The LSP-R is the most widely used self-report listening instrument in communication research and has established internal consistency and latent variable test–retest correlations (Bodie et al., 2013). This self-administered instrument assesses an individual’s preferred listening style based on respondents’ rating of 24 items on a seven-point Likert scale. The LSP-R identifies four types of listening style: Relational, Analytical, Task-Oriented and Critical Listening.
The AELS measures the active and emotional involvement of a listener across three key stages of the listening process: sensing, processing and responding (Bodie et al., 2013). Respondents’ performance in each stage is assessed by their agreement with 11 statements using a seven-point Likert scale. Example items include ‘I am sensitive to what others are not saying’ (sensing), ‘I summarise points of agreement and disagreement when appropriate’ (processing) and ‘I ask questions that show my understanding of others’ position’ (responding). The instrument has reported construct validity (Bodie, 2011).
The ICCS identifies competencies across 10 domains of interpersonal relationships: self-disclosure, empathy, social relaxation, assertiveness, interaction management, altercentricism, expressiveness, supportiveness, immediacy and environmental control (Rubin and Martin, 1994). Participants rate 30 items on a five-point Likert scale. The scale has established reliability and concurrent validity.
The RAU measures seven aspects of resilience in university students: find your calling, living authentically, interacting cooperatively, managing stress, building networks, maintaining perspective and staying healthy. Respondents rate their agreement of 19 items on a seven-point Likert scale. For the purposes of this study, interacting cooperatively was incorporated into the living authentically scale. The instrument has reported satisfactory convergent and discriminant validity and good internal consistency reliability with a Cronbach’s alpha coefficient of .81, where .70 or above is considered adequate (Turner et al., 2017).
The RSA examines intrapersonal and interpersonal protective factors that facilitate adaptation to psychosocial adversities. The instrument comprises 33 items that participants rate on a seven-point Likert scale and responses load to six factors: personal strength/perception of self, planned future, social competence, structured style, family cohesion and social resources. The instrument has proven internal consistency and its construct validity is supported (Hjemdal et al., 2011).
Data management and analysis
The Statistical Package for the Social Sciences (SPSS), version 20, for Windows, was used for data entry, storage and analysis. The RAU and RSA subscale scores were correlated with the LSP, AELS and ICCS subscale scores using Spearman rho correlations. Multi-linear regression analyses were completed to determine if aspects of listening and communication were significant predictors of resilience in the sample population. An independent variable was only included in the regression analysis if it was significantly correlated with the dependent variable.
Preliminary analyses were completed to ensure there were no violations of the assumptions of normality, linearity, multicollinearity and homoscedasticity. A resampling technique, ‘bootstrapping’, a type of robust statistic that infers a population from sample data, was used (Chernick, 2007). By taking, with replacement, the values from the original sample to obtain 1000 bootstrapped samples, the accuracy of the confidence interval (CI) estimation can be improved. Results were considered statistically significant at the 0.05 alpha level.
Procedures
Ethics approval for the project was obtained from the Monash University Human Research Ethics Committee (MUHREC) (Project Number: CF15/12823). Respondents were informed of the purpose of the study, the voluntary nature of their participation and of the procedures to ensure their anonymity in all published outputs. Students were asked to complete a questionnaire containing demographic questions, the LSP-R, AELS, ICCS, RAU and RSA. The questionnaire took approximately 20 minutes to complete and consent on the part of the students was implied by its completion and return. No data were identifiable.
Results
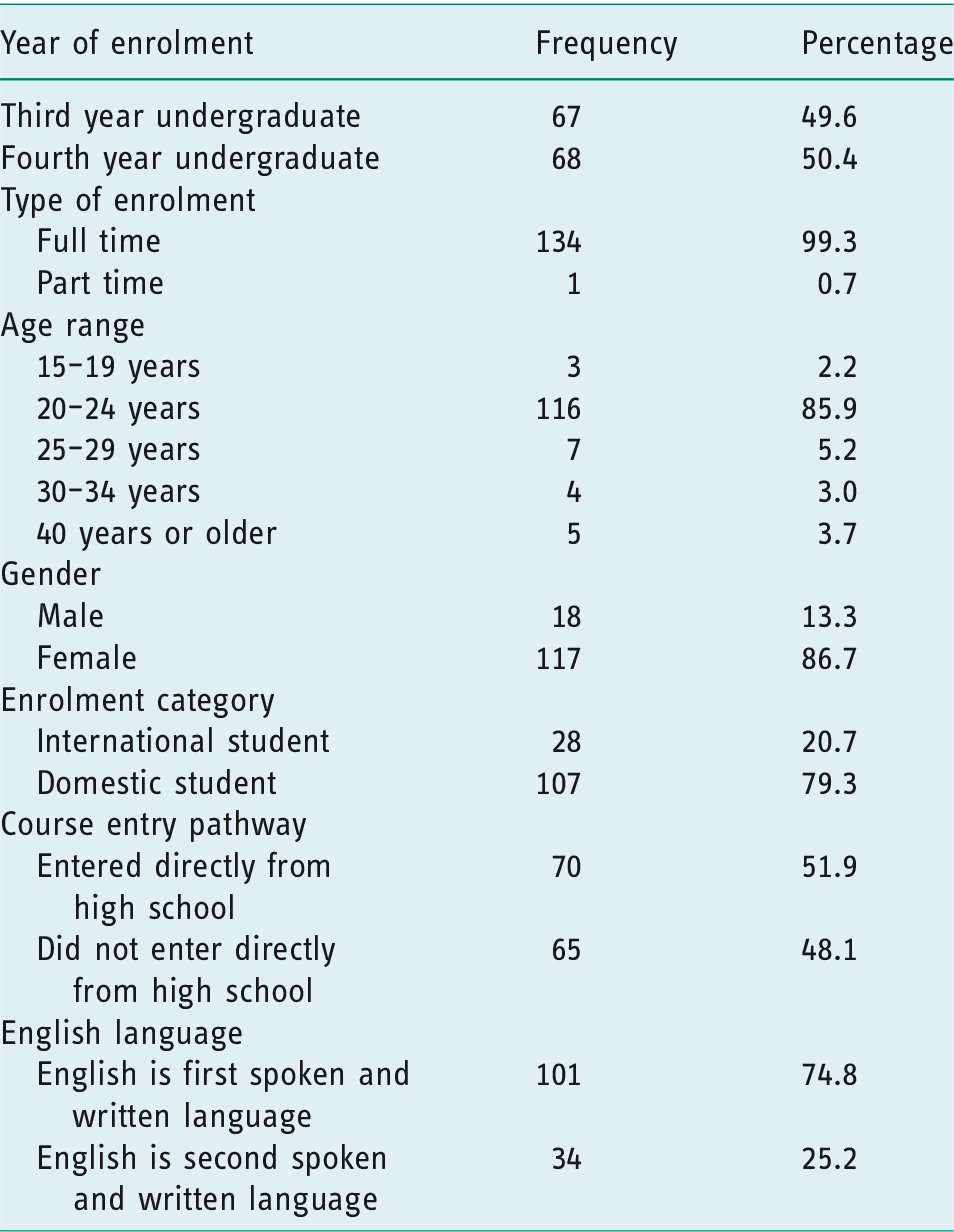
The full demographic findings are reported in Table 1. The sample of third- and fourth-year undergraduate students was predominantly female, enrolled full-time and aged 20–24 years. The majority had English as their first language and were classified as domestic students.
Demographic data (n = 135).
Scores across the subscales of the resilience instruments were in the upper range, with the highest performances recorded on the measures of find your calling (M 2.49; SD 3.72), living authentically (M 27.66; SD 4.18), social resources (M 41.47; SD 7.90) and planned future (M 20.90; SD 4.81). Performances on the LSP-R and AELS listening subscales were consistently high, as were scores recorded on the 10 interpersonal communication domains of the ICCS. The full mean scores are provided in Table 2.
RAU, RSA, LSP, AELS and ICCS comparative mean scores (n = 135).
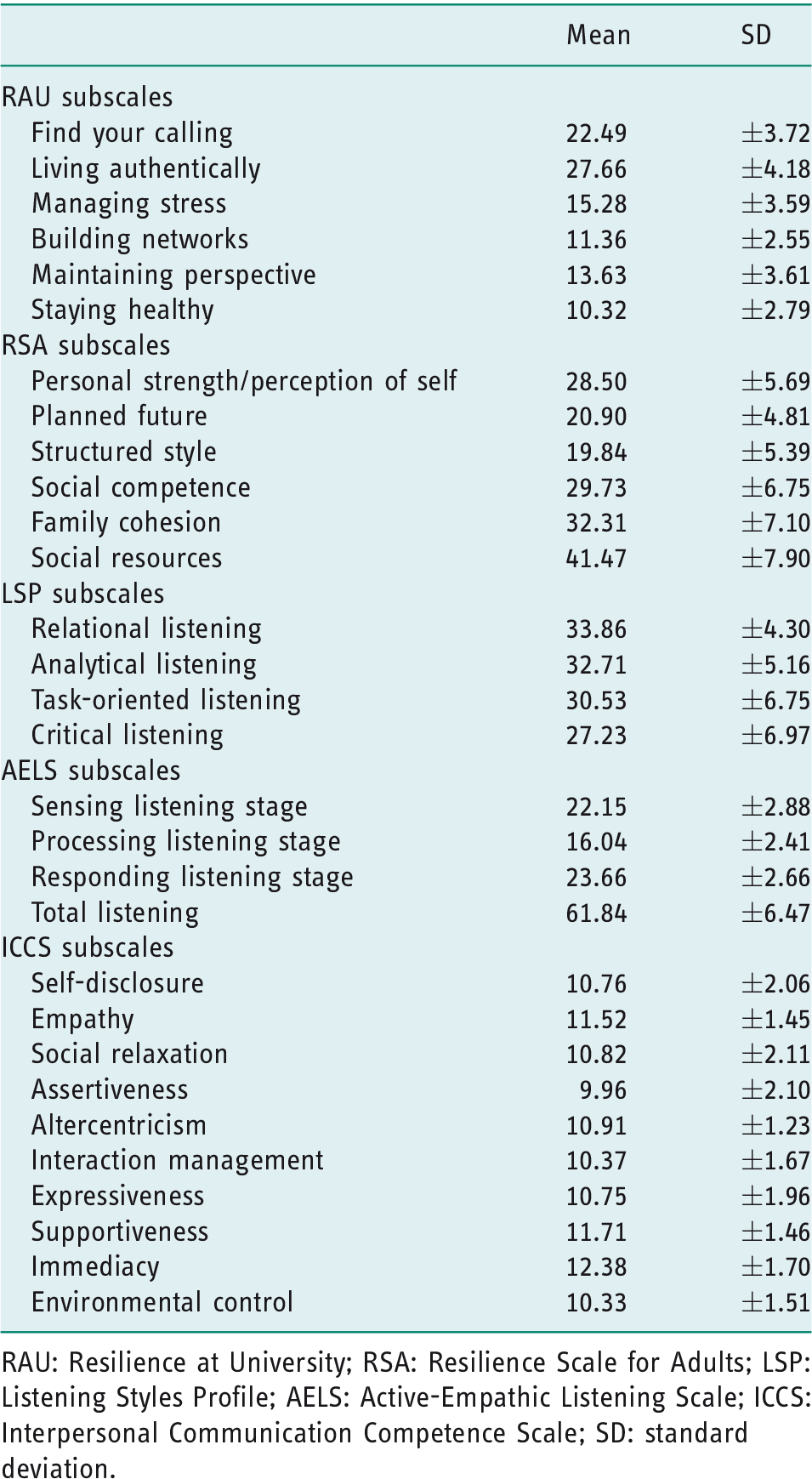
RAU: Resilience at University; RSA: Resilience Scale for Adults; LSP: Listening Styles Profile; AELS: Active-Empathic Listening Scale; ICCS: Interpersonal Communication Competence Scale; SD: standard deviation.
Regression analysis was completed focusing on the 12 dependent resilience variables: find your calling, living authentically, managing stress, building networks, maintaining perspective, staying healthy, personal strength/perception of self, planned future, structured style, social competence, family cohesion and social resources. Nine regression models were significant predictors of resilience in the current sample. See Table 3 for full regression statistics.
Linear regression analysis between RAU/RSA scores and LSP, AELS and ICCS subscales (n = 135; bootstrapped sample of 1000).

RAU: Resilience At University; RSA: Resilience Scale for Adults; LSP: Listening Styles Profile; AELS: Active-Empathic Listening Scale; ICCS: Interpersonal Communication Competence Scale; Constant: y-intercepts of regression line; B: unstandardised beta coefficient; SE B: standard error for the unstandardised beta; β: standardised beta; t: the t test statistic; p: probability statistic; CI: confidence interval; LL: lower limit; UL: upper limit; BCa: bias-corrected and accelerated.
Results considered statistically significant at the 0.05 alpha level: statistically significant independent variables denoted in
B remained unchanged after bootstrapping.
Bootstrapping specifications: (a) sampling method – simple; (b) # of samples – 1000; (c) CI level – 95%; and (d) CI type – BCa.
R = .375; R square = .141; adjusted R square = .093.
R = .468; R square = .219; adjusted R square = .156.
R = .322; R square = .104; adjusted R square = .076.
R = .415; R square = .172; adjusted R square = .119.
R = .255; R square = .065; adjusted R square = .051.
R = .230; R square = .053; adjusted R square = .031.
R = .394 R square = .155; adjusted R square = .116.
R = .364; R square = .133; adjusted R square = .092.
R = .282; R square = .080; adjusted R square = .044.
R = .518 R square = .268; adjusted R square = .222.
R = .172; R square = .029; adjusted R square = .015.
R = .409; R square = .167; adjusted R square = .122.
Find your calling
The model, comprising seven independent variables from the AELS, LSP-R and ICCS, uniquely explained 9.3% of the find your calling score (adjusted R2 = .093, F(7, 127) = 2.967, p = .006 BCa 95% CI [1.281, 15.615], based on 1000 bootstrap samples). One independent variable made a unique contribution to overall variance: sensing listening (5.0%, p = .009, BCa 95% CI [.087, .591]) based on 1000 bootstrap samples.
Living authentically
The model comprised 10 independent variables from the AELS and ICCS that together uniquely explained 15.6% of the living authentically score (adjusted R2 = .156, F(10, 124) = 3.479, p = .000, BCa 95% CI [4.172, 20.333], based on 1000 bootstrap samples). One independent variable made a unique contribution to overall variance: sensing listening (4.3%, p = .011, BCa 95% CI [.0114, .728]) based on 1000 bootstrap samples.
Managing stress
The model, comprising four independent variables from the LSP and ICCS, uniquely explained 7.6% of the managing stress score (adjusted R2 = .076, F(4, 130) = 3.762, p = .006, BCa 95% CI [−.257, 10.273], based on 1000 bootstrap samples). One independent variable made a unique contribution to overall variance: analytical listening (4.4%, p = .022, BCa 95% CI [.018, .265]) based on 1000 bootstrap samples.
Maintaining perspective
The model, comprising two independent variables from the LSP and ICCS, uniquely explained 5.1% of the maintaining perspective score (adjusted R2 = .051, F(2, 132) = 4.603, p = .012, BCa 95% CI [1.766, 11.213], based on 1000 bootstrap samples). Both independent variables made a unique contribution to overall variance: analytical listening (2.7%, p = .038, BCa 95% CI [.015, .215]) and self-disclosure (3.6%, p = .035, BCa 95% CI [.044, .651]) based on 1000 bootstrap samples
Personal strength/perception of self
The model, comprising six independent variables from the ICCS, uniquely explained 11.6% of the personal strength/perception of self score (adjusted R2 = .116, F(6, 128) = 3.923, p = .001, BCa 95% CI [4.376, 23.628], based on 1000 bootstrap samples). No independent variable made a unique contribution to overall variance.
Planned future
The model comprised six independent variables from the ICCS and uniquely explained 9.2% of the planned future score (adjusted R2 = .092, F(6, 128) = 3.264, p = .005, BCa 95% CI [6.372, 33.566], based on 1000 bootstrap samples). One independent variable made a unique contribution to overall variance: self-disclosure (3.4%, p = .047, BCa 95% CI [.014, 1.396]) based on 1000 bootstrap samples.
Structured style
The model comprised five independent variables from the ICCS and uniquely explained 4.4% of the structured style score (adjusted R2 = .044, F(5, 129) = 2.229, p = .055, BCa 95% CI [7.317, 22.037], based on 1000 bootstrap samples). The independent variables were not statistically significant.
Social competence
The model comprised eight independent variables from the LSP-R, AELS and ICCS, and uniquely explained 22.2% of the social competence score (adjusted R2 = .222, F(8, 126) = 5.771, p = .000, BCa 95% CI [−4.216, 23.000], based on 1000 bootstrap samples). One independent variable made a unique contribution to overall variance: social relaxation (8.5%, p = .001, BCa 95% CI [.584, 1.659]) based on 1000 bootstrap samples.
Social resources
The model comprised seven independent variables from the AELS and ICCS, and uniquely explained 12.2% of the social resources score (adjusted R2 = .122, F(7, 127) = 3.649, p = .001, BCa 95% CI [3.607, 39.802], based on 1000 bootstrap samples). One independent variable made a unique contribution to overall variance: self-disclosure (6.7%, p = .003, BCa 95% CI [.514, 2.460]) based on 1000 bootstrap samples.
Discussion
Students performed well on the LSP-R relational, analytical and transactional listening scales and recorded good to very good mean scores in the active-empathic listening domains of sensing, processing and responding. Moderate to high scores were observed across the ICCS interpersonal communication scales, students performing especially well on measures of empathy, supportiveness and immediacy. These results indicate strong coping mechanisms in the sample of occupational therapy students, with notable scores recorded on the vocational, attitudinal and support-related resilience scales. This contrasts with reports of the difficulties experienced by medical students in the clinical setting, predominantly related to poor team dynamics, which lead to increased stress and negative impact on wellbeing among students (Houpy et al., 2017).
While these results represent an encouraging finding for allied health educators, the mean scores should be viewed in the context of the demographic profile of the sample in which females (87%), 20–24-year-olds (88%) and third (50%) and fourth-year (50%) students predominated. The influence of gender is well documented, with studies showing that females are consistently associated with better academic outcomes (Watson, 2013). In their third and fourth years of study students undertake practice education placements, during which they are exposed to the realities of interacting with colleagues and patients. Learning to communicate effectively with co-workers within different settings and with patients from diverse backgrounds represents a challenging stage in the formation of students’ professional self-identity. Research suggests that female occupational therapy students are more confident and motivated in overcoming personal challenges than their male counterparts and use opportunities afforded by practice placements to develop core attributes of listening and communication in the health setting, such as clinical reasoning and relational skills (Seah et al., 2011). It may also be the case that as students in their final years of study, their prior academic experience has equipped them with the independent learning, reflective practice and group work skills to drive proficiencies in active listening and interpersonal communication that serve to strengthen coping mechanisms, as reflected in students’ performance on the resilience scales.
Regression analysis produced several key findings, foremost of which were the associations observed between the sensing and analytical listening styles and vocational and strategic aspects of resilience (finding your calling, living authentically, managing stress and maintaining perspective). Further significant findings were establishing the interpersonal communication variables, self-disclosure and social relaxation, as significant predictors of social resilience (social relaxation) and identifying self-disclosure as a predictor of attitudinal resilience-enhancing factors (maintaining perspective and planned future).
Factors of listening that build resilience
Investigation of students’ performance on the sensing listening scale in relation to measures of resilience yielded particularly useful insights into the benefits of an active-empathic listening style as a facilitator of vocational resilience factors. The caring professions are characterised by health professionals who are driven by a desire to deploy their skills and knowledge to assist patients and clients in need of clinical and therapeutic treatment; many students in the health professions education sector therefore experience a strong vocational calling. Deriving satisfaction in one’s chosen discipline and finding authenticity in one’s study path and career are prevalent features within occupational therapy. According to Wood (2016), it is a profession that will attract those who believe in ‘fiduciary responsibility’ in which upholding the needs of clients and society and placing the wellbeing of the people and groups they serve takes precedent over self-interest. It is possible to deduce that listening with sensitivity allied to an open disposition, a willingness to share feelings and an ability to engage with clients and co-workers empowers students’ core values and facilitates their emerging professional identity.
Important components of self-identity in allied health students are an acute sensitivity to the emotional needs of a patient or client in which the practitioner attends to the implicit and explicit aspects of a speaker’s message. This may include an awareness of what is implied but not stated, understanding how others feel, and recognising non-verbal cues and dispositions such as facial expressions, illustrative gestures, vocal modulation and posture shifts (Rubin and Martin, 1994). In developing and employing their empathic, intuitive and listening skills, it is suggested that students experience authenticity in their interactions with patients and colleagues that strengthens their sense of belonging and a perception they are undertaking work that fits with their core values and beliefs; in other words, vocational fulfilment.
Research has illustrated the benefits of empathic, attentive and non-judgemental listener–speaker interactions for improving the clarity of information imparted, resulting in reduced anxiety levels and heightened feelings of professional authenticity and wellbeing in healthcare professionals (Itzchakov et al., 2018). The evidence is that students who respond and express themselves in a considered, sensitive manner also experience improved interactions and supportive communications with colleagues (McDonald et al., 2013).
Identifying the predictive value of a highly attuned empathic listening style in relation to the living authentically resilience scale suggests that intuition and openness are key facets in contributing to student wellbeing in the university environment. It also indicates that knowing one’s personal strengths and using them regularly, twinned with a belief in providing help to peers and not being afraid to ask for feedback, promotes key aspects of resilience such as collegiality, adaptability and flexibility. Within the therapeutic health disciplines, these elements are essential for building engagement and feelings of connection, mutuality and trust that assist in determining treatment goals.
The finding that an analytical listening style was positively associated with resilience factors indicates that it may act as a stabilising influence, enabling students to manage and overcome the stresses and strains of university life by facilitating them to maintain a sense of perspective and empowering their stress management capabilities. Analytical listening is characterised by a tendency to wait for all the facts to be presented and consideration of all sides of an issue before forming a judgement; in other words, engaging in systematic thinking in which content informs decision-making (Bodie et al., 2013). This cool and level-headed approach is particularly important within the context of allied health, where practitioners are often confronted with challenging interactions yet are required to implement considered and well-thought-out care and treatment plans. Analytical listening is especially relevant in occupational therapy practice, where rehabilitation and the requirement for clients to undertake specific exercises necessitates the delivery of information and instructions in ways that clients understand and are prepared to commit to.
The benefits of analytical listening are highlighted in studies of medical students that identified an association between full engagement, where the student attends to the full message of the speaker before making a judgement, and lower incidences of burn out and fewer depressive symptoms (Thompson et al., 2016). The benefits of engaged listening for students’ mental health has been observed in occupational therapy students working in a variety of practice education settings, in whom wellbeing and self-care are recognised as integral components of ‘professional resilience’ (Ashby et al., 2013). This is contingent with students’ performance on the managing stress and maintaining perspective resilience scales, which suggests students have reliable ways to relax when under pressure, take frequent breaks from study to maintain their strength and energy, and are not fazed for long by adverse events.
Establishing a positive correlation between sensing and analytical listening styles and resilience factors suggests that open, sensitive, considered and systematic listening instils in students an inner strength that reduces their vulnerability to occupational stressors and assists in the management of stress levels.
Factors of interpersonal communication that build resilience
The interpersonal communication variables, self-disclosure and social relaxation, were found to be significant predictors of resilience in the sample group. The strong association observed between self-disclosure and the resilience factor of social resources highlights the central role of social elements in developing resilience. The availability of social support, the appreciation and encouragement of family and friends, and a willingness to seek external help if needed are important support mechanisms for health professions students, who will frequently encounter and experience stressful clinical events during training. This is borne out in studies from the nursing and medical arenas, which suggest that students perceive the clinical education process as a stressful experience, leading to feelings of anxiety, fatigue and lack of motivation (Sanderson and Brewer, 2017; Wood, 2016). The detrimental effect this has on course retention rates through burnout and emotional exhaustion represents a serious concern for educators. The evidence, however, is that the effects of stressful events are mitigated in those students who receive encouragement from their family and peers, which, allied with support from faculty and academic supervisors, enhances resilience and wellbeing (Mansfield et al., 2016). Social supports for occupational therapy students could also be contextualised within an occupational perspective on health and wellbeing since some of these social factors (for example relaxation, social support systems) can also be viewed as occupational factors. They provide supporting evidence for the potential resilience-enhancing role of occupations as proposed by an occupational perspective of health and wellbeing. The social aspects of the environment are mentioned in the Canadian Model of Occupational Performance and Engagement (Polatajko et al., 2007), the Occupational Therapy Practice Framework – third edition published by the American Occupational Therapy Association (2014), and the work of Wilcock and Hocking (2015) on an occupational perspective on health.
This finding is augmented by the positive association observed between the interpersonal attribute, social relaxation, and the resilience-promoting factor, social competence. While this is not an entirely unexpected outcome, it serves to demonstrate the benefits of finding time outside of studies to relax with friends in countering the stresses and strains of pre-professional training. The benefits of personal and social competences that facilitate students to manage stress, maintain perspective and interact cooperatively are particularly important for pre-qualified occupational therapists, who are often working within interprofessional teams and are at risk of professional isolation.
Social competencies such as flexibility, the ability to form friendships and working relationships, and the positive use of humour are recognised as core components in building resilience (Friborg et al., 2005). In the current study, the attributes of approachability and satisfaction gained from fostering close personal and working alliances are reflected in the high scores recorded on other measures of interpersonal communication including self-disclosure, expressiveness, supportiveness and immediacy.
Regression analysis also revealed self-disclosure to be a significant predictor of students’ ability to maintain a sense of perspective when things go wrong. For students undertaking practice placements across a range of diverse settings, learning how to reframe setbacks, maintain focus on a solution and manage negativity are essential attributes in countering challenges, at both the clinical and interpersonal levels. It is important to acknowledge, however, that disclosure is only effective if it achieves the desired goal of promoting self-expression and developing the therapeutic/clinical relationship – in this regard, it aligns closely to the notion of resilience by facilitating confidence in decision-making and interacting with colleagues and clients.
Identifying self-disclosure as a predictor of clarity and direction regarding career choices (planned future) in the sample group indicates that attitudinal facets such as an ability to plan ahead, maintain a positive outlook and be goal-oriented in one’s objectives represent positive resources that enhance resilience in students.
The findings of this study establish the predictive value of aspects of listening and interpersonal communication in relation to resilience and will improve academic and fieldwork educators’ understanding of resiliency in students. More specifically, the outcomes will inform the design of teaching and learning activities and materials that can be used by occupational therapy academic staff and practice educators to improve students’ preparation and orientation prior to placements. The findings will be disseminated through educational initiatives such as role-play exercises, group work skills and critical self-reflective tasks that optimise opportunities for students to acquire the listening and interpersonal communication skills that strengthen resilience capacities. Likewise, considering the social ecology of resilience perspective, academic and fieldwork educators can create learning environments that promote resilient behaviours in students.
Study limitations
Limitations associated with this study include the convenience sampling approach used for recruitment and data generation purposes. As the participants were recruited from a single education programme, generalisability of the findings is limited. It was not possible to obtain data on non-respondents to the self-report questionnaire for confidentiality and ethical reasons. Since the self-report scales were used to gather the data for this study, the issue of bias reporting related to social desirability also needs to be considered.
Finally, the link between listening and interpersonal communication skills and resilience in occupational therapy students could potentially be bi-directional. In other words, listening and interpersonal communication skills (as measured by the AELS, LSP-R and ICCS) could be the dependent variables and resilience (as measured by the RAU and RSA) could be the independent variable. It is possible that resilience as a trait could be an influencing or contributing factor towards students’ listening and interpersonal skills. However, in the context of the current study, whether listening and interpersonal communication skills were predictive factors contributing to occupational therapy students’ resilience was investigated.
Future research
Further investigation in this area of teaching and learning research is recommended to replicate the findings of the current study and generate new insights that add to the knowledge base on the relationship between listening and communication skills and resilience in allied health students. The generation of longitudinal data that track changes in students’ listening and communication skills and investigation of their impact on resilience levels and coping mechanisms may identify other predictors of resilience that can be used to further inform curricula design. Finally, whether resilience in health professional students is predictive of listening and interpersonal communication skills could be investigated to determine empirically if a bi-directional relationship exists between these two sets of variables.
Conclusion
The key findings demonstrated that components of listening and interpersonal communication are positively related to occupational students’ resilience levels. The results indicate that the measurement of listening and interpersonal communication capabilities may be a useful predictive tool for resilience and a basis for improving curricula to promote resilience in occupational therapy students as part of the continuum of pre-professional training. The outcomes will assist academic and fieldwork educators to meet the challenge of preparing graduates with highly attuned listening and communication skills to successfully complete course programmes and function effectively as members of inter-disciplinary teams across a variety of settings, and who are equipped with effective resilience and coping strategies to enable them to thrive and survive in their future careers. Occupational therapy academic and fieldwork educators are encouraged to consider features of the clinical learning environments that promote resilience in students, and this can inform curriculum planning and the continuing professional development provided for fieldwork educators.
Key findings
Competencies in sensing and analytical listening were predictive of vocational and strategic aspects of resilience in students. The interpersonal communication variables self-disclosure and social relaxation were significant predictors of students’ social and attitudinal resilience.
What the study has added
Listening and interpersonal communication competencies in occupational therapy students are directly associated with their resilience. Educators are encouraged to consider internal and external factors to the student to promote resilience.
Footnotes
Research ethics
Ethics approval for the project was obtained from the Monash University Human Research Ethics Committee (MUHREC) (Project Number: CF15/12823) in 2018.
Consent
Written informed consent was obtained from all study participants for their responses to the Active-Empathetic Listening Scale, Listening Styles Profile-Revised, Interpersonal Communication Competence Scale, Resilience at University and Resilience Scale for Adults instruments to be included, analysed and reported in a de-identified, combined manner in the current study.
Declaration of conflicting interests
The authors confirm that there is no conflict of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors disclose receipt of the following financial support for the research and publication of this article: The study was funded through a grant received from the Monash Education Academy – Learning and Teaching 2018 Small Grants Scheme, Monash University – Peninsula Campus, Victoria, Australia. The funding received covered the salary costs of a research assistant who helped with the data collection and data entry.
Contributorship
Ted Brown and Mong-lin Yu researched literature, applied for ethical approval and contributed to the development of the data. All authors contributed to the methodology of the project and the statistical analysis plan. Ted Brown carried out the statistical analysis. All authors interpreted the data analysis results and contributed to writing the manuscript. Likewise, all authors reviewed and edited the manuscript and approved the final version.