
Abstract
Introduction
The purpose of this research was to describe participation restrictions in younger and older adult cancer survivors post treatment.
Method
Younger adult cancer survivors (n = 20) and older adult cancer survivors (n = 21) completed questionnaires and a semi-structured interview of satisfaction with daily life activities and self-reported health outcomes in a single visit. Reports were based on recall during treatment and current perspectives post treatment.
Results
Despite general health short forms revealing health within normal limits, semi-structured interview approaches revealed dissatisfaction with occupational performance in both younger and older adult cancer survivors. Older adults reported persistent dissatisfaction with instrumental activities from diagnosis through post treatment compared to younger adult cancer survivors. Older adults received fewer referrals for cancer rehabilitation services (19%) compared to younger adult cancer survivors (50%).
Conclusion
Dissatisfaction with daily life activities persists several years post cancer diagnosis in older and younger adult cancer survivors, despite self-reported health within normal limits. Impairment-based short forms may lack sensitivity to detect activity limitations and participation restrictions conveyed through in-depth assessment. Adoption of more comprehensive screening methods may be needed for timely referral to cancer-based occupational therapy services.
Introduction
There have been multiple calls-to-action to better understand the nature and magnitude of disability in cancer populations (Alfano and Pergolotti, 2018; Newman et al., 2019b). The World Health Organization’s International Classification of Functioning, Disability, and Health describes disability as a multifactorial construct among body structures and function, activities and participation, and contextual factors (World Health Organization, 2001). While characterization of cancer-related disability has been investigated in terms of impairment-focused outcomes (Newman et al., 2019b), few studies document implications of cancer and cancer treatment on other domains, including participation restrictions (Hunter et al., 2017).
In order for occupational therapy practitioners to appropriately treat occupational performance deficits, we must have a better understanding of how participation restrictions manifest in a variety of cancer populations and at different points in the cancer care continuum. The cancer care continuum refers to all phases of illness from diagnosis to the end of life (National Cancer Institute, 2019a). Comprehensive occupational therapy prioritizes improved participation (American Occupational Therapy Association, 2014). Without knowledge of how participation is impacted by the cancer experience, we run the risk of having poor targets for intervention development, and/or ineffective or imprecise outcomes (for example social isolation, sedentary behavior, recurrence, chronic symptoms) (Newman et al., 2019b).
A key tenet of occupational therapy intervention is client-centered care (American Occupational Therapy Association, 2014). Client-centered care is influenced by many factors such as age, type of occupational performance deficit, and impact of health condition. The age of a person and stage of recovery in the cancer care continuum influence a client’s cancer experience and occupational performance (Baxter et al., 2017; Lyons et al., 2017). Understanding how participation restrictions differ or coincide across populations (for example younger versus older adults) as well as time since diagnosis (for example acute treatment, post treatment, long-term survivorship, palliative care) may alter the way in which occupational therapists prescribe services and intervene. Currently, there are limited published articles detailing participation restrictions during acute cancer treatment (Lyons et al., 2013) and in younger populations (Lyons et al., 2012). There is limited evidence discussing changes in disability long-term and in older populations. This knowledge is important as there is a substantive increase in post-treatment survivorship; most survivors are living past 5- and 10-year benchmarks (American Cancer Society, 2018). By 2040, it is predicted that 70% of cancer survivors will be over the age of 65 years (Bluethmann et al., 2016). Furthermore, a better understanding of changes in activity engagement throughout adulthood and at various points across the cancer care continuum are warranted.
This study explored the prevalence of participation restrictions and functional wellbeing in younger adult and older adult cancer survivors who were all post treatment. The primary aim of this cross-sectional study was to examine the impact of cancer on daily life activities based on recall of activities during treatment and current experiences post treatment. The secondary aim was to explore self-reported health outcomes with a semi-structured assessment of satisfaction regarding participation in daily life activities.
Method
Recruitment procedures
To ensure inclusion of a heterogenous sample of various diagnoses and time since treatment, two groups of participants were recruited: younger adult cancer survivors and older adult cancer survivors. For this descriptive study, a cancer survivor was defined as an “individual … from the time of diagnosis until end of life” (National Cancer Institute, 2019b). Younger adult cancer survivors were included if they had a previous diagnosis of cancer, were between the ages of 30 and 64 years, community-dwelling, English speaking, and lived within 50 miles of the university. Older adult cancer survivors were included if they had a previous diagnosis of cancer, were 65 years or older, community-dwelling, English speaking, and lived within 50 miles of the university. Individuals were excluded if they had a sole diagnosis of basal cell carcinoma. Cancer survivors were recruited through three methods: (a) recruitment flyers; (b) recruitment presentations at cancer-specific community support groups and local senior community centers; and (c) a university-based research registry.
Interested participants completed a detailed phone screening with the principal investigator to ensure eligibility criteria. Eligible participants then scheduled an appointment to complete informed consent. If the participant consented, they completed the Older Americans Resources and Services (OARS) Comorbidity questionnaire (Fillenbaum and Smyer, 1981) and an assessment battery (Table 1) in their home or a university laboratory space. Participants were provided US$10 for completing the assessment and compensation for parking. Ethical approval of this study was provided by the University Institutional Review Board.
Assessments.
Instruments
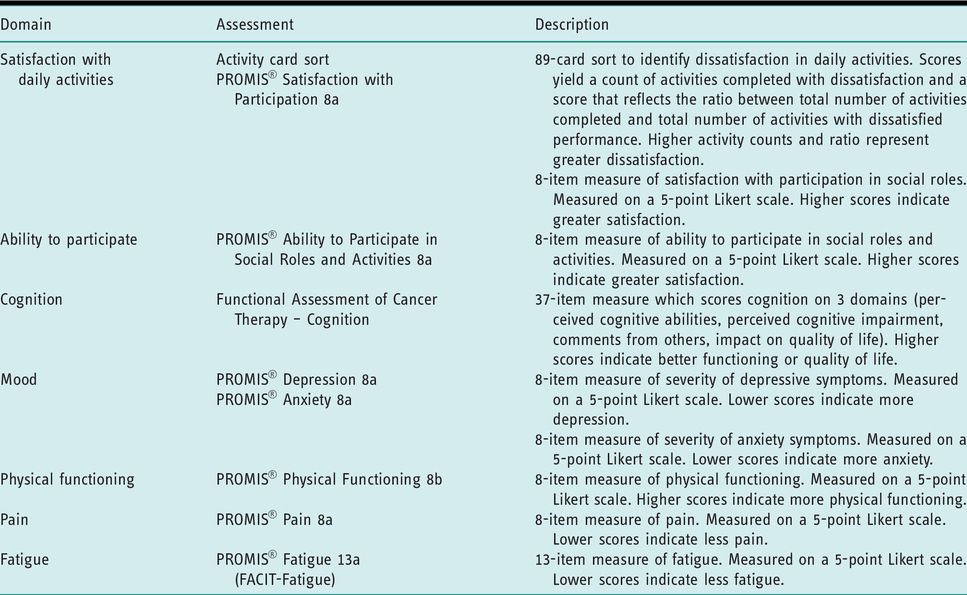
Table 1 describes the assessments and scoring used to examine the primary and secondary research questions, and to characterize the sample.
Participation restrictions
A modified version of the Activity Sort Card (ACS) (Baum and Edwards, 2001) was used to identify satisfaction with performance in activities through retrospective recall of experiences during primary cancer treatment, and through current experiences post treatment. Permission to use the administration and interpretation of the tool in the manner described was provided by one of the primary authors of the ACS (C. Baum, personal communication, February 26, 2019). Four categories of activities were represented: (a) instrumental activities of daily living (for example cooking meals, shopping, or car maintenance); (b) high physical demand leisure (for example tennis, woodworking, camping); (c) low physical demand leisure (for example knitting, reading, bird watching); and (d) social activities (for example entertaining, eating at a restaurant). To describe satisfaction with activities during the cancer experience, participants initially sorted the 89 activity cards into categories of (a) never done prior to cancer diagnosis; and (b) done prior to cancer diagnosis. Activities sorted as “done prior to cancer diagnosis” were then resorted into “satisfied with performance” and “dissatisfied with performance” to reflect level of satisfaction in the activities during cancer treatment. To reflect a survivor’s current satisfaction with activity performance, cards were resorted following similar steps: (a) initial sort compared activities they currently do and don’t do; and (b) of the activities they currently do, with which are they satisfied and dissatisfied with their performance. The ACS yields a count of activities completed during cancer treatment and currently. The sorts also reflect a ratio between total activities completed and total number of activities with dissatisfied performance. Higher activity counts and larger ratios represent greater dissatisfaction in performance of daily activities. Other variations of the ACS have been studied and used to characterize changes in activity engagement in cancer populations (Fleischer and Howell, 2017; Lyons et al., 2010, 2019; Newman et al., 2019a). The tool has demonstrated strong internal consistency (α > 0.86) and is significantly associated with quality of life, performance status, and functional wellbeing (Lyons et al., 2010).
Self-reported health
Multiple Patient-Reported Outcome Measurement Information System (PROMIS®) general population short forms were used to evaluate current perceived health in the following domains: mood (anxiety, depression), pain, physical function, ability to participate in social roles, satisfaction with participation in social roles, and fatigue. Each of the selected PROMIS® measures has undergone extensive psychometric analysis (Reeve et al., 2007) and has been previously used to measure health and screen for impairments in cancer populations (Wagner et al., 2015). PROMIS® measure scores are interpreted as T-scores, with an average score of 50 and standard deviation of 10. We measured the domain of cognition using the Functional Assessment of Cancer Therapy – Cognition (FACT-Cog) (Wagner et al., 2009). This commonly used self-report questionnaire (Van Dyk et al., 2019) was validated in cancer populations to measure perceived cognitive abilities, perceived cognitive impairments, comments from others regarding cognition, and impact on quality of life (Wagner et al., 2009). The (FACT-Cog) was developed specifically to assess self-reported cognitive difficulties in cancer survivors, and is regularly administered in observational studies (Van Dyk et al., 2019). For this reason we used this measure to augment the PROMIS measures of self-reported outcomes in other domains. Higher scores represent better functioning or quality of life. For simplification of interpretation, raw scores were transformed into z-scores (Mean = 0, SD = 1). Interpretation of higher versus lower scores is explained in Table 1.
Analysis
Descriptive analyses summarized participant demographic and clinical characteristics. Chi-square, t-test, and non-parametric alternatives were used to compare older adult cancer survivors and younger adult cancer survivors. Normality was evaluated by the Shapiro–Wilk test and visual analysis of box plots. The Wilcoxon signed rank test compared changes in dissatisfaction over time in both younger adult cancer survivor and older adult cancer survivor groups. Given the descriptive nature of the aims, we did not compute a power analysis. Descriptive analyses were completed using SPSS statistical software (IBM SPSS Statistics for Windows, Version 24.0). The significance level was set at .05.
Results
Sample characteristics
The sample is described in Table 2. We recruited 41 participants who had completed primary cancer treatment. Of the 21 older adult cancer survivors, mean age was 73.3 ± 7.2 years old (range 65–91 years), mean education was 15.2 ± 3.3 years, and a higher proportion were female and white. The majority of older adult cancer survivors had previous diagnoses of breast cancer; however, there was a diverse representation of lung, prostate, colon, lymphoma, and thyroid cancers. On average, older adult cancer survivors were 11 years post diagnosis, ranging from 2–40 years. The younger adult cancer survivor group had a mean age of 52.0 ±10.7 years, mean education of 14.7 ± 2.4 years, and were predominantly female, white, and married. The majority of younger adult cancer survivors had previous diagnoses of breast cancer; however, there was a diverse representation of thyroid, lymphoma, uterine, bladder, and head and neck cancers. Overall, the groups were similar in cancer diagnosis, employment, education, and gender. However, there were significant differences between age, marital status, comorbidity, and years since diagnosis between the groups.
Demographic and clinical characteristics of participants (n = 41).

Note: p < .05. Bold variables were significantly different between population groups.
Participants reported whether or not they received cancer rehabilitation services. Cancer rehabilitation was defined as interventions directed at managing impairments, activity limitations, or participation restrictions associated with cancer or cancer-related treatments (Alfano and Pergolotti, 2018). Only 19% (n = 4) of the older adult cancer survivors received a combination of cancer rehabilitation services; 50% (n = 10) of the younger adult cancer survivors received cancer-related rehabilitation services. Of the older adults (n = 4) who received cancer rehabilitation services, two required acute rehabilitation in the forms of mobility groups and post-surgical education. All four older adults reported receiving outpatient therapy for pelvic floor training, debility, lymphedema management, and/or durable medical equipment prescription, and two reported home health rehabilitation for nursing-specific interventions (for example urostomy training). The younger adult survivors reported more opportunities with cancer rehabilitation. Nine of the 10 younger adult survivors received outpatient therapies for general strength and conditioning, lymphedema services, and pelvic floor management. Four younger adults received referrals for physical therapy screenings post-operatively and two participants received home health management from speech language pathology for swallowing and feeding-related impairments.
Dissatisfaction with participation
Table 3 illustrates the medians and ranges of dissatisfaction with various instrumental activities of daily living, leisure, and social activities. During treatment, older adult and younger adult cancer survivors recalled experiencing the greatest dissatisfaction with performance in high demand leisure activities (for example exercise, sports, camping): 45% and 50% respectively. Interestingly, both younger and older adult survivors recalled a great range of dissatisfaction with performance when receiving cancer treatments.
Dissatisfaction with daily life activities – Activity card sort results.
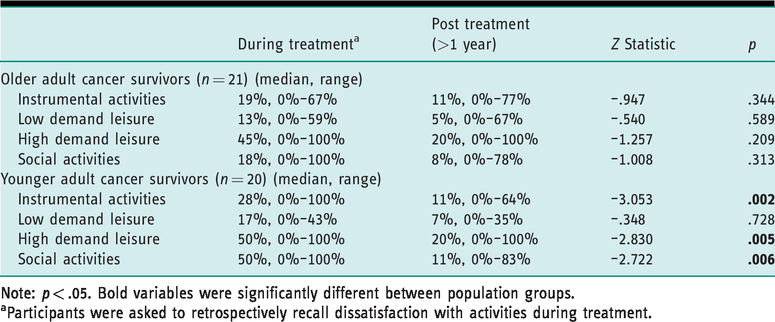
Note: p < .05. Bold variables were significantly different between population groups.
aParticipants were asked to retrospectively recall dissatisfaction with activities during treatment.
Dissatisfaction with daily life activities was lower but persistent post treatment, in some cases several years post cancer diagnosis. Results of the post-treatment dissatisfaction with activity performance remained variable within each group. A Wilcoxon signed-ranks test indicated that younger adult cancer survivors had significantly reduced post-cancer dissatisfaction with activity performance in instrumental activities of daily living (Z = –3.053, p = .002), high demand leisure (Z = –2.830, p = .005), and social activities (Z = –2.722, p = .006) compared to during treatment. In contrast, dissatisfaction with activity performance persisted and remained statistically similar in older adult cancer survivors during cancer treatment through to their current performance.
Table 4 illustrates the younger and older adult cancer survivors’ current self-reported health through symptom and activity-based questionnaires. The self-reported health questionnaires revealed the cancer survivors’ perceptions of current symptoms to be within normal ranges. In contrast to persistent dissatisfaction with participation seen in the ACS, PROMIS® short forms convey normative responses in participation. There were no significant differences in self-reported short brief measures between younger and older adult cancer survivors.
Current self-reported health (n = 41).
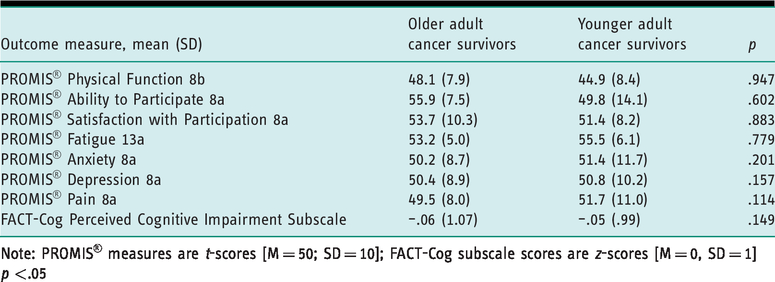
Note: PROMIS® measures are t-scores [M = 50; SD = 10]; FACT-Cog subscale scores are z-scores [M = 0, SD = 1]
p <.05
Discussion and implications
Surprisingly, there are discrepancies in the detection of participation restrictions in older and younger adult cancer survivors based on measurement approach. Despite continued dissatisfaction with occupational performance in various activity domains, general health short forms revealed self-reported health categories within population norms. This presents two interesting points. First, short forms that are typically used as clinical intake screens may lack sensitivity to detect residual impairments and participation restrictions experienced by both younger and older adult cancer survivors post treatment. Second, lack of sensitivity in short forms may be one reason why cancer rehabilitation prescription is under-utilized across all cancer survivors. Thus, we may need to identify and implement more comprehensive screening tactics, such as in-depth interview techniques, in order to detect changes to dissatisfaction and limitations in cancer survivors’ occupational performance.
Conflicting results between clinical short forms and semi-structured interview approaches, like a modified activity card sort, revealed a lack of congruence between impairment-based concerns and sustained occupational performance dissatisfaction. While impairment-driven rehabilitation (Silver et al., 2013) is a common model used in cancer rehabilitation to restore and improve function, rehabilitation practitioners cannot rely on impairment-based screening or intervention to generalize to resumption of roles and routines in daily life. The evidence suggests that changes in impairment-based concerns do not generalize to changes in participation (Newman et al., 2019b). Of the small portion of the study sample that received cancer rehabilitation services, referrals were only linked to impairment-related concerns of mobility, lymphedema management, debility, and swallowing. Despite receiving impairment-based rehabilitation, both younger and older adult cancer survivors continue to express ongoing dissatisfaction in occupational performance. Alfano and Pergolotti (2018) recommended that ongoing cancer survivor assessments should adopt a more comprehensive perspective of function, moving beyond identification of neuromusculoskeletal and cognitive impairments, to identification and treatment of activity limitations and participation restrictions in work and leisure across the cancer care continuum.
Occupational therapy practitioners are uniquely skilled in interview techniques related to occupational performance (American Occupational Therapy Association, 2014). This finding presents an opportunity for occupational therapy practitioners to create and refine existing interview tools to capture ongoing and changing occupational performance concerns in cancer populations. Given that occupational therapy practitioners are also skillful in interview related to occupational performance, occupational therapy practitioners may hold a role in the administration of disability screens within oncology and survivorship clinics.
The results also revealed the magnitude of the impact of cancer on participation restrictions. Performance data revealed that both younger and older adult survivors present a widespread range of dissatisfaction in a variety of instrumental activities of daily living. The sample’s heterogeneity of age, time since diagnosis, and type of diagnosis captured the uniqueness of each cancer survivor’s recovery trajectory. Younger and older adult cancer survivors recalled greatest dissatisfaction in high demand leisure and social activities during cancer treatment. Lyons and colleagues (2013) reported similar results in older adult cancer survivors, who reported an average 12% reduction in activity level, with greater reductions in high physical demand leisure and social activities.
Overall, younger adult cancer survivors had higher median dissatisfaction in all activity domains compared to older adult cancer survivors during cancer treatment. Greater dissatisfaction in activity performance may be explained by younger age. According to Blank and Bellizi (2007), age may serve as a protective factor against cancer-related distress. Younger adults, who are diagnosed at an earlier age compared to the older adult counterparts, face decreased emotional regulation, fewer coping skills, and greater competition between required roles and routines (for example employee, caregiver to children and parents, student, partner, etc.) (Blank and Bellizzi, 2008). In addition, younger age and healthier pre-cancer status may make changes in occupational performance more overt compared to older adults who may have experienced pre-clinical disability or modifications in activity performance prior to cancer treatment (Fried et al., 1991).
While younger adult cancer survivors recalled a significant improvement in activity satisfaction in instrumental activities of daily living, high demand leisure, and social activities over time, older adult cancer survivors reported similar dissatisfaction in recall of activities during treatment and current experiences post treatment. Although not significant, there was a greater proportion of older adults more than 5 years post treatment. Given the small sample size, it is not possible to determine the impact of time since diagnosis on recall of experiences during treatment. Not unlike the current study sample, previous literature reported that nearly 65% of all older adult cancer survivors report persistent occupational performance deficits (Pergolotti et al., 2015). Pergolotti and colleagues later reveal that only 9% of those with reported deficits even received referral to cancer rehabilitation services. Limited cancer rehabilitation referral similarly occurred in the present sample. Without adequate services, older adults may not be able to compensate for cancer-related disability. Limitations in participation can have implications for broader health concerns among cancer survivors (Alfano and Pergolotti, 2018; Alfano et al., 2019). Sustained dissatisfaction may be attributed to other factors as well. Older adult cancer survivors had a greater number of comorbidities that may exacerbate the long-term side effects of cancer and cancer treatment (Bellizzi and Rowland, 2007). Additionally, older adult cancer survivors may have experienced greater dissatisfaction in performance as they had less social support to complete social activities (Yoo et al., 2010), as exemplified by a greater percentage of widowers.
Limitations and future directions
Because this was a cross-sectional study, recall bias may influence reporting of participation restrictions during cancer treatment. In addition, the cross-sectional design does not permit inference about causality between the cancer diagnosis and dissatisfaction with activity performance. Another limitation of the study is homogeneity of race and education. We did not recruit participants who were in the midst of cancer treatment. Thus, participants’ recall of experiences during treatment may be biased, and may not generalize to other samples in active treatment. In addition, varying lengths since diagnosis limit our understanding of evolving change in activity performance satisfaction since diagnosis. Dissatisfaction is one aspect of occupational performance. Changes in participation restriction may also be measured by changes in frequency, type of activity, and difficulty completing an activity. Future analyses may consider collecting information changes in various aspects of participation to capture the constructs’ multidimensionality.
Conclusion
Dissatisfaction with daily life activities persists several years post cancer diagnosis in older and younger adult cancer survivors, despite self-reported health within normal limits. Impairment-based short forms used in oncology clinics may lack sensitivity to detect activity limitations and participation restrictions conveyed through in-depth assessment. Adoption of more comprehensive screening methods may be needed for timely referral to cancer-based occupational therapy services.
Key findings
Dissatisfaction with daily life activities persists several years post cancer treatment in older and younger adult cancer survivors. Use of semi-structured interview approaches may better detect occupational performance deficits compared to general health short forms.
What the study has added
Given that general health short forms may lack the sensitivity to detect occupational performance deficits, alternative interview screening approaches may be needed for timely referral to cancer-based occupational therapy services.
Footnotes
Acknowledgments
The authors would like to acknowledge Haley Feller, BA, for her contributions in data collection.
Research Ethics
Ethical approval was obtained from the University of Pittsburgh Institutional Review Board (PRO18030367) on July 11, 2018.
Consent
All participants provided written informed consent to participate in the study.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. Portions of these data have been presented at the 2019 American Congress of Rehabilitation Medicine Conference on November 6, 2019, in Chicago, Illinois, in poster presentation. Abstract submission for this poster presentation will be published in the Archives of Physical Medicine and Rehabilitation.
Contributorship
All authors researched the literature and applied for ethical approval. Rachelle Brick and Elizabeth Skidmore contributed to the development of the data. All authors contributed to the methodology of the project and statistical analysis plan. Rachelle Brick carried out the statistical analysis and wrote the first draft of the manuscript. Rachelle Brick and Elizabeth Skidmore interpreted the data. All authors reviewed and edited the manuscript and approved the final version.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: University of Pittsburgh, Department of Occupational Therapy.