
Abstract
Introduction
While occupational therapists promote quality of life enabling occupation, many receive little to no training on palliative and end-of-life care. This study synthesizes relevant literature to find out what is known about training for them on this matter.
Methods
A scoping review using Arksey and O’Malley’s five-stage framework exploring literature on palliative and end-of-life care training in occupational therapy (French or English; undergraduate or graduate). The first author screened the titles, abstracts, and keywords and selected literature to be read by the teams to extract and include relevant knowledge. Corroborated thematic analysis synthesized the findings.
Result
Out of the 384 publications initially identified, 25 were included in the review. To be trained in palliative and end-of-life care, occupational therapists have to (a) be exposed to knowledge on specific (b) topics required for competent practice using (c) educational strategies supporting learning about palliative and end-of-life care.
Conclusion
Whereas introductory-level knowledge of palliative and end-of-life care should be offered to all students, advanced training should allow occupational therapists to master the philosophy of this type of care, deepen the understanding of topics such as being confronted with death, and empower them to advocate for their unique contribution.
Introduction
Palliative and end-of-life care are two related, but distinct, areas of practice for healthcare professionals, including occupational therapists. On the one hand, the World Health Organization (WHO)(2017) defines palliative care as an approach that aims to improve the quality of life of both clients and their families facing a life-threatening illness. Palliative care addresses the prevention and the relief of suffering by means of early and thorough assessment and treatment of pain, as well as other physical, psychosocial, and spiritual problems (WHO, 2017). On the other hand, end-of-life care refers to caring for people in decline who are deemed to be terminal or dying in the foreseeable (near) future (Canadian Institute for Health Information, 2011). Therefore, end-of-life care usually describes the care offered when death is imminent (Palliative Care Program Working Group, 2012), whereas palliative care should be offered at the early stages of a disease, from the time of diagnosis, and potentially to the end of life (Hawley, 2014). Although palliative and end-of-life care are not synonymous, they remain connected (Izumi et al., 2012).
This distinction between these two terms is misunderstood by the general population and even by healthcare professionals (Aldridge et al., 2016). Most healthcare providers and most of the public assume that palliative care is limited to the end-of-life stage (Aldridge et al., 2016). Moreover, most healthcare professionals, including occupational therapists, have little to no training on the principles of palliative and end-of-life care (Connor et al., 2002; Dawson and Barker, 1995). Yet, with this particularly vulnerable clientele, healthcare professionals need to acquire understanding of what palliative care is and the potential benefits for the person in preventing and relieving suffering, whether physical, psychosocial, or spiritual.
To achieve this, better training in palliative care has been recommended for healthcare professionals (WHO, 2017), including for occupational therapists (Australia’s Special Interest Groups, 2015; Canadian Association of Occupational Therapy (CAOT), 2011).Indeed, occupational therapists have stated that they lack training regarding their unique roles in this specific context of care (Ashworth, 2014; Eva and Morgan, 2018; Halkett et al., 2010; Keesing and Rosenwax, 2013).Moreover, Hammill et al. (2017) suggested that most occupational therapists will be in contact with dying clients over the course of their professional careers. In fact, 95% of occupational therapists will face the death of a client within or outside palliative care units (Cipriani et al., 2000). Consequently, all occupational therapists, regardless of their field of practice, should understand and come to terms with palliative care.
To meet the educational needs of occupational therapists and enhance their competency in this area of practice, a comprehensive synthesis about what must be learned in palliative and end-of-life care is required. Such a synthesis would support occupational therapists who want to know more about this area of practice, inform the skills required to work with dying individuals, and inform occupational therapy curriculum design in end-of-life care. Therefore, the purpose of this study was to synthesize relevant literature on occupational therapists’ training needs regarding palliative and end-of-life care.
Methods
This scoping review uses Arksey and O’Malley’s (2005) five-stage framework, including the enhancements proposed by Levac et al. (2010) and Colquhoun et al. (2014), which is considered appropriate to map the key concepts underlying a research area. The research team was comprised of a student (CTC), an academic professor (AB), and a researcher (MG).
Identifying the research question
Our question was: What is known about training in palliative and end-of-life care for occupational therapists?
Identifying relevant studies
Searches were conducted in Medline/PubMed, CINAHL, SCOPUS, OTDbase, OTSkeeker, ERIC, and Education. Keywords included “occupational therap*” AND (“end-of-life” OR “palliative” OR dying OR “terminal care” OR “life-threatening illness*” OR hospice OR “terminally ill” OR “life-limiting chronic illness” OR “terminal diagnosis”) AND (education OR learning OR training OR teaching). All peer-reviewed publications before 21 October 2019 were considered. Sources published in other languages than English or French were excluded. The search strategy conducted by the student (CTC) was validated by an experienced librarian in health sciences (Figure 1). The first author (CTC) screened the titles, abstracts, and keywords of publications identified in the literature search for eligibility. The reference list of all eligible publications was manually searched to identify additional publications. The retained publications underwent a full-text review by two members of the team (CTC and AB). In cases of disagreement, a third member (MG) was invited to help reach a consensus.
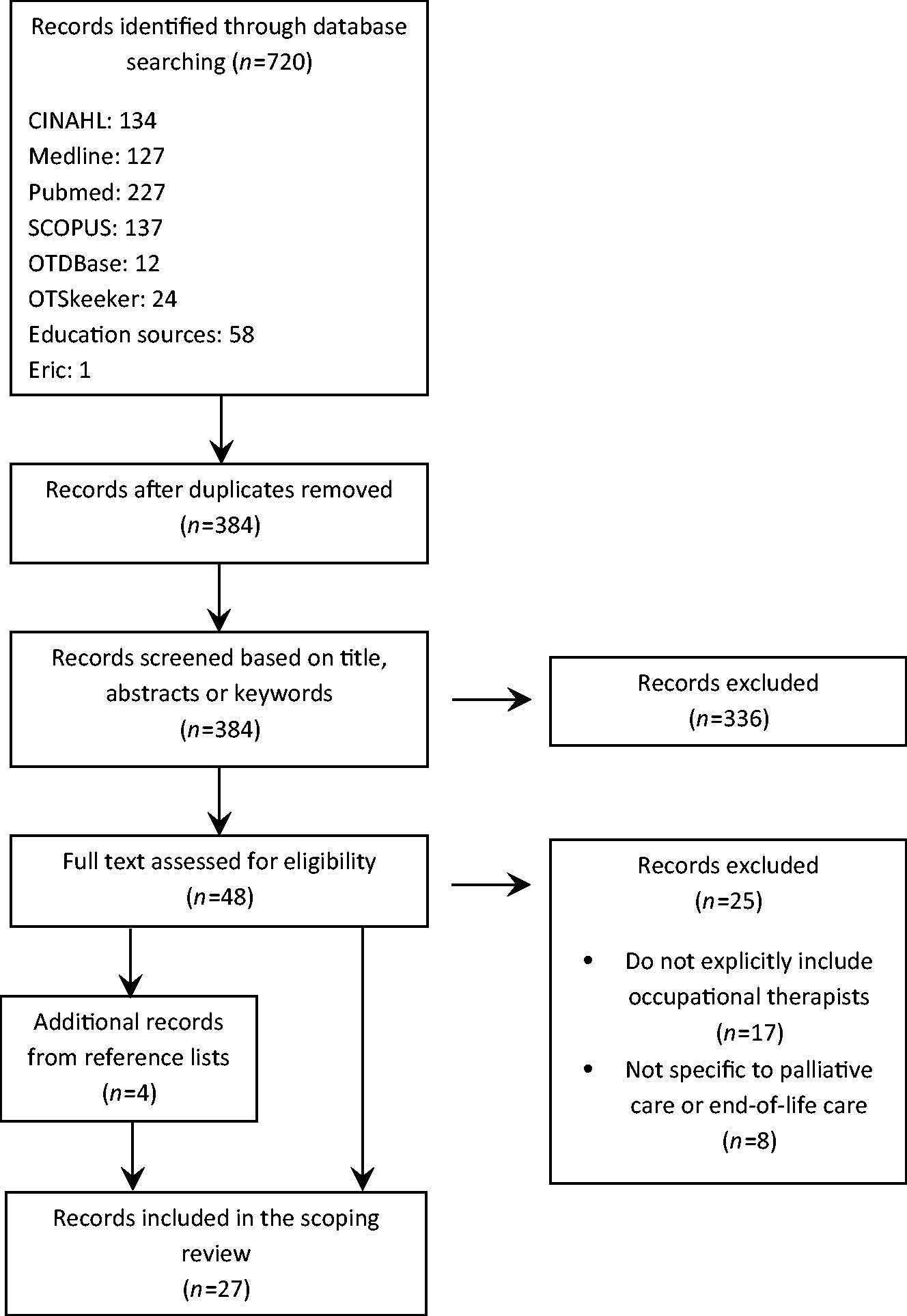
Overall search strategy and selection of papers for final review.
Study selection
To be included in this scoping review, eligible publications had to address palliative or end-of-life care as defined in the introduction. Moreover, publications had to focus on training for undergraduate or graduate occupational therapists, which is defined as the process of learning or teaching the skills and knowledge needed (Cambridge Dictionary of American English, 2008). Publications addressing other members of the interdisciplinary team, without explicitly referring to occupational therapists, were excluded.
Charting the data
The research team collectively developed the data-charting form as proposed by Levac et al. (2010). The first team member (CTC) read each publication and extracted the following information: authors’ name, year of publication, the country where the study was conducted, objectives, methodology, results, key discussion, and concepts relative to training in palliative and end-of-life care.
Collating, summarizing, and reporting results
Thematic analysis was used to synthesize and interpret summaries by using descriptive codes (Paillé and Mucchielli, 2016). Excel was used to store and organize the data and complete coding. The first team member (CTC) identified emerging themes iteratively from the codes. Data analyses were corroborated by the second team member (AB). Emerging conclusions were elaborated in meetings of the entire research team.
Results
The initial search yielded 720 potentially relevant publications, and 336 records were removed, since almost half were duplicates (Figure 1). After screening by title and abstract, 48 papers were read in full, of which 25 were disregarded because they did not explicitly refer to occupational therapists or to palliative or end-of-life care. Documents retained were mostly published in the last 10 years, and papers originated mainly from Australia (n = 10), Canada (n = 6), and the United States (n = 4).
Thematic analysis
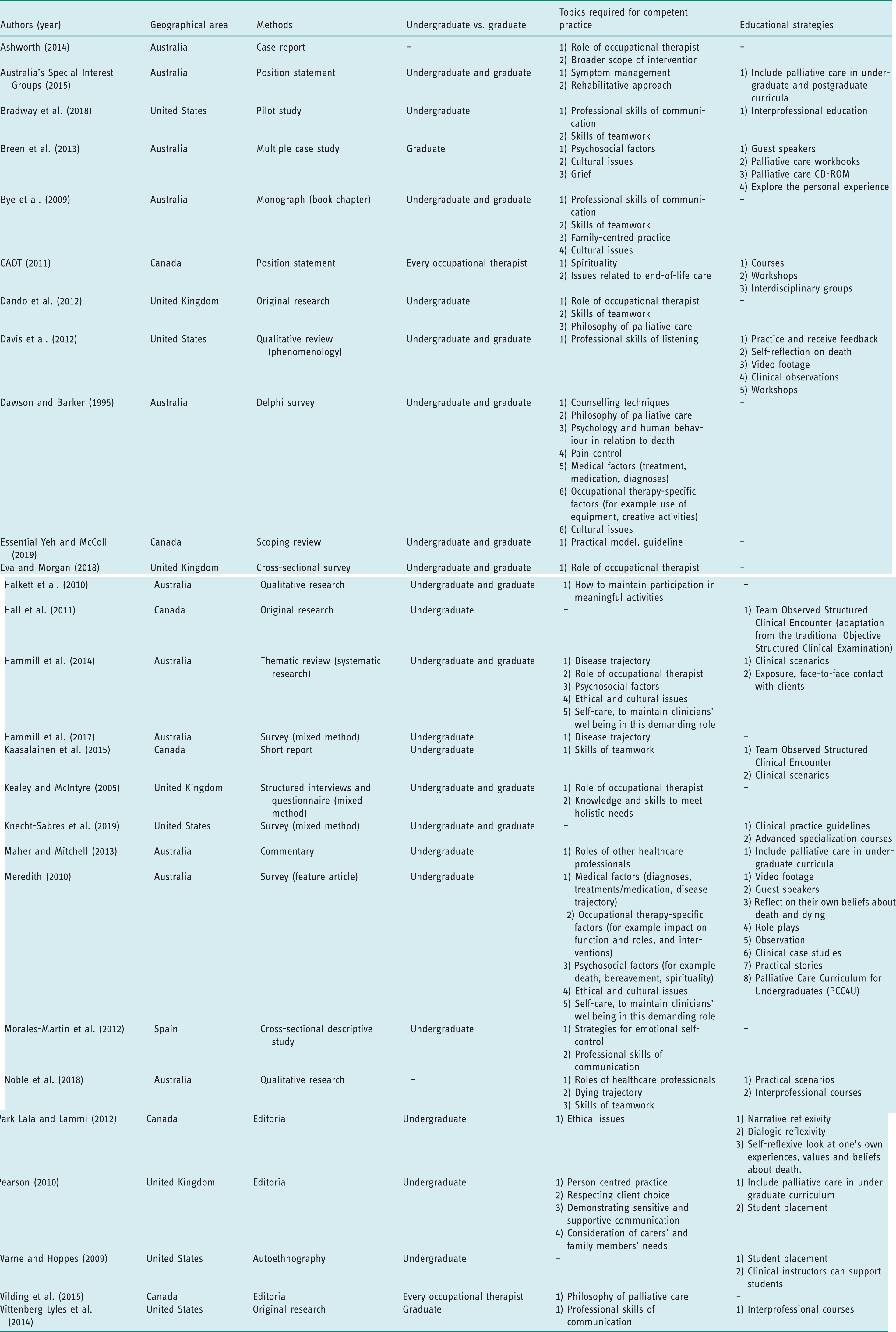
Relevant literature on the training of palliative and end-of-life care for occupational therapists was mapped around three emerging themes: exposure to knowledge, topics required for competent practice, and educational strategies (Table 1).
Exposure to knowledge. Twelve articles stated that all occupational therapists should receive introductory-level training on palliative and end-of-life care (CAOT, 2011; Warne and Hoppes, 2009; Wilding, 2015) during their undergraduate curriculum (Bye et al., 2009; Dando et al., 2012; Halkett et al., 2010; Hammill et al., 2014, 2017; Kealey and McIntyre, 2005; Maher and Mitchell, 2013; Meredith, 2010; Pearson, 2010). For example, Kealey and McIntyre (2005) mentioned that all undergraduate students in occupational therapy should acquire the knowledge and skills necessary to meet the holistic needs of dying people. In Australia, Meredith (2010) found that 54% of occupational therapists reported having received no training on palliative and end-of-life care, and she concluded that there is still work to be done to improve on the education provided to occupational therapists.
Six papers discussed the importance of increasing training at a graduate level (Australia’s Special Interest Groups, 2015; Bye et al., 2009; CAOT, 2011; Dawson and Barker, 1995; Hammill et al., 2014; Kealey and McIntyre, 2005) whereas two papers focused on postgraduate training (Bye et al., 2009; Davis et al., 2013). For instance, coping with the death of a client and competence in listening could be better learned through practice and experience or at the graduate level (Bye et al., 2009; Davis et al., 2013).
Topics required for competent practice. Occupational therapists should be trained in many topics to prepare them for practice in end-of-life care. Table 1 synthesizes what should be covered, and these topics falls into two categories: (a) knowledge and (b) skills.
Summary of education topics on palliative and end-of-life care and strategies (n = 27).
Training on palliative and end-of-life care should prepare occupational therapists to meet the needs of people living with grief and loss. In three papers, authors suggest that training must include psychosocial factors such as grief, loss, bereavement, spirituality, and achieving a ‘good death experience’ (Breen et al., 2013; Hammill et al., 2014; Meredith, 2010). Occupational therapists should learn the stages of bereavement and what constitutes a good death (Breen et al., 2013). There are cultural differences in relation to grief and death that occupational therapists will face and must deal with (Breen et al., 2013; Dawson and Barker, 1995). Consequently, five papers emphasized that cultural differences regarding end of life should be explored in undergraduate programmes (Breen et al., 2013; Bye et al., 2009; Dawson and Barker, 1995; Hammill et al., 2014; Meredith, 2010). Moreover, palliative and end-of-life care raises numerous ethical issues that should be specifically addressed (Hammill et al., 2014; Meredith, 2010). In addition, four other articles emphasized that occupational therapists should learn about clinical factors such as diagnoses, treatments, medications, and disease trajectory (Dawson and Barker, 1995; Hammill et al., 2014, 2017; Meredith, 2010).
Still in relation to the theoretical knowledge to be learned, Essential Yeh and McColl (2019) proposed in the last year a practical model to guide interventions in palliative and end-of-life care based on occupation.According to these authors, this model should be taught to occupational therapists, as it offers guidelines for care in this field. The model includes five themes: (a) valued occupations as a primary medium of intervention, (b) occupation classified as doing, being, belonging, and becoming; (c) occupation can change; (d) affirming life versus preparing for death; and (e) safe and supportive environment. The model is dynamic and can move forward or backward depending on the trajectory of the terminal illness. For the authors, a model-based clinical education can help occupational therapists improve their professional identity, competence, and confidence to work in palliative care (Essential Yeh and McColl, 2019).
Finally, some specific skills are required to enable a competent practice.These skills arise from the unique role of the occupational therapist in palliative and end-of-life care. In three papers, authors suggest that occupational therapists have a desire to learn more about their own role in palliative and end-of-life care practice (Ashworth, 2014; Eva and Morgan, 2018; Hammill et al., 2014). For example, a survey conducted by Meredith (2010) revealed that occupational therapists feel underprepared to work with people living with a terminal illness because their role is not well-defined. Consequently, according to Ashworth (2014), a broader scope of interventions in palliative and end-of-life care should be taught to prepare occupational therapists to fully assume their potential roles. Halkett et al. (2010) discussed that training should be given on interventions directed at maintaining participation in meaningful activities. Meredith (2010) added that training should be provided on the impact of end of life on a person’s skills and roles.
Educational strategies to learn about palliative and end-of-life care. Many options are suggested to enhance training on palliative and end-of-life care. Table 1 presents what has been found throughout the literature.
Meredith (2010) described which resources are currently used to teach palliative care in six Australian universities, and which other resources are requested by the schools. Many resources are desired by programmes in occupational therapy, including specific video footage concretely showing the practice of occupational therapy in this context (Davis et al., 2013; Meredith, 2010), clinical case studies (Hammill et al., 2014; Meredith, 2010), and role playing (Meredith, 2010). Some teaching resources are already used by some university programmes, such as the Palliative Care Curriculum for Undergraduates (PCC4U), which is a resource kit that was developed for all undergraduate students in any profession who need to learn about the role of palliative care and its principles (Meredith, 2010). Also, guest speakers have been found throughout the literature to be a resource that is either already being used by undergraduate programmes in occupational therapy (Breen et al., 2013; Halkett et al., 2010) or is planned to be used (Meredith, 2010). For example, in some Australian universities, issues of loss and grief are taught by a guest speaker working in palliative care (Breen et al., 2013). In one Australian university, students spend up to 12 hours in direct learning activities given in part by an occupational therapist working in paediatric palliative care (Halkett et al., 2010).
Davis et al. (2013) suggested that teaching listening skills should include methods such as a period of practice, feedback, and promoting self-reflection on the death experience. Three papers reported that these methods should also be incorporated to enhance learning about palliative and end-of-life care (Breen et al., 2013; Meredith, 2010; Park Lala and Lammi, 2012). Moreover, Wittenberg-Lyles et al. (2014) have mentioned that interprofessional courses could be a good way for occupational therapists to learn communication and listening skills. Interprofessional courses along with practical scenarios could be a way to teach teamwork skills (Bradway et al., 2018) and the roles of each healthcare professional (Kaasalainen et al., 2015; Noble et al., 2018).
According to Warne and Hoppes (2009), there are specific strategies that can support students in occupational therapy doing a fieldwork in palliative and end-of-life care. In their autoethnography, Warne and Hoppes (2009) mentioned that occupational therapy programmes have a responsibility to promote a safe learning environment. For Breen et al. (2013), teachers and clinical supervisors should be a model in end-of-life situations; their experiences and ease with the subject could modulate training to occupational therapy students. Occupational therapy students should be encouraged to talk about end of life with their clinical supervisors in order to be more at ease about addressing it with their clients. To do this, Park Lala and Lammi (2012) suggest narrative reflexivity and dialogic reflexivity to allow self-reflection on a student’s experiences, values, and beliefs about death. According to Park Lala and Lammi (2012), narrative reflexivity and dialogic reflexivity are two reflexive approaches that allow students to develop ethical skills and sensitivity to death, both needed when working in end-of-life care. Three other papers emphasized that exposure to clients through face-to-face contact and allowing them to make clinical observations are valuable strategies for occupational therapy students (Davis et al., 2013; Hammill et al., 2014; Meredith, 2010).
According to Knecht-Sabres et al. (2019), clinical practice guidelines should be developed to improve the training occupational therapists receive. Guidelines can be viewed as an educational strategy to teach the role of occupational therapists in palliative and end-of-life care (Knecht-Sabre et al., 2019).
Still, some authors mentioned that the skills needed to work in palliative and end-of-life care come with experience (Bye et al., 2009; Davis et al., 2013). According to Davis et al. (2013), ‘It may be that working in end-of-life care requires insight and skills that only an experienced therapist has acquired and that this area of practice is not suitable for new graduates’ (p. 19).
Discussion
This scoping review aimed to synthesize relevant literature on palliative and end-of-life care training essential to occupational therapists. Every undergraduate occupational therapy student should learn about the philosophy of palliative care, the role of different healthcare professionals, teamwork skills, communication, and should acquire knowledge about grief, bereavement, and spirituality. Other topics, such as coping with the death of a client, could be taught in greater depth to occupational therapists working in palliative and end-of-life care. Educational strategies such as guest speakers, guidelines or clinical case studies, exposure to dying clients, self-reflection, and role play are relevant.
The current need to provide more training on palliative and end-of-life care that we have identified has also been discussed by many other authors (Breen et al., 2013; CAOT, 2011; Hammill et al., 2017; Kealey and McIntyre, 2005; Pearson, 2010), but only one study identified in this scoping review explored how to do it (Meredith, 2010). Morales-Martín et al. (2012) suggest that undergraduate health science students in Spain, including in occupational therapy, feel unprepared to deal with dying people. Hammill et al. (2014) also report in a thematic review that current training does not prepare students in occupational therapy to work with clients in palliative and end-of-life care. According to Dawson and Barker (1995), 64% of occupational therapists report having received no specific training to work with individuals with a terminal illness during their undergraduate studies. Fifteen years later, the situation doesn’t seem to have changed in this country (Meredith. 2010).
If improving training in palliative and end-of-life care for occupational therapists is an established target, information about how to meet this goal is scarce. Occupational therapists are not the only professionals facing this challenge: preparation for palliative and end-of-life care is also described as inadequate for medicine (Carrasco et al., 2015; Sullivan et al., 2003), speech pathology (Pascoe et al., 2018), and nursing programmes (Gillan et al., 2014). Unfortunately, few studies have been conducted on training in palliative and end-of-life care (for example Dawson and Barker, 1995; Meredith, 2010), and training was not the main topic of the publications reviewed (for example Halkett et al., 2010; Hammill et al., 2014; Kealey and McIntyre, 2005). If this scoping review brought out different educational strategies that are either desired or already in use, it is now necessary to optimize and share them with all occupational therapy programmes, including through scientific research. Future studies could explore relevant strategies to increase occupational therapists’ competency in a palliative and end-of-life context.
Interestingly, Australia has produced half of the articles found over the last few years; it might be a country with more awareness regarding palliative and end-of-life care in occupational therapy and thus a leader in the area. Other countries could look at what is being done there.
It is surprising to note that none of the articles reviewed address the ethical issues faced by occupational therapists working with a person who is planning, organizing and precipitating his or her own death to avoid further suffering or distress in a palliative care situation. In the context of legal changes to end-of-life care in numerous countries (Griffiths et al., 2008, Hurst and Mauron, 2003; Reel, 2018), including access to voluntary euthanasia in Canada (An Act to amend the Criminal Code and to make related amendments to other Acts (medical assistance in dying), Bill C-14, Government of Canada, 2016; Act respecting end-of-life care, CQLR c S-32.0001, Government of Quebec, 2016), in Australia (Voluntary Assisted Dying Act, No. 61 of 2017, Victorian Government, 2017), and in the United States (End of life, Pub. L. No. AB-15, Ch 1, Part 1.85, Sect 443, 15, California Assembly, 2015), occupational therapists need to be informed, worldwide. Occupational therapists are facing a new context of practice with some of their clients requesting assistance to die (Gordon et al., 2015). Occupational therapy programmes should question their curriculum to be sure they are adequately preparing their students to cope with the contemporary challenges of providing palliative and end-of-life care.
One should note our inability to distinguish between palliative and end-of-life care, given that for the most part, publications used these terms interchangeably. The terms ‘palliative care’ and ‘end-of-life care’ were not always defined in the reviewed publication, and if they were, palliative care was sometimes seen as restricted to the end-of-life period (Hammill et al., 2014; Kealey and McIntyre, 2005). Indeed, some authors seemed to use the two terms as synonyms (Halkett et al., 2010; Meredith, 2010). Yet, as suggested by the palliative integrative approach (Canadian Hospice Palliative Care Association, 2013; Hawley, 2014), even if palliative and end-of-life care are on the same continuum, with the aim of preserving quality of life and ensuring the comfort of clients with a terminal illness, they are distinct concepts.Palliative care and end-of-life training needs might be quite different. For example, training in palliative care should also address rehabilitation, as proposed by Hawley (2014), since end of life is not the only life trajectory for clients suffering from a life-threatening illness.
Surprisingly, there is no consensus on the role of occupational therapists in end-of-life care in the literature analysed. Even if Keesing and Rosenwax (2013) argue that the role of occupational therapists is well-documented, others reported the lack of evidence on this subject (Hammill et al., 2014). Halkett et al. (2010) explored potential barriers to occupational therapy practice. They suggested that a lack of training regarding their own role may explain why occupational therapists do not promote their potential contribution in this area of practice (Halkett et al., 2010).
Study limitations
Titles and abstracts were no-double screened to include or exclude the papers in this scoping study. This methodological choice limits the reliability of the identification process of the relevant studies. To overcome this limit, the first author was more inclusive, retaining the document when ambivalent and increasing the number of documents read in their entirety.
Quality assessment of the papers reviewed or ordering the level of evidence of their conclusions was not performed, in line with recommendations from Arksey and O’Malley (2005) as well as Levac et al. (2010) for scoping studies. Therefore, readers must keep in mind one limit of this review: it does not determine whether specific topics need to be prioritized, or which educational strategies are most robust when training occupational therapists in palliative and end-of-life care, for example. Those are future directions of research.
Finally, only scientific literature was scanned. One book chapter was identified by conducting the search strategy in the selected database (Bye et al., 2009). It was retained for its relevance, since scoping reviews may include grey literature. However, no additional attempt was made to find other textbooks, proceedings, or unpublished work. Although exhaustive, this scoping study is consequently partial. For instance, this review did not include information on the training currently offered by professional associations.
Conclusion
Every undergraduate student in occupational therapy should receive introductory training regarding palliative and end-of-life care (for example philosophy of palliative care, grief, bereavement, loss, and achieving a good death). Since palliative and end-of-life care are sensitive subjects that require a safe learning environment, education strategies such as self-reflection and exposure to dying clients under supervision should be encouraged. This article might support occupational therapists in targeting continuing education goals in palliative and end-of-life care and find strategies to meet these goals. In summary, this scoping review highlights the need for occupational therapists to be more aware of palliative and end-of-life care and will contribute to clarifying their role – including through future research – allowing them to better advocate for their unique contribution.
Key points for occupational therapy
Every occupational therapist needs to receive training on palliative and end-of-life care. Training must focus on the philosophy of palliative care and make the distinction between palliative and end-of-life care. Educational strategies to promote learning should include supervised exposure to dying clients.
Footnotes
Acknowledgements
The authors are grateful to Annick Bourget for her contribution to this study and to the enhancement of teaching occupational therapy.
Research ethics
Not applicable to this scoping review.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: this research received no specific grant from any funding agency in the public, commercial, or non-profit sectors. However, some Fonds de recherche du Québec – Santé (FRQS) grants for new investigators granted to MG were used to conduct this work.
Contributorship
Both authors have contributed to data analysis and interpretation. They have co-drafted the paper, approved the final version for publication, and are accountable for all aspects of this work.