
Abstract
Introduction
Lower back injuries can prevent people from engaging in the occupation of work, which is considered to be beneficial to physical and mental wellbeing. Return-to-work programmes aim to support people to re-engage with work; however, the success of these can be varied. The aim of this review was to explore what factors facilitated a return to work for those in employment, and what the factors may be in preventing others from making a successful return to work.
Method
A systematic search of the literature identified 10 qualitative research studies, and a meta-ethnographic approach was then used to critique and synthesise the findings to provide a line of argument.
Findings
Interrogation of the selected studies brought about three third-order interpretations as follows: enabling injured workers to return to work safely; challenging negative assumptions; overcoming organisational barriers.
Conclusion
The study supports previous findings that emphasise consideration of wider organisational and psychosocial factors relating to supporting people to return to work, rather than focusing solely on the injured worker. Suggestions are made for the modification of current work practices, the need for a strength-based approach to rehabilitation and for occupational therapists who might work with people living with back pain.
Introduction
The economic impact of musculoskeletal disorders in developed countries is significant. In 2016/2017, an estimated 507,000 people in the United Kingdom (UK) with musculoskeletal disorders cost the economy in excess of £6 billion (Nestorova and Mircheva, 2018). Musculoskeletal disorders include injuries that may affect bones, muscles and joints (da Costa and Vieira, 2010), with the most common form involving the lower back (Soklaridis et al., 2010). Snodgrass (2011) reported that 20.4% of work injuries necessitating time away from work in the United States of America were related to the lower back.
The consequences of prolonged absenteeism from work has significant consequences for both physical and mental health (Waddell and Burton, 2006). There is a risk that prolonged absenteeism could lead to a state of occupational deprivation, whereby individuals are restricted from acquiring, using or enjoying the occupation of work (Wilcock, 1998). For the economy, significant costs are incurred due to absenteeism, loss of productivity and increased healthcare (Centers for Disease Control and Prevention, 2016).
Figures regarding successful return to work vary considerably across countries, with return-to-work rates ranging between 22% and 62% in German and Dutch populations, for example (Anema et al., 2009). What is consistent, however, is that the longer a person is absent, the less likely they will be successful in returning to work (Anema et al., 2009; Heijbel et al., 2006). Previous studies have identified factors that can influence the success of return-to-work interventions. For example, MacEachen et al. (2006) reported mechanisms that can affect the success of return to work, which include taking into account relationships between parties (such as workers, employers and physicians), work modifications and other organisational dynamics.
Park and Bhattacharya (2013) found that a person who has a history of compensation claims is more likely to be terminated from employment than their non-injured counterparts, and concluded that this implied there were lingering ill effects due to injury. Another factor that may influence the return-to-work process is the individual’s perception of their injury and expectation regarding prognosis. Heijbel et al. (2006) found that those with a negative self-prediction of their ability to return to work were less likely to make a success of this than those with a positive outlook. Heijbel et al. (2006) concluded that changing views from negative to positive is crucial to facilitate successful return to work. While programmes may differ in the range of interventions provided, it is generally accepted that they should address a combination of psychological, environmental and external factors (Iles et al., 2008).
The above literature reflects the return-to-work process generally, rather than focusing on individuals who experience lower back pain. Considering the prevalence of lower back injuries and the consequences associated with long-term absenteeism from work, it is vital to understand how best to support people to return to work and develop interventions that reflect the needs of individuals who experience lower back pain and are attempting to return to work. No systematic review, to the researchers’ knowledge, has attempted to draw together current evidence on the factors that can support the return-to-work process for workers with lower back pain. The PROSPERO International prospective register of systematic reviews was searched on 20 December 2018 and yielded no results. Furthermore, quantitative research has been prevalent in this field, with a relatively limited focus on the experiences of those involved in the return-to-work process (Ryan et al., 2014).
The aim of this review was to explore what factors facilitated a return to work for those in employment, and what the factors may be in preventing others from making a successful return to work. A meta-ethnographic approach, as originally proposed by Noblit and Hare (1988), was used to draw comparisons and highlight differences between studies in order to generate new insights. This approach was considered suitable to address the above aim due to its interpretive rather than integrative approach. By combining findings from separate studies into a synthesis it is anticipated that practitioners might benefit from acquiring new insights in this field.
Method
Search strategy
On 23 January 2019, the electronic databases PubMed, Health Research Premium Collection, AMED, CINAHL, MEDINE and PsycINFO were searched for articles related to lower back injuries and the return-to-work process. Search terms used included ‘low* back pain’, ‘lumbar pain’, ‘return* to work’ and ‘vocational rehabilitation’. Return to work and absence from work were used as separate concepts in order to maximise the amount of relevant material generated. Noblit and Hare (1988) recommend an exhaustive search to identify all relevant accounts and articles published; a search was carried out therefore between 1 January 2009 and 23 January 2019 to ensure findings reflected current work practices.
Duplications were then discarded and the remaining papers were manually screened using predetermined inclusion and exclusion criteria. For an article to be included, it must have been published in a peer-reviewed journal, report primary, qualitative data and relate to rehabilitation and return to work. Papers were excluded when the focus was on musculoskeletal injuries generally rather than lower back and if the study referred to prevention of injury rather than rehabilitation. Examples of articles excluded include: papers relating to prevention or acute phases of injury rather than rehabilitation; papers which laid out a protocol for research or feasibility trials; papers related to specific populations; quantitative papers; and papers related to developing research tools.
A process of citation chaining was used to identify additional papers relevant to the review’s aim. Backward searching was used to screen the references of the included papers in order to identify any further articles (Boland et al., 2017). Forward searching using Google Scholar ‘cited reference search’ was used to identify which papers had subsequently cited the key reference. See Figure 1 for details of articles retrieved at each stage of the search using the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines (Moher et al., 2009).
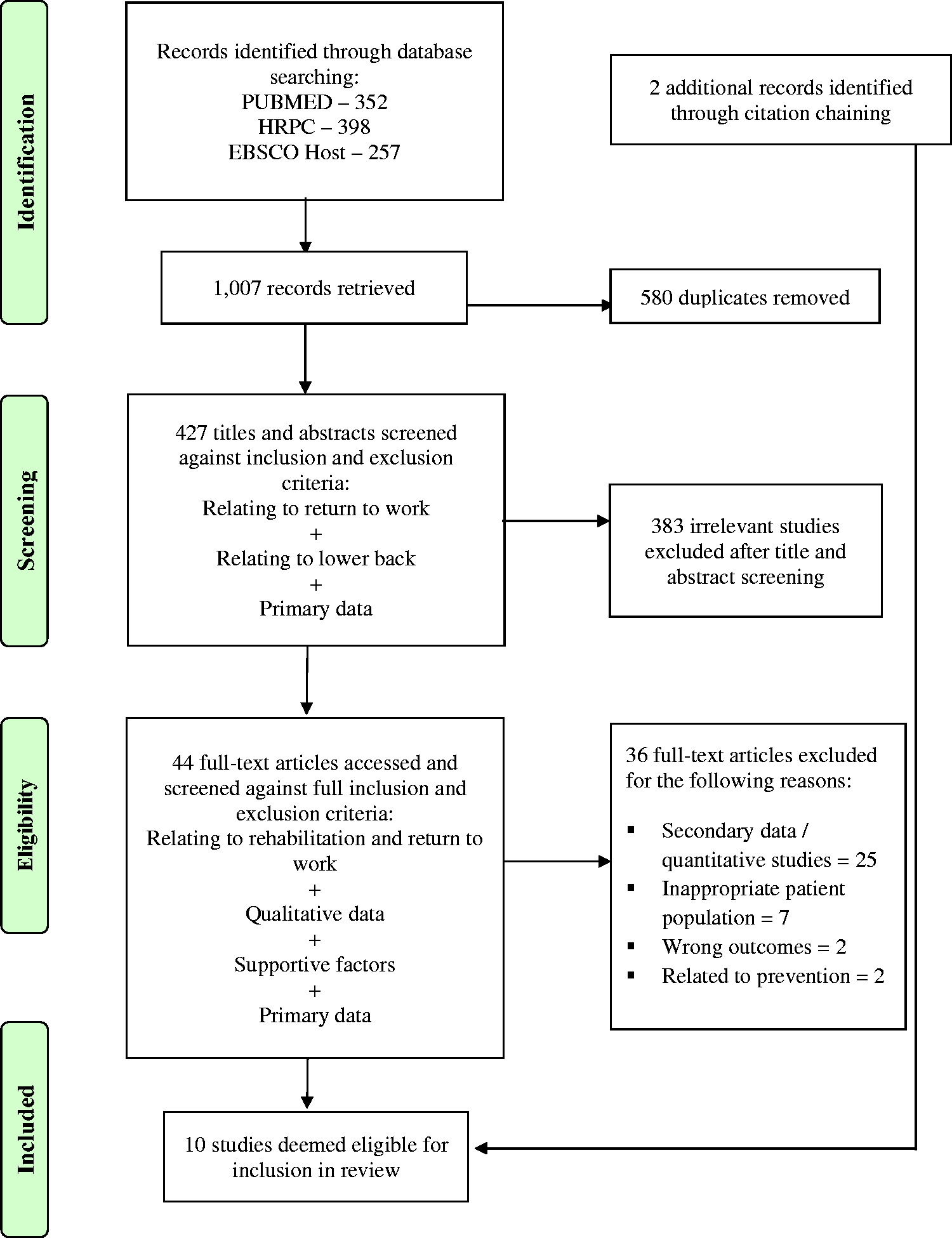
Number of studies identified and screened. Based on the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) flow diagram (Moher et al., 2009).
Study selection
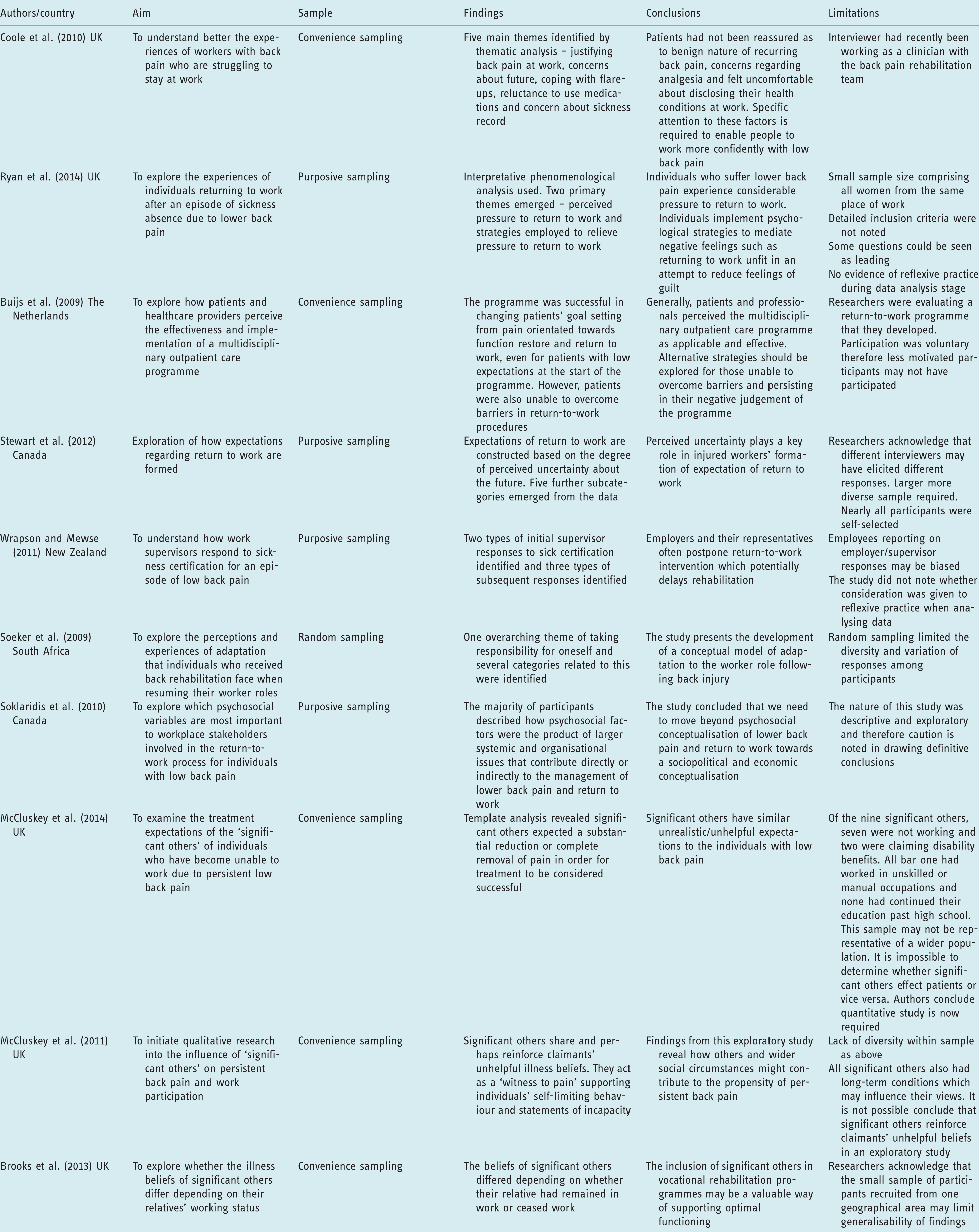
This review only included primary data from peer-reviewed journals in order to facilitate systematic and transparent searching of databases and for clarity of reporting results (Boland et al., 2017). The findings presented do not include articles reporting secondary data due to the risk of misinterpreting original findings. Grey literature was not used due to difficulties ascertaining peer-reviewed status and because of the challenge this presents for systematic reporting (Boland et al., 2017). The methodological quality of the included studies was judged using the National Critical Appraisal Skills Programme (Critical Appraisal Skills Programme, 2018). The appraisal tool assisted the recording of key findings, as well as to identify strengths and limitations of the studies (see Table 1).
Summary of selected studies.
Data analysis
Analysis was influenced by the authors’ interpretation of the findings and consideration of the original participant quotes presented in the identified studies. The meta-ethnographic process of Noblit and Hare (1988) was followed, which allows immersion in the writing and findings of included studies in order to interpret the overall findings. The initial stages of this process determine that the researcher must select a topic and initial area of interest, undertake a systematic search of the literature to identify relevant articles and then repeatedly read the research noting common or recurring concepts (Britten et al., 2002). The concepts from each study were then translated into one another to identify reciprocal or refutational categories (see Table 2). The final stage of the process was to synthesise and express the translations into a line of argument (see Table 3).
Concepts from selected studies.

Synthesis: concepts, second and third-order interpretations.

Statement of researchers’ interests
The researchers held a relativist ontological position, and approached this review from a constructivist epistemology. Constructivism proposes that there are multiple socially constructed meanings that may or may not be shared among individuals or across cultures (Guba and Lincoln, 1994). This epistemological position fitted well with meta-ethnography in order to interpret findings from the qualitative research sourced. An awareness was adopted that personal interpretation would be integral to the review of the literature (Noblit and Hare, 1988). Nadin and Cassell (2006) suggested all researchers should be aware of their own epistemological assumptions and should make a commitment to reflexivity, in this regard a reflexive diary was maintained by the first author which was discussed with the second author to identify, explore and challenge assumptions.
Findings
Enabling injured workers to return to work safely
The workers’ personal characteristics, attitudes and perceptions
This theme relates to how the personal characteristics, attitudes and perceptions of each injured individual can affect certain aspects of the return-to-work process. For example, across several studies factors such as ‘motivation’ and ‘taking responsibility for one’s self’ positively influenced people’s ability to return to work (Buijs et al., 2009; Soeker et al., 2009; Stewart et al., 2012). Soeker et al. (2009) noted that workers who were more competent in their roles saw themselves as assertive and were proactive in their care and were more likely to experience positive outcomes.
Similarly, participants in the study by Brooks et al. (2013) described the benefits of working, such as contributing to positive self-identity and offering a welcome distraction from back pain. However, other studies found the perceptions that workers hold about themselves may also limit their ability to engage with rehabilitation. For example, self-doubt, fear of re-injury, despair, lack of control and lack of confidence influenced people’s beliefs about their ability to return to work (Brooks et al., 2013; Buijs et al., 2009; Coole et al., 2010; McCluskey et al., 2011; Ryan et al., 2014; Stewart et al., 2012). Where attitudes such as these originate was explored in the study by Soklaridis et al. (2010), who found that people’s attitudes towards injuries, recovery times and compensation are inherited from the family they grew up in and the culture of their community.
Significant others
Consideration of wider systems and the influence of significant others is discussed in several studies. For example, significant others may reinforce claimants’ unhelpful beliefs regarding their lower back condition, including fear of pain, re-injury and pessimism over their ability to return to work (Brooks et al., 2013; McCluskey et al., 2011, 2014; Ryan et al, 2014; Soklaridis et al., 2010). Brooks et al. (2013) found that the appraisal of injured workers by significant others, such as a relative, was different depending on whether their relative was working or not. Those who were working were perceived as ‘stoical’ and ‘heroic’, whereas relatives in the non-working sample were perceived as ‘blameless victims’ and were more likely to be labelled ‘disabled’. A potential limitation of these findings, however, is that all patients in the out-of-work sample had to attribute their lack of work participation to their back condition to be eligible for the study. It is, therefore, unsurprising arguably that the relatives of these people were more likely to label them as ‘disabled’. Furthermore, the mean age of the non-working sample was 7.8 years older for patients and 24.9 years older for significant others compared to the working sample. There is a possibility that differences exist in how this older group perceive their abilities due to age.
Nonetheless, similarities exist regarding treatment expectations and beliefs between significant others and their injured relatives. It is possible that expectations among the parties are mutually reinforcing and may further contribute to work disability. By working with back-injured individuals, as well as their social network, it may be possible to support injured workers to return to work better.
Modification of work duties, activity and environment
In addition to psychosocial interventions, adapting the physical environment and making changes to work duties is a further way injured workers may be enabled to continue in their work. A number of positive modifications to work duties and practices were noted across studies (Brooks et al., 2013; Buijs et al., 2009; Ryan et al, 2014; Soeker et al., 2009; Wrapson and Mewse, 2011). This included the implementation of a phased return, the usefulness of graded activity programmes, provision of equipment or advice on ergonomics and light or reduced duties. Other factors that supported participants to modify their work duties included having multiple skills and being able to do alternative tasks that did not aggravate their symptoms, being aware of utilising ergonomics and energy conservation, and being in jobs which enabled participants to find a balance between sedentary positions and physical movement.
Conversely, a number of barriers to return to work were also noted across studies (Ryan et al, 2014, Soklaridis et al., 2010; Stewart et al., 2012; Wrapson and Mewse, 2011). Lack of modified duties was one major factor that could delay return to work, particularly in small businesses due to a lack of availability of appropriate duties. For some participants, the experience of modified duties led to feelings of guilt and the possibility of being a burden to colleagues. Soklaridis et al. (2010) found that modified duties were felt to be socially inappropriate in one instance in which male workers were expected to undertake duties ordinarily done by female workers. However, one could argue that this view does little to challenge the occupational segregation by gender that already exists and appears to be becoming more entrenched within current work practices (Huppatz and Goodwin, 2013).
Challenging negative assumptions
Credibility
Lower back pain is described as an ‘invisible’ disability in several studies and it is noted that conditions such as lower back pain can be viewed as ‘bogus’ in the workplace or by health professionals and insurers (Brooks et al. 2013; Coole et al., 2010; McCluskey et al., 2011; Ryan et al., 2014; Soklaridis et al., 2010; Stewart et al., 2012; Wrapson and Mewse, 2011). The absence of visible injury in some instances can lead to workers experiencing negative appraisals of their injuries from others, and may result in a fear of disclosing their back pain. One participant relayed that her employer had stated ‘…you planned all this’ in response to her providing sick certification (Wrapson and Mewse, 2011). As a consequence of not feeling believed, many participants felt the need to justify or prove their symptoms through seeking medical investigations or obtaining a diagnosis (Coole et al., 2010; McCluskey et al., 2011; Stewart et al., 2012).
For some participants, the fear of disclosing a lower back injury may be due to anticipation of discrimination in the workplace. Coole et al. (2010) and Stewart et al. (2012) noted how injured workers may be unfairly penalised due to their injuries (e.g. regarding future work opportunities), and may be perceived as being ‘to blame’. This concept was also noted by Soklaridis et al. (2010), who questioned whether emphasis on psychosocial factors may place the fault with the injured worker and consequently perpetuate the stereotyping and stigmatising of injured workers. These judgements could lead to discriminatory practice occurring in the workplace, which creates fear and uncertainty about the future for injured workers. It is possible, however, that the concept of credibility of illness is something that is imagined and not based in reality. For example, Ryan et al. (2014) reported that one strategy for mediating work–condition conflict is re-appraising the views of others, including colleagues and management: … it was mostly my mental state … imagining that they were thinking the worst of the situation rather than they would be supportive and just glad to have me back, which in reality it turned out to be … (participant in Ryan et al., 2014).
Uncertainty
A number of uncertainties were reported regarding the return-to-work process and future work capacity across several studies. For example, some participants described feeling lost, anxious and insecure about the future and others relayed concerns about earlier than anticipated retirement and future work capacity (Coole et al., 2010, McCluskey et al., 2014; Ryan et al., 2014; Soeker et al., 2009; Stewart et al., 2012; Wrapson and Mewse, 2011). I’ve still got another – 21 years left at work…. The concern is if me [sic] back’s killing me [sic] now, what am I going to be like in later times? (participant in Coole et al., 2010).
Overcoming organisational barriers
Communication
The predominance of feedback across the studies was that there was often a lack of communication and coordination in the return-to-work process. This was particularly highlighted for those seeking compensation in relation to workplace injuries (Soklaridis et al., 2010). Even when employers did communicate with workers, this was sometimes perceived as superficial, with one participant suggesting that employers had ulterior motives for having contact rather than a genuine interest in the worker’s recovery (Ryan et al., 2014). However, Buijs et al. (2009) found that protocolled communication fostered information sharing between health professionals and with their patients, which influenced patient compliance and provided clear explanations, advice and goal setting. Having improved communication and transparency between parties is one way of overcoming organisational barriers to return to work, provided this is done in a way that is viewed as being supportive rather than punitive.
Workplace relations
Another way of overcoming organisational barriers to return to work is to foster positive workplace relations. Several participants expressed feeling supported by employers in returning to work, and it was noted that having good personal relationships with line managers often facilitated flexible working arrangements (Brooks et al., 2013; Ryan et al., 2014; Wrapson and Mewse, 2011). However, not all participants had a positive experience of workplace relationships. Many described a pressure to return to work and feelings of guilt associated with taking time off (Coole et al., 2010; Ryan et al., 2014). Others reported that employers responded negatively or apathetically regarding sickness leave, which in some instances made workers feel their jobs were in jeopardy (Wrapson and Mewse, 2011). From the employer’s perspective, passive behaviour may be the consequence of not wanting to push employees too hard. Soklaridis et al. (2010) stated that small employers were concerned about creating feelings of resentment and frustration from the employee.
‘System’ issues
Further organisational barriers were noted by Soklaridis et al. (2010), who uses the term ‘system’ issues to describe the components of a large organisational system that can contribute directly and indirectly to the management of lower back pain and return to work. System issues can include dysfunction within and between compensation systems, unions, workplace and healthcare systems, which may include waiting periods within the healthcare, punitive measures, or poor implementation of occupational health advice (Buijs et al., 2009; Coole et al., 2010; McCluskey et al., 2014; Ryan et al., 2014; Soeker et al., 2009; Soklaridis et al., 2010, Stewart et al., 2012). Positive system factors include continued education and training of workers, and in one instance changes in political systems which assisted back-injured workers (Soeker et al., 2009).
Discussion and implications
Although many people successfully return to work following lower back injury or episodes of back pain, there are improvements that could be made to the return-to-work process that could potentially benefit injured workers, employers and the wider economy (Soklaridis et al., 2010). In this review, there were several key findings, which employers and return-to-work professionals may wish to consider. Firstly, injured employees should be enabled to return to work as soon as possible to avoid deconditioning and the development of intrinsic barriers such as fear of re-injury or self-doubt (Stewart et al., 2012). This is supported by research that suggests returning to work is beneficial for health (Health and Safety Executive, 2004; Waddell and Burton, 2006). For those who argue that an early return to work could cause more harm (MacEachen et al., 2007), any early return to work should make use of phased return-to-work programmes or modified work duties to minimise the risk of aggravating lower back conditions and exacerbating the worker’s experience of pain (Ryan et al., 2014). Particular attention should be given to small businesses that may be unable to offer appropriate alternative duties or feel that they are putting pressure on workers to return (Soklaridis et al., 2010).
A pressure to return to work is often felt by workers who either feel guilty due to the extra burden on their colleagues in their absence, or are fearful of losing their jobs. In some instances, these internal or external pressures can result in injured workers returning to their usual duties too quickly, potentially exacerbating their condition or jeopardising their recovery (Ryan et al., 2014). Soklaridis et al. (2010) reported that this is particularly the case for some immigrant workers who may be fearful of losing their jobs, or experience difficulty explaining their injury due to language barriers.
The research suggests that in order to address this issue of pressure to return to work, healthcare providers need to do more to support injured workers by gauging when those living with back pain are truly ready to return to work (Buijs et al., 2009; Ryan et al., 2014). Individuals should be given education about their back condition, with emphasis on function rather than diagnosis, as a means to empower individuals to make better informed decisions regarding their recovery and return to work. This may address some of the difficulties with regard to injured workers perceiving a need for a diagnosis (Coole et al., 2010), and may combat a perceived lack of control in their return to work (Stewart et al., 2012).
A further way of challenging perceptions that may exist is to foster openness in the workplace and encourage people to reappraise situations. For example, Ryan et al. (2014) suggested using cognitive behavioural therapy techniques to encourage workers to re-appraise the views of others and openly discuss their relationships with others. This allows for any potential conflicts to be identified and addressed to support the return-to-work process. This could also be used with significant others to challenge the possibly entrenched views that they hold and to break the cycle of reinforcement that may occur between injured workers and their significant others.
Employers, compensation providers, health professionals and human resources staff need to be aware of the reasons injured workers may not be candid about their symptoms. For example, Brooks et al. (2013) noted that workers and their significant others are more likely to emphasise the impact of their illness due to the stringent tests and assessments they experience when applying for benefits. Conversely, some injured workers are likely to play down their symptoms due to fear of stigma, discrimination, job loss and lack of future work opportunities (Coole et al., 2010).
Crucially, sociocultural stereotypes around ‘malingering’ and ‘benefit cheats’ need to be challenged (Brooks et al., 2013), and anti-discriminatory laws need to be strictly followed. Despite anti-discrimination and equality laws, such as the Equality Act (2010) in the UK or the Employment Equity Act (Republic of South Africa, 1998), this review found that the injured workers’ experience was that discrimination in the workplace was common (Coole et al., 2010; Stewart et al., 2012).
Several studies noted that work practices contradicted guidance on return to work. For example, Soklaridis et al. (2010) noted that there were delays in return-to-work procedures and poor communication between parties. Coole et al. (2010) noted that absence management procedures were viewed as ‘punitive’. Improvements should be made to the way absences are managed, and the return-to-work procedure needs to be more supportive to enhance the employees’ experience. As suggested by Soklaridis et al. (2010), one aspect of this support could relate to effective communication, whereby healthcare providers and compensation systems work together to ensure the worker is receiving timely care.
Employers, and small businesses in particular, should be supported to provide necessary work modifications and allow sufficient time for recovery (Soklaridis et al., 2010). Other strategies to support early return to work would be to consider the range of possible duties workers may be able to undertake. By considering a broader pool of jobs, there may be more opportunity for injured workers to return to lighter roles and for employers to be able to implement recommended modifications. This could also tackle the issue of fear of re-injury among injured workers, which is reported in several of the reviewed studies (Brooks et al., 2013; Coole et al., 2010; McCluskey et al., 2011; Stewart et al., 2012). The focus of such interventions is to enable workers, employers and return-to-work professionals to find solutions that may facilitate early return to work and reduce the risk of prolonged absenteeism which could lead to a state of occupational deprivation.
Towards a strengths-based approach
One finding of this meta-ethnography is that the research often emphasises the barriers injured workers face and the things they are unable to do, often feeling at the mercy of the systems that exist. Pessimism regarding the future is evident in a number of studies, for example McCluskey et al. (2011) noted that workers were doubtful about the likelihood of returning to work, and had become increasingly self-limiting and fearful of work activity.
Taking an alternative approach, Brooks et al. (2013) were of the opinion that having a ‘can-do’ attitude may be associated with better functioning in terms of work participation. Similarly, Soeker et al. (2009) emphasised the importance of maintaining a positive attitude in order to facilitate rehabilitation. These views are congruent with having a strengths-based approach, which emphasises the individual’s strengths, what they can do, and the support that is available to them (Social Care Institute of Excellence, 2015). This way of working has been commonplace in UK social care systems since the introduction of the Care Act (2014).
For occupational therapists working in health and social care settings, supporting workers to understand their condition and focusing on function rather than disability may foster a sense of control. This, in turn, could act as a protective factor against the development of intrinsic barriers such as fear of re-injury or self-doubt. Within vocational rehabilitation, occupational therapists can support workers and employers to adapt work duties, identify lighter roles, provide ergonomic equipment and modify work schedules. This expertise is crucial in enabling workers to return to work and prevent long-term absenteeism or unemployment.
Strengths and limitations
This review draws together the experiences of injured workers, significant others, healthcare providers and other professionals involved in the return-to-work process, allowing for different perspectives on return to work to be compared and synthesised. The review included studies pertaining to workers who had returned to work, as well as those who were absent or unemployed. The review also highlights that some of the experiences mentioned are not exclusive to people in the UK, but also to workers in other parts of Europe, South Africa, Canada and New Zealand. However, it is acknowledged that all participants in the studies were from countries with developed healthcare services, which may limit the transferability of these findings.
The inclusion of grey literature may have allowed access to a more diverse evidence base. It is possible that by including grey literature, issues around publication bias could be reduced; however, new challenges can emerge related to appraising methodological quality (Paez, 2017).
Future research could distinguish between chronic and acute lower back pain to allow for more specific identification of barriers and facilitators to return to work at various stages of rehabilitation. Similarly, focussing on particular groups of workers (e.g. factory or agricultural workers) might enhance the transferability of findings. Exploring differences between workers who sustained injury at or outside of work may also have a bearing on return-to-work practices, particularly if the former adds a further layer of complexity due to involvement of workplace compensation factors.
Conclusion
This review suggests that there are shared experiences among back-injured workers from different work settings and countries who are attempting to return to work. This meta-ethnography supports previous findings which emphasise consideration of wider organisational and psychosocial influences in supporting a person to return to work, rather than placing blame with the injured worker. The review highlights that some existing return-to-work practices might not comply with legislation, thereby hindering progress towards greater equality and anti-discrimination. The review provides some suggestions for modification of current return-to-work practices, and emphasises the need for a strengths-based approach to rehabilitation. Suggestions are made for occupational therapists who might work with people living with back pain.
Key findings
Challenges in returning to work relate to person characteristics, social support and the workers’ organisation return-to-work process. Sociocultural stereotyping is harmful for injured workers.
What the study has added
A greater understanding of how people with lower-back injuries can be best supported when attempting to return to work. Consideration of how occupational therapy practice can facilitate the return-to-work process.
Footnotes
Acknowledgements
Thanks are extended to Audrey Yong (Senior Lecturer, University of Brighton) for her feedback on an initial draft of this paper.
Research ethics
Ethics approval was not required for this study.
Declaration of conflicting interests
The author(s) confirm that there is no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.
Contributorship
Rebecca Robart and Paul Boyle contributed to the conceptualisation and design of the review. Rebecca Robart conducted the database/literature search, screened titles and abstracts, screened full texts and refined the inclusion/exclusion criteria. Rebecca Robart extracted, collated and summarized the data in consultation with Paul Boyle. Rebecca Robart maintained a reflexive diary and discussed concept development with Paul Boyle. Both authors reviewed and edited the manuscript and approved the final version.