
Abstract
Introduction
The study aims were to assess impact of an intensive camp-based intervention using a hybrid model of modified constraint induced movement therapy with bimanual therapy in children with upper extremity impairment, and to see if improvements persisted over time.
Method
Twenty subjects participated. Eight subjects attended camp 2 years in a row, and 12 subjects attended camp only 1 year. The Assisting Hand Assessment and Children’s Hand-use Experience Questionnaire were administered before and after camp. Assisting Hand Assessment and Children’s Hand-use Experience Questionnaire scores were compared between assessments using linear mixed effects models, adjusting for covariates (age and Manual Ability Classification System level) and the repeated measures within subjects.
Results
Assisting Hand Assessment score improved during the intervention phase for subjects at all Manual Ability Classification System levels (p ≤ 0.0001). Improvement was maintained long-term at 1 year post. Children’s Hand-use Experience Questionnaire scores for grasp efficacy and time taken were significantly improved during intervention but not maintained at 1 year post. The feeling bothered dimension showed no significant change over time.
Conclusion
A hybrid model of modified constraint induced movement therapy and bimanual therapy was effective in improving bimanual function for children with varying levels of neurologic hemiparesis, with changes maintained long-term.
Keywords
Introduction and literature review
Unilateral upper extremity weakness or paresis in children can be caused by congenital and traumatic conditions affecting the central nervous system (CNS). Examples of these congenital and traumatic conditions include cerebral palsy (CP) with hemiparesis or peripheral nerve system injuries such as perinatal brachial plexus injury. Children with upper extremity weakness or paresis have difficulty performing unimanual and bimanual activities, affecting their ability to execute daily tasks for successful participation at home, school, and other environments (Gordon et al., 2005).
During early stages of motor development, children with hemiparesis experience unsuccessful attempts and negative feedback when performing bimanual tasks. Children learn that the affected upper extremity is not an effective stabilizer or manipulator (Gordon et al., 2005; Taub, 2004; Taub et al., 2004). Children may learn strategies using only one hand to play and perform daily activities. This leads to avoidance or learned non-use of the affected upper extremity, which is known as “developmental disregard” (DeLuca, 2002; Gordon et al., 2005; Hoare et al., 2007).
Growing evidence supports constraint induced movement therapy (CIMT) and modified constraint induced movement therapy (mCIMT) as effective interventions for improving upper extremity activities and self-care in children with CP (Novak et al., 2013). CIMT is an upper extremity intervention that includes two key components: (a) restraint of the unaffected upper extremity paired with (b) intensive structured practice (Taub et al., 2004). In the original model of CIMT, the unaffected upper extremity is restrained for 90% of waking hours for a minimum of 2 weeks, and 3 or more hours of intensive training is provided (Taub et al., 1993, 1999). mCIMT is an adapted version of CIMT that varies from Taub’s original model in the type of restraint used, type of structured motor training, duration of intervention per day, length of program, location, context, and/or provider training (Eliasson et al., 2014). Using CIMT and mCIMT, the therapist aims to improve motor performance by overcoming learned non-use or developmental disuse. Cortical reorganization results from motor training (Inguaggiato et al., 2013; Mark and Taub, 2004; Taub, 2004).
CIMT appears to improve motor performance of the affected upper extremity, which may impact bimanual performance, but does not specifically target bimanual coordination impairments (Charles and Gordon, 2007). Bimanual therapy is an evidence-based, assessment-driven intervention aimed at coordinating the activity of the affected hand with the dominant, non-affected hand (Gordon et al., 2007). Bimanual therapy directly addresses impairments in bimanual coordination through massed practice of bimanual hand function (Aarts et al., 2012). Research supports that bimanual therapy implemented at the same frequency/intensity as CIMT results in benefits that are equivalent to CIMT (Deppe et al., 2013; Fedrizzi et al., 2013; Gordon et al., 2011; Sakzewski et al., 2011).
Hybrid models of upper extremity intervention may address the strengths and weaknesses of CIMT and bimanual therapy. A recent systematic review postulates that a combined approach may yield greater gains compared to CIMT or bimanual approaches alone (Dong et al., 2013). Research studies investigating the effects of this combined approach are few but emerging (Aarts et al., 2010; Boyd et al., 2013; Brandao et al., 2010).
A group of experts identified various “knowledge gaps” in CIMT research, including type of practice, type of structured skills, long-term outcomes, and predictive factors such as severity of impairments. Research studying the effectiveness of hybrid approaches is limited. The purpose of this study was to (a) assess the impact of an intensive camp-based intervention using a hybrid model of mCIMT with bimanual therapy; (b) assess the impact of this hybrid model on children with varying severity of neurologic hemiparesis; and (c) investigate whether this model of intervention would sustain change over time. We hypothesized that participation in the camp would improve bimanual hand function in school-aged children with varying severities of neurologic hemiparesis, and improvements would be sustained long-term, as measured by the Assisting Hand Assessment (AHA) and Children’s Hand-Use Experience Questionnaire (CHEQ 2.0).
Method
Participants
This study was approved by the hospital’s Institutional Review Board with a waiver of consent for retrospective use of data collected previously for clinical purposes. A retrospective review was conducted of subjects participating in a summer constraint induced movement therapy camp at our institution during the years 2015 to 2017. Requirements for camp participation included age 6–12 years, upper extremity weakness or paresis from non-progressive CNS impairments, Manual Ability Classification System (MACS) levels I–III (Eliasson et al., 2006), no visual impairments, and the ability to follow directions.
Measures
Two assessment tools were chosen for this study to reflect typical manual performance rather than maximal capacity. The AHA is a Rasch-developed assessment tool with established validity (content and construct), reliability (inter/intra-rater, test–retest), and responsiveness to change with treatment for children aged 18 months to 12 years with unilateral upper extremity impairments (Eliasson et al., 2005; Holmefur et al., 2007; Krumlinde-Sundholm et al., 2007). The AHA is a standardized, criterion-referenced assessment designed to measure how effectively children perform bimanual activities. It measures quality and quantity of bimanual upper extremity use through 22 items scored on a four-point scale, with scores expressed in logits (log-odds probability units, used to transform ordinal data to an interval scale with a hierarchical structure of difficulty). Higher AHA logit scores indicate better bimanual functional performance (Krumlinde-Sundholm and Eliasson, 2003; Velozo et al., 1999). As a measure of typical performance rather than best capacity, changes in AHA scores likely reflect a change in bimanual hand-use suggesting that a new motor pattern has been integrated (Hoare et al., 2007; Klingels et al., 2010; Krumlinde-Sundholm and Eliasson, 2003). AHA version 4.4 was used and raw scores converted to AHA units using the conversions referenced in Krumlinde-Sundholm (2012). The smallest detectable difference (SDD) for the AHA is four raw scores, five AHA units (Klingels et al., 2010). The AHA was administered by AHA-certified occupational therapists for all study subjects. Inter-rater reliability for AHA scoring among the occupational therapists was tested and found to be high [average ICC 0.98, coefficient of variation 7% (+/– 2)].
The CHEQ 2.0 was also administered to campers. The CHEQ is a questionnaire that describes how children with unilateral upper extremity impairments use the affected hand during everyday bimanual activities (Skold et al., 2011). The parent and child provide responses on 27 activities, specifically whether activities are performed independently and if one or two hands are used. There are also questions about perceived hand-use, time taken to complete activities as compared to peers, and experience of feeling bothered while doing certain activities (Amer et al., 2016). The CHEQ has been validated (content and construct validity) for children and youth ages 6–18 years of age with unilateral impairments and confirmed by Rasch Analysis (Skold et al., 2011). The CHEQ was chosen as it is readily available online, fairly quick to administer, and provides information on each child’s experiences of how they perform daily tasks. It should be noted that raw score data from 2015 had to be converted from the old CHEQ version to logits or a 0–100 scale to be compatible with CHEQ 2.0, as the new version was not available at the time of the camp.
Occupational therapists assessed each subject at two different time points each year of camp attendance: 1 month prior to the start of camp and on the last day of camp. The timeline of assessments is detailed in Figure 1.
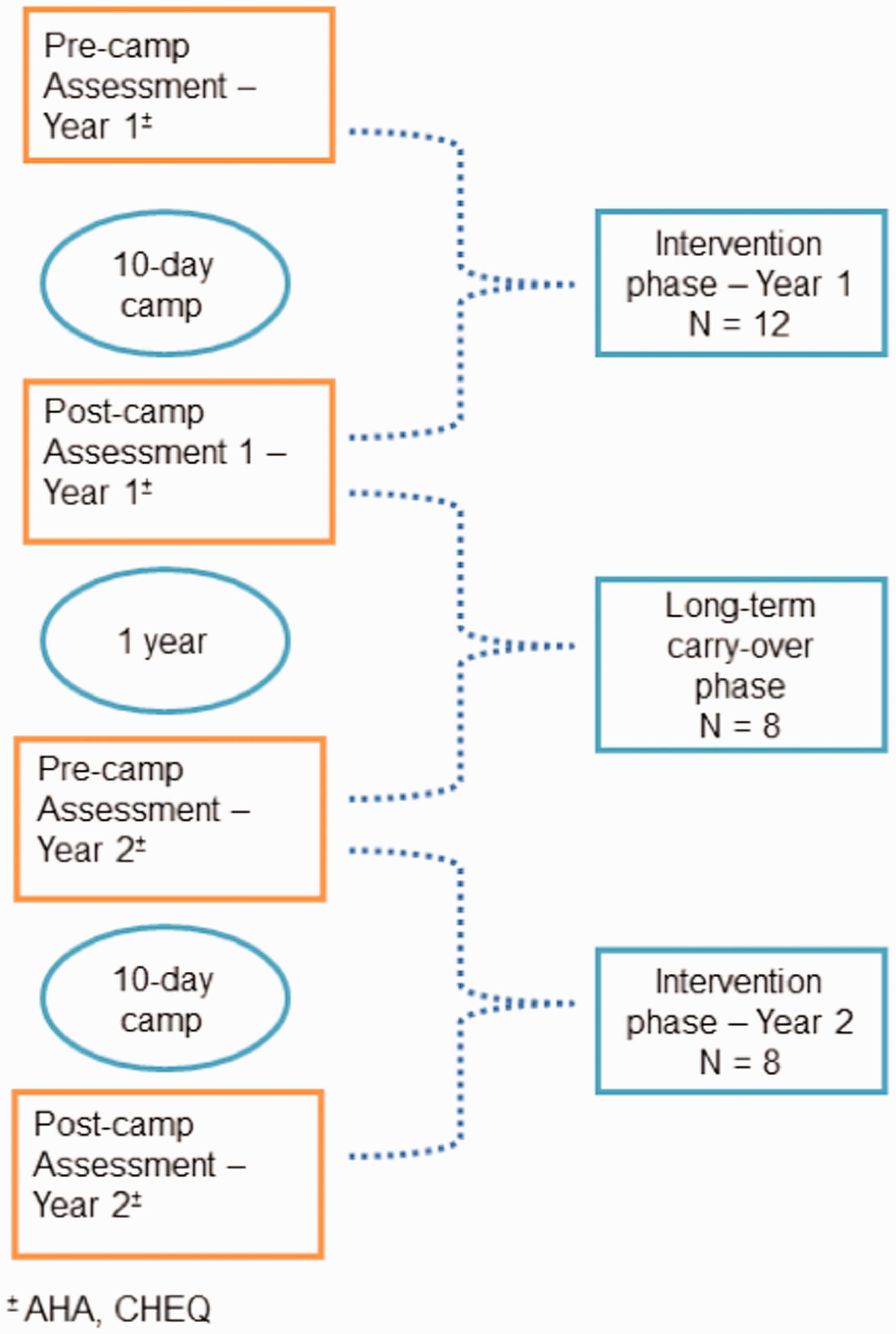
Assessment timeline.
Intervention
Camp was held during the summer for 6 hours per day for 10 days with a 2-day weekend break in the middle, for a total of 60 hours of intervention. Using a hybrid model, the intervention included 2 hours of mCIMT immediately followed by 4 hours of bimanual therapy. A pre-fabricated hand splint that restricted motion from the fingertips to mid-forearm was used as a constraint on the dominant hand during mCIMT (Hoare et al., 2010).
Occupational therapists and occupational therapy interns led camp activities. All occupational therapists were experienced in evaluating and treating children with hemiparesis and were certified in using the AHA. All occupational therapy interns had been trained in treatment of hemiparesis and concepts of the AHA, and were supervised by the occupational therapists. Therapists worked with the children at a 3:1 child-to-therapist ratio, assisted by “sidekick counselors” (other therapists from the Rehabilitation Department) and other allied health professionals (music therapy, animal-assisted therapy, art therapy).
The occupational therapists set individualized goals for each camper based on their pre-camp AHA assessment. Goals were determined based on emerging hand skills that the occupational therapist judged the child would be able to attain by end of the two-week period. Figure 2 illustrates goal determination based on pre-test AHA goals and the child’s MACS level. The figures show examples of how a theme-based activity was adapted to appropriately challenge a child’s skill level and enhance motor learning by grading the activity, adequately placing activity items, and using verbal cues. For a child functioning at MACS level I, goals included advanced skills that are near the top of the AHA Rasch-analyzed hierarchy of bimanual skills such as in-hand manipulation (Figure 2). For a child at MACS level III, appropriate goals were to stabilize objects with grip/support or focus on upper arm movements that are lower bimanual skills on the hierarchy (Figure 2).
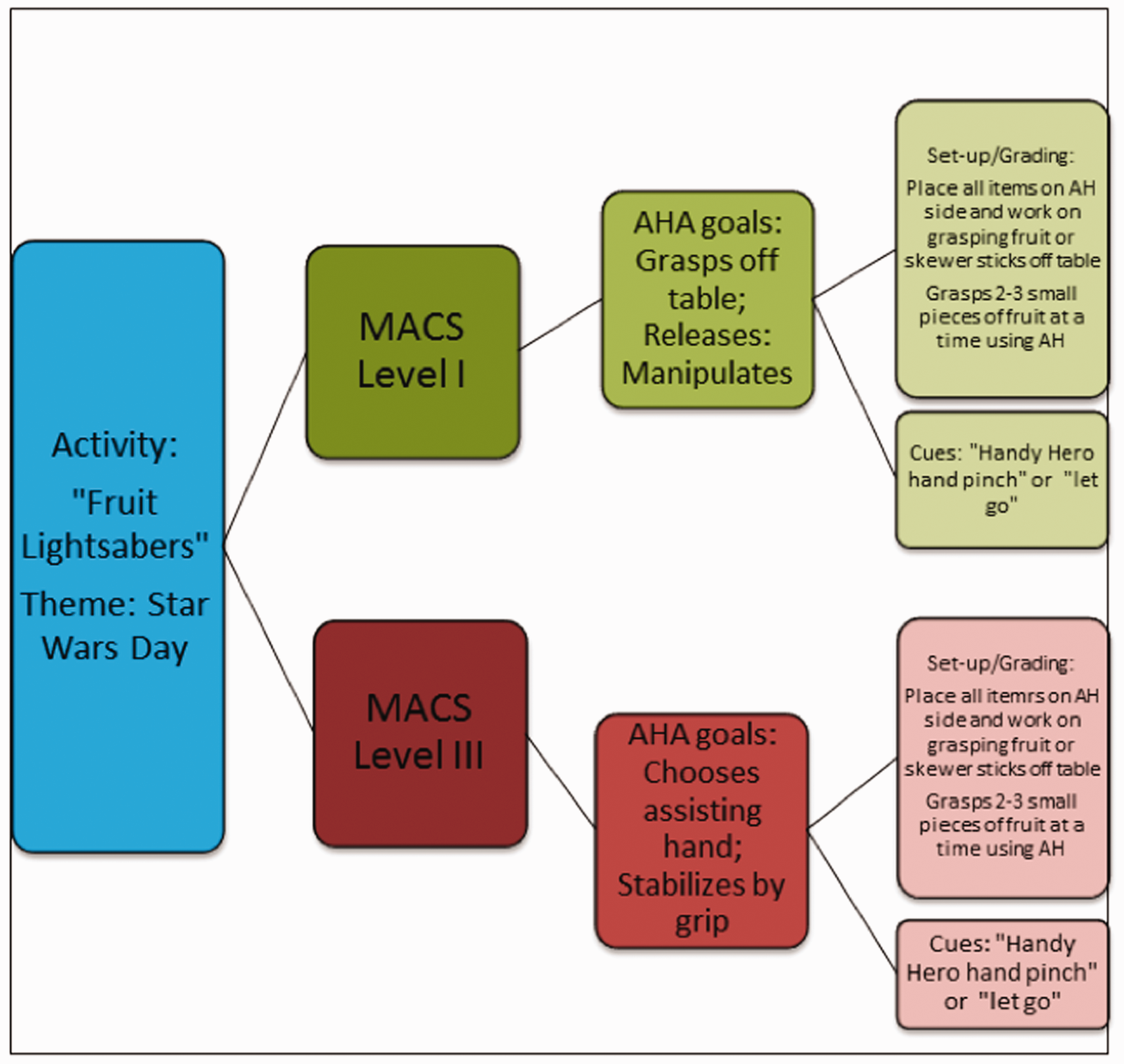
Sample of individual goal determination for children functioning at MACS levels I and III.
Camp activities were designed around “hero” themes aimed at capturing the intrinsic motivation of a child to play. Sample activities included superhero training courses, animal-assisted obstacle courses, arts and crafts, music, water play, yoga, gardening, and snack preparation that reflected the “hero” theme of each day. In addition to motivational aspects, benefits of hero-themed activities in a group setting included empowerment and peer encouragement. From the start of camp, the affected hand was referred to as the “Handy Hero” hand to empower each child. A closed group Facebook page was also utilized to create a sense of community among staff, campers, and families (Aarts et al., 2012). Finally, families were invited to a “Cape-ing” ceremony at the commencement of camp to highlight the learned skills and achievements of each camper.
Analysis
Statistical analysis was conducted using STATA software (version 12.1, StataCorp, College Station, Texas, USA). Means and standard deviations were calculated for baseline subject characteristics. AHA and CHEQ scores were compared between assessments using linear mixed effects models, adjusting for covariates (age, MACS level) and the repeated measures within subjects. Specifically, participant was included as a random effect in the linear model, while visit, age, and MACS level were included as fixed effects. Significance was set at p < 0.05.
Results/findings
Twenty subjects participated in the camp between 2015 and 2017, and were included in the data analysis. Subject demographics and baseline AHA and CHEQ scores are presented in Table 1.
Subject demographics and baseline information.
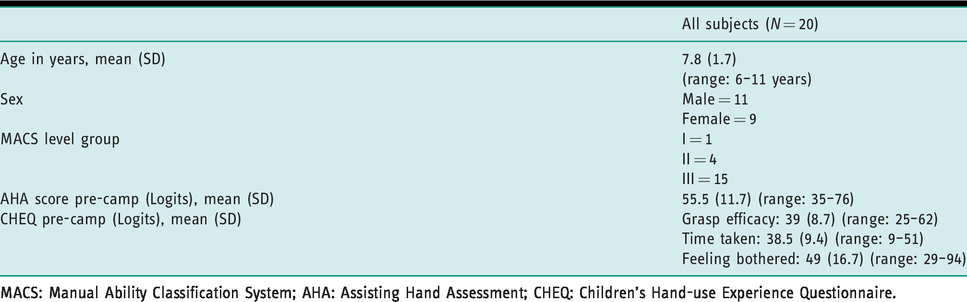
MACS: Manual Ability Classification System; AHA: Assisting Hand Assessment; CHEQ: Children’s Hand-use Experience Questionnaire.
The 20 subjects were all diagnosed with cerebral palsy, unilateral involvement. Eight subjects attended camp 2 years in a row and were tested four times. Twelve subjects attended camp only 1 year and were tested two times.
Change for the AHA was significant during the first 2 years of camp. AHA scores improved pre- to post-camp (intervention) each year, and the improvement was maintained between post-camp the first year and pre-camp the next year (carry-over) (Table 2). Improvement was independent of age and MACS level. Nine of 20 subjects (45%) experienced a change greater than or equal to the SDD of 5 AHA units during the first year of camp, and 7/9 (78%) in the second year, with a combined total of 16/29 campers (55%) experiencing such change in both years.
AHA scores (data are presented in mean logits (SD)).

AHA: Assisting Hand Assessment.
a Pre-1 vs. Post-1 (p < 0.0001), Pre-1 vs. Pre-2 (p = 0.02), Pre-1 vs. Post-2 (p < 0.0001).
b Differences unrelated to MACS level (level II–p = 0.28, level III–p = 0.07) and age (p = 0.82).
CHEQ scores for grasp efficacy and time taken were significantly improved during camp the first year (intervention) but declined significantly to pre-camp levels between the post-camp assessment the first year and the pre-camp assessment the next year (carry-over). These changes were unrelated to age or MACS level. Though improvements were seen in these dimensions of the CHEQ during the second camp year they did not reach statistical significance, likely due to limited sample size in the second year. The feeling bothered dimension showed no significant change over time (Table 3).
CHEQ scores (data are presented in mean logits (SD)).
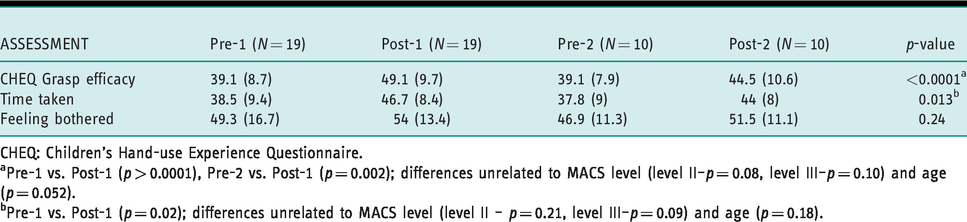
CHEQ: Children’s Hand-use Experience Questionnaire.
aPre-1 vs. Post-1 (p > 0.0001), Pre-2 vs. Post-1 (p = 0.002); differences unrelated to MACS level (level II–p = 0.08, level III–p = 0.10) and age (p = 0.052).
bPre-1 vs. Post-1 (p = 0.02); differences unrelated to MACS level (level II – p = 0.21, level III–p = 0.09) and age (p = 0.18).
Discussion and implications
The study results show that use of a hybrid model of mCIMT in a theme-based camp setting is feasible and effective in producing improvements in bimanual function for children with neurologic upper extremity involvement. Improvements were seen in children with hemiplegia functioning at MACS levels I–III, supporting our first hypothesis that children would benefit regardless of the magnitude of their impairment. The intervention design of this hybrid study differed from other hybrid model studies of a prolonged session of mCIMT followed by a shorter session of bimanual therapy. For example, Aarts et al. (2012) investigated the effectiveness of 6 weeks of mCIMT followed by 2 weeks of bimanual training (Aarts et al., 2010). The intervention used by Brandao et al. (2010) included 2 weeks of mCIMT followed by 1 week of bimanual training (Brandao et al., 2010). Boyd, et al. (2013) proposed a study design that comprises of 5 days of mCIMT followed by 5 days of bimanual therapy compared to a standard care group (Boyd et al., 2013). Both Aarts et al. (2012) and Brandao et al. (2010) found that the hybrid groups demonstrated significant improvements in most assessments measuring activity and participation outcomes, including the AHA (Aarts et al., 2010; Brandao et al., 2010). The current study offered mCIMT and bimanual training on the same day. The gains made from mCIMT training could then be applied immediately to practice in bimanual coordination activities.
The gains in bimanual function (as measured by the AHA) made during camp were maintained at 1 year post-camp, which is a finding that matched our expectations. CHEQ scores for grasp efficacy and time taken were significantly improved during camp the first year (intervention), but declined significantly to pre-camp levels between the post-camp assessment of the first year and the pre-camp assessment the next year (carry-over). These changes were unrelated to age or MACS level. Though improvements were seen in these dimensions of the CHEQ during the second camp year they did not reach statistical significance, likely due to limited sample size in the second year. The feeling bothered dimension showed no significant change over time. This raises the question of whether the intervention model used leads to sustained changes in caregiver’s perception of their child’s bimanual function in daily activities performed at home. An increase in bimanual function or changes within the International Classification of Functioning, Disability and Health (ICF) Activities Level may not necessarily translate to caregiver perceptions of child’s participation in meaningful occupations over time.
Implementation of the hybrid model of mCIMT in a camp-based setting with children of varying functional ability was challenging but also motivating and rewarding for all involved. Individualized goals were established and supported each child’s progression of bimanual hand function. Therapeutic activities were adjusted to provide the “just right challenge” to recruit children’s intrinsic motivation (Miller et al., 2016). Children engaged in group tasks and encouraged each other to persevere through challenging activities, enhancing therapeutic outcomes. Children were initially frustrated by mCIMT activities but, as camp progressed and skills improved, they were more easily engaged in the graded challenging tasks. Parents commented on the benefits of social peer interaction among children with similar physical challenges. They expressed a sense of community and belonging, especially as each child completed the same challenging activities.
Therapists who provided intervention during camp were certified in the AHA with experience applying the AHA Rasch analysis hierarchy to treat children with hemiparesis. Programs using hybrid models should consider incorporating at least one therapist who is certified in the AHA to support goal-setting and provider training.
Limitations
Due to limited resources and time constraints, the pre-camp assessment was performed 1 month prior to start of camp. There is a possibility that changes seen during the intervention phase may have occurred or begun in the month before camp participation started, though this is unlikely. Single-group design and use of non-blinded assessors were limitations to this current study. Finally, small sample size is a limitation to the current study, and the findings should be confirmed with a larger group of children.
Conclusion
This paper describes an intensive, theme-based summer camp program using a hybrid model of modified constraint induced movement therapy and bimanual therapy that was effective in improving bimanual function for children with neurologic hemiparesis across MACS levels I–III, with changes sustained 1 year after camp. However, improvement in perception of grasp effectiveness and time taken during bimanual activities after intervention was not maintained 1 year after camp. Further exploration of this is warranted.
Key findings
A theme-based hybrid mCIMT camp is feasible and effective. Bimanual function improvement was maintained at 1 year for MACS levels I–III. Perception of grasp efficacy and time efficiency showed shorter-term improvements.
What the study has added
This study provides evidence that camp-based hybrid CIMT is effective for improving bimanual function in children with varying levels of unilateral impairment, and may improve parent perception of grasp efficacy and time efficiency.
Footnotes
Research ethics
Full ethics approval (CCI-10-00041, 2019).
Declaration of conflicting interests
The authors confirm that there is no conflict of interest.
Consent
A waiver of consent was granted by the authors’ institution for retrospective use of data collected previously for clinical purposes.
Contributorship
Gina Kim Lee and Marielle Pascual conceptualized and directed the camp, trained camp personnel, and recruited participants. Gina Kim Lee and Marielle Pascual also applied for and maintained ethical approval for the retrospective study, collected outcome data, performed literature review, and wrote the initial draft of the manuscript. Susan Rethlefsen contributed to the retrospective study design, performed statistical analysis and interpreted results, contributed to manuscript preparation and revision. All authors reviewed and edited the manuscript and approved the final version.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.