
Abstract
Introduction
Postural tachycardia syndrome is a form of orthostatic intolerance that often leads to functional impairment.
Methods
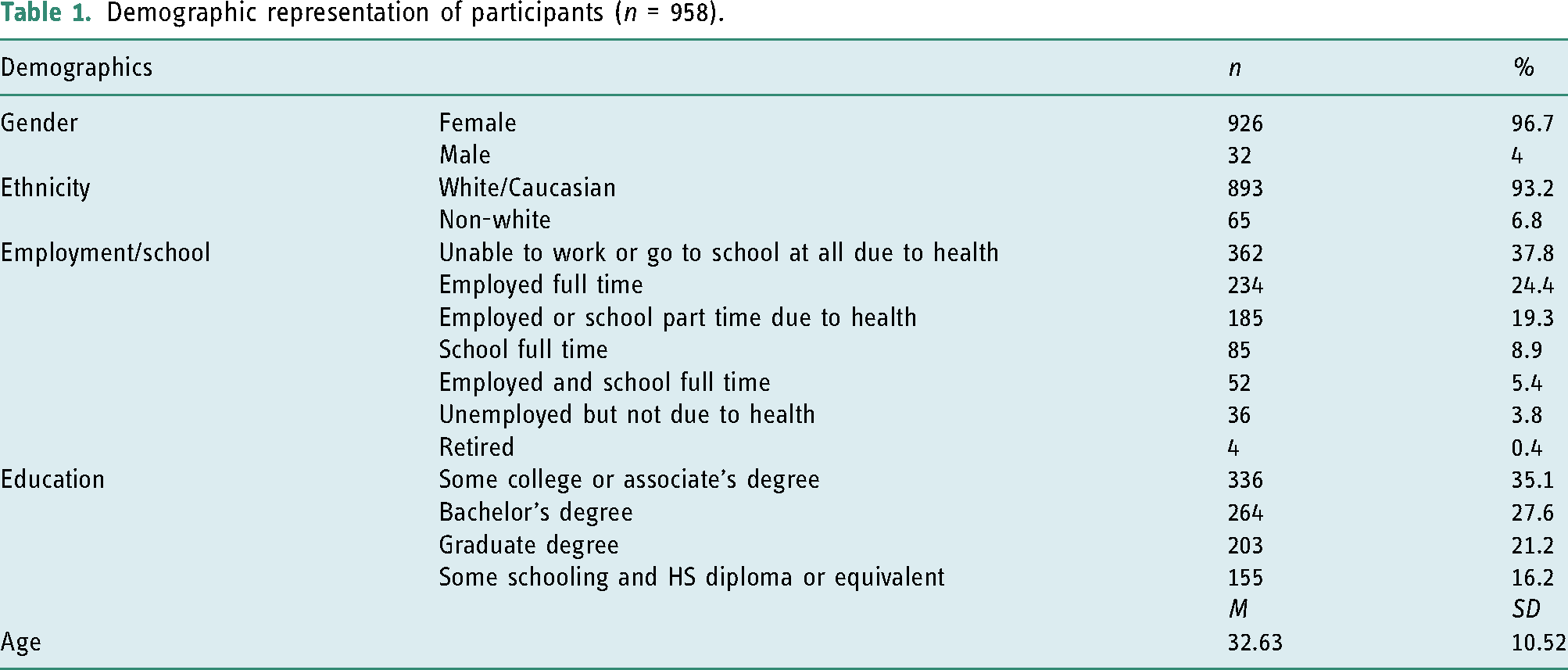
This survey explored functional status and impact of symptoms in adults (n = 958) ages 18 to 60 (M = 32.63 ± 10.52 years, 96.7% female) with postural tachycardia syndrome.
Results
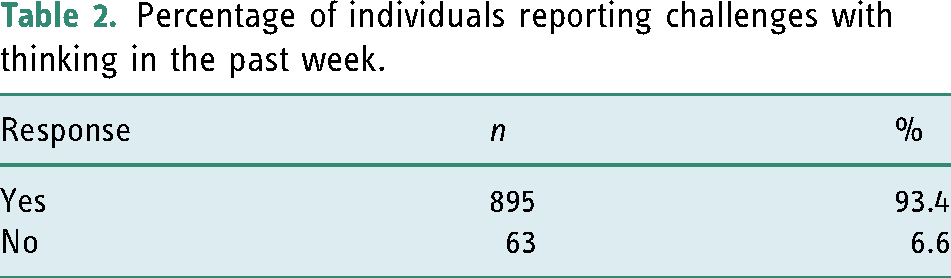
Individuals reported an average of 11 daily life activities impacted by postural tachycardia syndrome with high levels of self-perceived disability. Additionally, 93.4% reported some degree of cognitive impairment and falls occurred in 55.3% of participants annually. Despite frequent falls and functional impairment, participants infrequently (26.9%) utilized therapy services.
Conclusion
Individuals with postural tachycardia syndrome are at an increased risk of experiencing disability and often require assistance with daily activities. Further research is necessary to understand the potential role of therapy in improving function and quality of life.
Introduction
Postural tachycardia syndrome (POTS) is a relatively common form of orthostatic intolerance, with an estimated prevalence between 500,000 and 3,000,000 Americans, often with many symptoms that suggest impairment in multiple body systems (Garland et al., 2015). Symptoms of orthostatic intolerance in POTS patients may include tachycardia, postural lightheadedness, pre-syncope and syncope, palpitations, chest pain, nausea, cognitive impairment, visual disturbances, lower extremity weakness, shortness of breath, headache, neck pain, flushing, abnormal sweating, and anxiety (Goodman, 2018). Patients with POTS report several other symptoms that are not orthostatic in nature. These non-orthostatic symptoms may affect the quality of life and the ability to carry out daily activities. Examples of non-orthostatic symptoms frequently reported by POTS patients include gastrointestinal signs (nausea, dysphagia, abdominal pain, constipation, and diarrhea), pain, fatigue, cognitive symptoms (often referred to as brain fog), and urinary symptoms. Women of childbearing age are the most likely to experience POTS (Thieben et al., 2007). The cause of POTS is unclear. Postural tachycardia syndrome patients commonly report a history of antecedent illness before symptom onset. Others may report the onset of symptoms following concussion or surgical procedure. While many individuals have no obvious identifiable precipitating event, co-morbid conditions such as Ehlers-Danlos syndrome, migraine, mast cell activation syndrome, chronic fatigue syndrome, and chronic pain conditions may be present in POTS patients (Goodman, 2018). Regardless of the cause, patients with POTS experience deconditioning and exercise intolerance, whether at the onset of symptoms or following a resultant decrease in activity level (Fu and Levine, 2018). Treatment of POTS most commonly includes prescription medications and lifestyle recommendations such as exercise, increased salt and fluid intake, elevating the head of the bed, and the use of compression garments (Sheldon et al., 2015).
The root cause of POTS is unclear, which leads to challenges in understanding functional deficits. Patients with POTS frequently have diminished sleep quality. Patients report increased fatigue, daytime sleepiness, and sleep problems (Bagai et al., 2011). The levels of fatigue and sleepiness are similar to those with chronic fatigue syndrome; however, individuals with POTS have a significantly higher autonomic symptom burden (McDonald et al., 2014). Researchers have suggested pain to be a factor in function (Cook and Sandroni, 2018). Cognition is one of the most prevalent and debilitating symptoms (Miller and Raj, 2018; Raj et al., 2018; Ross et al., 2013). Cognitive dysfunction often presents with difficulties in word-finding, attention, processing speed, and executive function (Raj et al., 2018; Rich et al., 2020). Psychosocial factors may play a role in the degree of functional disability, including hypervigilance and catastrophic cognitions (Benrud-Larson et al., 2003).
Due to the diverse and often severe symptoms that suggest impairment in multiple body systems, patients often lose independence and decrease participation. Benrud-Larson et al. (2002) reported that approximately 25% of individuals are disabled and unable to work. Previously, researchers have suggested functional impairment to be similar to individuals with chronic obstructive pulmonary disease or congestive heart failure (Sheldon et al., 2015). In a pilot survey study that we conducted of 674 individuals with POTS, all participants identified functional limitations because of POTS symptoms with the highest incidence of limitation in the following areas in descending order: exercise, cooking, physical demands of work, bathing, and getting out of bed in the morning (Rich et al., 2018). Welford and McKenna (2016) found that 76.8% of individuals with POTS require assistance during self-care activities, and 29.3% cannot work as a direct result of symptoms. There is a need to expand on existing literature with more detail regarding specific domains of function, the prevalence of rehabilitation and falls, and the use of strategies and tools.
Studies documenting non-pharmacologic rehabilitation intervention are limited. There have been two clinical studies documenting improvement in symptoms through exercise training (Fu et al., 2010; Winker et al., 2005). Although single-subject case studies have been published in occupational and physical therapy treatment, there are no studies that characterize and quantify explicit deficits in each functional domain and there is a gap in publications evaluating non-pharmacologic interventions such as rehabilitative therapies.
The aim of this study is to examine the impact of POTS on (a) basic activities of daily living (BADLs), (b) instrumental activities of daily living (IADLs), (c) work and school, (d) rest and sleep (e) leisure and play, and (f) social participation. These domains reflect the Occupational Therapy Practice Framework modified by data from the pilot study (American Occupational Therapy Association, 2020; Rich et al., 2018). Additionally, we share data on treatment strategies that individuals use to compensate for these functional challenges. Through an occupational therapy lens, the researchers set out to understand elements for rehabilitation practice as a whole, including both the use of occupational and physical therapy. Specifically, the researchers analyze functional status, the impact of symptoms on daily life, cognitive status, falls, self-management, and therapy experiences. We hypothesized that participants would identify multiple daily function areas impacted by POTS, especially limitations in functional mobility, work and school, and social participation. We anticipated cognitive impairment in the majority, based on previous studies, and expected falls in a portion of the sample. We also predicted that individuals might have received limited therapy (occupational or physical therapy) but more frequently would utilize self-management strategies to remediate functional challenges.
Method
Participants
We recruited participants via an electronic link on the Dysautonomia International Facebook page over 10 days. Dysautonomia International is a non-profit organization with a worldwide reach; well-respected autonomic researchers utilize it as a source for research recruitment (Shaw et al., 2019). All participants gave electronic informed consent before inclusion in the study. Participants did not receive compensation for their time or efforts. Participants were required to be between ages 18 and 60 and be diagnosed with POTS by a medical doctor. Exclusion occurred if an individual responded as a family member or friend of a person with POTS or outside the stated age requirements.
Design
The present study adopted a survey design with quantitative and qualitative components. The survey contained sections as described throughout this manuscript to include a quantitative single-item functional status question described below and the impact of symptoms on daily life in the month prior by using “select all that apply” from the provided domains. Participants reported cognitive status on a single question regarding the experience of challenges with “thinking” in the week prior. Falls were recorded across the year before the survey, using a single item yes/no response followed by a question regarding the need for medical intervention in those that answered “yes.” Additionally, self-management questions included two topics: (a) strategies with prioritizing the top three most helpful and (b) tools with multiple-select options for use in the month prior. Finally, assessment of therapy experience included a multiple-choice question regarding a history (unlimited time) of receiving occupational therapy, physical therapy, both, or neither, for treatment of POTS symptoms. The authors did not examine patients’ clinical records, rather explored individuals’ perceptions of their lived experience. These individuals’ lived experience is valuable for researchers and clinicians to identify existing strategies found to be successful in addition to understanding areas of focus for treatment and future research.
Procedure
We conducted the survey using the secure web-based platform, PsychData. This study received exception through the Institutional Review Board at the lead university on the study, protocol #20473. Demographic information collected in the survey included age, gender, education status, ethnicity, and employment. Survey questions on the functional domains consisted of multiple-select checkboxes, Likert scales, and multiple-choice questions. A prefacing statement instructed participants to answer all POTS symptom questions to the fullest extent possible, limiting the focus of co-morbid conditions.
Statistical analyses
Descriptive analysis involved IBM SPSS Statistics version 25 to examine the frequencies and percentages for the demographics, the functional domains, adaptive tools and strategies, incidence of cognitive impairment, and types of therapy services (IBM Corp, 2017).
Measures
Linear analog scale of function
One question included a linear analog scale that asked participants “on a scale from 1 to 10, where 1 is not able to do anything in daily life and 10 can do everything you want to do, where would you rate your ability to do the things you want/need to do in daily life?” Participants then responded on a scale with language as follows: “1: I cannot do anything I want or need to do” and “10: I can do everything I want or need to do.” This was a standalone rating and participants were not specifically instructed to compare to prior level of function. Researchers have used these types of rating scales as patient self-assessments to determine the self-perceived level of functioning and allow individuals to communicate the overall quality of life with care providers and researchers (Locke et al., 2007).
Identification of occupational domains
In conjunction with the Occupational Therapy Practice Framework, the pilot study led to focus on the representative domains of occupational performance and excluded those that were not reported to be commonly impacted (e.g., dressing) in this population (American Occupational Therapy Association, 2020; Rich et al., 2018). Additionally, functional tasks identified as frequently challenging due to POTS (e.g., getting out of bed in the morning, morning routine) were grouped using relevant and easy-to-understand language to ensure applicability and comprehension. We operationalized morning routine as “tooth brushing, dressing, cooking/eating breakfast, styling hair, and/or applying makeup.” Functional mobility included “getting around during the day, climbing stairs, and/or wheelchair mobility,” with “falls” defined as “coming to rest inadvertently on the ground or floor or other lower level (World Health Organization, 2018).” In response to this previous work and the occupational therapy framework, we identified the following occupational domains with specific categories, which can be found in Figures 2–4: BADLs, IADLs, work and school, rest and sleep, leisure and play, and social participation (American Occupational Therapy Association, 2020; Rich et al., 2018).
Self-management
The options for self-management, including both the strategies and the tools questions, were determined through response to the pilot study (Rich et al., 2018). We designed the pilot study options for strategies utilizing best-evidence recommendations for managing the condition in journal articles, from patient support groups, and through input from patients who reviewed the survey. Tools were determined similarly, incorporating most frequent recommendations from expert providers in the literature and patient feedback. In the present study, the authors included the most commonly chosen strategies and tools from the pilot study.
Results
Demographic representation of participants (n = 958).
Functional status
When given a single-item numerical linear analog self-assessment, 61.3% of individuals reported their current level of function to be at 5/10 or less (M = 4.87, mode = 3) (Figure 1) (n = 922). Level of functionality as reported on a 1–10 scale where 1 represents inability to do anything the person wants or needs to do in daily life and 10 represents ability to perform all necessary or desired activities.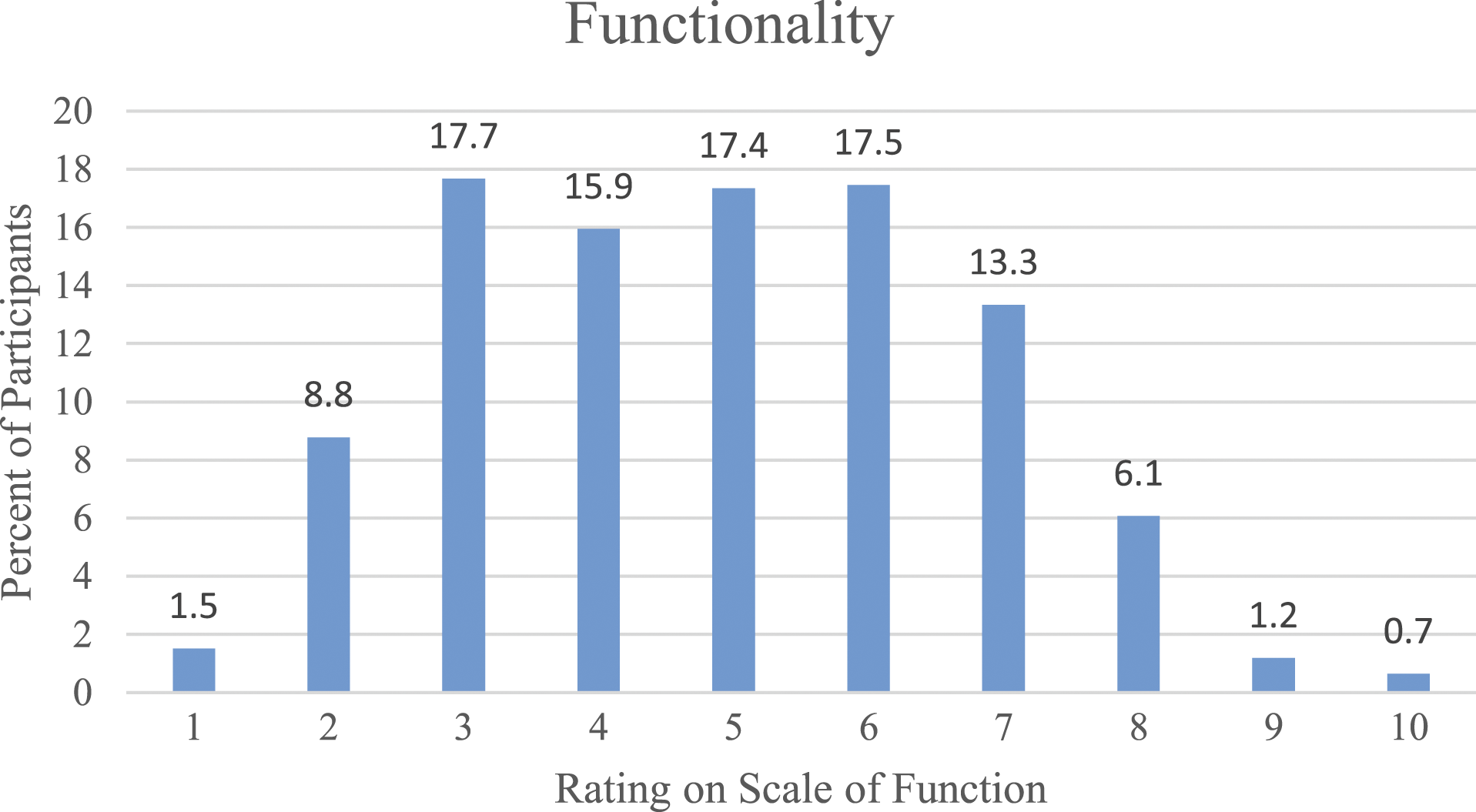
Impact of symptoms on daily life
An overwhelming majority (98.5%) of participants reported that POTS negatively impacted their daily life throughout the month prior to completing survey (n = 958). When all areas of life that were impacted by POTS symptoms were summed per participant, out of a total number of 18 potential areas of daily life, on average there were 11 areas of daily life that were impacted by POTS symptoms (M = 11.03±4.18, range: 0–18). More than 90% of the sample identified five or more areas of life affected (91.2%), and 33% of participants identified 13 or more areas. The basic ADL (BADL) most frequently cited was bathing or showering (79.2%), followed by getting out of bed in the morning (74.6%) (Figure 2). The most common instrumental ADL (IADL) affected was home management (82.2%), followed by shopping (76.8%) and meal preparation and cleanup (75.1%) (Figure 3). While a majority of participants (69.9%) reported impacts to either work or school, 30.1% identified impairment in both domains (Figure 4). Percentage of individuals negatively impacted by postural tachycardia syndrome in their basic activities of daily livings. These domains do not sum to 100% because “check all that apply” was asked for these questions. Percentage of individuals negatively impacted by postural tachycardia syndrome in their IADLs. These domains do not sum to 100% because “check all that apply” was asked for these questions. POTS: postural tachycardia syndrome; IADL: instrumental activities of daily living. Percentage of individuals negatively impacted by postural tachycardia syndrome in additional areas of life. These domains do not sum to 100% because “check all that apply” was asked for these questions.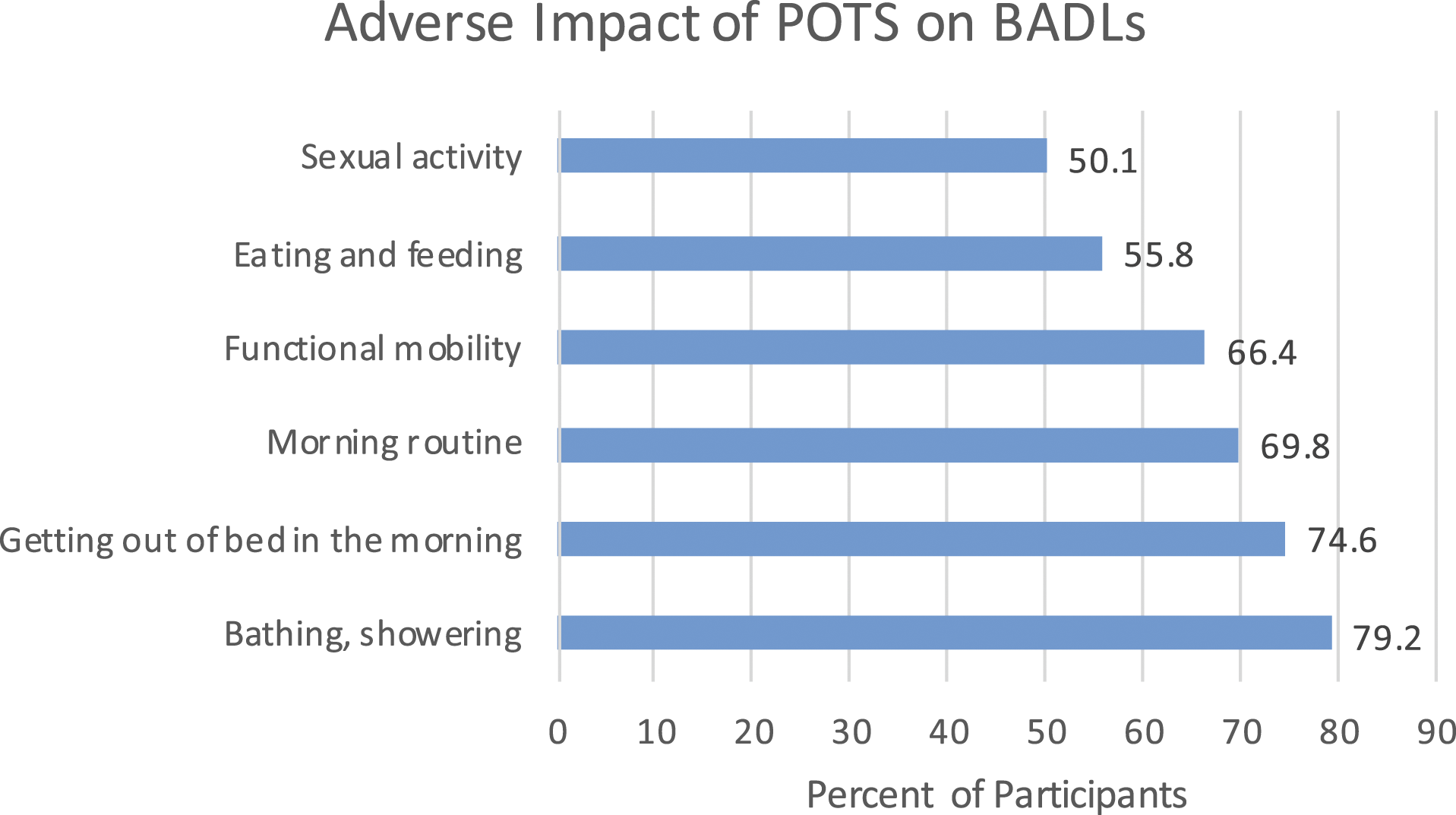


Cognitive status
Percentage of individuals reporting challenges with thinking in the past week.
Falls
In full, 55.3% of participants reported a fall in the past year. A year timeframe was chosen as we anticipated falls to be less frequently occurring; additionally, this is a frequent measure in other populations to serve as a comparison value. Of those who had fallen, a quarter of these individuals required medical attention.
Self-management
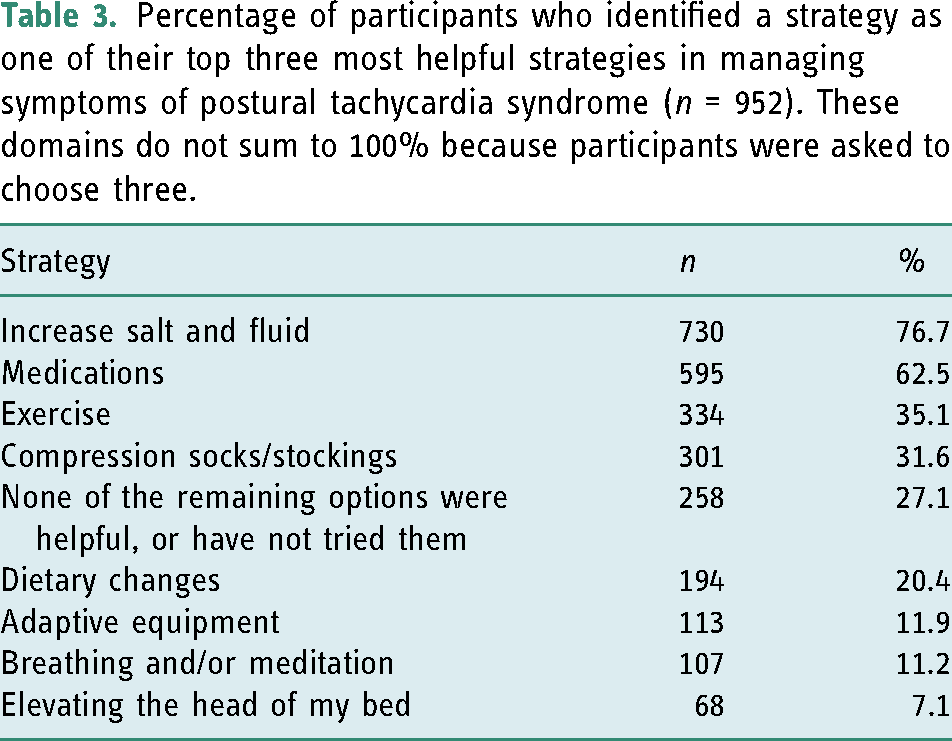
Percentage of participants who identified a strategy as one of their top three most helpful strategies in managing symptoms of postural tachycardia syndrome (n = 952). These domains do not sum to 100% because participants were asked to choose three.
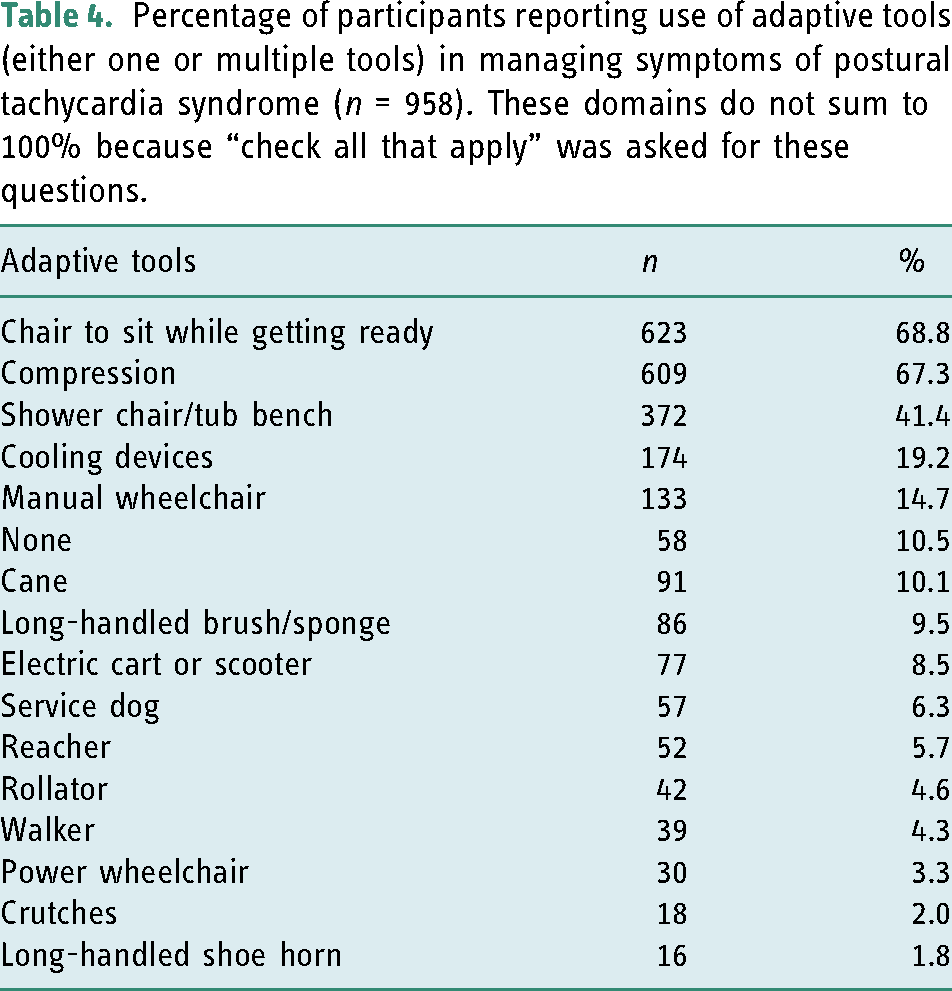
Percentage of participants reporting use of adaptive tools (either one or multiple tools) in managing symptoms of postural tachycardia syndrome (n = 958). These domains do not sum to 100% because “check all that apply” was asked for these questions.
Therapy
Per report, 26.9% of the study sample received occupational and/or physical therapy to treat their POTS symptoms at some point in time. Physical therapy was more highly utilized (25.9%) than occupational therapy (5.5%). A small number received both therapy services (4.4%) (n = 958).
Discussion
Within each category of participant responses, the current study brings to light the impact of POTS on daily function in a population comparable in age and gender but exceeding in prevalence to multiple sclerosis (Wallin et al., 2019). This study demonstrates that individuals with POTS experience high levels of self-perceived impairment, global functional deficits across a variety of specific areas of life, high incidence of cognitive deficits, routine falls, and low utilization of therapy services. Furthermore, the results indicate that individuals with POTS seek treatment strategies to alleviate symptoms and improve participation and the use of compensatory devices. This discussion elaborates on each of the functional domains affected by POTS and proposes potential clinical implications for therapists’ role in improving individuals’ quality of life with POTS. Ultimately, we aim to provide a basis for further clinical research.
The sample was similar to other studies, with previous research documenting an average age of participants at 30.2 years, keeping in mind the present study included only those over the age of 18 (Thieben et al., 2007). Literature has shown a 4.5:1 female to male ratio, and the present study represented a vast majority of female participants (Benarroch, 2012).
Functional status
There is limited documentation of patients’ perceived level of impairment and follow-through on using a variety of interventions and compensatory strategies. This relatively large sample reported substantial impairment in functionality. Symptoms limit more than one-third of participants from working or attending school, which further demonstrates a significant loss of functionality. This level of work and school limitation is slightly higher but relatively consistent with other studies (Benrud-Larson et al., 2002).
Impact of symptoms on daily life
Previous studies have not included the specific domains of daily activity most highly impacted by POTS. However, reports of deficits are almost universally present (98.5%). Perhaps most striking in the study findings was the impact frequency of IADLs (home management, shopping, meal preparation, and driving) and often-overlooked areas of socialization and leisure activities. In isolation or comprehensively, these activities likely contribute an underappreciated amount to a decrease in quality of life. Studies less commonly cite these domains in the literature and discussion of interventions to address these functional deficits is almost non-existent in this population. Patients may feel less compelled to share their challenges with these under-recognized areas due to a fear of stigma, the underappreciated necessity of these skills for quality of life, and/or limited time in providers’ offices to open a broader dialogue. Regardless, it is crucial to notice the incidence of these challenges with IADLs, socialization, and leisure.
It is worthwhile to emphasize that despite the relatively low-frequency reports of impact on child-rearing (20.8%), religious/spiritual activities (31.4%), and school (38.5%), these areas were not applicable for all participants. Therefore, influences on these other activities are comparable to BADLs in the segment of the population affected (e.g., parents, individuals with faith, and students). Similarly, the results regarding the impact of symptoms on work may be underrepresented as a portion of the study sample may not be pursuing work endeavors due to age or stage in life. Even so, these data are relevant in directing health care providers to address commonly reported areas of impact while taking roles and routines into consideration.
Cognitive status
The vast majority (93.5%) of the sample reported cognitive impairment. Known areas of impairment in this population include attention, executive function, processing speed, and memory, with frequent reports of brain fog, forgetfulness, challenges with word-finding, and difficulty thinking (Raj et al., 2018). These deficit areas are not unlike what is observed in patients with other central nervous system disorders, occurring in POTS approximately 1.3–2 times as often as outcomes on neuropsychology batteries in multiple sclerosis and Parkinson disease (Benedict et al., 2006; Sumowski et al., 2018; Yang et al., 2016). Note that these reports are based on objective outcomes from standardized assessments, instead of patient-reported perception of impairment, as was used in this study. In a self-reported study of 3108 cancer survivors following treatment, the incidence of cognitive dysfunction was half of that reported in the present study, with similar impairment (Schmidt et al., 2016). Additional research is needed to identify the objective prevalence of cognitive impairment in individuals with POTS; however, from a clinical standpoint, a patient’s self-perception of impairment is often meaningful for understanding patient needs and experience of their condition. These cognitive challenges likely impact socializing with friends and family, work responsibilities, school, driving, and financial management among other tasks. BADL limitations, while less directly impacted by cognitive impairments, are still clinically reported by patients as “fogginess” exacerbated by positional changes or actions such as standing in a hot shower (Ross et al., 2013). Patients report cognitive impairment as one of the most debilitating symptoms of the condition with a known adverse impact on the quality of life (Raj et al., 2018). Although participants self-reported cognitive challenges are extremely valuable, objective standardized performance-based characterization of cognitive domains could help generalize the findings and more importantly address strategies to mitigate them. Further research is necessary to understand better the mechanism of cognitive impairment, and potential treatment modalities, given the breadth of resulting functional deficits for the patients.
Falls
Not only do symptoms limit participation in daily life, but in this study, over half of the participants (55.3%) reported falling in the past year, and a quarter of those falls required medical attention. Most concerning about these falls are the possibilities of head injuries, which may further worsen symptoms. The CDC reports that one in five falls results in serious injury, and falls contributed to more than US$50 billion in medical costs in 2015 (Centers for Disease Control and Prevention, 2019). Commonly reported symptoms in patients with POTS—lower body weakness, difficulty with walking and balance, and vision problems—are frequently cited as risk factors for a fall (“Important Facts about Falls,” 2017). The environment and circumstances around these falls are unclear, limiting the understanding of the cause. Cognitive impairment in patients with more severe deficits may lead to more falls. We would expect a portion of falls to occur in the shower due to static standing in a warm environment, taking into account the mechanism of orthostatic intolerance and anecdotal evidence. Less than half of participants reported use of a shower chair or tub bench; this could be due to various factors including the stigma of using medical equipment, lack of knowledge regarding equipment, restricted financial means, and/or poor recognition of symptom onset and need to sit. Due to the nature of orthostatic symptoms, falls are likely to occur in positions of static standing (e.g., waiting in lines or shopping), moving from a position of recumbency to standing (e.g., getting out of bed or rising from chair/floor), and/or with increased exertion (e.g., exercise or climbing stairs). The use of durable medical equipment such as a shower chair or mobility device may play a role in decreasing additional falls. Per the current study, the cause of falls and the relationship between age and falls is unclear; longitudinal follow up is indicated to better understand this issue.
Self-management
Participants self-identified increased salt and fluid intake as the most effective method for intervention. As this is a thoroughly documented, non-invasive, and well-tolerated first-line treatment in the POTS management, it is not surprising that it was highly cited by the participants. However, it is unclear if this remedy for symptom-reduction results in sustained and impactful improvement, given that most patients continue to suffer from ongoing impairment in function. The specific reason for patients most frequently citing proper fluid balance as efficacious is not concrete, as they may not have tried other strategies, may not have tolerated other methods or adverse side effects, or may truly have not experienced as positive of an effect from other interventions. Additional research is needed to understand the exact prevalence of best outcomes using different approaches.
In a recent survey-based study, nearly one-third of participants with POTS who reported symptom improvement attributed medications as the primary factor (Shaw et al., 2019). In 52% of participants, non-pharmacologic intervention offers some improvement (Shaw et al., 2019). Interventions, both pharmacologic and non-pharmacologic, are limited, and while many individuals may see clinical improvement, most will not be “cured” (Arnold et al., 2018). This ongoing presentation of symptoms highlights the need for specific, targeted intervention to improve patient functionality during valued and meaningful activities.
Therapy
The results showcase the underutilization of occupational and physical therapies, with approximately one quarter receiving one or both services, despite previously reported levels of functional impairment. The reason behind the limited utilization of therapy within the patient population remains unclear. We postulate that this may be a result of multiple factors including (a) lack of research and evidence-based studies in rehabilitation and POTS, (b) knowledge gap for clinicians and absence of instruction on POTS in educational programs, (c) absence of clinical guidelines for therapists, (d) limited awareness of rehabilitation services, (e) adverse experiences in patients who have received therapy, and/or (f) lack of referrals from medical providers.
The average length of time from onset of symptoms until diagnosis is presently 4.7 years (Shaw et al., 2019). Increased awareness of POTS diagnosis and treatment in the medical community is imperative. If physicians and medical staff recognize symptoms of POTS and refer to knowledgeable providers for additional diagnostic work-up, patients have potential for acquiring new treatment strategies. The need for increased awareness of POTS symptomatology and treatment among rehabilitation therapists is less commonly discussed by researchers but is worth addressing due to the potential benefit for this patient population.
Clinical implications
Postural tachycardia syndrome is a condition responsible for substantial functional limitations in the majority of patients. Occupational and physical therapists commonly treat patients with conditions that exist co-morbidly with POTS, such as concussion, hypermobility, and chronic pain. The symptomatic presentation of POTS is not unlike a variety of other disorders seen in clinical practice. Therapists frequently treat patients with various vestibular, pain, fatigue, gastrointestinal, and orthostatic symptoms. The knowledge base and intervention options to treat these individuals, while unique in POTS, shares several similarities and serves as a basis for continued learning.
Physical reconditioning and engagement in daily life activities are primary foci of treatment in individuals with POTS. To date, there is no evidence that the severity of autonomic dysfunction as measured on autonomic testing in an individual with POTS correlates with disability. Exercise is regarded as an essential, cost-effective treatment component with minimal, if any, side effects when performed appropriately. Despite exercise intolerance with acute adverse side effects in the immediate, patients frequently can increase tolerance and see long-term benefits for a variety of symptoms. However, exercise must be prescribed in a graded, individualized manner, recognizing signs of fatigue, dyspnea on exertion, and joint hypermobility. This study demonstrates that physical therapy and, to a larger degree, occupational therapy are underutilized in treatment of patients with POTS.
The present study demonstrates the vast array of challenges individuals with POTS experience as a result of their condition(s). Occupational therapists are uniquely qualified to address the broader picture, combining physical, psychological, and social factors to treat the whole person and offer a comprehensive approach to treatment. Physical therapists are highly skilled in individualizing exercises to limit fear of movement and maximize outcomes for a patient, taking into consideration their unique health needs. Therapists may choose to utilize interventions including energy conservation, sleep hygiene, nutrient balance, cognitive rehabilitation, engagement in social and leisure activities, work and school accommodations, cognitive-behavioral interventions, and lifestyle modifications to name a few. Notably, the training of occupational and physical therapists involves preparation to treat a variety of medical conditions. These occupational and physical therapists can make modifications to ensure safety, taking into account co-morbid conditions such as joint hypermobility, chronic pain conditions, and gastrointestinal complications. Further research is necessary to identify occupational and physical therapists’ role in the treatment process to improve patients’ participation and independence.
Limitations
While valuable and offering new information, the current findings require additional validation with at least five limitations. First, due to the nature of a social media–based electronic survey using a convenience sample, the study responses may not be representative of the greater community with POTS and those who do not utilize social media. We are optimistic that the large sample size does help to account for this. The study reflects a greater percentage of women than what is generally documented in existing literature. Second, despite best efforts to screen participants, since the participants were responsible for honesty in representing themselves, there is always risk that a parent or loved one provided the data, in which case the data would be representative of how those around the patient see their experience of POTS. It is also possible the individual did not receive an actual diagnosis by a physician using specific POTS criteria. Third, we did not collect information regarding particular roles and therefore could not analyze the domains of child-rearing, religious/spiritual activities, and school separately. Thus, the frequency of impact is unclear among the population in which these domains are applicable. Fourth, there are limits in the types of data collected, and elements of quality of life, for example, were not included to limit participant burden. Fifth, survey advertisements emphasized therapy services, so individuals may have chosen to take the survey based on this information, which may have biased the sample as well. However, we gave no compensation for participating in this study, which otherwise could have unintentionally biased the sample toward those individuals looking for additional financial support.
Conclusion
Overall, participants reported high levels of functional impairment and impact in various domains, most frequently including home management, bathing or showering, shopping, social participation, and meal preparation and cleanup. Patients reported trials of multiple treatment strategies, such as increased salt and fluid intake, medications, exercise, and compression garments. Even so, there were high incidences of falls, cognitive impairment, and the use of non-pharmacologic compensatory devices. Despite the above-stated challenges, results show low utilization of therapy services. Additional research will help determine if and how therapy services might play a role in individuals’ functional status with POTS. In light of the need for treatment interventions, research and clinical trials are essential to determine best practices for rehabilitative therapy treatments.
Key findings
Individuals reported an average of 11 daily life activities impacted by POTS with high levels of self-perceived disability. Cognitive impairment was reported in 93.4% weekly and falls occurred in 55.3% of participants annually. Despite frequent falls and functional impairment, participants infrequently (26.9%) utilized therapy services.
What the study has added
Evidence of functional impairment and falls in the absence of therapy services in most adults with POTS, despite using a wealth of strategies, showcases the need for novel treatment approaches by trained professionals.
Footnotes
Acknowledgments
We would like to thank Dysautonomia International for their support in reviewing the survey materials and distributing them to their patient community.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Research ethics
This study received exception through the Institutional Review Board at the Texas Woman’s University, protocol #20473 in 2019.