
Abstract
Keywords
Introduction
Mental disorders encompass a wide array of psychiatric conditions that impair cognitive, emotional, and behavioral skills (Spitzer et al., 2018). Worldwide, more than 450 million people suffer from mental disorders (World Health Organization, 2019). The impact of mental disorders extends to influence the individual’s occupational capacity to carry out daily occupations, which are necessary for maintaining health and well-being (Bowie et al., 2010). Moreover, individuals with mental disorders experience limitations in performing daily life occupations, such as self-care, work, and leisure (Edlund et al., 2018).
Occupational performance of daily occupations includes various areas of occupation such as basic activities of daily living (ADLs), more complex instrumental activities of daily living (IADLs), education, work, social interaction, and leisure (Amini et al., 2014). Furthermore, healthcare professionals (e.g., psychiatrists and occupational therapists) have always been keen to evaluate health-related outcomes, including disease symptoms, occupational performance, and quality of life among individuals with mental disorders (Revicki et al., 2014). These outcomes assist occupational therapists in designing appropriate interventions to meet the needs of their clients. Unfortunately, there is limited evidence on how individuals with mental disorders perform daily life occupations, and what occupations they perceive as challenging.
Several old studies (Ivarsson et al., 2004; Boyer et al., 2000; Lang et al., 1999; Honkonen, 1995) investigated occupational performance challenges in occupational areas among individuals with mental disorders. Birken et al. (2018) studied the development of an occupational therapy intervention for adults with mental disorders following their discharge from the hospital in the United Kingdom. They found that individuals with mental disorders complained of occupational performance challenges, such as, meal preparation and leisure participation post-discharge. A study by Brown (2011), which utilized a qualitative design, was conducted in Canada to describe the early effects of mental disorders on the occupational performance. Accordingly, the mental disorders’ condition first affected the participants’ ability in performing self-care and hygiene. At a later phase, it was found that social interaction, work, and educational performance were less affected (Brown, 2011).
Other studies have investigated the factors that affect the occupational performance in individuals with mental disorders (Kuszni et al., 2000; Depp et al., 2012; Carpintero and Santamaria-Vazquez, 2017; Habtamu et al., 2018). In rural Ethiopia, a study by Habtamu et al. (2018) investigated the factors associated with occupational performance challenges. They concluded several factors that have contributed to the improvements of occupational performance, such as focusing on the residual symptoms, poverty, medication side effects, and stigma. Whereas, increasing age, being unmarried, living in rural regions, continuous course of psychosis, and higher symptom severity were all associated with occupational performance impairment (Habtamu et al., 2018). Furthermore, Carpintero and Santamaria-Vazquez (2017) studied the relationship between volition (motivation) and the occupational performance. Findings showed that high levels of volition and regular participation in occupational therapy rehabilitation programs were associated with the improvement of occupational performance in both daily occupations and community participation. However, lengthy institutionalization reduced this volition. Another study by Depp et al. (2012) investigated the influence of cognitive impairment and affective symptoms on employment and residential independence. They reported that both the neurocognitive ability and affective symptoms were strong predictors of employment and residential occupational performance (Depp et al., 2012).
Along with mental health, satisfaction also has an important aspect of concern in rehabilitation intervention (Chaudhury et al., 2018). Thus, raising awareness about applying the interdisciplinary model in mental health sectors will make satisfaction one of the most commonly desired outcomes in individuals with mental disorders (Gellert, 1993; Chaudhury et al., 2018). Satisfaction is the cognitive judgment of one’s whole life (Diener, 1995; Strine et al., 2008). It reflects the performance-related quality of life (Meule and Voderholzer, 2020) and contributes to health and well-being (Allen and Anderson, 2018).
According to the Canadian Model of Occupational Performance (CMOP), satisfaction about performance of daily life activities complements occupational performance (Townsend, 1997; Kavanagh, 2006). Moreover, satisfaction about occupational performance was studied in numerous populations, such as stroke (Jaber et al., 2018), cancer (Dehghan et al., 2020), and older adults (Tuntland et al., 2016). However, evidence about satisfaction in mental disorders is scarce and did not focus on satisfaction related to performance in specific daily life activities, like self-care or work. For example, a study by Siu et al. (2015) examined the factors that affected subjective satisfaction in individuals with schizophrenia, and found that the satisfaction in this population might have measured their treatment outcomes. Similarly, Lombardo et al. (2018) reported that individuals with mental disorders had lower life satisfaction. Both studies (Siu et al., 2015; Lombardo et al., 2018) did not show what activities were related to lower satisfaction. In a systematic review, it was reported that using objective measures of satisfaction with individuals with mental disorders was more common than using subjective measures (Nevarez-Flores et al., 2019). However, our study assessed the satisfaction of individuals with mental disorders on each occupational performance challenge.
As discussed above, the evidence about occupational performance in individuals with mental disorders is limited in the number of new studies (i.e., only old related studies by Lang et al., 1999; Boyer et al., 2000; Ivarsson et al., 2004), methods used in terms of sample size (e.g., Boyer et al., 2000, Bejerholm and Eklund, 2004; Brown, 2011; Carpintero and Santamaria- Vazquez, 2017), and assessment tools that did not capture a wide variety of daily life activities (Brown, 2011; Birken et al., 2018).Also, to the best of the author’s knowledge, there have been no previous studies regarding this topic in the Middle East. Given the significant role of context in shaping everyday life activities (Kuszni et al., 2000; Depp et al., 2012; Carpintero and Santamaria-Vazquez, 2017; Habtamu et al., 2018), cultural differences between the Western and Arabian countries may affect both the occupational performance (Townsend, 1997; Kavanagh, 2006) and satisfaction level (Phipps and Richardson, 2007). Additionally, studying occupational performance and satisfaction in individuals with mental disorders in Jordan is a basic step before performing further interventional studies in the future. This is justified by the increasing demand for mental health services, including occupational therapy due to the Syrian and Iraqi crises as reported by WHO (World Health Organization, 2019).
Existing evidence regarding occupational performance and satisfaction in mental disorders did not explore all areas of occupation (De Graaf et al., 2012) or specific mental disorders (Edlund et al., 2018), and is limited in both the number of studies and the methodology used (Druss et al., 2009). Also, there are no studies regarding the occupational performance of mental disorders in the Arab world. Therefore, this study aimed to (1) explore the occupational performance and satisfaction in individuals with mental disorders; (2) explore the specific challenging daily life activities in all areas of occupations; and (3) investigate the relationships between occupational performance and satisfaction, and demographic and condition-related characteristics in individuals with mental disorders.
Research questions
This study aimed to answer the following research questions: 1. What are the occupational performance challenges among individuals with mental disorders? 2. How are demographic characteristics related to occupational performance in individuals with mental disorders? 3. What are the demographic characteristics that can predict the occupational performance of individuals with mental disorders?
Method
Design
A cross-sectional, descriptive, correlational design was used to explore the occupational performance of individuals with mental disorders, and the demographic and health-related characteristics that are associated with occupational performance.
Setting
The study took place in different mental health clinics and major public psychiatric hospitals in Jordan. Also, the occupational therapy clinics located in two Jordanian university hospitals were asked about their clients.
Participants
The current study used a convenient sample of in- and out-patients in the Jordanian psychiatric hospitals and clinics. Ninety-five participants with a confirmed diagnosis of mental disorders were recruited. Most of the sample was from Al-Fuhais hospital (79, 83.2%), whereas other hospitals provided only a few individuals with mental disorders (5, 5.2%).
The inclusion criteria of the individuals with a confirmed mental disorder (e.g., schizophrenia, bipolar disorder, depression, personality disorders, and anxiety disorders) were 18 years of age or older at the time of assessment, had a score of ≥ 19 on the Montreal Cognitive Assessment (MoCA) which represented normal to mild cognitive impairment (Nasreddine et al., 2005), and able to understand (spoken or written) Arabic or English languages.
The study excluded individuals with mental disorders who were not capable of participating in the study interview, and had a score of < 19 points in MoCA, which indicated moderate to severe cognitive impairment. (Nasreddine et al., 2005)
Instruments
The Canadian Occupational Performance Measure
The COPM is a client-centered assessment tool (Law et al., 1994) that was derived from the COPM principles (Warren, 2002). It is used to enable a patient to identify his or her priorities and restrictions in everyday life and to assess the occupational performance in all areas of life, including self-care, leisure, and productivity (Law et al., 1996). A systematic review of the literature by Parker and Sykes (2006) found that the COPM interview has enabled patients to name and frame their challenges, empowered them to be more critical of their performance, and allowed them to become experts on their circumstances.
Generally, the COPM has many advantages. According to a study conducted by Dedding et al. (2004), results showed that the COPM provided information that could not be obtained using current standard health measurement tools. Moreover, it is known to provide an individualized perspective of the patient’s preferences, values, and judgments regarding their occupational performance, which facilitates the ability for clinical decision-making. Additionally, it monitors functional progress (Carswell et al., 2004) and communication within a multidisciplinary team (Fedden et al., 1999). The systematic review by Parker and Sykes (2006) found that the COPM interview has enabled patients to name and frame their challenges, empowered them to be more critical of their performance, and allowed them to be experts regarding their circumstances.
However, the COPM is only applicable to patients with good cognition (Carswell et al., 2004) because most of the individuals with mental disorders complain of cognitive deficits (Pan et al., 2003). This current study focused on individuals with normal to mild cognitive impairment and has two subscales: occupational performance and satisfaction. Occupational performance is scored on a numeric scale from 1 to 10: a score of “1” indicates that the individual is not able to do it at all, whereas “10” indicates that the individual is able to do it all. Likewise, satisfaction scores are also ranged on a numeric scale from 1 to 10: a score of “1” being not satisfied at all with the way the individual with mental disorders does it, and “10” for being extremely satisfied.
Several researchers have examined the reliability and validity of COPM in different country contexts. For example, Pan et al. (2003) examined the test–retest reliability of COPM with 141 individuals with mental disorders within 2–4 weeks between the two assessment sessions. The correlation coefficient of the test–retest scores ranged from r = .842 in performance scores and r = .847 in satisfaction with performance. Thus, reflected the fact that the test–retest reliability was good in COPM with individuals with mental disorders. In addition, face validity was found good in assessing occupational performance (Law et al., 1998). Concerning convergent validity, Dedding et al. (2004) found 63% of matched occupational performance deficits among 97 individuals with different diagnoses. Also, 74% of occupational performance deficits matched with the items in the Disability and Impact Profile, as well as, 49% with the Sickness Impact Profile. Furthermore, among 152 individuals with different diagnoses, construct validity had a positive significant correlation between COPM scores and three self-reported questionnaires (Sickness Impact Profile, Disability and Impact Profile, and Impact on Participation and Autonomy) (Eyssen et al., 2011).
In the current study, individuals with mental disorders completed a four-step semi-structured interview with the researcher. First, the individuals identified occupational performance issues into three main occupational areas; self-care, productivity, and leisure. Second, they rated the importance of the identified occupational performance issues from 1 to 10; the higher the rating score, the more important the occupational performance issues were to the individual. Furthermore, the researcher showed a Likert-type visual scale in each rating step. Third, the individual determined the top five occupations from the whole three areas. However, if there were more than one that had the same high rate, then the individual would choose the ones that he or she wanted to focus on during the treatment. After determining the top five occupations, the individual rated the occupational performance and satisfaction from his or her perspective for each one of the five occupations. The rating was from 1 to 10 for each occupation; the higher the rating, the better. Fourth, the researcher calculated the COPM mean score for both the performance subscore and the satisfaction subscore separately, which was done by taking the average of the five occupational scores in the occupational performance and satisfaction.
The Montreal Cognitive Assessment (MoCA)
MoCA is a brief cognitive 30-point screening test designed to detect mild cognitive impairments, which can be administered within 10 min (Nasreddine et al., 2005), and assess several cognitive functions (Maust et al., 2012). It is available in Arabic and English (Rahman and El-Gaafary, 2009), so if the patient could read and speak in English, he was free to use the language of his choice.
MoCA test–retest reliability was high and had a correlation coefficient of 0.92 in both Arabic (Rahman and El-Gaafary, 2009) and English versions (Nassredine et al., 2005). Additionally, it had a good high degree of internal consistency in both Arabic (Rahman and El-Gaafary, 2009) and English versions as well (Nasreddine et al., 2005), and the Cronbach’s alpha of the standardized items was 0.83. Also, content validity between MoCA and the Mini Mental Status Examination scores close correlation was established (Nassredine et al., 2005).
The aim of screening cognitive skills in this study was to include individuals with either normal or mild cognitive impairment and exclude moderate to severe impairments. This can be justified by the fact that COPM, in this study, needs self-awareness and consciousness to be applied. Thus, checking up the basic cognitive skills is necessary.
Demographic and health-related questionnaire
This questionnaire collected demographic information from the participant’s information that focused on age, gender, educational level, work status, marital status, and monthly income. The health-related information contains the diagnosis and insight, which were extracted from the medical file of individual’s with mental disorder profile. Health-related information about the patient’s insight was documented by the psychiatrist working in the instructions where recruitment took place.
Procedure
Recruitment occurred between January 2020 and July 2020. A total of 95 individuals with mental disorders were enrolled to participate in this current study. The initial interview was conducted with clients who were attending a public psychiatric hospital or psychiatric clinic to receive mental health care or rehabilitation services. If the clients agreed to participate and were able to respond to the interview, then their file was read. Afterward, the patient’s medical file was read by the researcher either in the nursing room of the in-patient department or in the archive room in the out-patient department. The aim of reading the file was to check on the demographical information, diagnosis, members of the health care team providers, medical referral method, medications with their doses, other health conditions, and the signs and symptoms that were experienced in their last visit.
Next, the researcher assessed the cognitive performance by using a screening test MoCA. The patients, who have met the inclusion criteria, received an information letter regarding the research project, and were explicitly informed that they could withdraw from the study whenever they wanted to. Whoever was interested in participating in the study then, signed the informed consent form to complete the rest of the study measures.
Each participant took from 60 to 90 min, in total, to complete all measures, including the initial interview which was done in a quiet room. The researcher made sure that the participant was not hungry, did not complain from drowsiness or dizziness, and felt safe. If family or any companion accompanied the participant, then the researcher would ask the participant for permission to let them attend the assessment. Moreover, if the researcher noticed that the patient’s companion had caused distraction or tried to help the patient in answering the questions, then would ask him or her to keep silent or sit away.
If any data was missing, it was collected within 1 week, either in person or by telephoning the participant.
Data analyses
Statistical analysis was performed using the SPSS software version 20.0 to analyze the data. Descriptive statistics were calculated by mean ± SD which was used for continuous variables, and by frequencies and percentage which were used for categorical variables.
Descriptive statistics were used to investigate the frequencies of the reported occupations and the mean ± SD was also used to explore the occupational performance of individuals with mental disorders. Additionally, the Spearman rank-order correlation was also used to investigate the relationship between the occupational performance score and demographic characteristics, such as age, gender, marital status, working status, monthly income, and level of education. Moreover, the Spearman rank-order correlation was used to investigate the relationship between occupational performance score and health-related characteristics, such as diagnosis and insight. A simple linear regression was applied for working status with occupational performance score to predict the occupational performance.
Ethical consideration
Individuals with mental disorders were enrolled for this study after receiving the Institutional Review Board (IRB) approval from the Jordan University of Science and Technology. For protection purposes against harm and risk of the individual’s rights, the researchers considered the participants privacy, confidentiality, and his or her right to decide to participate in this study. All participants were assured that they could withdraw from the study whenever they wanted without explaining the reasons. They were also assured that withdrawal would not affect their care routines.
Results
One hundred and forty individuals with mental disorders were approached. Out of those individuals, 20 refused to participate in the study and 25 were excluded because they did not meet the inclusion criteria. In the end, a total of 95 individuals with mental disorders agreed to participate and provided a consent form. Moreover, the response rate was of 85.7%.
Demographic and health-related statistics
Description of occupational performance and satisfaction with demographic characteristics (n = 95).

SD; standard deviation; JOD: Jordan dinar.
Description of the occupational performance
In COPM, 95 individuals rated their performance and satisfaction with the top five concerned occupations in a numeric score out of 10. The total score mean ± SD of the occupational performance was (5.8 ± 1.7), while the mean ± SD of the satisfaction was (5.6 ± 2.0) (see Table 1). Individuals with bipolar disorder showed the highest mean scores of occupational performance and satisfaction, (6.48 ± 1.91), (6.49 ± 1.92), respectively. The lowest mean scores of occupational performance and satisfaction were found in individuals with depression (4.25 ± 1.42), (4.10 ± 1.69), respectively (see Table 1).
According to the occupational therapy practice framework classification of occupational areas, IADLs was the most reported area (165, 35%) throughout the whole occupational areas of the top five concerned occupations. Moreover, ADLs (109, 23%), social interaction (89, 18.2%), and work (48, 10.1%) were revealed to be the most frequently reported areas. Particularly, family social interaction (45, 9.5%) and financial management (41, 8.7%) had been the most frequent subareas of the occupational areas reported through the whole reported functions. Furthermore, personal hygiene and grooming (38, 8%), bathing and showering (37, 7.8%), home management (36, 7.6%), and job performance (33, 7%) were also frequently reported (see Figure 1). Occupational areas throughout the whole reported occupations.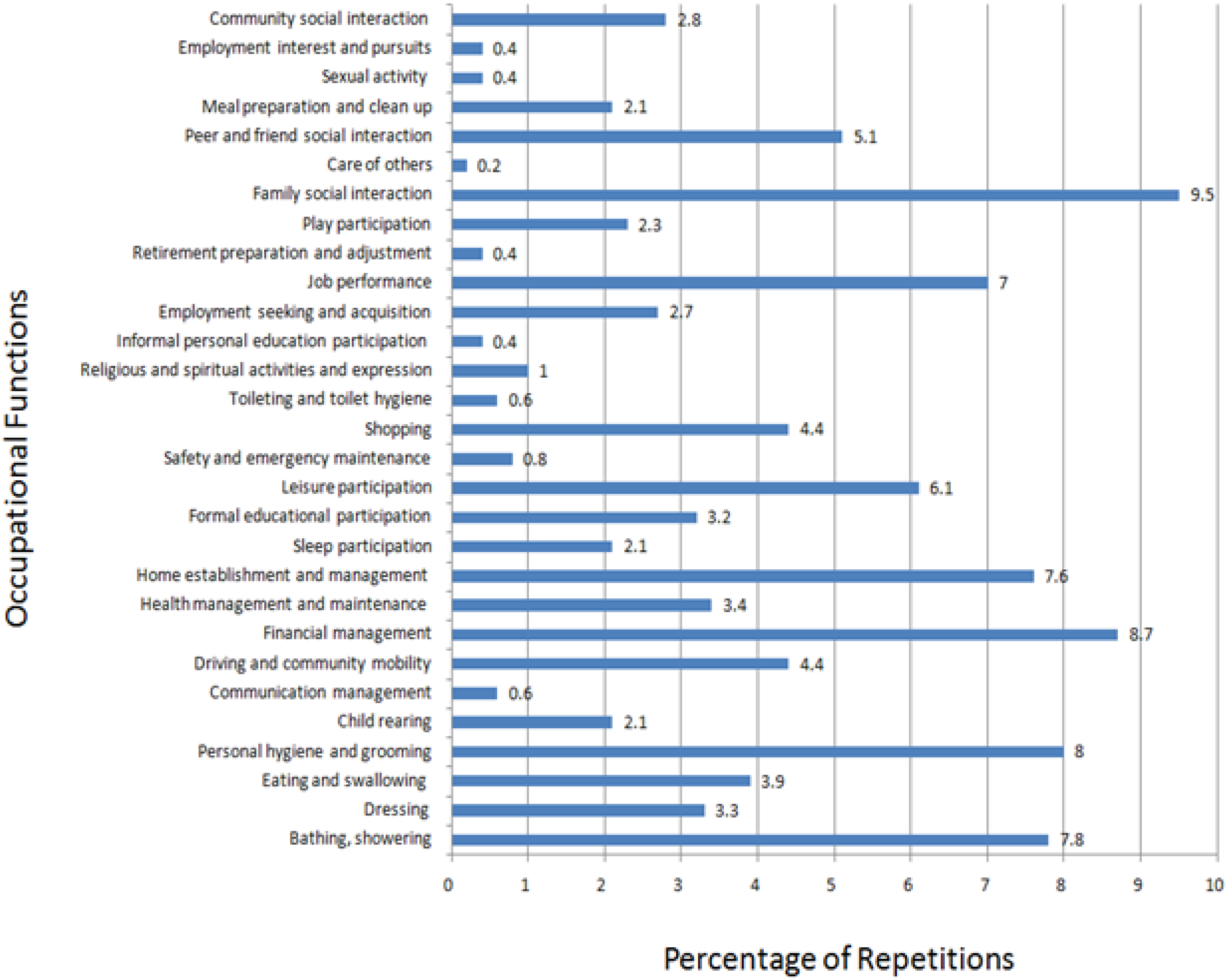
Interestingly, the ADLs area was more reported among individuals with schizophrenia than other diagnoses. While individuals with bipolar reported rest and sleep more frequently than the other diagnosis groups, depression reported the work area. Moreover, individuals with anxiety and personality disorders frequently reported the social participation area more than the other groups (see Figure 2 that clarifies the occupational performance areas among different diagnoses). Distribution of the reported occupations among different diagnoses. ADLs, activities of daily living; IADLs, instrumental activities of daily living. This figure clarifies the repetitions of reporting the occupational areas between the diagnoses groups.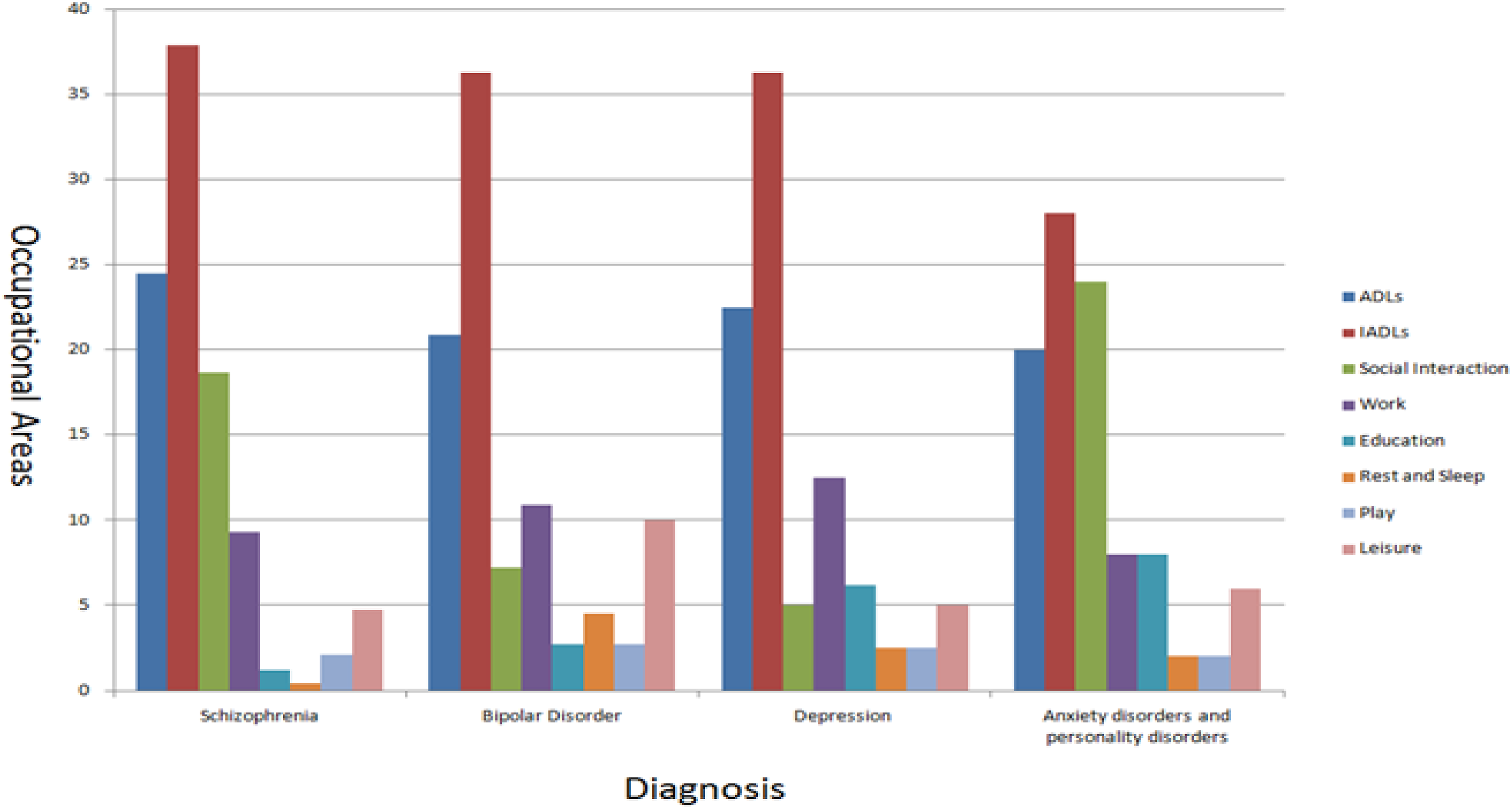
Furthermore, participants above the age of 30 reported higher occupational performance and satisfaction ratings compared to other groups. In addition, it was also found that higher education levels showed lower occupational performance and satisfaction rates compared to lower educational groups. Finally, individuals with full insight rated themselves with lower occupational performance and satisfaction rates compared to other groups of insight (see Table 1).
Correlations
Spearman rank-order correlations showed significant relationships between occupational performance with diagnosis and working status (r = −0.219), (r = 0.243), respectively, p < 0.05. In addition, Spearman rank-order correlations had very weak relationships between occupational performance and gender, insight status, marital status, monthly income, and level of education because the correlation values were (r = −0.008), (r = 0.194), (r = 0.159), (r = −0.110), and (r = −0.177), respectively. Also, the relationships were insignificant at 95% confidence interval because the p-values were lower than 0.05 (p = 0.935), (p = 0.060), (p = 0.125), (p = 0.288), and (p = 0.086), respectively.
A simple linear regression was calculated to predict the occupational performance based on working status. We calculated value of (f) for the model (6.137), which was a statistically significant value at (α ≤ 0.05), and the value of (R2 = 0.062). This means that the demographic and health-related characteristics of the form explained the percentage value of (6.2%) variance in performance score of the COPM. In addition, there was a significant effect of work status on the performance score since (beta = 0.249, t = 2.477, and Sig = 0.015). Therefore, the work status affected the occupational performance at α ≤ 0.05.
Discussion
To the best of our knowledge, this is the first study in the Arab world and Middle Eastern area to investigate the occupational performance among individuals with mental disorders. It explored the relationship between different client factors with occupational performance and satisfaction of individuals with mental disorders.
Furthermore, this study found that individuals with mental disorders complained of occupational performance and satisfaction in different occupational areas. These results were consistent with most other international studies (Haglund et al., 1998; Girard et al., 1999; Bejerholm and Eklund, 2004; Keyes, 2005; Birken et al., 2018; Edlund et al., 2018).
The total mean ± SD of performance was (5.8 ± 1.7), and the mean was around the median of the range of 1–10 points in the COPM score. Notably, study participants tended to answer with scores at the extreme ends of the point scale. This explanation is congruent with a study by Ivarsson et al. (2004), which emphasized that when using scales for individuals with mental disorders, results may be limited to the extreme categories of the scale.
While individuals with bipolar disorder showed the highest scores, individuals with depression had the lowest. Particularly, the occupational performance of individuals with depression was lower than individuals with bipolar disorder and individuals with schizophrenia. This result aligns with what Girard et al. (1999) found, which was that the least occupational performance was within individuals with schizophrenia. Also, they reported that individuals with depression had better occupational performance than schizophrenia. This disagreement can be manifested from their reported limitations that they only focused on ADLs and had a wide age range. Occupations would be different, as would the association of abilities with age. Moreover, they focused on the occupational therapists’ perspectives, rather than the individuals’ self-perception.
The most challenged occupational area among the occupational performance individuals with mental disorders was IADLs. Social interaction and work occupations were also frequently reported by individuals with mental disorders. However, the work occupation was reported by many individuals with depression, whereas individuals with bipolar disorder frequently reported rest and sleep, and leisure occupations.
Moreover, individuals with schizophrenia frequently complained of social interaction challenges. Ivarsson et al. (2004) explored the self-perceived occupational performance among 51 individuals with severe mental disorders in Sweden. They reported that play and leisure were the most impaired occupations in individuals with mental disorders perspectives. This result can be explained that the mean ± SD age of their study’s participants was (46.76 ± 11.83), an age group in which people care more about play and leisure. Also, they found that 50% of the participants required assistance while performing occupations that needed planning and organization, which is congruent with the findings of this current study. Occupational Therapy Practice Framework defines IADLs as the occupations that support daily life and require more complex interactions than ADLs (Amini et al., 2014). Moreover, Honkonen (1995) found that 75% of individuals with schizophrenia faced no challenges in performing ADLs, while 27% of them have faced challenges in ADLs due to hospitalization or dependence on another person. Along a similar line, Lang et al. (1999) reported that individuals with mental disorders reported fewer ADL challenges. Individuals with anxiety disorders or personality disorders frequently complained in the educational area. This difference in result may be because individuals in this group of the current study were in the learning stage.
In particular, most individuals with mental disorders suffer from family social interaction and financial management performance challenges. Also, personal hygiene and grooming, bathing and showering, home management, and job performance were the most frequently reported occupational performance and satisfaction challenges by the individuals with mental disorders. It was concluded by Birken et al. (2018) that individuals with mental disorders complained about home management and leisure participation, which were the most affected functions post-discharge from the hospital. Also, Keyes (2005) reported that individuals with mental disorders complained from challenges in ADLs, job performance (more missed working days compared with healthy individuals), and psycho-socially. Moreover, Ivarsson et al. (2004) emphasized that full-insight men who lived alone cared more about work. According to CMOP occupational classification, most individuals with mental disorders complained from occupational performance challenges in self-care, which is consistent with Brown (2011).
Individuals with schizophrenia complained from problems in ADLs. In conclusion, negative symptoms and cognitive dysfunction seen in schizophrenia may lead to challenges in ADLs (Hsu et al., 2017; Samuel et al., 2018).
Moreover, individuals with depression complained from work challenges, which is consistent with Depp et al. (2012) and Nigatu et al. (2015). Next, individuals with depression complained from lack of interest and motivation (Regier et al., 2013), in working status, absence, and at-work performance (Lemer and Henke, 2008). Meanwhile, individuals with bipolar disorders complained of sleep challenges, which is consistent with Zangani et al. (2020). This can be explained because they complain of hyperactivity and decreased need for sleep (Regier et al., 2013).
Furthermore, individuals with anxiety and personality disorders had challenges in social interaction. Since most of the individuals with anxiety and personality disorders mainly had social phobia, obsessive-compulsive anxiety disorders, borderline personality disorders, and antisocial personality disorders, they complained from social participation challenges.
Highly educated participants rated their perceived occupational performance and satisfaction with performance lower than participants with less education. Gordon and Arvey (1975) reported that highly educated workers had less satisfaction about their work compared to individuals with less educational levels. In addition, individuals with mental disorders complained from the constant changes in their employment due to relapses. Work changes were strongly correlated with low self-esteem and satisfaction (Khare et al., 2011). On the other hand, Ghubach et al. (2010) has reported that the higher the educational level, the better the satisfaction. This inconsistency could be explained that our study sample included inpatients which affected their perceived satisfaction.
Additionally, individuals with high internalized insight were more aware of their own limitations and strengths, and therefore, they rated themselves as having lower perceived performance and satisfaction. Gaziel et al. (2015) reported that there was a strong negative relationship between insight and self-stigma which, in their order, affected the satisfaction of life activities.
There was a correlation between occupational performance with diagnosis, meaning that individuals with different diagnosis have different occupational performances. All individuals with mental disorders emphasized that they have faced challenges in the occupational performance of IADLs, although they differ in other occupational reportings. For illustration, individuals with schizophrenia tended to report challenges in ADLs, while individuals with depression tended to report challenges in the work area. Additionally, individuals with bipolar disorder tended to face challenges in performing leisure occupations, while individuals with anxiety and personality disorders faced problems in social interaction occupations. The correlation between occupational performance and diagnosis was reported by several researchers from different countries (Haglund et al., 1998; Girard et al., 1999; Depp et al., 2012; Edlund et al., 2018).
On the other hand, there was a correlation between occupational performance and work status. This means that individuals with mental disorders, who were working at the time of assessment, had a better higher occupational performance. This result is consistent with international studies (Keyes, 2005; Blank et al., 2008; Brown, 2011; Cornelius et al., 2011; Henderson et al., 2011; Depp et al., 2012; Knudsen et al., 2012; Modini et al., 2016). It was emphasized in a systematic review by Cornelius et al. (2011) that working status was one of the most frequent factors that caused permanent disability for individuals with mental disorders. In addition, Henderson et al. (2011) reported that there was a relationship between work area and mental disorders. However, they reported that there were several factors that affected their decision in seeking a sick leave or being absent from work, and suggested that individual’s perceptions, beliefs, and other psycho-social influences contributed in their work performance challenges (Henderson et al., 2011). Moreover, Knudsen et al. (2012) concluded that long periods of absence or recurrence of sickness leaves were common in individuals with mental disorders.
Conclusions
It was concluded that individuals with mental disorders had low occupational performance and satisfaction total scores, and the most reported occupational area was IADLs. Additionally, there was a relationship between work status and occupational performance and satisfaction, and also between the diagnosis and occupational performance. Moreover, work status could be a predictor of the occupational performance. Since our study did not compare occupational performance and satisfaction between individuals with and without mental disorders, the conclusion should be considered with caution. Future research should include a control group of individuals without mental disorders.
Limitations
There are several possible limitations in this study. First, cross-sectional studies are unable to give causation and direction of the relationships. Second, the recruitment method of individuals with mental disorders was focused on inpatients, due to the lack of other occupational therapy centers in the psychiatric field. Also, the hospital environment already affects the occupational performance and satisfaction within individuals. More so, assessing occupational performance in the hospital may affect the results.
Last, the side effects of medication on occupational performance were not considered. Most of the participants were inpatients and in the modification treatment stage. Modification treatment means that the psychiatrists were modifying the treatment from one medical line to another to reach the best response. But this process may lead to occupational performance instability, as it may have affected our results.
Recommendations
This study should be considered a beginning in rehabilitation research among individuals with mental disorders in Jordan. Assessing the individuals with mental disorders in their real environments and contexts could change the results dramatically. Moreover, including families, friends, and employers would contribute to giving a more complete picture of their occupational performance.
Qualitative studies are essential to give a deeper understanding of occupational performance and satisfaction among individuals with mental disorders. In this instance, this study has highlighted the need of occupational performance among individuals with mental disorders in Jordan, which may open new pathways for future studies using randomized controlled trials.
Moreover, determining the occupational performance of the individuals with mental disorders could guide interdisciplinary teamwork either in research or practical work. Nevertheless, recruiting a larger sample size would contribute to describing the relationship between demographical characteristics and occupational performance. In addition, recruiting a larger sample size would allow the differences between small disorder groups like anxiety disorders and personality disorders to be more profound.
Key findings
• Individuals with mental disorders had reported low occupational performance and satisfaction in their life by using COPM. • IADLs occupation is the most frequent occupational area that individuals with mental disorders had reported in their occupational performance problem list. • There is a relationship between occupational performance and satisfaction with working status. • There is a relationship between occupational performance and diagnosis. • Working status may be a predictor of occupational performance.
What this study has added
This is the first study in the Arab and Middle Eastern areas to investigate the occupational performance and satisfaction of individuals with mental disorders by using the COPM. Foremost, it is a fundamental study for higher-level studies such as randomized control trial designs.
Footnotes
Acknowledgments
This project was a result of multidisciplinary teamwork efforts. From two different Jordanian universities; The Jordanian University of Science and Technology and The Hashemite University, occupational therapists and nurses were working together.
Author Contributions
Hanan I. Madi, Noor T. Ismael, Shaher H. Hamaideh, and Ala’a F. Jaber were involved in the concept and design of the study, in the acquisition of the data, in drafting the manuscript, and analyzing the data.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by the Jordanian University of Science and Technology, Irbid, Jordan (grant number: 20200074).
Research ethics
Institutional Review Board (IRB) approval from the Jordan University of Science and Technology were gotten for this study (44/128/2019).
Consent
Participants gave written consent. All participants were assured that they could withdraw from the study whenever they wanted and did not need to explain the reasons. They were also assured that withdrawal would not affect their care routines.
Patient and Public Involvement
During the development, progress, and reporting of the submitted research, Patient and Public Involvement in the research was included at all stages of the research.