
Abstract
Introduction
Self-management post-stroke is essential where healthcare systems are stretched and stroke prevalence remains high. Self-management is recommended in stroke guidelines however, the quality of guidelines can vary and the evidence underpinning recommendations is unclear. The objectives of this paper are to identify and appraise current stroke guidelines, synthesise self-management recommendations and assess the evidentiary basis of these recommendations.
Method
Stroke guidelines were retrieved from a search of four databases and stroke association websites in July 2021. Four independent reviewers assessed their quality using the Appraisal of Guidelines Research and Evaluation 2nd Edition instrument. Self-management recommendations were extracted by hand, evaluated, synthesised and the evidence underpinning them appraised using the Canadian Stroke Best Practice Recommendations framework.
Results
Eleven guidelines were included in this systematic review, all of excellent methodological quality overall. One hundred and sixty-one recommendations were extracted from these guidelines and grouped into ten principles of self-management. A quarter of the recommendations were underpinned by level A evidence, 32% level B and 43% level C.
Conclusion
Although current stroke guidelines are of high methodological quality, there are considerable inconsistencies in self-management recommendations within and between these guidelines, with varying strengths of underpinning evidence. This article identifies a need for universal consensus regarding evidence-based self-management post-stroke.
Introduction and literature review
Stroke
Stroke is a leading cause of morbidity and mortality globally, with approximately half of people with stroke (PwS) left with residual impairments such as reduced mobility, fatigue and depression (Boncoraglia et al., 2019). Such impairments diminish an individual’s quality of life, increase carer burden and challenge healthcare systems (McHutchison et al., 2019). Despite a 42% decrease in stroke incidence in high income countries in recent years, stroke prevalence is projected to increase to 77 million people globally by the year 2030, due to decreasing stroke mortality rates and an ever-ageing population (Boncoraglia et al., 2019). Consequently, the impact of stroke on healthcare services will continue to grow, increasing demand for innovative, yet person-centred approaches in stroke care.
Self-management post-stroke
It is argued that self-management programmes could help address the long-term consequences of stroke and support stretched healthcare systems (Jones et al., 2016; Sadler et al., 2017). Self-management is defined by Lennon et al. (2013: 868) as ‘an individual’s ability to manage the symptoms, treatment, physical and psychosocial consequences and lifestyle changes inherent with living with a chronic disease’. Jones et al. (2016) suggests that self-efficacy is the main underlying concept of self-management, with shared decision-making and knowledge highlighted as key principles. However, there is inconsistency in the definition of self-management internationally and between disciplines (Sadler et al., 2017). Therefore, for the purpose of this review, self-management is understood as ‘an intervention which empowers the patient to manage their own condition and/or rehabilitation programme with the guidance of a healthcare professional, in order to live their life as independently as possible’. Some research has been conducted into how occupational therapy based self-management programmes can offer value for PwS (Atler et al., 2017), with qualitative evidence indicating that PwS understand the potential self-management programmes offer them to maintain or improve their quality of life. However, evidence for self-management and occupational therapy appears to be developing more rapidly for people with other chronic conditions than for PwS (Garvey et al., 2015). The aim of occupational therapy throughout stroke care pathways is to optimise people’s function and independence after a stroke through physical and cognitive rehabilitation and explore compensatory strategies, such as the provision of assistive technologies and home modifications, to promote self-management. Given occupational therapists play such a pivotal role in self-management throughout stroke care pathways, it is important to identify the key principles of self-management that occupational therapists can consider when designing their intervention and align their practice with the most recent evidence in this field. We sought to do this by synthesising the self-management guidance from guidelines for PwS.
Clinical practice guidelines
According to Heiwe et al. (2011), nearly 80% of clinicians utilise guidelines to inform their work. Guidelines are ‘statements that include recommendations intended to optimize patient care that are informed by systematic review of evidence and an assessment of the benefits and harms of alternative care options’ (Institute of Medicine, 2011: 26). Favourable guidelines are thorough and robust, clearly stating editorial independence and detailing cost implications of recommendations, while poorly constructed guidelines may not employ systematic reviews to underpin recommendations or may omit patient preference (Jolliffe et al., 2018; Martinez-Garcia et al., 2012). Well-constructed guidelines can optimise patient care however, the Institute of Medicine (2011) argues that the trustworthiness of stroke guidelines is debatable, given the variability in how they are formulated. Poorly evidenced guidelines risk the dissemination of inaccurate knowledge, highlighting the need to evaluate the suitability of current stroke guidelines to support self-management in stroke care.
Self-management post-stroke is essential to support PwS and to optimise healthcare resources. However, inconsistency in the definition of self-management in stroke literature and potential variability in stroke guideline quality, among other factors outside the scope of this review, limit the implementation of self-management post-stroke in practice for occupational therapists. Therefore, this article aims to (1) identify up-to-date, international stroke guidelines and synthesise their self-management recommendations, and (2) assess the quality of such guidelines including the evidentiary basis of their recommendations.
Method
The Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines (Page et al., 2021) were adhered to when planning and conducting this systematic review (Appendix 1). Written informed consent and ethical approval were not required.
Search strategy
Sources searched
Stroke association and guideline database websites were searched in July 2021 using the search tab on each website to search for key words such as ‘stroke’, ‘guideline’ and ‘self-management’ and hand searching the guidelines section of each website, where available. Where numerous results were returned, the titles of such articles were extracted into a word document. Finally, reference lists of included guidelines were checked. Duplicates were removed using the ‘remove duplicates’ function in Rayyan, which is one of the functions of this software (Quzzani et al., 2016), and then checked during the screening process.
Inclusion/Exclusion
Titles and abstracts of retrieved articles were screened by two independent reviewers (LH reviewing all and PB and SL reviewing half each) using Rayyan according to the following criteria (Quzzani et al., 2016):
Inclusion criteria Guidelines focused on stroke management only, Guidelines that make recommendations on self-management post-stroke for adults (>18), Guidelines published between January 2012 and July 2021, The most recent version of the guideline and Guidelines published or translated into English.
Exclusion criteria Guidelines that focused on palliative care only, Guidelines that focused on the organisation of stroke systems and not the care of PwS and Guidelines that made recommendations on the prevention of stroke only.
Guidelines published since January 2012 were included as it is recommended that guidelines are updated every three to 5 years (Almazrou Mazrou, 2013). To allow time for publication and dissemination of new guidelines this period was extended in this study. Furthermore, self-management recommendations focused primarily on the prevention of stroke were outside the scope of this review. Guidelines which met the above criteria were assessed via full text for inclusion in the review.
Appraisal of guidelines
The methodological quality of included guidelines was assessed using the Appraisal of Guidelines Research and Evaluation 2nd Edition (AGREE-II) instrument (AGREE Next Steps Consortium, 2009). This tool is widely accepted within the guideline development community internationally and is valid and reliable. It consists of 23 items across six domains: Scope and Purpose, Stakeholder Involvement, Rigour of Development, Clarity of Presentation, Applicability and Editorial Independence. Four reviewers independently (LH, PB, SL and AMcC) conducted the appraisal exercise and met to agree a consensus score for seven of the included guidelines (Canada 2019a, 2019b, 2019c; Canada 2018; USA 2019; Netherlands 2014; Australia 2021). Raw AGREE-II scores for the remaining guidelines were taken from the appraisal exercise in McCurtin et al. (2020), in which two authors of this paper (PB and AMcC) were involved. The same appraisal method was used in both studies. Scores for each domain were then converted to a scaled domain percentage as per the AGREE-II User’s Manual for all included guidelines, with a score of greater than 60% in at least five domains denoting a high-quality guideline (Quintyne and Kavanagh, 2017). Each reviewer also derived an overall score and recommendation for use for each guideline. Overall guideline percentages were calculated (mean of six scaled domain percentages) for comparison purposes only and did not influence ratings of guideline quality.
Data extraction and analysis
Each included guideline was reviewed and recommendations which met the definition of self-management for the purpose of this review were extracted into a word document and classified under six categories developed by Lorig and Holman (2003): • Knowledge (including information provision), • Problem-solving, • Shared decision-making, • Resource utilisation, • Partnership with a healthcare professional and • Taking action.
Where self-management recommendations did not fit into these categories, supplementary classifications were added by the authors based on self-management literature in PwS (Jones et al., 2016; Lennon et al., 2013; Warner et al., 2015). Recommendations with no clear evidentiary basis were excluded as the focus of this review was to synthesise evidence-based self-management recommendations for clinicians to implement in practice. A level of evidence was retrieved for each self-management recommendation from the guideline directly if identified within the guideline and if not, by using the Canadian Stroke Best Practice Recommendations framework (Hebert et al., 2015). The Canadian Stroke Best Practice Recommendations framework was designed to evaluate the underpinning evidence in stroke guidelines and clearly defines each category, where level A represents strong evidentiary basis, level B epitomises moderate quality evidence and level C represents limited research support and/or clinical expertise.
Results
Included guidelines
A total of 2329 documents were retrieved from initial searches and 11 guidelines met inclusion criteria (Figure 1). Fourteen guidelines were excluded as they were out-of-date (n = 6), did not make any post-stroke self-management recommendations (n = 6) or focused on secondary prevention of stroke only (n = 2) (Appendix 3). PRISMA flow diagram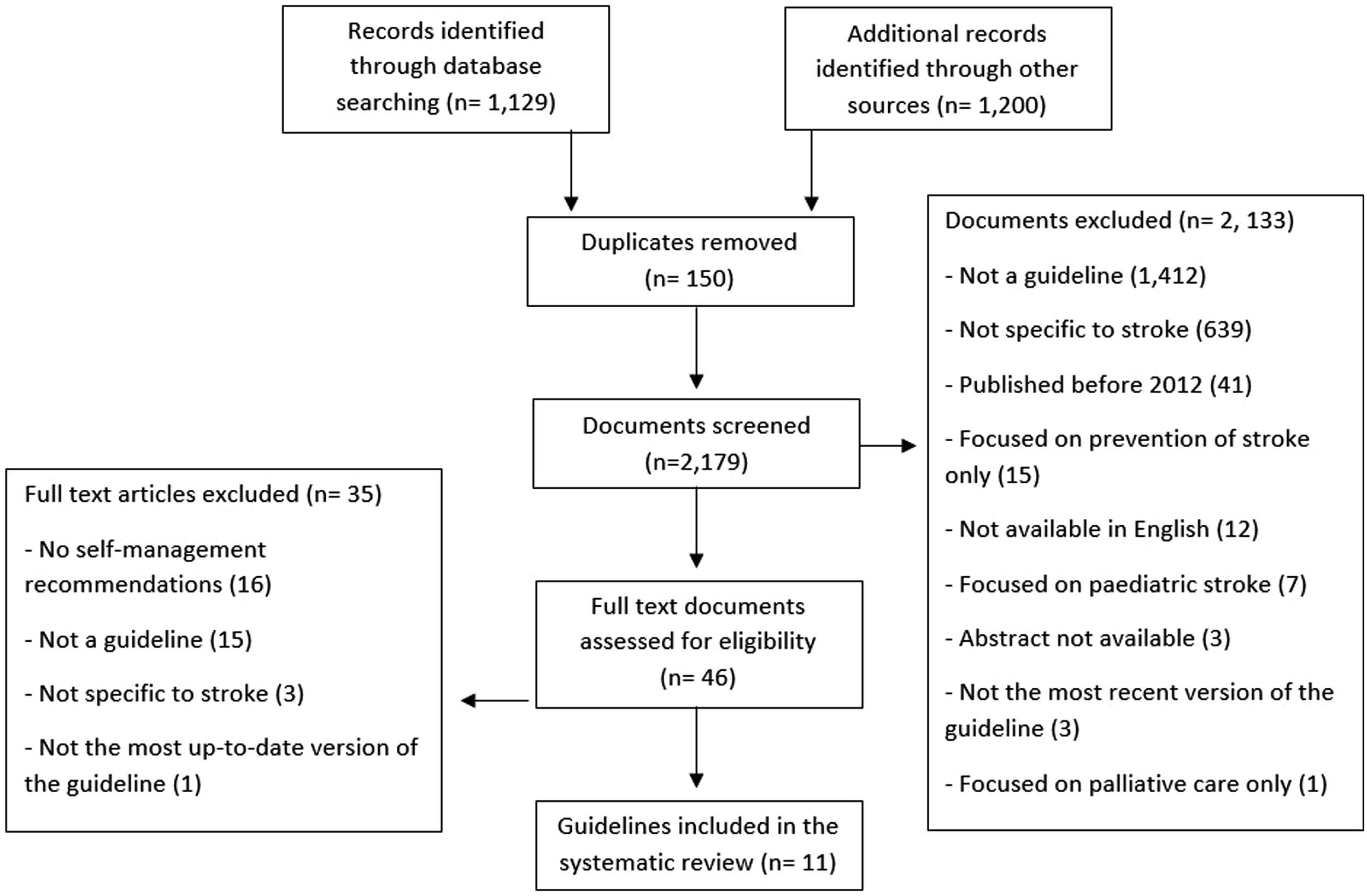
Included guidelines

Quality of included guidelines
Eleven guidelines were critically appraised using the AGREE-II instrument. Overall, the included guidelines were of high quality, with nine scoring greater than 60% in all six domains (Appendix 4). UK 2016 scored highest overall (92.6%), followed closely by UK 2013 (91.7%) and Canada 2019a (88.4%) (Figure 2). Guidelines scored highest in ‘Scope and Purpose’ (94.7%) and lowest in ‘Applicability’ (72.8%). The overall score for USA 2016 was impacted by poor rating in ‘Stakeholder Involvement’ (29.2%) and ‘Applicability’ (58.3%). Cameroon 2013 was ranked lowest and was the only guideline to score less than 60% overall, only meeting this status in two domains: ‘Scope and Purpose’ (86.1%) and ‘Applicability’ (60.4%). Overall AGREE-II percentages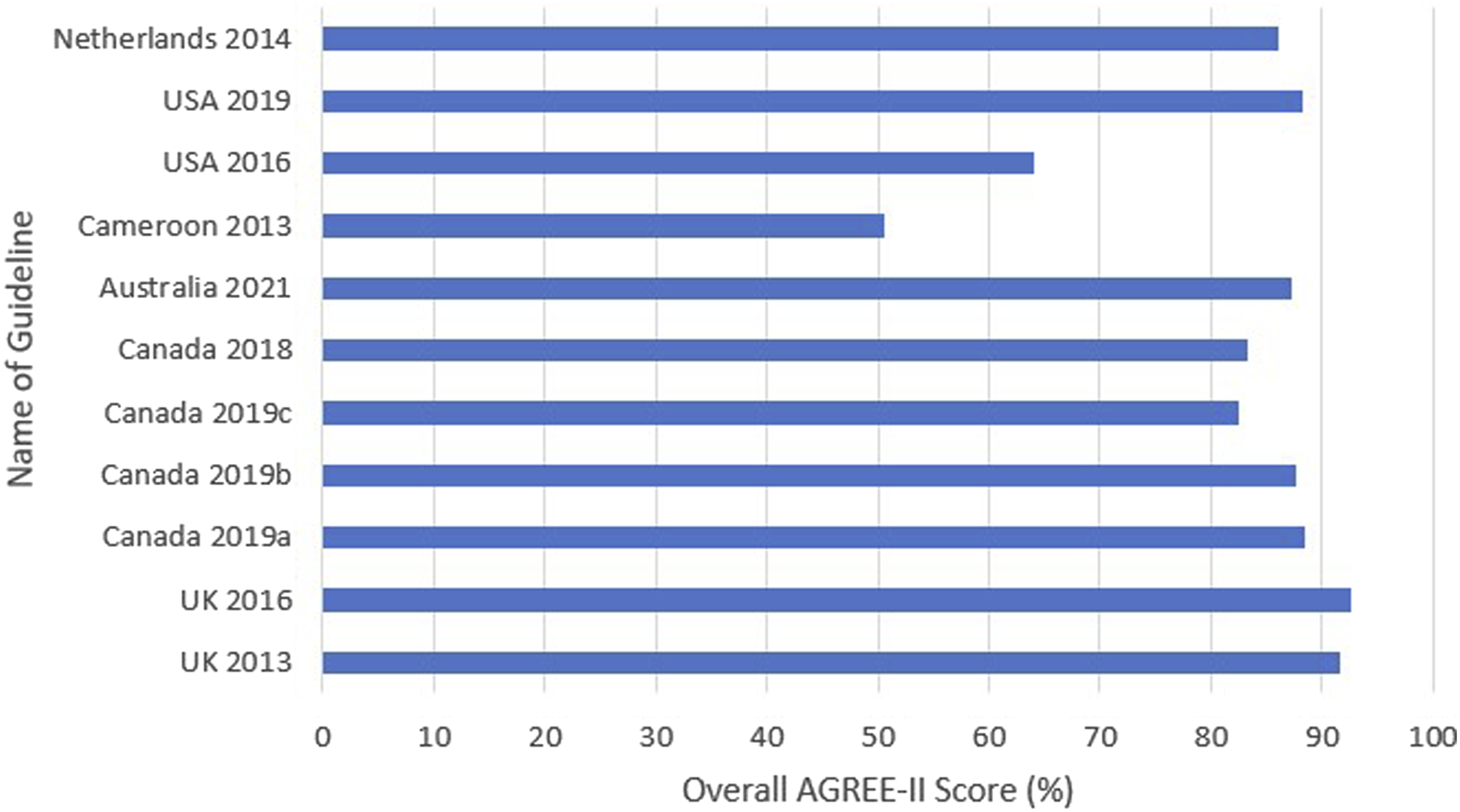
Data extraction: Self-management recommendations
Although the phrase ‘self-management’ is mentioned in half of the included guidelines, recommendations regarding a self-management programme were only present in UK 2016 and Australia 2021. Australia 2021 did not indicate whether generic, stroke-specific or individualised self-management programmes are more beneficial for PwS. On the other hand, UK 2016 recommended an individualised self-management programme only. Elements of such programmes include information on medication, advice on compliance to stroke management plans and psychological education. Furthermore, UK 2016 recommended that self-management plans should be based on increasing the stroke survivor’s self-efficacy, and that PwS should practice self-care outside formal therapy time. On the contrary, Canada 2019b recommended that self-efficacy should be supported ‘by providing opportunities to learn and master self-management skills’. Increasing self-efficacy is also recommended in Canada 2019c as a treatment for memory impairment. No detailed self-management intervention was available in any up-to-date stroke guideline.
Based on the definition for self-management for the purpose of this review, 184 potential self-management recommendations were extracted from the included guidelines. Twenty-three self-management recommendations, including both recommendations from Netherlands 2014, were excluded secondary to a lack of underpinning evidence. A list of such recommendations is available on request. Therefore, 161 recommendations from ten guidelines were included in data synthesis (Appendix 5). Within these recommendations, there were ten self-management principles identified; four fitting the principles defined by Lorig and Holman (2003) (problem-solving, shared decision-making, resource utilisation and partnership with a healthcare professional), two derived from Lorig and Holman’s (2003) fifth principle ‘taking action’ (further developed into collaborative goal setting and behaviour change for this review) as it appeared more intuitive for occupational therapists to view this concept as two separate strategies, and four additional principles developed by the authors based on relevant literature in self-management and stroke which did not fit existing categories, to best summarise all relevant self-management recommendations within the guidelines (knowledge, carer involvement, support and reintegration into the community) (Jones et al., 2016; Lennon et al., 2013; Warner et al., 2015). A description of each self-management principle and its frequency across guidelines is detailed in Figure 3. Principle 1: Problem-solving Ten self-management principles included and their frequency (n =, %) in self-management recommendations in included guidelines

Problem-solving, used to overcome a barrier, was recommended in UK 2016 and USA 2016, with the latter guideline including an explicit link to evidence showcasing a detailed problem-solving intervention. Problem-solving was also recommended twice in Canada 2019c as an internal strategy to ameliorate both cognitive and mental health impairments. Principle 2: Shared decision-making
This self-management principle was mentioned 13 times across five guidelines, with examples including that PwS and their carers should be involved in decisions about their transfer of care (UK 2013; UK 2016; Canada 2019b), continence management, aphasia intervention plans (Australia 2021) and nutritional support (Canada 2019a). Principle 3: Resource utilisation
Resource utilisation, in the form of accessing disability services and specialised services such as continence clinics and telemedicine, was recommended 16 times across four guidelines (UK 2013; UK 2016; Australia 2021; Canada 2019b). Further, Australia 2021 recommended local peer support groups for PwS and for their carers, while Canada 2019b made this recommendation solely for PwS. These two guidelines also recommended community-based self-management programmes, with the latter guideline also stating that PwS should be made aware of suitable resources to help them navigate the healthcare system. Principle 4: Partnership with a healthcare professional
This self-management principle was recommended six times across four of the included guidelines. Australia 2021, Canada 2019b and UK 2016 recommended that PwS should receive a point of contact for further advice and support post-discharge, with UK 2013 recommending this specifically in the context of a hand splint. UK 2016 also recommended that there needs to be a designated healthcare professional as a point of contact for the carer. Principle 5: Knowledge
Knowledge, including the provision of information, was the most frequently recommended self-management principle (n = 77), present on average seven times per guideline. USA 2019 was the only guideline to omit this principle (Appendix 5), while it was most evident in UK 2016 (n = 23), covering topics such as driving, falls and aphasia. There were many general recommendations made regarding knowledge also; education should take place at all stages of stroke recovery and should be reinforced if required. Further, Cameroon 2013 recommended that PwS need to be involved in their rehabilitation to understand the principles of self-management, concluding that information provision alone is not enough. This is echoed in Canada 2019a where it is recommended that PwS are encouraged to integrate skills learned in therapy into their daily routine. Principle 6: Involvement of a carer
The involvement of a carer in the post-stroke rehabilitation journey was recommended in all guidelines except USA 2019. Within this principle, there were references to general carer involvement (n = 11), carer knowledge (n = 52) and carer support (n = 9). The involvement of a carer was recommended most commonly in UK 2016 (n = 22). This guideline recommended a carer education programme focusing on information about stroke, potential problems post-stroke, practice caring for PwS and the provision of practical and emotional support for the carer as necessary. Furthermore, Australia 2021 recommended ‘active task practice’ for PwS lead by the carer outside of formal therapy sessions. Principle 7: Support
Although sometimes overlapping with the principle ‘partnership with a healthcare professional’ and the sub-theme of ‘carer involvement’; ‘carer support’, supporting PwS is also a self-management principle and was recommended in half of the included guidelines (USA 2016; UK 2013, 2016; Australia 2021; Canada 2019b); PwS should be supported by a variety of people, both physically and psychologically, throughout their post-stroke journey, especially at times of low self-esteem and low self-efficacy. Principle 8: Reintegration into the community
USA 2016, UK 2016 and Canada 2019b were the only guidelines to make a recommendation on reintegration into the community. The two former guidelines recommended collaborative goal setting to empower PwS to partake in leisure activities and therefore, increase their participation in the community. Canada 2019b made seven recommendations regarding this principle, including recommendations around community exercise programmes and engagement in vocational interests. Principle 9: Collaborative goal setting
Collaborative goal setting was recommended in half of the guidelines (UK 2013, 2016; Australia 2021; Canada 2019b, c), with recommendations relatively similar throughout; involvement of PwS and their carer in the goal setting process, specifically in the context of spasticity (UK 2016). Most guidelines also recommended explanation of the goal setting process to PwS and their carer. Principle 10: Behaviour change
Behaviour change was the only self-management principle recommended in USA 2019. Like UK 2016, Australia 2021 and Canada 2019c, this guideline recommended behaviour change as an intervention to treat anxiety and depression, with motivational interviewing the most common intervention. UK 2016 also recommended behaviour change as a treatment for aphasia and urinary incontinence.
Data extraction: Levels of evidence
UK 2016 was the only guideline that did not assign a level of evidence to each recommendation within the guideline. UK 2013, Australia 2021 and USA 2019 utilised the Grading of Recommendations Assessment, Development and Evaluation (GRADE) framework (Balshem et al., 2011). The level of evidence underpinning recommendations in such guidelines was assigned by LH using the Canadian Stroke Best Practice Recommendations framework (Hebert et al., 2015) (Appendix 5). All other guidelines included in data synthesis (n = 6) had already employed this same tool.
In general, there was mixed quality evidence underpinning self-management recommendations, with 25% of recommendations level A, 32% level B and 43% level C (Appendix 5). However, 16 of the 40 level A recommendations cited other guidelines as their evidentiary basis, making their level of evidence questionable in the context of this study. Encouraging self-management through behaviour change was the only principle to solely employ level A (25%, n = 1) and level B (75%, n = 3) evidence to underpin its recommendations, with collaborative goal setting also having a relatively good evidence base (two thirds were level A evidence). On the other hand, over half (55.8%) of the knowledge recommendations were level C, with 19.5% level A and 24.7% level B. Problem-solving had limited research support with no level A recommendations, three level B (75%, n = 3) and one level C (25%, n = 1). Furthermore, recommendations regarding self-management programmes were supported by level A evidence in UK 2016 (n = 3) and level B evidence in Australia 2021 (n = 3).
Discussion and implications
To the best of our knowledge, this is the first systematic review to explore the quality of up-to-date stroke guidelines in relation to self-management. Although there is evidence from systematic reviews to suggest self-management post-stroke is effective, through promotion of person-centred autonomy (Warner et al., 2015) and reduction of the strain on healthcare systems, there is absence of the explicit term ‘self-management’ in stroke guidelines and therefore, its implementation in practice. Thus, we have presented occupational therapists with a synthesised set of self-management principles, where evidence and implementation advice were also available, and their level of evidence from ten high-quality international stroke guidelines, as a step towards improving the implementation of self-management in stroke care.
Quality of guidelines
Included guidelines were of excellent quality overall. When results of this review are compared to those of Rohde et al. (2013), the improvement in the development process of stroke guidelines in recent decades is evident; UK 2016, Australia 2021 and USA 2019 have improved their overall AGREE-II scores by 7.0%, 27.2% and 44.8% respectively, compared to the previous version of the same guidelines. This said, variation between development processes of stroke guidelines still exist. This was most evident in Cameroon 2013 where the guideline development group failed to explicitly state funding sources, conflicts of interest or the procedure for updating the guideline. Moreover, across all included guidelines, ‘Applicability’ was the lowest scoring domain, followed by ‘Stakeholder Involvement’. Guidelines fell short in ‘Applicability’ as barriers and facilitators and tools to support implementation were absent from many of the guidelines. The views and preferences of the target population were not sought consistently, which is another major limitation of current stroke guidelines as patient preference is an important element of evidence-based practice.
Contrastingly, guidelines scored well in the domains ‘Scope and Purpose’ and ‘Editorial Independence’. High scores in ‘Editorial Independence’ is a promising finding as conflicts of interest or influence from funding bodies can cause bias and produce skewed, unreliable recommendations.
This study highlights to clinicians and policy-makers that many commonly used guidelines in a British and Irish context (e.g. Scottish Intercollegiate Guideline Network, 2010) are outdated and therefore, more up-to-date guidelines from elsewhere are recommended for consideration. Clinicians could use the AGREE-II scores outlined in this paper to assist them in selecting well-designed guidelines to inform their practice.
Self-management recommendations
Recommendations regarding specifically designed self-management programmes were only present in UK 2016 and Australia 2021. Such absence in leading stroke guidelines can be associated with the lack of a consistent, internationally recognised self-management definition (Sadler et al., 2017), making it difficult for guideline development groups to recommend consistently, and therefore reducing its adoption in practice. This inconsistency is heightened due to different guideline development groups producing stroke guidelines with various methodological frameworks at different time points.
Both Australia 2021 and UK 2016 have a chapter dedicated to self-management, each making three self-management recommendations however, insufficient detail impacts an occupational therapist’s ability to utilise them in practice. Australia 2021 does not indicate which type of self-management programme provides better outcomes for PwS. The latter guideline states, in line with recent evidence in stroke (Jones et al., 2016), that ‘self-efficacy may mediate self-management’ and that an individualised programme is most effective. However, such programmes are challenging to implement in stroke care as they must be integrated into existing rehabilitation to mitigate large associated cost and time implications (Jones et al., 2016). Furthermore, despite a wealth of evidence showing that self-management programmes based on self-efficacy are effective and are currently being utilised in practice to facilitate self-management in PwS (Jones et al., 2016), Canada 2019b and 2019c are the only other guidelines to recommend self-efficacy. In conclusion, there is a gap between primary research literature and guidelines regarding the evidence for self-management post-stroke, meaning detailed, consistent self-management recommendations which can be implemented in practice are omitted from current stroke guidelines.
Furthermore, inconsistent self-management principles in stroke literature makes implementing self-management based on its principles in stroke guidelines a difficult task. For example, Lorig and Holman (2003) do not consider collaborative goal setting as a self-management principle whereas Warner et al. (2015) and Jones et al. (2016) do. Therefore, in this article, additional principles to the five recognised by Lorig and Holman (2003) were required to capture all relevant self-management recommendations within the guidelines. Knowledge was the most consistently recommended self-management principle, which is promising as it is considered the most effective principle, where its implementation has shown large benefits in the stroke survivor’s awareness of their own health, self-efficacy and self-management. Carer knowledge was also frequently recommended (23.2%). Conversely, principles of collaborative goal setting and behaviour change, both of which are considered important to clinicians and PwS, are poorly represented in current stroke guidelines.
Where self-management recommendations in stroke guidelines can be extracted by clinicians, their evidence base limits the ability of such recommendations to aid clinical decision-making. The majority of self-management recommendations in stroke guidelines are not founded on high-quality experimental evidence, with 42.9% based on writing group consensus and/or limited research evidence. Moreover, 12.5% of self-management recommendations present in included guidelines lacked any underpinning evidence. Thus, self-management recommendations with low levels of evidence have been highlighted in this review for researchers, clinicians and healthcare decision- and policy-makers.
Although the challenge for occupational therapists of delivering self-management in practice is likely multifaceted, the absence of detailed self-management recommendations in leading stroke guidelines, coupled with the lack of a self-management definition and inconsistent self-management principles in stroke literature, is one issue as it is unclear for occupational therapists what self-management principles should be prioritised for adoption in practice. It therefore begs the question whether current stroke guidelines are indeed the best tools to facilitate the implementation of self-management post-stroke. Two key recommendations are the development of a consensus of self-management post-stroke which is recognised globally and subsequently, an international guideline for self-management in PwS.
That said, there are some clear take-away messages from this review for occupational therapists working in stroke care, who are motivated to develop or embed self-management principles in their practice. Firstly, taking time to develop and deliver information about stroke symptoms and resources (including discharge options), which are accessible to their clients and carers is valuable at enabling self-management as this was a consistently cited self-management principle. Secondly, shared decision-making is also connected to enabling both patient and family (and joint) communication around goal setting and prioritisation during intervention. These findings are consistent with wider literature on self-management (Dineen-Griffin et al., 2019; Lenzen et al., 2015).
Strengths and limitations
The robust and transparent search strategy conducted in our review, which included 18 stroke association and guideline database websites, is a strength of this article. This type of search strategy is important as many guideline developers post guidelines directly online, rather than through bibliographic sources (ADAPTE Collaboration, 2009). Identified articles were screened by two independent reviewers. This was followed by the precise application of eligibility criteria to identify up-to-date, international stroke guidelines. Included guidelines were critically appraised by four independent reviewers as per the AGREE-II user’s manual (ADAPTE Collaboration, 2009). Finally, all identified self-management recommendations were synthesised, along with their corresponding level of evidence in a clear, accessible way for occupational therapists to utilise in practice. However, there are some limitations which could have biased our study. Firstly, only guidelines published or translated into English were included, meaning guidelines written in other languages could have been neglected. Moreover, our review was biased towards evidence and health services in Western countries with nine of the eleven included guidelines published in Europe, North America and USA. Thirdly, the software Rayyan (Quzzani et al., 2016), used to screen articles for inclusion, has some limitations; it does not collate reasons for excluding articles during the screening process and does not produce a PRISMA diagram (Kellermeyer et al., 2018). Fourthly, one author (LH) independently extracted the self-management recommendations by hand, increasing the risk of sample bias. Finally, we acknowledge the limited consideration of qualitative research in this review, given that guidelines inherently privilege quantitative literature, and that some useful qualitative evidence in the area of self-management post-stroke may have been omitted.
Future research
The findings of this review identify several areas for future research. Stroke guidelines which are more than five years old must be updated to avoid the dissemination of inaccurate or out-dated knowledge (Almazrou Mazrou, 2013). Such updates must include PwS as stakeholders early in the development process and tools for implementing the guideline, along with a discussion regarding barriers and facilitators to implementation as these areas were ranked lowest in this study on the AGREE-II tool. Secondly, a systematic review which encompasses self-management recommendations regarding secondary prevention of stroke could be valuable. Thirdly, additional high-quality trials, to establish optimal self-management programme length and content specific to PwS are also essential, as current systematic reviews are unable to establish these principles due to the large heterogeneity between published post-stroke self-management programmes (Jones et al., 2016). In addition, we recommend that a qualitative systematic review or meta-analysis is conducted to complement stroke guidelines and aid the implementation of self-management in stroke practice. Finally, a mixed methods scoping review would be beneficial to map the current literature and aid the development of a universal, international guideline regarding self-management in PwS, which could improve the consistency of this intervention in practice and reduce the pressure on healthcare systems (Jones et al., 2016).
Conclusion
Current, up-to-date stroke guidelines are of high methodological quality overall. However, the lack of detailed self-management recommendations in such guidelines, coupled with the absence of a self-management definition and inconsistent self-management principles in stroke literature, is one of the barriers to the implementation of self-management in practice using current stroke guidelines. Furthermore, the evidentiary basis of self-management recommendations is of varying quality. This study identifies a need to develop a consensus of self-management post-stroke, which is recognised worldwide and thereafter, a universal, international guideline for self-management in PwS.
Key findings
• The lack of the explicit term ‘self-management’ in current stroke guidelines limits its implementation in practice. • A consensus of self-management is essential to advance research and support the healthcare system.
What the study has added
This article highlights that many commonly used international stroke guidelines are outdated and presents clinicians with an accessible list of 161 self-management recommendations along with their level of evidence.
Footnotes
Contributorship
PB conceived the study. LH, PB and SL were involved in study design and database/website searching. All authors critically appraisal the included guidelines. LH extracted, evaluated and synthesised the data. All authors were involved in reviewing and editing the manuscript and approved the final version for submission.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Appendix 1. PRISMA checklist
Section and topic
Item #
Checklist item
Location where item is reported
Title
Title
1
Identify the report as a systematic review
Page 1
Abstract
Abstract
2
See the PRISMA 2020 for Abstracts checklist (Table 2)
Page 1
Introduction
Rationale
3
Describe the rationale for the review in the context of existing knowledge
Page 2 and 3
Objectives
4
Provide an explicit statement of the objective(s) or question(s) the review addresses
Page 3
Methods
Eligibility criteria
5
Specify the inclusion and exclusion criteria for the review and how studies were grouped for the syntheses
Page 4
Information sources
6
Specify all databases, registers, websites, organisations, reference lists and other sources searched or consulted to identify studies. Specify the date when each source was last searched or consulted
Page 3 and 4 and Table 1
Search strategy
7
Present the full search strategies for all databases, registers and websites, including any filters and limits used
Appendix 2
Selection process
8
Specify the methods used to decide whether a study met the inclusion criteria of the review, including how many reviewers screened each record and each report retrieved, whether they worked independently, and if applicable, details of automation tools used in the process
Page 4 and 5
Data collection process
9
Specify the methods used to collect data from reports, including how many reviewers collected data from each report, whether they worked independently, any processes for obtaining or confirming data from study investigators, and if applicable, details of automation tools used in the process
Page 5 and 6
Data items
10a
List and define all outcomes for which data were sought. Specify whether all results that were compatible with each outcome domain in each study were sought (e.g. for all measures, time points and analyses), and if not, the methods used to decide which results to collect
Page 5 and 6
10b
List and define all other variables for which data were sought (e.g. participant and intervention characteristics and funding sources). Describe any assumptions made about any missing or unclear information
N/A
Study risk of bias assessment
11
Specify the methods used to assess risk of bias in the included studies, including details of the tool(s) used, how many reviewers assessed each study and whether they worked independently, and if applicable, details of automation tools used in the process
Page 5
Effect measures
12
Specify for each outcome the effect measure(s) (e.g. risk ratio and mean difference) used in the synthesis or presentation of results
N/A
Synthesis methods
13a
Describe the processes used to decide which studies were eligible for each synthesis (e.g. tabulating the study intervention characteristics and comparing against the planned groups for each synthesis (item #5))
N/A
13b
Describe any methods required to prepare the data for presentation or synthesis, such as handling of missing summary statistics, or data conversions
N/A
13c
Describe any methods used to tabulate or visually display results of individual studies and syntheses
N/A
13d
Describe any methods used to synthesise results and provide a rationale for the choice(s). If meta-analysis was performed, describe the model(s), method(s) to identify the presence and extent of statistical heterogeneity, and software package(s) used
Page 5
13e
Describe any methods used to explore possible causes of heterogeneity among study results (e.g. subgroup analysis and meta-regression)
N/A
13f
Describe any sensitivity analyses conducted to assess robustness of the synthesised results
N/A
Reporting bias assessment
14
Describe any methods used to assess risk of bias due to missing results in a synthesis (arising from reporting biases)
N/A
Certainty assessment
15
Describe any methods used to assess certainty (or confidence) in the body of evidence for an outcome
Page 5 and 6
Results
Study selection
16a
Describe the results of the search and selection process, from the number of records identified in the search to the number of studies included in the review, ideally using a flow diagram (see Figure 1)
Page 6 and Figure 1
16b
Cite studies that might appear to meet the inclusion criteria, but which were excluded, and explain why they were excluded
Page 6 and Appendix 3
Study characteristics
17
Cite each included study and present its characteristics
Table 2
Risk of bias in studies
18
Present assessments of risk of bias for each included study
Page 6, Figure 2 and Appendix 4
Results of individual studies
19
For all outcomes, present, for each study: (a) summary statistics for each group (where appropriate) and (b) an effect estimate and its precision (e.g. confidence/credible interval), ideally using structured tables or plots
N/A
Results of syntheses
20a
For each synthesis, briefly summarise the characteristics and risk of bias among contributing studies
Page 8-10
20b
Present results of all statistical syntheses conducted. If meta-analysis was done, present for each the summary estimate and its precision (e.g. confidence/credible interval) and measures of statistical heterogeneity. If comparing groups, describe the direction of the effect
N/A
20c
Present results of all investigations of possible causes of heterogeneity among study results
N/A
20d
Present results of all sensitivity analyses conducted to assess the robustness of the synthesised results
N/A
Reporting biases
21
Present assessments of risk of bias due to missing results (arising from reporting biases) for each synthesis assessed
N/A
Certainty of evidence
22
Present assessments of certainty (or confidence) in the body of evidence for each outcome assessed
Page 10 and 11
Discussion
Discussion
23a
Provide a general interpretation of the results in the context of other evidence
Page 11-13
23b
Discuss any limitations of the evidence included in the review
Page 12 and 13
23c
Discuss any limitations of the review processes used
Page 14
23d
Discuss implications of the results for practice, policy and future research
Page 14
Other information
Registration and protocol
24a
Provide registration information for the review, including register name and registration number, or state that the review was not registered
N/A
24b
Indicate where the review protocol can be accessed, or state that a protocol was not prepared
N/A
24c
Describe and explain any amendments to information provided at registration or in the protocol
N/A
Support
25
Describe sources of financial or non-financial support for the review, and the role of the funders or sponsors in the review
Page 16
Competing interests
26
Declare any competing interests of review authors
Page 16
Availability of data, code and other materials
27
Report which of the following are publicly available and where they can be found: template data collection forms; data extracted from included studies; data used for all analyses; analytic code and any other materials used in the review
N/A
Appendix 2. Sample search for Scopus (completed 20/02/2021)
Search string
Limitations
Number of hits
Stroke OR cerebrovasc* OR cva* OR post-stroke OR cerebral accident
214,756
Guideline* OR clinical guideline* OR practice guideline* OR consensus OR expert consensus OR opinion* OR expert opinion* OR expert testimon* OR clinical consensus OR clinical opinion OR consensus document OR recommendation
290,074
Self-management OR self-efficacy OR self-care OR empowerment
661,086
Parkinson* disease OR PD OR traumatic brain injury OR TBI OR acquired brain injury OR ABI OR pediatric* OR paediatric* OR child OR adolescen*
129,946
(Stroke OR cerebrovasc* OR cva* OR post-stroke OR post-stroke OR cerebral accident) AND (Guideline* OR clinical guideline* OR practice guideline* OR consensus OR expert consensus OR opinion* OR expert opinion* OR expert testimon* OR clinical consensus OR clinical opinion OR consensus document OR recommendation) AND (Self-management OR self-efficacy OR self-care OR empowerment) NOT (Parkinson* disease OR PD OR traumatic brain injury OR TBI OR acquired brain injury OR ABI OR pediatric* OR paediatric* OR child OR adolescen*)
English only 2012-2021
316
Appendix 3. Excluded guidelines
Key: D = published before 2012, S = no self-management recommendations in the guideline, SP = secondary prevention recommendations only.
Guideline
Year
Developing organization
Funding/support source
Reason for exclusion
Ireland
2010
The Irish Heart Foundation
MSD Ireland
D
SIGN #118
2010
Scottish Intercollegiate Network (SIGN)
NHS Quality Improvement Scotland
D
SIGN #119
2010
Scottish Intercollegiate Network (SIGN)
NHS Quality Improvement Scotland
D
New Zealand
2010
Stroke Foundation of New Zealand
New Zealand Ministry of Health
D
Ontario
2011
Registered Nurses’ Association of Ontario/Heart and Stroke Foundation of Ontario
The Government of Ontario
D
Philippines
2010
The Stroke Society of the Philippines (SSP)
Not clearly stated
D
UK
2019
National Institute for Health and Care Excellence
Not clearly stated
S
USA
2018
American Heart Association (AHA)/American Stroke Association (ASA)
The American Association of Neurological Surgeons and Congress of Neurological Surgeons and The Society for Academic Emergency Medicine and Neurocritical Care Society
S
USA
2019
ICSI Diagnosis and Initial Treatment of Ischemic Stroke Work Group
The Institute for Clinical Systems Improvement
S
Qatar
2016
Ministry of Public Health in Qatar
Ministry of Public Health in Qatar
S
Malaysia
2012
Malaysian Society of Neurosciences
Boehringer Ingelheim (M) Sd. Bhd
S
Germany
2013
German Nutrition Society (DGEM) German Society for Neurology, German Geriatric Society
German Nutrition Society (DGEM) German Society for Neurology, German Geriatric Society
S
Canada
2017
Secondary Prevention of Stroke writing group
Heart and Stroke Foundation, Canada
SP
USA
2014
American Heart Association/American Stroke Association
Not clearly stated
SP
Appendix 4. AGREE-II scores
Guideline
Scaled domain percentage (domain score)
Scope and purpose
Stakeholder involvement
Rigour of development
Clarity of presentation
Applicability
Editorial independence
Overall score
Recommendation
UK 2013
98.6% (83)
91.7% (78)
96.6% (217)
91.7% (78)
88.5% (101)
83.3% (48)
91.7% (605)
Yes
UK 2016
100% (84)
81.9% (71)
94.8% (214)
94.4% (80)
84.4% (97)
100% (56)
92.6% (602)
Yes
Canada 2019a
95.8% (81)
95.8% (81)
78.1% (182)
88.9% (76)
71.9% (85)
100% (56)
88.4% (561)
Yes
Canada 2019b
95.8% (81)
91.7% (78)
78.1% (182)
88.9% (76)
71.9% (85)
100% (56)
87.7% (558)
Yes
Canada 2019c
97.2% (82)
72.2% (64)
76.6% (179)
90.3% (77)
64.6% (78)
93.8% (53)
82.5% (533)
Yes
Canada 2018
100% (84)
72.2% (64)
75.5% (177)
83.3% (72)
70.8% (84)
97.9% (55)
83.3% (536)
Yes
Australia 2021
100% (84)
97.2% (82)
89.6% (204)
86.1% (74)
76.0% (89)
75% (44)
87.3% (577)
Yes
Cameroon 2013
86.1% (74)
41.7% (42)
36.5% (102)
59.7% (55)
60.4% (74)
18.8% (17)
50.5% (364)
Yes
USA 2016
77.8% (68)
29.2% (33)
73.4% (173)
68.1% (61)
58.3% (72)
77.1% (45)
64.0% (452)
Yes
USA 2019
93.1% (79)
95.8% (81)
94.8% (214)
98.6% (83)
84.4% (81)
62.5% (30)
88.2% (568)
Yes
Netherlands 2014
97.2% (82)
80.6% (70)
82.3% (190)
88.9% (76)
69.8% (83)
97.9% (47)
86.1% (548)
Yes
Appendix 5. Included self-management recommendations
*Level of evidence was assigned by LH.
Guideline
Extracted recommendation
Self-management principle
Main evidence cited
Level of evidence
Canada 2018
All patients, family members and informal caregivers should receive timely and comprehensive information, education and skills training by all interdisciplinary team members (9.0, iv)
Knowledge and carer knowledge
Canada 2016 Guideline
A
USA 2019
We suggest offering cognitive behavioural therapy for treatment of post-stroke depression
Behaviour change
Other Guidelines
Wang et al., 2018B*
USA 2016
It may be reasonable that family/caregiver support include some or all of the following on a regular basis:
Education
Training
Counselling
Development of a support structure
Financial assistanceCarer knowledge and carer support
Visser-Meily et al. 2005
Steiner et al. 2008
Campos de Oliveira et al. 2011
Thomas et al. 2008
Perrin et al. 2010
Levine et al. 2006
Salter et al. 2009
Lurbe-Peurto et al., 2012A
It is reasonable that individuals with stroke and their caregivers receive information targeted to home and environmental modifications designed to reduce falls
Knowledge and carer knowledge
Gillespie et al., 2012
B
It is reasonable to promote engagement in leisure and recreational pursuits, particularly through the provision of information on the importance of maintaining an active and healthy lifestyle
Knowledge andreintegration into the community
Primack et al. 2012
Taylor et al. 2004
Aoyagi et al. 2010
Schwarzenegger et al., 2005B
It is reasonable to start education and self-management skill development about leisure/recreation activities during and in conjunction with in-patient rehabilitation
Knowledge
Van der Ploeg et al. 2007
Van Veenendaal et al., 1996B
Patient education about stroke is recommended. Patients should be provided with information, advice and the opportunity to talk about the impact of the illness on their lives
Knowledge and support
De Man-Van Ginkel et al., 2010
B
It is reasonable that caregivers, including family members, be involved in training and education related directly to home-based rehabilitation programs and be included as active partners in the planning and implementation or treatment activities under the supervision of professionals
Carer knowledge and carer Involvement
Bakas et al., 2014
B
It is reasonable to foster the development of self-management skills for problem-solving for overcoming barriers to engagement in active activities
Problem-solving
Desrosiers et al., 2007
B
Patients, staff and caregivers should be educated about the prevention of skin breakdown
Knowledge and carer knowledge
Clinical consideration
C
Cameroon 2013
Stroke survivors and their families should be provided with timely, up-to-date information in conjunction with opportunities to learn from members of the team and other appropriate community service providers. Simple information provision alone is not effective
Knowledge and carer knowledge
Australia National Stroke Foundation 2010
SA
GCPA
Patients and their caregivers should be offered education programs to assist them in adapting to their new role
Knowledge and carer knowledge
Lindsay et al., 2010
B
Caregivers should be educated about correct handling of the hemiplegic arm
Carer knowledge
Lindsay et al. 2010
Stroke Canada Optimization of Rehabilitation through Evidence 2007B
Canada 2019c
It is reasonable to consider either cognitive-behavioural therapy or interpersonal therapy as one of the first line treatments for depressive symptoms post-stroke (1.3, i)
Behaviour change
Mitchell et al., 2009
B
Psychotherapy (cognitive behavioural therapy) may be considered as an adjunct treatment for post-stroke fatigue (3.2, iv)
Behaviour change
Zedlitz et al. 2012
Johansson et al., 2012B
Problem-solving therapy (i.e. cognitive-behaviour therapy) has been shown to have efficacy for prophylactic treatment for post-stroke depression (1.5, iii)
Behaviour change
Hackett et al. 2008
Mitchell et al., 2009B
Memory impairments may be treated with compensation using self-efficacy training, with some evidence for benefits to activity limitations (2.3, iv)
Self-efficacy
Cicerone et al. 2011
Das Nair et al., 2016B
Executive function deficits may be treated with metacognitive strategy training and/or formal problem-solving strategies, under the supervision of a trained therapist (2.3, v)
Problem-solving
Cicerone et al. 2011
Poulin et al. 2012
Chung et al., 2013B
Internal strategy training may be considered and includes strategies to improve goal management, problem-solving, time management and metacognitive reasoning (in people with vascular cognitive impairment)
Problem-solving and Collaborative goal setting
Cicerone et al. 2011
Das Nair et al., 2016B
Counselling on energy conservation strategies that consider optimizing daily function in high priority activities is recommended (3.2, vii)
Knowledge
Zedlitz et al., 2012
B
Counselling on the establishment of good sleep hygiene behaviours is recommended (3.2, vii)
Knowledge
McEvoy et al. 2012
Ponchel et al., 2015B
Provide education to people who have experienced a stroke, their families and informal caregivers, on daily time management and planning a balance of activities with rest period (3.2, ix)
Knowledge and carer knowledge
Clarke et al. 2012
Wu et al., 2015C
Prior to discharge from acute care or inpatient rehabilitation, people who have experienced a stroke, their families and informal caregivers should be provided with basic information regarding the potential experience of post-stroke fatigue (3.1, i)
Knowledge and carer knowledge
Wu et al. 2015
Clarke et al., 2012C
UK 2013
Ensure that goal-setting meetings during stroke rehabilitation involve the person with stroke and, where appropriate, their family or carer in the discussion (1.2.9)
Collaborative goal setting
Rosewilliam (2011)
Hale (2010)A*
Tell the person with communication difficulties after stroke about community-based communication and support groups (such as those provided by the voluntary sector) and encourage them to participate. (1.8.9)
Resource utilisation
Bowen (2012)
B*
Provide information about local resources (for example, leisure, housing, social services and the voluntary sector) that can help to support the needs and priorities of the person with stroke and their family or carer (1.3.2)
Resource utilisation and knowledge
GDG consensus
Hoffman (2007)
Eilis (2005)C*
Take into consideration the impact of the stroke on the person’s family, friends and/or carers and, if appropriate, identify sources of support (1.2.6)
Carer support
GDG consensus
C*
Support and educate people after stroke and their families and carers, in relation to emotional adjustment to stroke, recognising that psychological needs may change over time and in different settings (1.5.2)
Knowledge, carer knowledge and support
Smith et al. (2012)
C*
Provide information for people with stroke and their families and carers on how to prevent pain or trauma to the shoulder if they are at risk of developing shoulder pain (for example, if they have upper limb weakness and spasticity) (1.9.20)
Knowledge and carer knowledge
GDG consensus
C*
Return-to-work issues should be identified as soon as possible after the person’s stroke, reviewed regularly and managed actively. Active management should include educating about the Equality Act 2010 and support available (for example, an access to work scheme)
Knowledge
Trexier (2010)
C*
Provide information so that people after stroke are able to recognise the development of complications of stroke, including frequent falls, spasticity, shoulder pain and incontinence (1.11.2)
Knowledge
GDG consensus
C*
Tell people who are participating in fitness activities after stroke about common potential problems, such as shoulder pain, and advise them to seek advice from their GP or therapist if these occur (1.9.9)
Knowledge and resource utilisation
GDG consensus
C*
Teach the person with stroke and their family or carer how to put the splint on and take it off, care for the splint and monitor for signs of redness and skin breakdown. Provide a point of contact for the person if concerned (hand and arm therapies) (1.9.13)
Knowledge, carer knowledge and partnership with a healthcare professional
GDG consensus
C*
Speech and language therapists should:
Knowledge, resource utilisation and carer knowledge
Bowen (2012)
C*
Hospitals should have systems in place to ensure that:
Shared decision-making, knowledge andsupport
GDG consensus
C*
Ensure that during goal-setting meetings, people with stroke are provided with an explanation of the goal-setting process, the information they need in a format that is accessible to them and the support they need to make decisions and take an active part in setting goals (1.2.10)
Collaborative goal setting
GDG consensus
C*
Working with the person with stroke and their family or carer, identify their information needs and how to deliver them, taking into account specific impairments such as aphasia and cognitive impairments. Pace the information to the person’s emotional adjustment (1.3.1)
Knowledge
GDG consensus, Hoffman 2007
C*
Australia 2020
Health professionals should initiate the process of setting goals and involvestroke survivors and their families and carers throughout the process. Goals for recovery should be client-centred, clearly communicated and documented so that both the stroke survivor (and their families/carers) and other members of the rehabilitation team are aware of goals set.
Collaborative goal setting
Sugavanam et al. 2013
A*
Goals should be set in collaboration with the stroke survivor and their family/carer (unless they choose not to participate) and should be well-defined, specific and challenging. They should be reviewed and updated regularly
Collaborative goal setting
Sugavanam et al. 2013
A*
All stroke survivors and their families/carers should be offered information tailored to meet their individual needs using relevant language and communication formats
Knowledge and carer knowledge
Forster et al., 2012
A*
Information should be provided at different stages of the recovery process
Knowledge
A*
An approach of active engagement with stroke survivors and their families/carers should be used allowing for the provision of material, opportunities for follow-up, clarification and reinforcement
Knowledge and carer involvement
A*
All stroke patients, particularly those with swallowing difficulties, should have assistance and/or education to maintain good oral and dental (including dentures) hygiene
Knowledge
Chipps et al. 2014
A*
Comprehensive discharge care plans that address the specific needs of the stroke survivor should be developed in conjunction with the stroke survivor and carer prior to discharge
Shared decision-making
Johnston et al. 2010
A*
Carers of stroke survivors should be provided with tailored information and support during all stages of the recovery process
Carer knowledge and carer support
Legg et al. 2011
A*
For stroke survivors who are at risk of falling, multifactorial interventions in the community, including an individually prescribed exercise program and advice on safety, should be provided
Knowledge
Verehyden et al. 2013
B*
For stroke survivors, psychological strategies (e.g. motivational interviewing) may be used to prevent depression
Behaviour change
Hackett et al., 2008
B*
A community continence management plan should be developed with the stroke survivor and family/carer prior to discharge and should include information on accessing continence resources and appropriate review in the community
Shared decision-making and resource utilisation
Thomas et al., 2008
B*
Stroke survivors and their families/carers should be given information about the availability and potential benefits of a local stroke support group and/or other sources of peer support before leaving hospital and when back in the community
Resource utilisation
Kruithof et al. 2013
B*
Stroke survivorswho are cognitively able and their carers should be made aware of the availability of generic self-management programs before discharge from hospital and be supported to access such programs once they have returned to the community
Resource utilisation and self-management programme
Fryer et al., 2016
B*
Stroke-specific self-management programs may be provided for those who require more specialised programs
Self-management programme
Parke et al., 2015
B*
A collaboratively developed self-management care plan may be used to harness and optimise self-management skills
Self-management programme
Lennon et al., 2013
B*
Relevant members of the interdisciplinary team should provide specific and tailored training for carers/family before the stroke survivor is discharged home
Carer knowledge
Forster et al., 2013
B*
Where appropriate home-based coordinated stroke services are available, early supported discharge services should be offered to stroke patients with mild to moderate disability
Support
Langhorne et al. 2017
B*
Stroke survivors with an identified perceptual impairment and their carer should receive verbal and written information about the impairment and practical advice/strategies to reduce risk (e.g. trips, falls and limb injury) and promote independence
Knowledge
Consensus-based recommendation
C*
To prevent complications related to shoulder subluxation, education and training aboutcorrect manual handling and positioning should be provided to the stroke survivor and their family/carer
Knowledge and carer knowledge
Consensus-based recommendation
C*
Stroke survivors and their families/carers should be provided with information and education about fatigue
Knowledge and carer knowledge
Consensus-base recommendation
C*
For stroke survivors with bowel dysfunction education and careful discharge planning should be provided
Knowledge
Consensus-based recommendation
C*
Any person wishing to drive again after a stroke or TIA should be provided with information about how stroke may affect his/her driving and the requirements and processes for returning to driving
Knowledge
Consensus-based recommendation
C*
Stroke survivors and their partners should be offered written information addressing issues relating to sexual intimacy and sexual dysfunction post-stroke.
Knowledge and carer knowledge
Consensus-based recommendation
C*
All carers involved in feeding patients should receive appropriate training in feeding and swallowing techniques
Carer knowledge
Practice point
C*
If a stroke survivor is discharged with either intermittent or indwelling catheterisation, they and their family/carer will require education about management, where to access supplies and who to contact in case of problems
Knowledge, carer knowledge and resource utilisation
Consensus-based recommendation
C*
Carers should be provided with information about the availability and potential benefits of local stroke support groups and services, at or before the person’s return to the community
Resource utilisation and carer support
Consensus-based recommendation
C*
Where a stroke patient is found to have aphasia, the clinician should:
Knowledge, carer knowledge and shared decision-making
Practice point
C*
This discharge planning process may involve self-management strategies (i.e. information on medications and compliance advice, goals and therapy to continue at home) and an appropriate contact number for any post-discharge queries
Knowledge and partnership with a healthcare professional
Consensus-based recommendation
C*
Carers should be supported to explore and develop problem-solving strategies, coping strategies and stress management techniques
Carer support
Consensus-based recommendation
C*
Where it is the wish of the stroke survivor, carers should be actively involved in the recovery process by assisting with goal setting, therapy sessions, discharge planning and long-term activities
Carer involvement
Consensus-based recommendation
C*
Stroke survivors with cognitive involvement who have difficulties in communication should have input from a suitably trained health professional including family education, supportand counselling as required
Carer knowledge and carer support
Consensus-based
C *
Stroke survivors should be encouraged to continue with active task practice outside of scheduled therapy sessions. This could include strategies such as:
Carer involvement
Consensus-based recommendation
C*
Carers should receive psychosocial support throughout the stroke recovery continuum to ensure carer wellbeing and the sustainability of the care arrangement. Carers should be supported to explore and develop problem-solving strategies, coping strategies and stress management techniques. The care arrangement has a significant impact on the relationship between caregiver and stroke survivor so psychosocial support should also be targeted towards protecting relationships within the stroke survivors support network
Carer support
Consensus-based recommendation
C*
UK 2016
People with stroke with constipation should be offered advice on diet, fluid intake and exercise an education and information for the person with stroke and their family/carers (4.5.1, E)
Knowledge and carer knowledge
NICE, 2007b; Cosgrave et al., 2006; Working Party consensus
A*
People with stroke and their family/carers should receive information and training in mouth care and maintaining good oral hygiene before transfer of their care from hospital (4, 4.11.1, D)
Knowledge and carer knowledge
Brady et al., 2006
A*
People with stroke should be offered falls risk assessment and management as part of their stroke rehabilitation, including training for them and their family/carers in how to get up after a fall. (4.9.3.1, A)
Knowledge and carer knowledge
NICE 2013a; Working Party consensus
A*
A facility that provides treatment for in-patients with stroke should include information, advice and support for people with stroke and their family/carers (2.4.2, K)
Knowledge, support, carer knowledge and carer support
Stroke Unit Trialists’ Collaboration 2013; NICE 2016
A*
People with significant changes in self-esteem, self-efficacy or identity after stroke should be offered information, support and advice and considered for one or more of the following psychological interventions:
Knowledge and support
Kendall et al., 2007; Watkins et al., 2007; De Man-van Ginkel et al., 2010; Jones and Riazi, 2010
A*
People with stroke should be actively involved in their rehabilitation through participating in the process of goal setting unless they choose not to, or are unable to because of the severity of their cognitive or linguistic impairments and being given help to understand the process of goal setting, and to define and articulate their personal goals. (2.10.1, A)
Collaborative goal setting
Malec et al., 1991; Wressle et al., 2002; Stein et al., 2003; Hurn et al., 2006; Levack et al., 2006; Holliday et al., 2007a, b; Working Party consensus
A*
People with stroke should be supported and involved in a self-management approach to their rehabilitation goals. (2.10.1, C)
Collaborative goal setting
Rosewilliams et al., 2011; Sugavanam et al., 2013; Taylor, 2012
A*
People with stroke should be offered self-management support based on self-efficacy, aimed at the knowledge and skills needed to manage life after stroke, with particular attention given to this at reviews and transfers of care. (2.13.1, A)
Self-management programme
Lennon et al., 2013; Parke et al., 2015; Warner et al., 2015; Working Party consensus
A*
As part of their self-management plan, people with stroke should be supported to identify social and leisure activities that they wish to participate in, taking into account their cognitive and practical skills. Healthcare professionals should:
Self-management program and reintegration into the community
Langstaff et al., 2014; Dorstyn et al., 2014; Obembe and Eng, 2015
A*
People with stroke should be helped to develop their own self-management plan. (5, 5.9.1.1, D)
Self-management programme
NICE 2016, Working party consensus
A*
The primary carer(s) of a person with stroke should be offered an educational programme which:
Carer involvement and carer knowledge
Patel et al., 2004; Legg et al., 2011; Forster et al., 2012 Working Party consensus; obligations under the 2014 Care Act
A*
When care is transferred out of hospital to the home or care home setting, the carer of a person with stroke should be offered:
Carer support
Working Party consensus; obligations under the 2014 Care Act
A*
People with stroke who are dependent in personal activities (e.g. dressing and toileting) should be offered a transition package before being transferred home that includes:
Resource utilisation and carer knowledge
Gräsel et al., 2006; Lannin et al., 2007b; Barras et al., 2010
A*
The primary carer(s) of a person with stroke should be provided with the contact details of a named healthcare professional (e.g. a stroke co-ordinator) who can provide further information and advice. (2.16.1, E)
Partnership with a healthcare professional
NICE 2016; Working Party consensus
A*
People with stroke should be provided with the contact details of a named healthcare professional (e.g. a stroke co-ordinator) who can provide further information and advice. (5, 5.9.1.1, C)
Partnership with a healthcare professional
NICE 2016, Working party consensus
A*
People with stroke with continued loss of urinary continence should be offered behavioural interventions such as:
Behaviour change
NICE, 2013c, 2015a
A*
People with or at risk of depression or anxiety after stroke should be offered brief psychological interventions such as motivational interviewing or problem-solving therapy (adapted if necessary for use with people with aphasia or cognitive problems) before considering antidepressant medication. (4, 4.10.1.1, B)
Behaviour change
Hackett et al., 2009a,b; NICE, 2009a; Campbell Burton et al., 2011, Watkins et al., 2011
A*
People with stroke who are discharged from specialist treatment with continuing problems with swallowing food or fluids safely should be trained, or have family/carers trained, in the management of their swallowing difficulty and be regularly reassessed. (Chapter 4, 4.16.1, K)
Knowledge and carer knowledge
NICE, 2006a; Heckert et al., 2009; Drury et al., 2014; Working Party consensus
B*
People who wish to return to work after stroke (paid or unpaid employment) should be advised on the most suitable time and way to return to work, if return is feasible (4.1.4.1, B)
Knowledge
Ntsiea et al. 2015
B*
People with communication problems after stroke should be assessed by a speech and language therapist to diagnose the problem and to explain the nature and implications to the person, their family/carers and the multi-disciplinary team (4.4.1.1, A)
Knowledge and carer knowledge
Brady et al. 2016
B*
People with stroke should be offered, as needed, specific treatments that include:
Self-care and carer knowledge
Walker et al., 2011 Working Party consensus
B*
People with aphasia and low mood after stroke should be considered for individual behavioural therapy, for example, from an assistant psychologist. (4, 4.10.1.1, D)
Behaviour change
Thomas et al., 2013
B*
People with stroke should be supported to set and monitor specific goals for interventions for spasticity using appropriate clinical measures for ease of care, pain and/or range of movement. (4, 4.15.1, B)
Collaborative goal setting
Turner-Stokes et al., 2013; Working Party consensus
B*
If the person with stroke agrees, family/carers should be involved in significant decisions as an additional source of information about the person both clinically and socially (2.16.1, B)
Shared decision-making
Working party consensus
C*
People with stroke should be involved in decisions about transfers of their care if they are able and offered copies of written communication between organisations and teams involved in their care. (2.6.1, B)
Shared decision-making
Asplund et al., 2009; Working Party consensus
C*
People with stroke and their family/carers should be involved in decisions about the transfer of their care out of hospital, and the care that will be provided (2.7.1, F)
Shared decision-making
Working Party consensus
C*
Before the transfer of care for a person with stroke from hospital to home (including a care home) they should be provided with:
Partnership with a healthcare professional and knowledge
Working Party consensus
C*
People with stroke, including those living in care homes, should continue to have access to specialist services after leaving hospital, and should be provided with information about how to contact them (2.7.1, K)
Resource utilisation
Working Party consensus
C*
People with stroke and their family/carers should be offered any practical support necessary to enable participation in service user consultations. (2.8.2, E)
Support
Working Party consensus
C*
Vocational rehabilitation programmes for people after stroke should include:
Problem-solving
Working party consensus
C*
People with swallowing difficulty after stroke should be provided with written guidance for all carers to use when feeding or providing fluids (4, 4.16.1, I)
Carer knowledge
Working party consensus
C*
People who wish to drive after stroke should be informed about eligibility for disabled concessions (e.g. Motability and the Blue Badge scheme). (4, 4.1.3.1, D)
Knowledge
Working Party consensus
C*
People without movement in the affected arm after a stroke should be trained in how to care for their affected arm and monitored for any change. (4.2.1, E)
Knowledge
Working party consensus
C*
People with apraxia after stroke should have the impairment and the impact on function explained to them, their family/carers and the multi-disciplinary team (4, 4.3.2.1, B)
Knowledge and carer knowledge
West et al., 2008; Vanbellingen et al., 2010, 2011
C*
People with impaired attention after stroke should have the impairment explained to them, their family/carers and the multi-disciplinary team (4.3.3.1, C)
Knowledge and carer knowledge
Loetscher and Lincoln, 2013; Working Party consensus
C*
People with an executive disorder after stroke should have the impairment and the impact on function explained to them, their family/carers and the multi-disciplinary team. (4.3.4.1, C)
Knowledge and carer knowledge
Working Party consensus
C*
People with memory impairment after stroke causing difficulties with rehabilitation should have the impairment explained to them, their family/carers and the multi-disciplinary team (4.3.5.1, B)
Knowledge and carer knowledge
Fish et al., 2008; Das Nair and Lincoln 2012; Working Party consensus
C*
People with agnosia after stroke should have the impairment explained to them, their family/carers and the multi-disciplinary team (4.3.6.1, B)
Knowledge and carer knowledge
Working Party consensus
C*
People with impaired awareness to one side after stroke should have the impairment explained to them, their family/carers and the multi-disciplinary team (4.3.7.1, C)
Knowledge and carer knowledge
Working Party consensus
C*
People with aphasia after stroke whose first language is not English should be assessed and provided with information about aphasia and communication practice in their preferred language (4.4.1.1, E)
Knowledge
Working party consensus
C*
People with fatigue after stroke and their family/carers should be given information, reassurance and support to identify their personal indicators and triggers for fatigue and supported to develop strategies to anticipate and manage fatigue (4.6.1, B)
Knowledge and carer knowledge
Working party consensus
C*
The specialist multi-disciplinary team should be involved in making decisions about mental capacity and should provide information and advice to the person with stroke (when appropriate) and their family/carers (4.8.1, B)
Knowledge and carer knowledge
Working party consensus
C*
People with mild or moderate symptoms of psychological distress, depression or anxiety after stroke should be given information, support and advice and considered for one or more of the following interventions:
Knowledge
Working party consensus
C*
People with functional loss in their arm after stroke should have the risk of shoulder pain reduced by ensuring that family/carers handle the affected arm correctly, avoiding mechanical stress and excessive range of movement (4.12.3.1, A)
Carer knowledge
Working party consensus
C*
People with sensory loss after stroke should be trained in how to avoid injury to the affected body parts (4.13.1, B)
Knowledge
Working party consensus
C*
People with altered vision, visual field defects or eye movement disorders after stroke should receive information, support and advice from an orthoptist and/or an ophthalmologist (4.17.1, B)
Knowledge
Working party consensus
C*
Canada 2019a
5.3 (a, v) Healthcare staff, patients and family should be educated to correctly protect, position and handle the involved arm
Knowledge and carer knowledge
Australia 2010
A
The team should promote the practice and transfer of skills gained in therapy into the patient’s daily routine during inpatient stay (3, vii)
Knowledge
UK 2016 Guideline
A
Patients and families should be involved in their management, goal setting and transition planning (4.1, iii, a)
Carer involvement
USA 2010 Guideline
A
Treatment to improve functional communication should include supported conversation techniques for potential communication partners of the person with aphasia (10, vii)
Carer knowledge
Simmons-Mackie et al., 2016
A
6. 3(iv) a. The patient, family and caregiver should be made aware of the patient’s increased risk for falls and given a list of precautions to reduce their risk of falling. b. The patient, family and caregiver should receive skills training to enable them to safely transfer and mobilize the patient (Level B). This should include what to do if a fall occurs and how to get up from a fall (Level C)
Knowledge and carer knowledge
Batchelor et al., 2012
B
People who have experienced a stroke, their families and caregivers should have early and active involvement in the rehabilitation process (2.1, I, e)
Carer involvement
Stroke Unit Trialists’ Collaboration, 2013
B
The decision to proceed with enteral nutrition support, i.e. tube feeding, should be made as early as possible after admission, usually within the first 3 days of admission in collaboration with the patient, family (or substitute decision-maker) and the interdisciplinary team (7.2, iii)
Shared decision-making
Dennis et al., 2005
B
All information intended for patient use should be available in aphasia-friendly formats (10, ix)
Knowledge
UK 2013
C
7.1 (v) Patients, families and caregivers should receive education on swallowing, prevention of aspiration and feeding recommendations
Knowledge and carer knowledge
Carnaby et al., 2006
C
10 (x) Families of persons with aphasia should be engaged in the entire process from screening through intervention, including family education and training in supported communication
Carer involvement
Bradley et al., 2016
C
The patient and family are also included as part of the core team (1.0, I, a)
Carer involvement
USA 2010 Guideline
C
Outpatient and/or in-home rehabilitation services should be provided by specialized interdisciplinary team members as appropriate to patient needs and in consultation with the patient and family (4.1, ii)
Shared decision-making
Lincoln et al., 2004
C
The choice of setting for outpatient and/or in-home rehabilitation service delivery should be based on patient functional rehabilitation needs, participation-related goals, availability of family/social support, patient and family preferences (4.1, iii)
Shared decision-making
Hiller and Inglis-Jassiem, 2010
C
Canada 2019b
2.0 Education for people with stroke, their families and caregivers, is an integral part of stroke care that should be included as part of all healthcare encounters, and during transitions
Knowledge and carer involvement
Forster et al., 2012
A
4.2 (iii) People with stroke should be encouraged to participate in evidence-based community exercise programs as appropriate
Reintegration into the community
Dorstyn et al. 2014
A
2.2 (vii) Family and caregiver education, hands-on training and skills development should be provided using an interdisciplinary approach based on the individual’s learning needs
Carer knowledge
Kalra et al. 2004
A
4.5 (iii) People with stroke who experience difficulty engaging in leisure and other social activities should receive targeted therapeutic interventions and individualized plans for participation based on collaborative goal-setting with their healthcare team
Collaborative goal setting and reintegration into the community
UK 2016
A
2.2 (ii) It is recommended that the individualized education plan:
Knowledge, shared decision-making and carer involvement
Eames et al. 2013
A
Persons with stroke, their families and caregivers, should be assessed and prepared for transitions between care stages and settings through information sharing, provision of education, skills training, psychosocial support, awareness of and assistance in accessing community services and resources
Knowledge, support and resource utilisation
Gallacher et al., 2013
B
1.2 (i) Support should be initiated from the onset of stroke and continue throughout all transitions and stages of care
Support
Cameron et al., 2013, Cameron et al., 2014
B
1.2 (ii) The use of telemedicine (e.g. video and web-based technologies and services such as web-based support groups and tele-rehabilitation), should be considered to increase access to ongoing support services, healthcare services and rehabilitation therapies following transitions to the community; especially in settings where people with stroke and their family members are unable to travel to access care and services
Resource utilisation
Chen et al., 2016, Laver et al., 2013, Chumbler et al., 2012, 2015
B
2.2 (v) Include reinforcement of information that has not been retained (e.g. medication information and management)
Knowledge
Eames et al., 2013
B
2.2 (vi) Education and information for people with stroke, family and caregivers should be provided both formally and informally in individual and group settings as appropriate
Knowledge and carer knowledge
Lennon et al., 2013, Eames et al., 2013
B
2.3 (i) Self-efficacy can be supported by providing opportunities to learn and master self-management skills
Self-efficacy
Lennon et al., 2013, Forster et al., 2007
B
2.3 (iv) People with stroke, their families and caregivers should be provided with resources and information which will enable self-management and the ability to navigate through the healthcare and social system
Knowledge and resource utilisation
Lennon et al., 2013, Forster et al., 2007
B
3.2 (ii) A transition planning process should be established as a well-organized collaboration between health professionals, the person with stroke, their family and caregivers
Shared decision-making
Bradley et al., 2016, Sulch et al., 2000, Shyu et al., 2008
B
3.2 (iii, a) The following should be considered throughout transition planning: Formulation of a goal-oriented transition plan (e.g. discharge date) with the person with stroke, family and caregivers
Shared decision-making
Sulch et al., 2000, 2002a, 2002b
B
3.2 (iv, b) Caregiver skills training specific to the current and ongoing needs of the person with stroke
Carer knowledge
Grasel et al., 2005
B
3.2 (iv, d) Written discharge instructions as a component of an individualized care plan that addresses the following issues as appropriate: functional ability at the time of discharge, risks and safety considerations, action plans for recovery, medications at discharge and instructions for adjustment, follow-up care, follow-up care provider contact information and information for one point of contact post-discharge
Partnership with a healthcare professional and knowledge
Australian 2017, UK 2016, Andrew et al., 2018
B
4.0 People with stroke, their families and caregivers should be provided with information, education, training, support and access to services throughout transitions to the community to optimize the return to life roles, activities and social participation
Knowledge and reintegration into the community
Dorstyn et al., 2014
B
4.6 (i) People with stroke, their family and caregivers should be educated and counselled on the potential impact of stroke on relationships
Knowledge and carer knowledge
Song et al., 2011
B
2.3 (ii) With consent, family members and caregivers may be invited and encouraged to attend care and therapy sessions and given the opportunity to learn proper skills to support self-management
Carer involvement
Huijbregts et al., 2008
C
4.4 (ii) Encourage resumption of vocational interests where possible. A gradual resumption could occur when appropriate
Reintegration into the community
Baldwin and Brusco 2011
C
4.4 (v, a) A designated member of the care team may provide counselling and information on employment benefits and legal rights to people who have had a stroke
Knowledge
Baldwin and Brusco 2011
C
4.4 (vi, a) With consent and where possible, the healthcare team may work with employers/educators to devise an appropriate return to work/school plan. Encourage employers and education providers to follow therapists’ recommendations with regards to work/school modifications and provide the flexibility to allow a return to work/school at an appropriate pace
Reintegration into the community
Baldwin and Brusco 2011, Ntsiea et al., 2014
C
4.5 (iv) People with stroke may ideally be provided with information and/or referral to community-based resources for engagement and self-management for ongoing physical, social, emotional, intellectual and spiritual activities and participation in the community
Resource utilisation, knowledge and reintegration into the community
Walker et al., 2004, Desrosier et al., 2007, Dorstyn et al., 2014
C
4.6 (ii, c) Consider providing verbal and written information adapted according to a person’s cognitive or communication abilities or deficits (regarding relationships and sexuality)
Knowledge
Guo et al., 2015
C
4.6 (iii) Education sessions for people with stroke and/or partners may address expected changes in intimacy and sexuality, strategies to maximize sexual function and frequently asked questions regarding relationships following a stroke
Knowledge and carer knowledge
Guo et al., 2015; Song et al., 2011
C
5.2 (iii) Residents in long-term care should have access to exercise, leisure opportunities and support to engage in personally valued activities
Reintegration into the community and support
Brajkovic et al., 2009
C
2.1 (iii) People with stroke, their families and caregivers should be provided with information about peer support groups in their community where available, descriptions of the services and benefits they offer, and be encouraged to consider participation
Resource utilisation
Cadilhac et al., 2011
C