
Abstract
Introduction:
Telerehabilitation is a tool for patients who, for different reasons, cannot participate in person with their physical presence. We aimed to identify the factors associated with satisfaction with telerehabilitation in families with children with neurodevelopmental disorders through a program that included physiotherapy, occupational therapy, and speech therapy.
Methods:
The program was developed during the COVID-19 lockdown period. Outcome measures: Child's age, the school stage to which they belonged, the person of reference in their daily care at home. The resources provided to the families, as well as the frequency of activities and difficulties detected, were evaluated through a survey.
Findings:
One hundred thirteen families responded to the survey. The general assessment resources were classified as very good. The average frequency of carrying out the activities was two times a week, with an average of 30 minutes per session. The ability to understand the information in the manual was not affected by the academic status of the caregivers (p = 0.286).
Conclusions:
This is the first study to quantify the multidisciplinary approach to children with neurodevelopmental disorders using telerehabilitation. The results show high levels of participation and satisfaction. The resources could be shared for their applicability in other countries whose families have similar needs conditioned by COVID-19.
Introduction
During the pandemic of COVID-19, every day we have had huge challenges in the health system with sobering realities in economics, medical, and political attention in our society (Wu et al., 2020). The global pandemic has driven both the medical community and society toward the digital practice of telehealth. Considering the uncertainty with COVID-19 and due to measures recommended by different organizations, rehabilitation professionals have had to differently adapt their therapeutic approaches. This new approach put in place since the beginning of the period of confinement has generated a profound rehabilitation in patient care (Barker-Davies et al., 2020). This unique situation has given rise to new challenges and opportunities in digital practice, since professionals may lack necessary telehealth skills (Barker-Davies et al., 2020; Khan and Amatya, 2020). Therefore, it is especially important to consider key recommendations for the development of this digital practice to make it safe and effective. Recent publications have presented a general classification of telehealth strategies according to the complexity of the technology from low-tech strategies (e.g. phone calls and videos/photos), to more technologically improved strategies that can offer personalized and specialized interventions (Camden and Silva, 2021).
Telerehabilitation has developed from parent disciplines of telemedicine and telehealth, providing a clear relationship to the field of telecare, suggesting that it faces different unique challenges of the concepts of medicine and health that address wider issues (van Houwelingen et al., 2016). It has been used to describe the provision of rehabilitation services from a distance, using communication technology (van Houwelingen et al., 2016) and as the clinical application of consultations, preventive actions, diagnosis, and therapy with audio-visual links and components (Pastora-Bernal et al., 2018; Sharma et al., 2019).
Telemedicine holds the promise to improve quality, increase patient access, and reduce healthcare costs. In addition, recent advances in telecommunication technologies have promoted the possibility of carrying out rehabilitation processes through the Internet. Studies suggest that increasing the intensity provided by telerehabilitation is a promising option to be offered to patients. (Agostini et al., 2015)
Current evidence supports our opinion that telerehabilitation is as effective as face-to-face rehabilitation in terms of evaluation (Cottrell et al., 2017, 2018), pain management (Cottrell et al., 2017, 2018), improved functionality (Rawstorn et al., 2016; Shukla et al., 2017), and health education (Hanlon et al., 2017).
The sudden and unexpected changes induced by the lockdown are likely to create new difficulties and needs for children with disabilities and their parents (Cacioppo et al., 2021). The hypothetical general impairment that children with disabilities may experience and the influence on their families has become a common concern in the medical community, especially in relation to the fundamental role that rehabilitation medicine should offer (Carda et al., 2020; Leochico, 2020).
The pandemic is likely to have a large impact on the health of these children, including their physical, mental, and social wellbeing as defined by the WHO in the International Classification of Functioning (Cacioppo et al., 2021).
With the pandemic caused by COVID19, the great need has arisen to maintain remote care for children with disabilities. Evidence suggests many applications in which telehealth can adequately replace traditional in-person visits, and there are many potential applications of telehealth to explore as a means of improving interdisciplinary rehabilitation team connectivity and outreach to pediatric patients (Camden and Silva, 2021; Curfman et al., 2021; Dietzen et al., 2020; Hsu et al., 2021; Maresca et al., 2020; Tenforde et al., 2020).
Although telerehabilitation has long been recognized as a promising means of providing rehabilitation therapy, the use of remote devices for rehabilitation in children was limited before the COVID-19 pandemic, due to culture, technology access, regulatory, and reimbursement barriers (Dorsey and Topol, 2016; Tomines, 2019). Considering the expansion of pediatric telehealth, a survey administered by the Supporting Pediatrics Research on Outcomes and Utilization of Telehealth program with 56 responses from mostly academic medical centers using pediatric telehealth-identified barriers including licensing requirements, provider interest, and limitations of training resources (Wang et al., 2020).
In our study, the recommended practices have been developed by professionals from all fields. Furthermore, the scientific evidence establishes a focus of the intervention to be the active participation of the patient through his motivations and interests, the management of environmental factors, and family training.
The purpose of the study is to evaluate the telerehabilitation program satisfaction, on the treatment of children with disabilities from different areas of rehabilitation, given the impossibility of offering them face-to-face treatment due to the pandemic situation. In addition, as secondary objectives, we have set ourselves to know the degree of compliance with the program and the possible difficulties that may arise to families.
The research questions were:
As is being done in other disciplines, is it possible to develop a telerehabilitation program for the pediatric population with neurodevelopmental disorders?
What factors influence the telerehabilitation program to develop optimally?
Are the families compliant with this kind of intervention?
Method
Design
A prospective longitudinal observational study was carried out following the STROBE guidelines (Cuschieri, 2019). It was developed in the Ciudad San Juan de Dios healthcare center, which corresponds to a care center for people with disabilities located in Las Palmas de Gran Canaria, Spain. The intervention, monitoring, and evaluation were carried out between March 13, 2020 (beginning of the lockdown period decreed by the Government of Spain) and June 15, 2020, the date on which the data collection was carried out. As of this date, therapeutic assistance began in person in a gradual manner at the Reference Center.
Participants
The intervention and follow-up were carried out with 142 children with neurodevelopmental disorders and their families. Inclusion criteria were belonging to the Centre of the Ciudad de San Juan de Dios in Las Palmas de Gran Canaria, availability of Smartphone with the applications “Zoom” and “WhatsApp.” Each family gave their consent to participate in the study through a form with a digital signature.
The age group to participate in the study included people from 1 to 21 years old. Given the characteristics of the Center (school for children with disabilities), the age groups are distributed by stages: Infant school (from 0 to 3 years old), First cycle (from 3 to 6 years old), Second cycle (from 6 to 15 years), Cycle Transit to adult life (from 15 to 18 years), Day Center (from 18 to 21 years), Ambulatory (from 6 to 15 years). In pre-pandemic conditions, the children who are part of the group known as “Ambulatory” are those who receive their school education at another school and go to the center only for rehabilitation treatment.
The functional status of the children was around a grade III and V with respect to the Gross Motor Function Measure (Ferre-Fernández et al., 2020). The diagnosis of the children who participated in the study corresponded to cerebral palsy (86.6%) and neurodevelopmental disorders related to metabolic disorders and movement disorders (13.4%).
Because the intervention and evaluation would be carried out only with the users of the Reference Center, the sample was obtained through non-probabilistic convenience sampling.
Intervention
Telerehabilitation program was implemented through the Zoom platform, connecting each family individually once a week. Through the camera they were advised, guided, and corrected on different therapeutic approaches. During the received sessions, the families were asked to show the tasks to ensure their correct execution. Given that the study was carried out during the stage of lockdown (only leaving the home for basic needs was authorized: doctor, pharmacy, and supermarket), the relatives were always with the child, which allowed him to interact and comply with the program with longer duration than in pre-pandemic conditions.
Furthermore, interdisciplinary meetings were held weekly with each of the therapists who were treating the same child along with virtual meetings with their families. Previously, each teacher of the child had had a tutorial in which they were informed and trained in the use of the videoconferencing tool. The teacher, the physiotherapist, the occupational therapist, the speech therapist, and the child’s family participated in all the multidisciplinary meetings. In addition, in each weekly individualized sessions that were carried out directly with the child, the family and each professional of the rehabilitation team spent 1 hour per teleconference session.
Therefore, each intervention session consisted of 1 hour of video conferencing with each professional (three individual sessions per week). A weekly distribution schedule had been previously provided to each family, which was agreed upon by both parties. Each session was structured in the same way: first, personal aspects and possible doubts from the previous session were discussed. Then a specific management proposal was made oriented to a task, game, and the child’s participation. The session ended by setting the guideline to follow using the manual as a guide, thus allowing them to remember it in a simpler way. Since the program was developed over 13 weeks, the total number of sessions (video conference) for each participant was 39 sessions.
The specific manual has been generated with recommended activities from the area of Physiotherapy, Occupational Therapy Speech therapy, according to the potential of each child. The contents of the manuals were prepared strictly focused on evidence-based medicine, as well as on the idea of family-centered rehabilitation therapy (Elangkovan and Shorey, 2020; Kim et al., 2021; McCoy et al., 2020; van Balen et al., 2019). Each manual was sent individually to each family in digital format. For its correct use and understanding, according to the guidelines to be followed, in the first videoconference sessions, time was dedicated to answering questions and teaching in real time with their children the handling guidelines that were included. In addition, during one of the sessions scheduled each week, the family was asked to demonstrate the proposed activities in order to make possible suggestions or corrections. With this action, even if the same family member was not present in the different sessions, mainly for work reasons, it did not allow us to ensure that the communication was similar for the whole family. The skills of both the main caregivers and siblings who might have a degree of involvement in the management of the participant were evaluated. To access the manuals, you can download it through the Supplemental Material.
Ethical and regulatory considerations
This study was conducted according to current Spanish legislation Organic Law 3/2018, of 5 December, Protection of Personal Data and guarantee of digital rights (Jefatura del Estado, 2018) and the Law 14/2007, of 3 July, on Biomedical Research (Jefatura del Estado, 2007). It was carried out according to the indications of the local Ethics Committee on Research with Humans. All participants previously signed an informed consent according to the bases established by the laws.
Analysis
The variables that were evaluated to describe the sample corresponded to the child’s age, the school stage to which he or she belonged, the person of reference in their daily care at home and the level of education of that person. It also included a survey about the satisfaction of the rehabilitation program, where a general evaluation of the attention of the Rehabilitation Service during the hospitalization period was analyzed, in relation to the consultations and support provided and the perception of different individual aspects in physiotherapy, speech therapy, and occupational therapy manuals. In relation to the degree of general satisfaction, the scores ranged from 1 (insufficient) to 5 (very good).
In addition, they were asked if they encountered any difficulties in completing the activities marked in relation to the time available, the space and the material they had, as well as understanding the objective of the tasks. It was evaluated from 1 to 5, according to the degree of difficulty under different aspects, so that 1 represented low difficulty, and 5 great difficulties. On the other hand, a record was made of the time when the activities were carried out and the weekly frequency.
To carry out the data collection, a self-prepared online survey was created through the Google Forms application, to be as accessible and practical as possible to families. Because the communication route was made through the WhatsApp mobile application, the parent or tutor’s consent was sought before starting the questionnaire.
To obtain the greatest number of responses, the link giving access to the survey was available for 2 weeks. In addition, they were asked if they had any kind of difficulty in accessing the program or the format itself when using it on their mobile phones. They were also offered the option of receiving the link via email. All families were contacted individually to make sure the information was received successfully. For more details, all questions and responses to the survey (Spanish) are available at https://forms.gle/AaZ7biwWBGEwAwB69. As Supplemental Material we have included the survey in English.
Statistical analysis
Statistical analysis of data was performed by the IBM SPSS Statistics 27 (IBM Corp. Released, 2020). . Categorical variables were summarized using frequencies and percentages. Numerical variables were summarized using the mean and the standard deviation (SD). To analyze the samples’ normality, the Kolmogorov-Smirnov was used. To analyze the correlation between two ordinal variables, the Spearman’s rho coefficient test was used. To compare more than two independent samples, in the absence of normality, the non-parametric Kruskal-Wallis test was used. The results were considered statistically significative if p < 0.05.
Results
The survey was sent to 142 families, of which 79.6% (approximately 80%) responded, obtaining a sample of 113 (n = 113). The general description of the participants can be seen in Table 1.
Baseline characteristics of participants.

To respond to the main objective of the study, we evaluated the families’ degree of satisfaction in reference to the care provided and the guidelines manual they received. Taking as positive values those who answered from “good” to “excellent,” the following were rated within that range: The general performance of the Rehabilitation Service (68%, 78 respondents), the accessibility to the information they requested (73%, 85 respondents) and the degree of satisfaction with the reply to queries (75%, 85 respondents). The results obtained in the survey, according to the type of question, are expressed in Table 2. In addition to the general assessment of the Rehabilitation Service, the score obtained is individually expressed in each of the manuals according to the field (physiotherapy, speech therapy, and occupational therapy).
Outcomes obtained in the satisfaction survey.
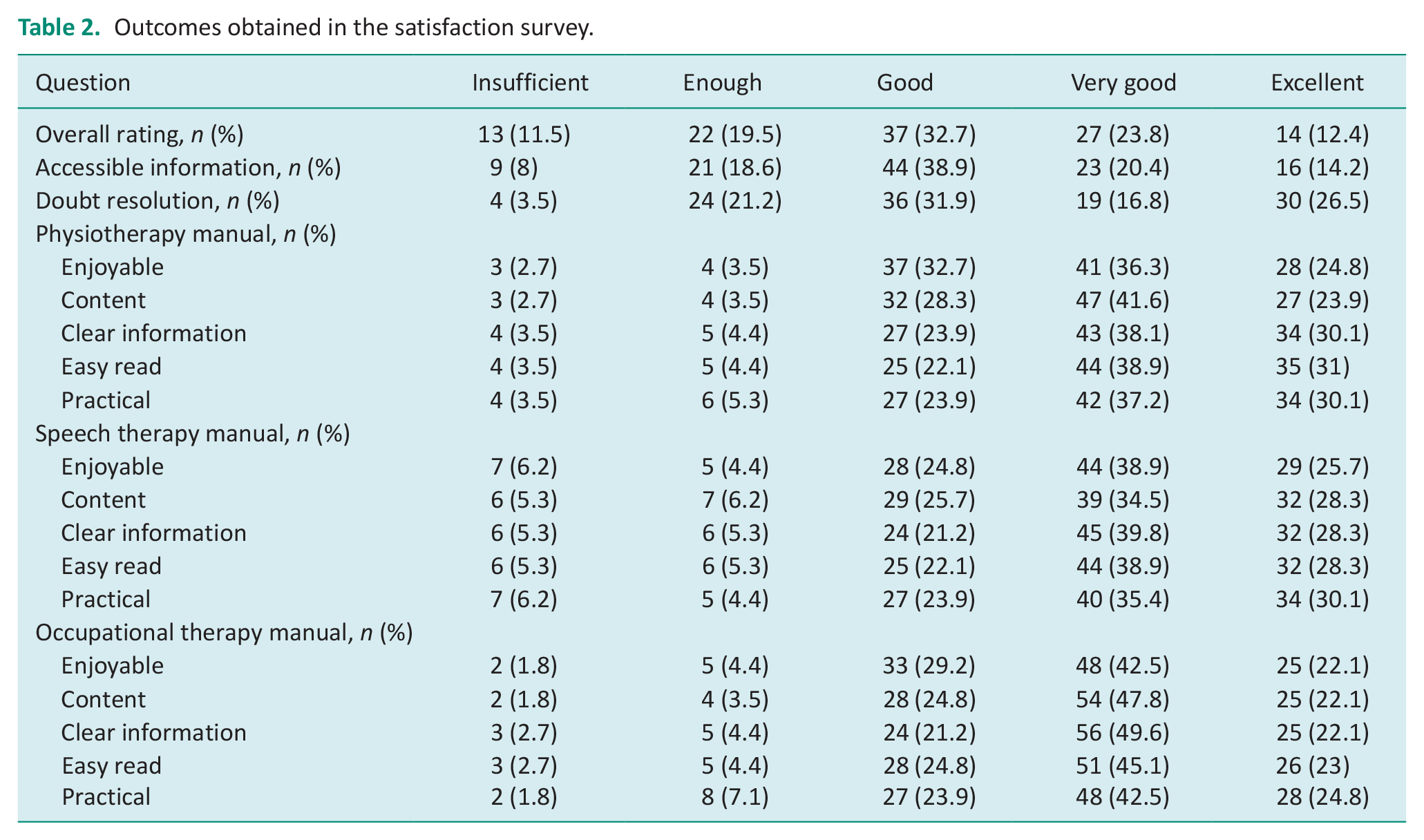
Considering that the score ranged from 5 (very good) to 1 (insufficient), we can affirm that the average global score can be classified as good. The score regarding the information provided and the average assessment in the resolution of doubts was good (3.06 ± 1.18), regarding the information provided, the mean score was good (3.14 ± 1.12), and (3.42 ± 1.19) in relation to queries resolved.
In the analyzed sample, the predominant frequency of activity was two times a week corresponding to 45% (51 cases) of caregivers who perform the recommended activities with children. Furthermore, 74% of the caregivers performed 30 minutes of activity per session. In relation to the time available, 42 (37.1%) of caregivers were employed through teleworking. However, in the families in which both parents continued to work, in all cases they reported that they always arranged for one of them to be with their child.
In relation to the possible difficulties that the families could find, they were asked to evaluate the degree of difficulty they found with respect to different factors, with 1 being no difficulty the lowest score, and 5 the greatest difficulty. The means and SDs found were 2.38 (1.33) in relation to the space to perform the tasks, 2.57 (1.25) in terms of time spent, 2.74 (1.32) regarding the necessary material, and 2.04 (1.15) in reference to the understanding of the contents.
When analyzing a possible relationship between the academic level and the degree of difficulty understanding the manual, no statistically significant differences were found (Kruskal–Wallis H = 1.854; p = 0.603). Although a significant correlation between the two ordinal variables is not detected (Spearman’s rho = −0.101; p = 0.289), the negative sign of the coefficient allows us to appreciate that, the higher the academic level, the lower the degree of difficulty in understanding the manual. The results expressed in Table 3 show the observed and expected frequencies, and the percentage of cases, according to the degree of difficulty, for each academic level.
Cross-table of variables academic level and degree of difficulty to understand the manual.

Discussion
The general evaluations of the physiotherapy, speech therapy, and occupational therapy manuals have been rated with very high marks by families: the type of content, the clarity of the information, the practical level and, very importantly, the fun factor.
It was observed that the comprehension of the information was not associated with the academic level of the caregiver. In addition, the overall assessment of the Rehabilitation Service during confinement has been rated as good.
Regarding involvement by families, it was observed that the most common trend was to carry out two sessions per week, with an average duration of 30 minutes per session.
Regarding technological use, and even though videoconferences are very common communication tools, there can be technical problems (disconnection, device failures) and technological difficulties. However, collaborators are available to offer technical support to patients by phone or email, without the need to visit the patient at home to install or verify any hardware.
The results of the studies show that patients are able to adhere to telerehabilitation and that they are able to maintain a good relationship with their therapist, even when direct interaction is not taking place (patient and therapist in the same geographical location) (Cabana et al., 2016). Our study confirms this. In addition, this method of interaction facilitates daily life, and it does not require the patient to move to receive treatment. By being at home, the patient’s motivation increases, and he feels more independent in his exercises. With the return to face-to-face activity, we believe that it can be a very useful tool to empower families and continue treatment outside of the medical consultation (Kalleson et al., 2019, 2021; Pierce et al., 2021). Similar findings were concluded by Pinnock and colleagues who suggested that the perceived benefits of telephone-based care compared to face-to-face consultation resulted in a recommendation that asthmatic patients in general practice should be offered a choice of consultation (Pinnock et al., 2005).
The usual care of children with special needs has become even more challenging during the COVID-19 lockdown, since parents found themselves involved throughout the whole day and often without the support of educational and rehabilitation services. To mitigate the feeling of being alone in direct caregiving of children with disabilities, we have developed potentially effective strategies to support the families of children with disabilities using telemedicine approaches. In addition to other similar studies (Ben-Pazi et al., 2020; Bican et al., (n.d.); Frigerio et al., 2022), a specific transdisciplinary manual was prepared. The purpose was only to serve as a support for those moments when the videoconference sessions were not being held, but also to provide material in different languages to be shared with society.
This experience has allowed us to gain more information about the potentiality of telerehabilitation and resulted in an excellent level of satisfaction of the caregivers. With appropriate education and consistent models of care, an increased use of telehealth may provide advances in remote patient care (Frigerio et al., 2022). We consider that, despite the return to face-to-face activity, it should be a resource to continue to be used to enhance family-based care, empower families, and increase the level of participation of children with disabilities.
On the other hand, other studies show that telerehabilitation may be comparable to in-person rehabilitation or better than no rehabilitation for conditions such as osteoarthritis, low back pain, hip and knee replacement, and multiple sclerosis, and also in the context of cardiac and pulmonary rehabilitation (Seron et al., 2021).
Some researches have been published including surveys and assessments of telerehabilitation needs for different patient groups and geographic settings internationally (Bennell et al., 2020; Rush et al., 2018). We also find in current literature studies evaluating patient satisfaction with telerehabilitation intervention, results that are generally positive and satisfactory (Moffet et al., 2017). The assessment of the patient’s needs and knowledge of their level of satisfaction are pillars on which the identification of the level of quality of healthcare is based.
In addition, telerehabilitation meets the expectations of patients and their satisfaction; this is especially true when carried out as a teleconsultation, because the feeling of daily presence is rewarded (Donaghy et al., 2019; O’Brien et al., 2018).
There are studies that have explored the impact of the COVID-19 pandemic on the practice of therapists, on mental health and the use of telerehabilitation strategies by therapists during the period of confinement (Dogruoz Karatekin et al., 2021; Ganesan et al., 2021). As healthcare personnel who have a close bond with the patient, we believe that telehealth-related tools have made it easier to reduce uncertainty about the status of our patients. Findings from other study groups suggest that the implementation of telehealth physical therapy during the COVID-19 pandemic was feasible and acceptable in this setting. Additionally, they promote this type of practice to guide future health policy, quality improvement, and scientific implementation initiatives to expand its use (Miller et al., 2021).
Regarding the limitations of the study, perhaps the technological barrier has possibly represented the main obstacle. Given the circumstances, there was no room for improvement in the quality of the families’ Internet connection, as well as the difference in the management skills of information technologies. Another possible limitation, related to not attending, is the ability to accurately interpret and execute what was tried to be recommended, as well as the possession of specific material that is sometimes used during treatment sessions. In our research we dedicated part of the sessions to adapting the proposed tasks with the material they had available. In most cases, it meant greater dedication of the available time but sometimes the proposed objectives of the session could not be met.
In addition, although the evaluation did not reflect it, in future interventions in other countries the available space could generate some difficulty. Perhaps it is a concern in which we agree with the study carried out by Pastora-Bernal et al. (Pastora-Bernal et al., 2018) identifying the lack of in-person interaction, technical problems, and the low quality of attention perception as the main concerns of patients with the telerehabilitation program. When it comes to caring for pediatric patients, most of whom depend on the caregiver, it was more difficult for us to interact in a clearer and more direct way, since we had to adapt at all times to the patient’s needs.
It is true that there are studies that speak of a dependence on the level of digital literacy of the patient, as well as their technological availability (Scott Kruse et al., 2018). Therefore, in this type of patient, we believe that we must be as precise as possible in the indications that we give to caregivers, and always adapted to each situation and characteristics of the caregiver and patient. Being in a lockdown situation, and that the main caregiver in most cases did not work or did telework, we could count on their full availability. However, in the current situation, we understand that there could be a decrease in the level of participation, involvement, and availability on their part.
Moreover, due to the nature of the survey dissemination, the data comes from a convenience sample and may not be representative of the field.
On the other hand, there are authors who establish as key aspects the adjustment to the treatment routine, the privacy of the data, as well as the lack of regulation in the handling of data (Hinman et al., 2017).
Conclusion
The response obtained in general has been satisfactory. The pandemic situation requires quick measures to try to cover most of the needs of families with children with impaired neurodevelopment, therefore we believe that a rehabilitative approach that integrates physical therapy, speech therapy, and occupational therapy of these characteristics is very important to be able to share it with other families from other parts of the world.
Key findings
Satisfaction with telerehabilitation was evaluated jointly between physical therapy, occupational therapy, and speech therapy.
The level of digital literacy of families, as well as their technological availability, is essential in a lockdown situation.
The pandemic situation requires rapid measures to try to cover most of the needs of families with children with neurodevelopmental disorders.
The majority trend of families when developing the rehabilitation program was two sessions per week, with an average duration of 30 minutes per session.
What the study has added
With the onset of the pandemic, a fundamental need has arisen to continue caring for the children we treat on a daily basis. The confinement situation imposed by the health authorities has generated an important change in our lives and, possibly, to a greater extent, in those families who must care for people with disabilities.
For this reason, we have developed various resources to try that families can continue to adopt to a certain extent for the process of rehabilitation of their children. In addition, the proposal that we send you is aimed at sharing our work with the whole world, and perhaps with the possibility of helping families in those countries where currently the COVID-19 has generated a greater need.
Supplemental Material
sj-pdf-1-bjo-10.1177_03080226221141322 – Supplemental material for Implementation of a telerehabilitation program for children with neurodevelopmental disorders during the lockdown caused by COVID-19
Supplemental material, sj-pdf-1-bjo-10.1177_03080226221141322 for Implementation of a telerehabilitation program for children with neurodevelopmental disorders during the lockdown caused by COVID-19 by Aníbal Báez-Suárez, Iraya Padrón-Rodriguez, Debora Santana-Cardeñosa, Lara Santana-Perez, Victoria Maria Lopez-Herrera and Romina Pestana-Miranda in British Journal of Occupational Therapy
Supplemental Material
sj-pdf-2-bjo-10.1177_03080226221141322 – Supplemental material for Implementation of a telerehabilitation program for children with neurodevelopmental disorders during the lockdown caused by COVID-19
Supplemental material, sj-pdf-2-bjo-10.1177_03080226221141322 for Implementation of a telerehabilitation program for children with neurodevelopmental disorders during the lockdown caused by COVID-19 by Aníbal Báez-Suárez, Iraya Padrón-Rodriguez, Debora Santana-Cardeñosa, Lara Santana-Perez, Victoria Maria Lopez-Herrera and Romina Pestana-Miranda in British Journal of Occupational Therapy
Supplemental Material
sj-pdf-3-bjo-10.1177_03080226221141322 – Supplemental material for Implementation of a telerehabilitation program for children with neurodevelopmental disorders during the lockdown caused by COVID-19
Supplemental material, sj-pdf-3-bjo-10.1177_03080226221141322 for Implementation of a telerehabilitation program for children with neurodevelopmental disorders during the lockdown caused by COVID-19 by Aníbal Báez-Suárez, Iraya Padrón-Rodriguez, Debora Santana-Cardeñosa, Lara Santana-Perez, Victoria Maria Lopez-Herrera and Romina Pestana-Miranda in British Journal of Occupational Therapy
Supplemental Material
sj-pdf-4-bjo-10.1177_03080226221141322 – Supplemental material for Implementation of a telerehabilitation program for children with neurodevelopmental disorders during the lockdown caused by COVID-19
Supplemental material, sj-pdf-4-bjo-10.1177_03080226221141322 for Implementation of a telerehabilitation program for children with neurodevelopmental disorders during the lockdown caused by COVID-19 by Aníbal Báez-Suárez, Iraya Padrón-Rodriguez, Debora Santana-Cardeñosa, Lara Santana-Perez, Victoria Maria Lopez-Herrera and Romina Pestana-Miranda in British Journal of Occupational Therapy
Supplemental Material
sj-pdf-5-bjo-10.1177_03080226221141322 – Supplemental material for Implementation of a telerehabilitation program for children with neurodevelopmental disorders during the lockdown caused by COVID-19
Supplemental material, sj-pdf-5-bjo-10.1177_03080226221141322 for Implementation of a telerehabilitation program for children with neurodevelopmental disorders during the lockdown caused by COVID-19 by Aníbal Báez-Suárez, Iraya Padrón-Rodriguez, Debora Santana-Cardeñosa, Lara Santana-Perez, Victoria Maria Lopez-Herrera and Romina Pestana-Miranda in British Journal of Occupational Therapy
Supplemental Material
sj-pdf-6-bjo-10.1177_03080226221141322 – Supplemental material for Implementation of a telerehabilitation program for children with neurodevelopmental disorders during the lockdown caused by COVID-19
Supplemental material, sj-pdf-6-bjo-10.1177_03080226221141322 for Implementation of a telerehabilitation program for children with neurodevelopmental disorders during the lockdown caused by COVID-19 by Aníbal Báez-Suárez, Iraya Padrón-Rodriguez, Debora Santana-Cardeñosa, Lara Santana-Perez, Victoria Maria Lopez-Herrera and Romina Pestana-Miranda in British Journal of Occupational Therapy
Supplemental Material
sj-pdf-7-bjo-10.1177_03080226221141322 – Supplemental material for Implementation of a telerehabilitation program for children with neurodevelopmental disorders during the lockdown caused by COVID-19
Supplemental material, sj-pdf-7-bjo-10.1177_03080226221141322 for Implementation of a telerehabilitation program for children with neurodevelopmental disorders during the lockdown caused by COVID-19 by Aníbal Báez-Suárez, Iraya Padrón-Rodriguez, Debora Santana-Cardeñosa, Lara Santana-Perez, Victoria Maria Lopez-Herrera and Romina Pestana-Miranda in British Journal of Occupational Therapy
Footnotes
Acknowledgements
We are grateful to all the workers of the Order of Saint John of God, and especially to then children and their families who have participated.
Research ethics
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. This is an observational study. The Saint John of God Hospital Research Ethics Committee has confirmed that no ethical approval is required.
Patient and public involvement data
During the development, progress, and reporting of the submitted research, Patient and Public Involvement in the research was: included in the reporting of the research.
Consent to participate
Written informed consent was obtained from all individual participants included in the study.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Contributorship
All authors (ABS, IPR, DSC, LSP, VLH, RPM) developed the project. ABS and RPM led the project. IPR performed the analyses and wrote the first draft of the article. All authors (ABS, IPR, DSC, LSP, VLH. RPM) critically reviewed and approved the final manuscript.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.