
Abstract
Introduction:
This study aims to explore the effectiveness of the Seniors’ Eye Rehabilitation (SEER) pilot programme, a visual rehabilitation home therapy by specialised low vision occupational therapists (LVOT).
Method:
This was an interventional, longitudinal cohort study. Participants were recruited from Singapore National Eye Centre Low Vision Clinic. The occupational therapy interventions include activities of daily living retraining, activities/home modifications, functional/community mobility training and patient/family education. Each participant set two individualised goals (Priority Goal 1 and Priority Goal 2). The Wilcoxon signed-rank test was used to compare baseline and 6-month follow-up scores for Australian Therapy Outcome Measures for Occupational Therapy (AusTOMs-OT) and the Goal Attainment Scale (GAS) (p < 0.05).
Results:
Forty-one participants (mean age: 67, 48.8% male) completed SEER. There was statistically significant reduction in activity limitations (1 median point change (MPC), Z = −4.21, p < 0.01), participation restrictions (1 MPC, Z = −3.951, p < 0.01) and improved well-being (0.5 MPC, Z = −3.668, p < 0.01) for Priority Goal 1 using AUSTOM-OT. With GAS, there was a statistically significant improvement in Priority Goal 1 (1 MPC, Z = −3.886, p < 0.01).
Conclusion:
The SEER programme was found to be effective in improving all domains of the AusTOMs-OT and GAS for Priority Goal 1. This provides evidence that visual rehabilitation home therapy by specialised LVOT is beneficial to older adults with visual impairment.
Keywords
Background of low vision rehabilitation in Singapore
Low vision is a visual impairment that cannot be corrected by regular eyeglasses, contact lenses, medication or surgery, and it interferes with the ability to perform everyday activities (National Eye Institute, 2022). Low vision adversely affects many daily activities, such as telling time, looking for daily items, using a phone, reading a book, managing medications and preparing a meal. A substantial body of literature has demonstrated a strong linear relationship between low vision and the inability to perform activities of daily living (ADL) and instrumental activities of daily living (IADL) in older adults (Mitchell, 2018; Nael, 2017; Servat et al., 2011; Taylor, 2016). The elderly with low vision struggle to maintain participation in important occupations; ultimately, the declining vision compels them to forgo meaningful occupations, reduce physical and social life functions and lose valuable occupational roles (Boey, 2021).
Low vision and blindness accounts for about one-third of the disease burden in Singapore (Singapore Ministry of Health, 2014). Current services are mainly based at the outpatient clinic level at tertiary hospitals. About half of the clients missed their appointments due to lack of caregiver to bring them for appointments or it is too cumbersome for them to come for appointments on their own due to their decreased mobility status secondary to their poor vision (Simon, 2008).
Importantly, the incidence of visual impairment is expected to increase with an ageing population in Singapore (Department of Statistics Singapore, 2015). In three separate local studies, up to 25% of 3269 surveyed Malay adults (Wong et al., 2008) and 3400 Indian adults (Zheng et al., 2011) between 40 and 79 years have bilateral low vision, and an underestimated prevalence of glaucoma in ethnic Chinese was found (Foster et al., 2000). In the Singapore National Eye Centre Low Vision Clinic, the number of new cases has increased from 302 in year 2010 to 387 in 2017.
Currently, low vision conditions are diagnosed in eye clinics within the tertiary hospitals, followed by sessions to manage their eye conditions. Tertiary hospital services locally are inclined towards a specialist approach (Chee, 2004), even though the understanding that managing low vision requires a multidisciplinary, transitional approach is not new (van Nispen, 2020). The limited and fragmented community capacities have resulted in the development of hospital-led multidisciplinary care programmes in Singapore. Three different tertiary hospitals have begun offering outpatient low vision occupational therapy services involving multidisciplinary care since 2011.
Suitable care model – the Seniors’ Eye Rehabilitation programme
In view of a lack of suitable care model in terms of limited post discharge care and in community and lack of transition for patient care from acute to community settings, a low vision home therapy service provided by low vision trained occupational therapists was mooted and piloted. This programme is called the Seniors’ Eye Rehabilitation (SEER) programme.
This SEER programme has a few programme objectives, namely streamline and support existing services in view of overall care fragmentation, reach out to more clients and caregivers to increase their function and quality of life (QoL) and increase capacities of community services in terms of knowledge and skills. It is intended to incorporate the entirety of the client’s journey from diagnosis by ophthalmologists, to visual aids prescription by low vision optometrists, low vision rehabilitation by trained occupational therapists (both in hospitals and community) and case management by a medical social worker (MSW). With this home therapy programme, community-based occupational therapists will take on referrals from acute-based occupational therapists after on the job training and workshops, effectively freeing acute resources and also empowering community-based occupational therapists with valuable clinical know-hows to manage low vision clients. This potentially helps to build capabilities within the community early to tackle the rising numbers of low vision elderly clients as Singapore ages. The flowchart of the SEER programme is shown in Figure 1.
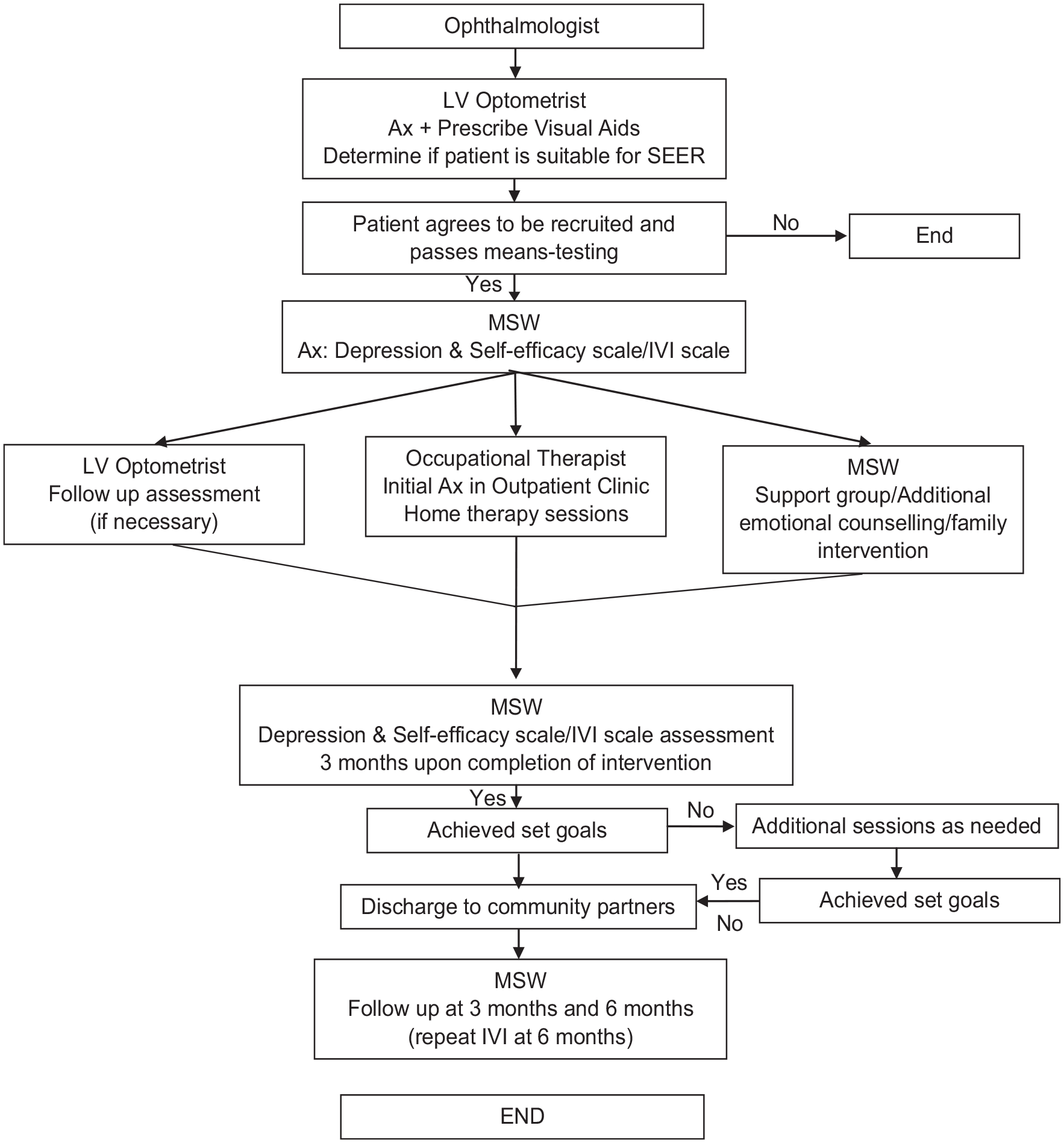
Flowchart of the Seniors’ Eye Rehabilitation (SEER) programme.
This article presents the effectiveness of the pilot low vision home therapy service provided by low vision trained occupational therapists for older adults with low vision.
Method
This programme and study has been approved by the Centralised Institutional Review Board – SingHealth. This study was an interventional, longitudinal cohort study, where the participants were recruited from a single centre based at the Singapore National Eye Centre Low Vision Clinic. The occupational therapy interventions include ADL retraining, activities adaptations, home modifications, functional and community mobility training and patient and family education.
Recruitment
Controlled quota sampling was conducted for this study to gather representative data. After being reviewed by the ophthalmologist and assessed by the optometrist to be suitable for the programme, informed consent and means testing is taken to recruit the participants from 5 October 2016 to 31 December 2017. The recruitment inclusion criteria are:
(1) Participants who are 50 years old and above
(2) Diagnosed as low vision with a visual acuity of 6/18 or worse and or visual field less than central 10°.
Participants who are younger than 50 years old and have a better vision acuity and or visual than the above inclusion criteria are excluded.
Efforts were taken to reduce potential sources of bias. Although blinding of raters and participants and allocation bias were not possible, raters standardised the scoring of the outcome measures by going through the rating guidelines together. Selection bias was also minimised by strictly adhering to the inclusion and exclusion criteria. No sample size calculation was conducted. Our sample size was one of convenience; however, we attempted to follow the general rule of thumb to recruit at least 30 participants (Browne, 1995).
Data collection
Demographics information such as age, gender, occupation and diagnostic group was collected. Each session takes up an hour. Participants are allowed more than five home therapy sessions subjected to the clinical judgement of the low vision trained occupational therapist.
Outcome measures
The Australian Therapy Outcome Measures for Occupational Therapy (AusTOMs-OT) and the Goal Attainment Scale (GAS) were used at the start and the end of the occupational therapy programme. The AusTOMs-OT was developed to measure global therapy outcomes and offers therapists a range of 12 function-focused scales (including self-care, domestic life, community life, upper limb function). Therapists evaluate the client’s status globally in relation to four domains: the underlying impairment, activity limitation, participation restriction and distress/well-being. This measure allows occupational therapists to capture global outcomes across multiple domains in just a few moments. Goals were collaboratively set with occupational therapists, following an initial assessment. Once goals were established, the occupational therapist selected the AusTOMs-OT scales most relevant to the participant’s goals and scored the participant’s current impairments and activity limitations (Smith, 2020). GAS offers a number of potential advantages as an outcome measure for rehabilitation. Given its individualised goal-setting nature, it has a positive therapeutic value in encouraging the patients to reach their goals (Rehabilitation Measures Database, 2020). The occupational therapist defined the outcomes, scored the baseline and then the goal attainment, after establishing an agreed set of priority goals with the participants, in line with their individual aspirations (Turner-Stokes, 2009).
Each participant was guided to set two individualised goals (Priority Goal 1 and Priority Goal 2). The follow-up period was 6 months. The AusTOMs-OT and the GAS were used as outcome measures. The Wilcoxon signed-rank test was used to compare baseline and follow-up scores (p < 0.05 considered significant) and a gain of ⩾0.5 point on AusTOMs-OT and ⩾1 point on the GAS was used to determine the effectiveness of the SEER programme.
Data analysis
For data analysis, SPSS Version 18.0 was used. Frequency data on the demographic information was obtained. Differences in AusTOMs-OT and GAS scores before and after the occupational therapy was analysed with the Wilcoxon signed-rank test. The Mann-Whitney U test and Fisher’s Exact test were used to determine the effect of age and gender of AusTOMs-OT and GAS, respectively.
Results
Forty-one participants completed the pilot SEER programme. Figure 2 shows the flowchart of the recruitment process.
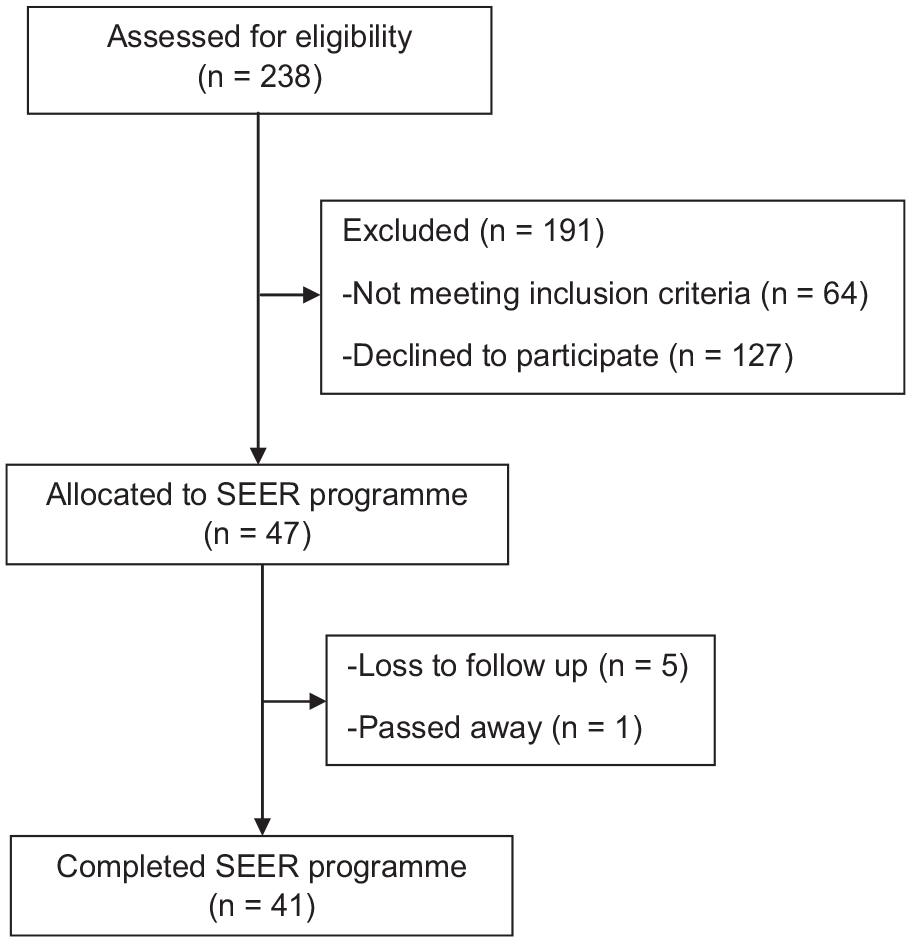
Flowchart of recruitment process.
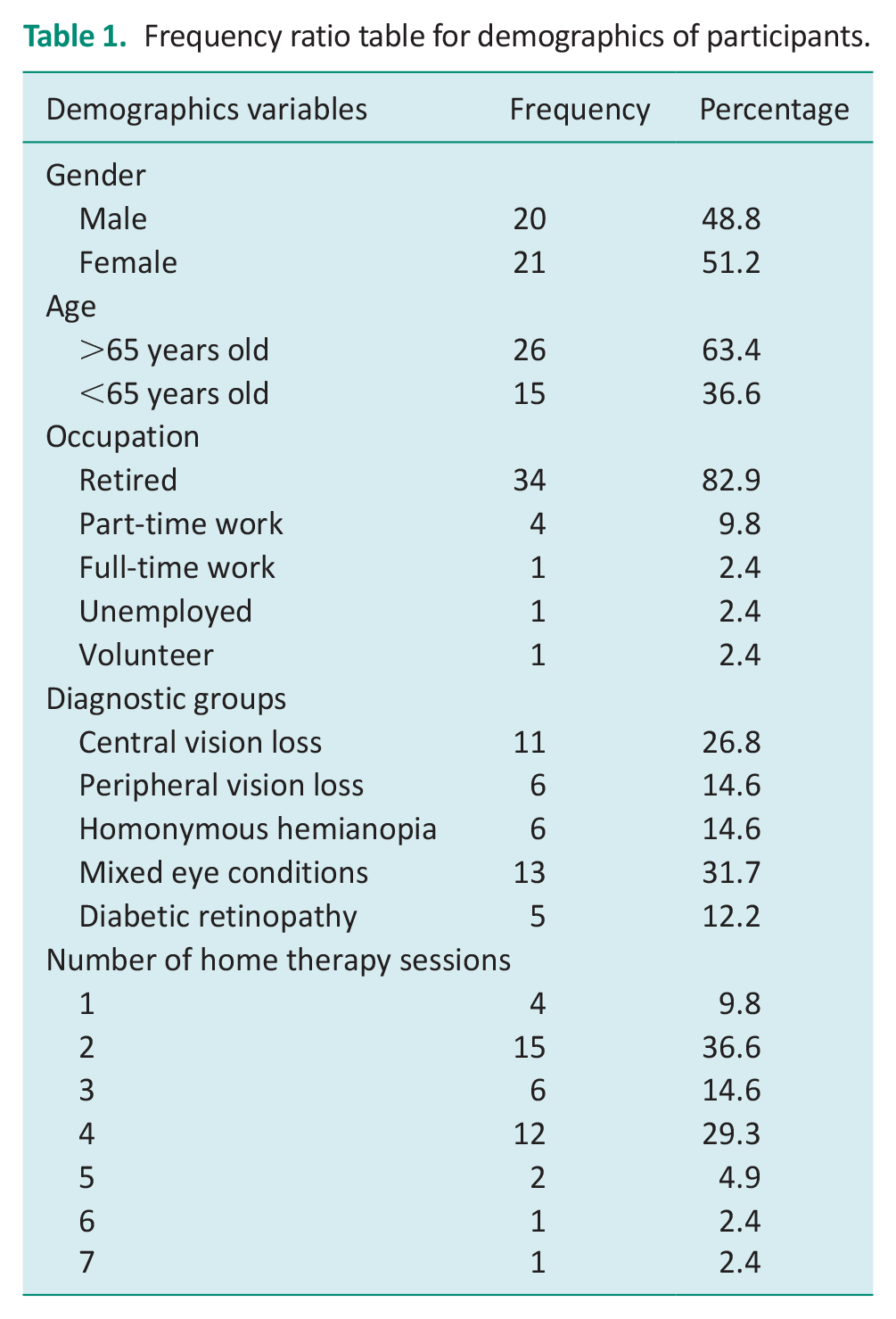
There were almost equal number of male (20) and female (21) participants. Twenty-six of the participants were above 65 years. Most participants (34) had retired. Four participants were doing part-time work while one was working full time and one was unemployed. There was one participant doing volunteer work. The breakdown of number of participants with different eye conditions is central (11), peripheral (6), homonymous hemianopia (6), mixed (13) and diabetic retinopathy (5). Most participants underwent 2 (15) or 4 sessions (12) of home therapy. Table 1 summarises the demographics of the participants. Table 2 summarise the pre and post-interventions scores of outcome measures AUSTOMs-OT and GAS respectively.
Frequency ratio table for demographics of participants.
Pre and post-intervention scores of outcome measure (AusTOMs-OT).
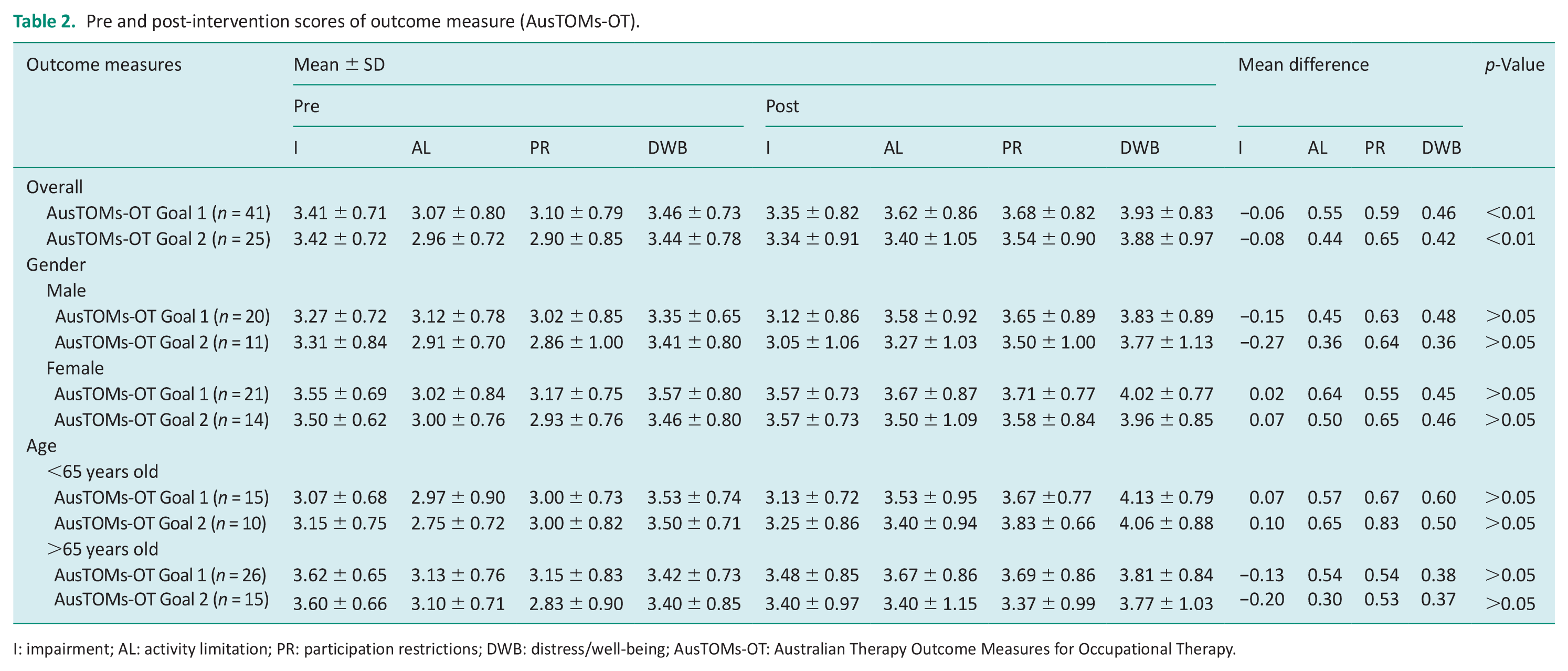
I: impairment; AL: activity limitation; PR: participation restrictions; DWB: distress/well-being; AusTOMs-OT: Australian Therapy Outcome Measures for Occupational Therapy.
For AusTOMs-OT Priority Goal 1, the most commonly used scales were ‘Functional walking and mobility’ (18, 43.9%) and ‘Carrying out daily life tasks and routines’ (8, 19.5%). For AusTOMs-OT Priority Goal 2, the most commonly used scales were ‘Functional walking and mobility’ (5, 12.2%)’, ‘Community life, recreation, leisure and play’ (5, 12.2%) and ‘Self-care’ (4, 9.8%).
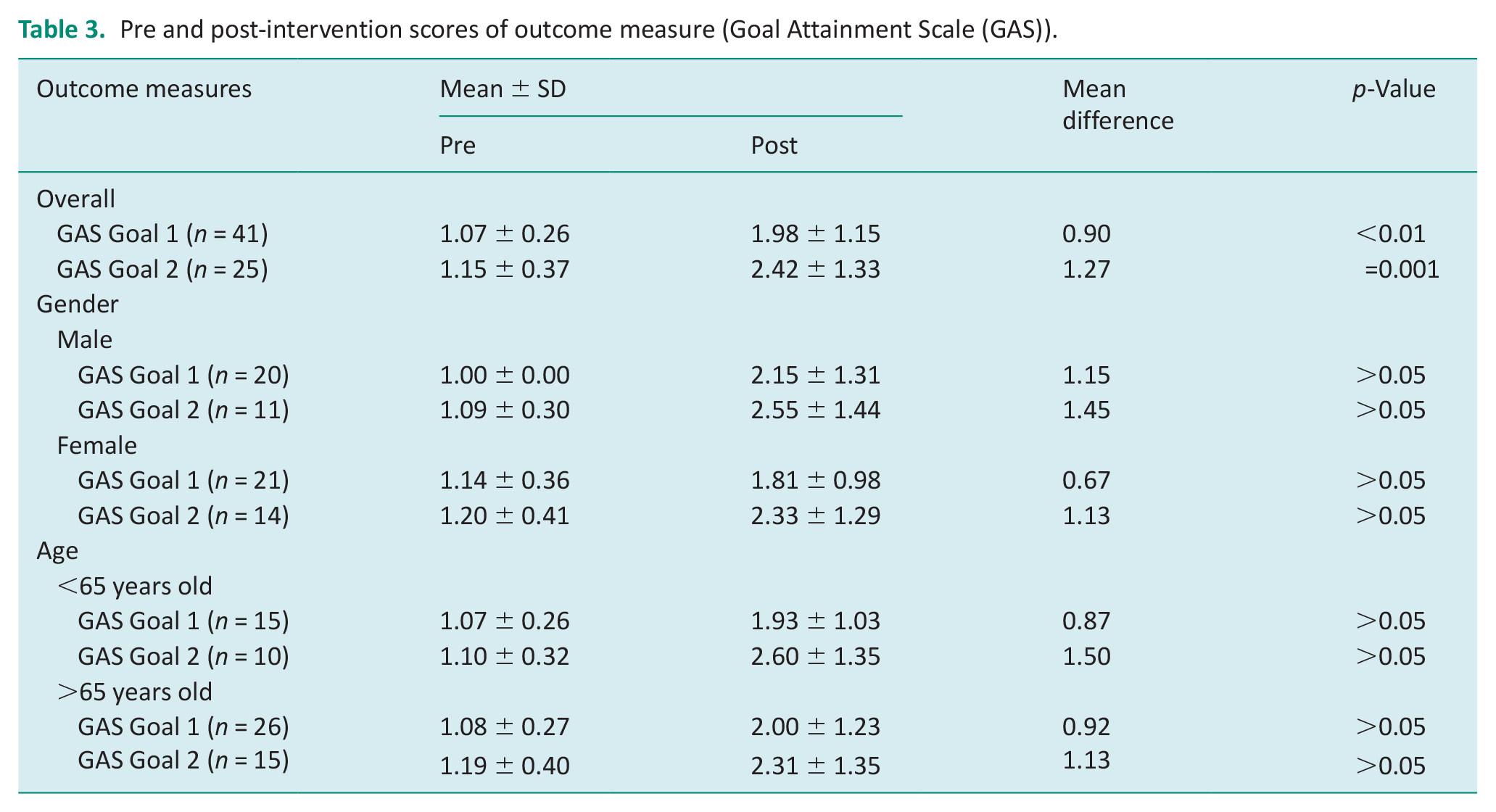
The SEER programme showed a statistically significant reduction in activity limitations (1 median point change (MPC), Z = −4.21, p < 0.01), a reduction in participation restrictions (1 MPC, Z = −3.951, p < 0.01) and improved well-being (0.5 MPC, Z = −3.668, p < 0.01) for Priority Goal 1 using AusTOMs-OT. For Priority Goal 2, AusTOMs-OT showed no statistically significant reduction in activity limitations (0 MPC, Z = 1.954, p < 0.051), but a significant reduction in participation restriction (0.75 MPC, Z = −2.777, p < 0.05) and improved well-being (0.5 MPC, Z = −2.509, p < 0.01). With GAS, a Wilcoxon signed-rank test showed that the SEER programme showed a statistically significant improvement in both Priority Goal 1 (1 MPC, Z = −3.886, p < 0.01) and Priority Goal 2 (1 MPC, Z = −3.433, p = 0.001).
A Mann-Whitney U test was conducted to determine whether there is an effect of age and gender on the efficacy of the SEER programme based on AusTOMs-OT. Participants below 65 years demonstrated better AusTOMs-OT outcomes across all AusTOMs-OT domains based on the Ranks table. We, therefore, conclude that there is a statistically significant difference in all the AusTOMs-OT domains (p > 0.05) for both priority goals between the two different age groups. There is also a statistically significant difference in all the AusTOMs-OT domains (p > 0.05) for both priority goals between the gender groups. Based on the Ranks table, female participants did better on the impairment and activity limitation domains for both Priority Goals 1 and 2 while male participants did better on the participation restriction and distress/well-being domains for both Priority Goals 1 and 2.
Fisher’s Exact test was conducted to determine whether there is an effect of age and gender on the efficacy of the SEER programme based on GAS. There is no significant difference between the two age groups (p > 0.05) and gender (p > 0.05) on both the Priority Goals 1 and 2 based on GAS.
The effectiveness of the SEER programme may be affected by the different clinical presentation of central vision loss and peripheral vision loss. Visual perceptual and cognitive problems may occur in cerebral visual impairments after brain injury, which may also affect the effectiveness of the programme. A pre-post analysis was not conducted due to small sample size. Tables 2 and 3 show the pre and post-interventions scores, including the overall, and between gender and age groups for AusTOMs-OT and GAS, respectively.
Pre and post-intervention scores of outcome measure (Goal Attainment Scale (GAS)).
Discussion
The SEER programme showed a statistically significant reduction in activity limitations, a reduction in participation restrictions and improved well-being for Priority Goal 1 using AusTOMs-OT. This study provides preliminary evidence that a home-based occupational therapy visual rehabilitation service has a positive influence on older adults’ participation in daily activities and well-being. The present evidence is based on an occupational therapy outcome measure and is in agreement with previous studies (Liu and Chang, 2020; Selivanova, 2019) showing effective rehabilitation by interventions with similar aspects to the present study, using different outcomes. However, the present exploratory findings are not consistent with a previous study (Reeves, 2004) who also examined a home-based rehabilitation intervention. That study did not find an effect of visual rehabilitation in a three-arm randomised controlled trial that compared: standard hospital clinic-based visual rehabilitation; standard hospital-based rehabilitation plus up to three additional home visits by a trained visual rehabilitation officer and standard hospital-based rehabilitation plus up to three non-rehabilitation home visits from a ‘community care worker’ (with no formal training). However, comparison is confounded given several differences to the design of the current study. The study (Reeves, 2004) only included participants with age-related macular degeneration and the visual rehabilitation officer focused on the use of low vision aids, while participants of the present study had low vision attributed to a range of causes and employed a range of rehabilitation intervention strategies encompassing several aspects of daily living. This more accurately reflects the nature of home-based low vision occupational rehabilitation, where multiple approaches are used based on the individual needs of patients. Additionally, different outcome measures were assessed.
For Priority Goal 2 involving IADL, only participation restriction demonstrated significant results. This could be that participation contexts are more practical and easier to adjust than activity contexts in view of the misfit between the person and the environment (Wahl, 1999) as a result of the declining low vision conditions.
Statistically insignificant results were demonstrated in impairment domains for both Priority Goals 1 and 2. This is not surprising in view of the chronic, progressive nature of low vision conditions (National Eye Institute, 2022).
Participants below 65 years demonstrated better AusTOMs-OT outcomes across all AusTOMs-OT domains in this study. These results are similar to the cross-sectional study done by Silva et al. (2018) although the focus is slanted towards a QoL measure. Female participants did better on the impairment and activity limitation domains for both Priority Goals 1 and 2 while male participants did better on the participation restriction and distress/well-being domains for both Priority Goals 1 and 2 in this study. In the study by Selivanova (2019), men were less likely to do well in functional and emotional aspects based on the National Eye Institute Visual Functioning Questionnaire (NEI VFQ-25). This is different to our study due to possible cultural differences.
For GAS, both Priority Goals 1 and 2 demonstrated significant changes. This is likely due to its sensitivity over standard measures, avoiding ceiling effects in this study (Rehabilitation Measures Database, 2020). This is also in line with a randomised controlled trial which showed that tailoring the interventions to meet participants’ personal rehabilitation goals had significantly greater gains in living skills performance than the control group, which received regular services that were not tailored (Pankow, 2004).
There is no significant difference between two age groups and gender on both the Priority Goals 1 and 2 based on GAS. This could be due to both age groups and gender groups optimising their rehabilitation potential based on the individualised nature of GAS (Turner-Stokes, 2009).
The involvement of the MSWs could have contributed to the improvements in well-being found in this pilot study. This was demonstrated by Lamoureux et al. (2007) who found significant but modest clinical improvements in emotional well-being in a low vision rehabilitation programme that included skilled welfare and support services. However, evaluating the psychosocial impact contributed by the MSW is beyond the scope of this pilot study.
Randomised controlled trials are needed to determine whether improvements in participation are due to engaging in the home-based low vision rehabilitation led by occupational therapists.
The conduct of the current study was undermined by recruitment to target. Barriers to recruitment occurred during or immediately after screening. Typical reasons given for declining to take part in the study included: household members or participants not open to home visits, participants dealing with other issues and not seeing rehabilitation as a priority at time of recruitment and potential participants not comfortable with taking part in a pilot programme. The strengths of the study include low vision trained occupational therapists to carry out the assessments and interventions; the analysis based on predefined outcomes and a follow-up period of 6 months. The limitations of the study include the modest sample size, non-masking of investigators and the lack of multiple study sites. To address these limitations, future researchers should consider a randomised controlled trial study design with single blinding where possible, and include a larger sample size, incorporating stratified sampling to enable more conclusive results relating to the effect of the programme interventions based on different diagnostic groups. Future researchers should also consider a multi-centre study design as it allows for enhancement of reproducibility and generalisability of the clinical work.
Conclusion
In Singapore, services for this population are growing but limited. The findings reported here may persuade policy planners in Singapore to recognise the value of home-based occupational therapy for low vision rehabilitation and build up the service provision. In conclusion, this study provides evidence that low vision home therapy rehabilitation provided by specialised low vision occupational therapists (LVOT) is beneficial to older adults with visual impairment and suggests that home-based low visual rehabilitation by trained occupational therapists is an important and useful part of an integrated care pathway. Further incentives and funding to improve accessibility to such a programme should be considered on a wider scale.
Key findings
Low vision home therapy rehabilitation by specialised LVOT benefits older adults with visual impairment
The benefits include reduction in activity limitations and participation and improved well-being according to AusTOMs-OT.
What the study has added
Low vision rehabilitation home therapy by specialised low vision occupational therapists benefits older adults with visual impairment and such a service is a critical part of an integrated care pathway.
Footnotes
Acknowledgements
We like to thank Dr Therma Cheung and Dr Silvana Choo for providing invaluable guidance on manuscript writing.
Research ethics
Ethical approval for the study was granted by Singhealth CentralInstitutionalised Review Board (CIRB).
Patient and public involvement data
During the development, progress and reporting of the submitted research, patient and public involvement in the research was not included at any stage of the research.
Consent
Informed consent was received from all participants.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study received funding from Temasek Foundation and Toteboard Singapore.
Contributorship
YT was involved in protocol development, study conception, data collection, data analysis and manuscript writing. CT was involved in protocol development, literature research and conceived the study. SH, LT and LC was involved in data collection.