
Abstract
Introduction:
Fatigue is one of the most common symptoms experienced by people with multiple sclerosis (MS) and can have a significant negative impact on participation in valued roles and activities. Understanding and supporting the management of MS fatigue is a priority to promote participation in life roles. This study explored how participants with MS who were enrolled in a fatigue management randomized clinical trial describe and explain their fatigue experience using a secondary qualitative analysis of interventionists’ treatment notes.
Method:
Clinical documentation including the subjective and objective portions of 85 treatment notes were collected and analyzed using a qualitative research design with multiphase coding.
Results:
Four major themes were identified including Fatigue Nature, Struggle, and Responding to the Reality of Fatigue with an overarching identified theme of Impact on Participation. Under the major themes, subthemes (11 total) were also identified and provided nuanced detail into each theme.
Conclusion:
People with MS fatigue describe their experience in a variety of ways. Findings will support occupational therapy practitioners to enhance empathy, understanding, and collaboration when working with clients with MS fatigue.
Introduction
Multiple sclerosis (MS) is the most common neurological disease of young adults (National Institute of Neurological Disorders and Stroke, 2021). There is no cure for MS and the disease reduces life expectancy by 7–8 years (75.9 years for individuals with MS; 83.4 years for the general population) (Marrie et al., 2015). Of all MS symptoms, fatigue has one of the greatest negative impacts on one’s experience of disability and is a limiting factor to participation (National Multiple Sclerosis Society (NMSS), 2022), as defined as an “involvement in a life situation” and participation restrictions as “problems an individual may experience in involvement in life situations” (World Health Organization, 2022). Approximately 80% of people with MS (pwMS) experience fatigue and it can negatively impact one’s ability to function at home and work (NMSS, 2022). Although there are various pharmacological interventions for MS in general, none have proven effective for limiting fatigue or its impact (Miller and Soundy, 2017). As such, individuals with MS are required to adapt, adjust, and self-manage the symptom in their daily life.
Recent qualitative literature has explored fatigue in MS and identified common themes of low energy, lethargy and exhaustion that go beyond normal tiredness. The impacts are significant on social life, emotional life, and cognition. People with MS often feel misunderstood with a difference in how they feel inside and how they are perceived by others. Still people struggle to accept and manage their condition (Eilertsen et al., 2015; Jaime-Lara et al., 2020; Penner et al., 2020). Occupational therapists (OT) are well poised to enhance or enable participation in roles and activities that are valuable or meaningful (Finlayson et al., 2008; Royal College of Occupational Therapists, n.d.). OTs use a variety of client-centered, evidence-based treatment strategies and approaches (e.g., remediation, restoration, compensation, adaptation, and the promotion of health and wellness (Preissner, 2014)) to overcome participation barriers in daily life including the areas of self-care, productivity, and leisure activities (Royal College of Occupational Therapists, n.d.). Enhancing occupational therapy providers’ appreciation of the experience of MS fatigue and utilizing evidence-based strategies to support the management of fatigue is key to ensuring the satisfactory participation and engagement of pwMS in desired and meaningful life activities and roles.
Self-management programs, such as the Managing Fatigue Programme, are efficacious and effective in minimizing the impact of fatigue for pwMS (Finlayson et al., 2011; Ghahari et al., 2010; Mathiowetz et al., 2005; Packer et al., 1995; Salomè et al., 2019). This substudy draws on participant data from a larger study titled
Method
Design
Secondary qualitative analysis was completed to better understand fatigue experiences of pwMS enrolled in a randomized control trial for fatigue management (Plow et al., 2020).
Sample and data collection
Eighty-five subjective and objective portions of documentation notes were selected and analyzed to capture the perspective of the participant. Specifically, notes from sessions 1 and 2 of therapist documentation (SOAP notes) from the REFRESH Study were initially selected by convenient sampling for 25 SOAP notes to begin qualitative exploration of the data and refinement of the research question. Purposive sampling was later used for an additional 60 SOAP notes distributed equally from the three modes of delivery, until data saturation began to emerge (Merriam and Tisdell, 2016). The subjective and objective portion of the notes were selected because they capture the perspective of the participant more than that of the interventionist.
The notes reflected a variety of participant and occupational therapists quotes. Specifically in session 1, participants were asked to provide a metaphor or brief description of their fatigue. In session 2, participants were asked to describe how they communicate their fatigue experience to others. Participant voice varies across the delivery modes as notes from group teleconference and one-to-one videoconferencing are written by OT while group internet-based notes are directly quoted from participants. It was important to include all three modes of delivery to obtain comprehensive descriptions of fatigue. OTs were trained in SOAP note documentation and encouraged to document the subjective section in the participants’ own words, using quotes when possible. The subjective section summarized important aspects of the session for participants. The objective section captured the measurable or observable information from the session relevant to participant engagement and often related to the subjective portion. Both pre- and post-COVID implementation of the REFRESH study were included.
Data analysis
A constructivist approach was selected to generate knowledge about how participants with MS describe and explain their fatigue and provide a foundation for analysis (Merriam and Tisdell, 2016; Patel, 2020). Coding included three phases in which all researchers were involved. In the first phase of coding, researchers independently coded a selection of data (N = 25). This open coding was done in vivo to retain context in which participants described their fatigue. All codes created were compared to establish an initial codebook where codes were rudimentarily grouped by common descriptions or similar descriptors. The initial codebook included all possible codes. The second phase utilized axial coding to apply the initial codebook to code 60 additional quotes. Following the application of the refined codebook, discussion helped establish consensus in refining groupings of codes into potential themes. Finally, selective coding was utilized to refine and define themes and codes/subthemes for the final codebook (Saldaña, 2016). Data was then reviewed and re-coded as necessary using the final code book to confirm its appropriateness to participant descriptions of fatigue. Quotes were, on occasion, overlapping and double-coded when appropriate. Microsoft suite (Excel) software was used throughout for data management and analysis.
Rigor
Rigor was ensured in this analysis consistent with qualitative research recommendations (Merriam and Tisdell, 2016). Internal validity was addressed using multiple investigators whom were involved in the REFRESH Study and participated in all phases of the study (Silverman and Marvasti, 2008). An extensive audit trail was kept throughout the course of this inquiry with members documenting all meetings, decisions, questions, and next steps at all phases of this project. The audit trail carefully defines the processes used for research question development, data selection, and analysis procedures (Lincoln and Guba, 1985). Consistency within the data completed by documenting therapists was maintained by uniform training as part of the (blinded) study. Ethical considerations were reviewed and approved centrally for all REFRESH study procedures at the Institutional Review Board of Case Western Reserve University.
Results
The average age of participants was 54 years, the majority of which identified as female (80%) and white (87.1%). They reported having MS for an average of approximately 17 years and reported being highly educated (70.6% bachelors’ degree or more). Table 1 outlines the characteristics of this study’s participants.
Characteristics of SOAP note project participants (N = 85).

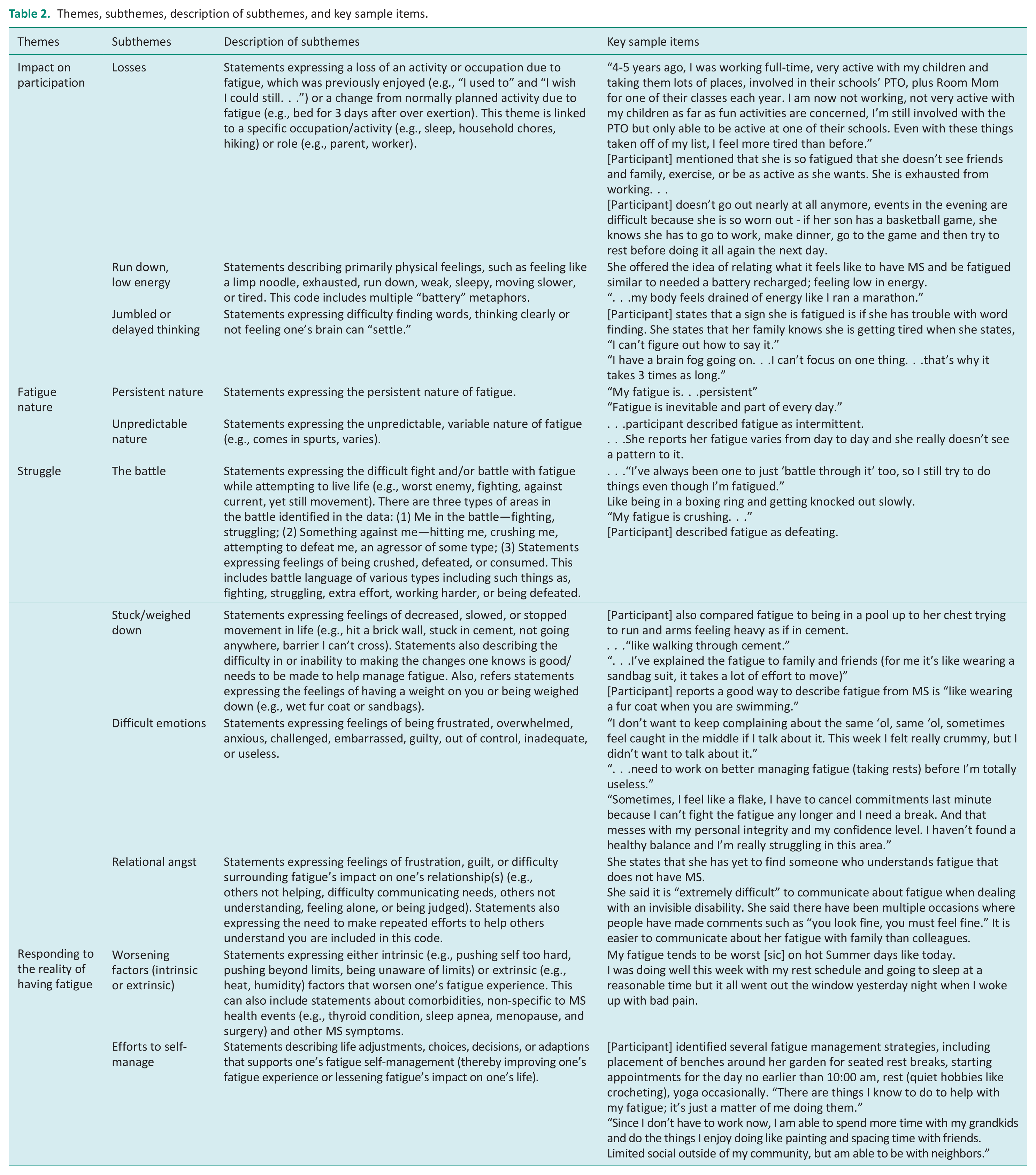
Four major themes (i.e., Impact on Participation, Fatigue Nature, Struggle, and Responding to the Reality of Fatigue) and 11 subthemes were identified. Table 2 outlines the identified themes and subthemes, including exemplar selected quotes for each subtheme. Participants discussed the struggle of responding to both the nature of and the reality of fatigue in their lives. A discussion of fatigue’s impact on participation was interwoven throughout.
Themes, subthemes, description of subthemes, and key sample items.
Impact on participation
Participants discussed diverse ways that they needed to adapt their participation because of their fatigue. Difficulty with participation changes emerged, especially in the areas of leisure and social participation. Participants described shifting participation choices and tension between their preferences, demands, and abilities, as they could no longer engage at a former frequency, time, or manner due to fatigue. Most often, participation in work, activities of daily living and instrumental activities of daily living were prioritized and participation in them resulted in fatigue that could negatively impact social and familial activities. Participating in activities such as seeing family or friends or helping with homework were in tension, especially in the evening for some as one person reported, “If there are events in the evening, I’m just so worn out.” Sometimes participants reported a tradeoff in which participating in one activity meant they had to give up another. Some indicated a slower pace to life and attention to the need to rest, while others reported that they participated beyond their capacity. “Over-participation” was an issue for some as participants, resulting in “crashing when finally home” or “being in bed for 2–3 days” after participating in an over extended certain manner.
Losses
Across all areas of participation, clinical documentation reflected circumstances where opportunities to participate were changed, reduced over time, or entirely lost. Many noted they used to enjoy leisure pursuits such as hiking, gardening, window shopping, participating at their child’s school, and exercise/fitness activities, which they can no longer do due to the physical demands or resulting fatigue. Sometimes more physical hobbies like sports or bike riding were replaced with sedentary hobbies such as crafting, playing chess, or using the computer. Many reported a change in work activities with participants describing a change in employment status (e.g., going full time to part time), a change in the way they worked (e.g., reducing physical demands), a change in employment (e.g., changing fields or finding a new job) and, in some cases, participants had to stop working entirely due to fatigue. Many of these changes were described as being dissatisfactory as participation losses were contextualized among their experience of MS fatigue.
Run down, low energy
Participants also used language like being run down or having low energy to describe fatigue’s impact on their physical body, and as such, on participation. Metaphors were used such as being “in a boxing ring and getting knocked out slowly” and “my body feels drained of energy like I ran a marathon.” Numerous quotes described low battery metaphors, feelings of depletion, exhaustion, or tiredness.
Jumbled or delayed thinking
In addition, clinical documentation reflected the impact on one’s mind related to cognitive fatigue and participation. They expressed challenges with jumbled or delayed thinking, including word finding, clarity, and focus. Examples include, “I have a brain fog going on. . .I can’t focus on one thing. . .that’s why it takes 3 times as long,” “Sometimes I can’t talk right, like I can’t get the words out right,” or having “mush mind.” Although some participants experienced an impact of fatigue to their mind or body, some experienced both: “moving slower and can’t process or do things as fast” and another, “Fatigue is my pronounced problem so far. The getting words together and feeling like I am walking through mud.”
Fatigue nature (persistent nature and unpredictable nature)
Participants experienced the nature of fatigue two ways: for some it was persistent and others unpredictable. Persistent daily fatigue created challenges in daily life. Active participants described awareness of fatigue in the background everyday as their fatigue was “nagging and persistent.” Those with unpredictable fatigue also found the presence of fatigue challenging. Each day is different with “some days not a problem and other days exhaustion takes over.” Presence of fatigue varied with both frequency and intensity. This makes planning and being consistent and reliable a challenge.
Struggle
Many of the participants described how they struggled with their fatigue. Overall, this theme was about participants’ approach of handling the tension of daily life demands and the impact of their fatigue. Within this theme, we identified four sub-themes: The Battle, Stuck/weighed down, Difficult emotions, and Relational angst. Some participants described experiences of fatigue as if they were physically battling against fatigue by fighting, exerting extra effort, or having to work much harder. Others experienced struggled with difficult emotions and relationships with others.
The battle
Participants described a fight against fatigue. For example, one participant described fatigue as their “worst enemy.” Some expressed a difficult fight and/or battle with fatigue while attempting to live a meaningful and fulfilling life. Some used metaphors to describe their struggles with fatigue. For example, one described their fatigue as “. . .a barrier I can’t cross.” Another described fatigue as, “Like being in a boxing ring and getting knocked out slowly.” These participants were actively trying to fight against their fatigue however they expressed a level of powerlessness against their enemy. Participants also shared that they felt crushed, defeated, or consumed. One participant described it by saying that it “. . .feels like the MS train hit me.” Others more generally described fatigue as “crushing,” “daunting,” and as their “worst enemy.”
Stuck/weighed down
In contrast to “The Battle,” in which participants were fighting back against fatigue, some participants expressed a sense of being stuck or weighed down. Some of these participants described a feeling of being “stuck” as they navigated life with fatigue, while others felt weighted down. Regardless of whether it was stuck or weighted down, these participants expressed feelings of decreased, slowed, or stopped movement in life. Participants who felt “stuck” described their fatigue as: “Feeling like ‘a stick in the mud’,” as if they were wearing “a strait jacket,” “walking through cement,” and feeling like they “hit a wall.” While some examples of feeling stuck were physical, others were more about lack of motivation. For example, one participant said, “There are things I know to do to help with my fatigue; it’s just a matter of me doing them.”
Others described decreased, slowed, or stopped movement in life. Those feeling weighed down by fatigue described their experience in a number of ways including feelings of having weight on. Participants who felt weighed down described their experience in a number of ways including: “Like wearing a fur coat when you are swimming,” feeling like “someone is pulling on me when I move,” and “like wearing a sandbag suit.”
Difficult emotions
Fatigue impacted struggles with difficult emotions within participants themselves. Many participants associated their fatigue as causing emotional turmoil or dread. They also described fatigue using words conveying negative emotions. The descriptors were simple, yet profound, such as: “exhausting,” “awful,” “overwhelming,” and “defeating.” An analogy used by one participant summed up his fatigue as “uncontrolled exhaustion” and “Feels like someone pulled the plug, and if you’re a car, all your oil drained out.” Some participants described internal angst, like feeling guilt or anxiety, because of not being able to accomplish all they want to do or activities taking so much longer to complete.
Participants expressed feeling inadequate or made self-deprecating remarks from internal angst about limitations and said that fatigue “messes with [their] personal integrity and confidence level.” Participants called themselves “lazy,” “a flake,” and often “become annoyed” with personal limitations or need for assistance.
Relational angst
Many participants experienced emotional angst in their relationships with others. Participants felt that even close family members “really don’t understand [their] fatigue,” or leave them feeling “weird.” Participants found relief from this angst when they learned that others struggle in the same ways they do. Having friends with MS or reading programme manuals discussing similar challenges decreased isolation and increased connection. In the workplace participants expressed fear and concerns about being judged by coworkers. They “[feared] being let go” or that others will judge them as not performing well enough leaving them “feeling weak.” This tended to increase isolation as participants avoided communication about their fatigue because they “[don’t] want people to think it was affecting [their] work.”
Responding to the reality of fatigue
Participants had a variety of responses to living with MS fatigue. Many identified specific worsening factors and challenges that interfered with fatigue self-management. Approaches to implement fatigue management strategies were varied and often began with awareness or testing new strategies for effectiveness.
Worsening factors
Participants identified factors that were associated with worsening fatigue. Caretaking demands such as caring for a child with autism impacted fatigue. Pain related to back surgery or other factors negatively impacted rest schedules and fatigue: “I was doing well with my rest schedule, and it all went out the window when I woke up with bad pain.” External factors such as warm weather and humidity tended to make fatigue worse, “. . .the humidity and heat has been tough on me.”
Participants made observations about behavioral patterns that played a role in worsening fatigue. There was a tendency among participants to overdo or to not take a break until exhausted, resulting in worsening fatigue. Participants stated, “I often overdo and then I pay for it for the next few days.” One individual said that they related to the person in the manual who says, “I tend to push myself too far and am exhausted at the end of the day.”
Efforts to self-manage
Even when participants were aware of strategies that could improve fatigue management, they described challenges to regular implementation. Desires to enhance participation in exercise were less consistent because one participant “[didn’t] feel like he can ask for help all the time” to get on his stationary bike. Sometimes the desire to remain active and to build in rest breaks were in conflict as participant stated “I try to push myself.” Others noticed the positive impact of energy banking and struggled with “how to [get] into a habit to remember to rest.”
Our findings indicated that there were activities that helped with fatigue management, such as engaging in valued activities. For example, one participant reports she “. . . doesn’t feel the tiredness as much” when she engages in photography. Other activities, such as not stopping until a task was done or ignoring early signs of fatigue, resulted in repercussions such as “paying for it for the next few days.” Prioritizing valued occupations and activities was a strategy that promoted enhanced fatigue management for several participants. With less work demands, participants had more time to be with grandchildren and enjoy hobbies such as painting and being with friends. Extra time to space activities or prioritizing chores and tasks improved fatigue management. Just engaging in favored activities for some resulted in positive outcomes as “she doesn’t think or feel the pain or tiredness as much.”
Participants use a variety of strategies to decide on and implement changes in habits, roles, or routines. For some, change was inspired by self-assessment or education. One participant noticed, “I don’t feel guilty about it. . .now, I am able to rest and know I am banking energy.” For others it required making a decision and testing it out which often involved communication with others such as politely communicating “I am going to go rest for a short time, please excuse me.” or “I will try to take 10 minutes in the morning or afternoon to just mentally rest at my desk.” Making changes is a process and can be done in many different ways. Rests can be planned or for others, “she takes them when she feels like it.”
Discussion and implications
Fatigue is a common, at times disabling, symptom experienced by individuals with MS. Enhancing the understanding of MS fatigue can contribute to provider empathy and to quality intervention planning and treatment approaches. Participants in this study described fatigue in a broad and diverse manner. This multidimensional view of fatigue is consistent with variability across, and even within, an individual with MS and the significant impact on daily life (Billones et al., 2021). A tailored approach to assessment and intervention planning, considering primary and secondary potential causes of fatigue, is needed to support the self-management of fatigue (Connolly et al., 2013; Labuc, 2021; Salomè et al., 2019). Participants expressed physical fatigue descriptors (e.g., feeling run down, low battery), cognitive fatigue descriptors (e.g., jumbled, mental fog), and fatigue’s impact on participation. To better access these varied experiences, a stronger understanding of an individual’s MS fatigue experience would be helpful. A self-report questionnaire that is reliable and valid to measure the multidimensional aspects of fatigue (Plow and Gunzler, 2022) is warranted. One way this could also be explored is through open-ended questions that encourage pwMS to describe their experience such as, “What is fatigue like for you?”; “How would you describe your fatigue experience?”; or “If you didn’t have fatigue, what would you be doing?” (Sleight, 2022).
Consistent with Eilertsen et al. (2015), fatigue had a significant impact on participants’ roles, activities, and occupations. They described the struggle to manage their fatigue and expressed having to give up valued activities, find new ones, and adapt in various ways on a daily basis (Penner et al., 2020). Supporting the expressed occupational demands and need for adaptation (American Occupational Therapy Association, 2020; Grajo, 2019) in the lived experience of fatigue is a necessary consideration in treatment planning and intervention. Especially salient to practitioners is tension that participants experienced between their preferences, the demands placed on them and their ability to adequately meet expectations as they work to accommodate fatigue. Providers should view this point of tension as an opportunity to help assess and intervene using supports and strategies to meet client’s desired, valued participation goals. This should include a holistic approach to assessing the occupational demands with considering the match between person, environment, occupation, and performance (Baum et al., 2015). Similarly, in regard to evaluation and outcomes, OT can consider how to best measure participation and how to support development of realistic goal writing and action planning around participation goals related to fatigue.
PwMS struggled with fatigue management in their daily life in profound ways. Sometimes participants failed to utilize self-management strategies falling back on enduring pain and pushing through fatigue. Participants reported using a variety of common strategies to self-manage and shared details about the process of making changes. Some common strategies reported included pacing, listening to the body, and balancing rest and activities. Participants explored and experimented to determine what worked for them and expressed benefits of creating habits for fatigue management and challenges of forming and maintaining them.
OTs working with pwMS may promote participation in valued activities as an important aspect of treatment for comprehensive fatigue management. Participant struggles with habit formation around meaningful occupations may not be linear but still worth pursuing. When participants attempt to make a routine change, they may experience setbacks as they consistently implement a strategy into their lives. OTs working with pwMS can help clients better navigate the fluctuations in the self-management process realizing progress and setbacks are common and expected. Participant’s efforts to gain control and live better lives amidst their fatigue may also be best supported by peer education or interaction. Barlow et al. (2009) demonstrated that when pwMS participated in a lay lead chronic disease self-management programme, they learned new skills and were reminded of the self-management skills they already knew. Occupational therapists intervention may be better supported long-term utilizing peer-support or mentoring opportunities related to fatigue management. Across all challenges, findings reinforced that pwMS demonstrated a determination to adapt to MS (Desborough et al., 2020).
Individual struggles in dealing with fatigue were exacerbated by feeling misunderstood and judged by friends, family, and coworkers who see them as healthy (Jaime-Lara et al., 2020; Lacerda et al., 2019), which can then result in a decrease in social confidence and impact communication efforts. These negative impacts may be alternatively approached in appreciating the value of metaphors. Metaphors may serve pwMS in their ability to richly describe fatigue, garner empathy, and serve as approachable representations of fatigue to others. Metaphors can also help healthcare providers better understand the experiences of others. By listening carefully to client’s use of metaphors, practitioners can have a deeper understanding of the fatigue experiences supporting the client-provider relationship and act as a means to better explore participant goals. Engagement with metaphors can provide an opportunity for helping pwMS to better understand themselves and simultaneously help others better understand their experiences, while at the same time yield understanding to the potential of catastrophizing fatigue by the nature of the selected metaphor (Arewasikporn et al., 2018). Applying empathy to better appreciate the experience of MS fatigue, providers can develop compassionate, informed treatment plans and interventions. Self-management successes may also be strengthened as metaphor and change have been shown to be linked (Sarpavaara, 2010).
Simply reading the definition of fatigue as a “subjective lack of physical and/or mental energy that is perceived by the individual or caregiver to interfere with usual and desired activities” (Multiple Sclerosis Council for Clinical Practice Guidelines, 1998: 2) may limit a practitioner’s ability to meaningfully understand the scope of how clients both perceive and experience fatigue in the context of their daily life. Ensuring a broader view inclusive of diverse fatigue experiences will enhance the client-therapist collaborative relationship, with the hope to support the management of fatigue and enhance valued participation.
Limitations
This sample represented a subset of participants from self-selecting persons interested in fatigue management and may not be representative of all persons with MS as the sample. For example, our study was underrepresented for those identifying as Black or African American or those outside of the Midwestern and Northeastern United States and more representative of those willing to engage in a self-management program. Further research inclusive of a more diverse population, and their experiences with MS fatigue, can improve understanding across cultures, socioeconomic status, education levels, and geographic regions to allow a more generalizable perspective on fatigue.
It is important to note that most of the data utilized was secondary clinical documentation initially intended to document participant performance in the Managing Fatigue programme with limited intention to be analyzed for fatigue experiences. Upon consideration, this documentation showed rich descriptions and metaphors of fatigue experiences that lent itself to qualitative analysis with implications for practitioners. Data was inclusive of some direct quotation from participants in the online arm of the study; however, participant experience as documented by OT that may indicate some limited application. Future directions should include analysis of MS fatigue experiences through first-hand or primary documentation to provide a holistic and accurate view of fatigue experiences by persons with MS.
Conclusion
The impact of MS fatigue is significant and is experienced and described in a variety of ways. Despite many challenges, participants strived to find ways to adjust to living with MS fatigue. Through attentive listening and collaboration, OT can play an important role in individualizing treatment and supporting people with the self-management of MS fatigue to enhance participation in meaningful occupations and roles.
Key findings
Experiences of MS fatigue are diverse and profound.
Individualized participation assessment and treatment is a priority for clients experiencing MS fatigue.
Empathy and listening are necessary treatment tools to support clients with MS in managing their fatigue.
What the study has added
This study has added a broader understanding of the diverse and profound experiences of fatigue and its impact on participation for those individuals with MS.
Footnotes
Acknowledgements
The authors would like to acknowledge the REFRESH study research team, participants, and occupational therapists for their contributions to this work.
Authors’ Note
Maureen Gecht-Silver is also affiliated to Adjunct Occupational Therapy Faculty, DePaul University, Chicago, IL.
Jacqueline Kish is also affiliated to Department of Occupational Therapy at the University of Illinois at Chicago.
Research ethics
The protocol is approved centrally by the Institutional Review Board at Case Western Reserve University [STUDY20180027].
Patient and public involvement data
During the development, progress, and reporting of the submitted research, patient and public involvement in the research was not included at any stage of the research.
Consent
All participants provided consent which was obtained online using REDCap.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported through a Patient-Centered Outcomes Research Institute (PCORI) Project Program Award (MS-1610-37015) [Grant Number: NCT03550170].
Contributorship
All authors researched literature, conceived and developed protocol for this qualitative study. Matthew Plow and Katharine Preissner were involved in gaining ethical approval for the larger PCORI study. All authors were involved in data analysis, writing the first draft of the manuscript, and reviewing/editing/approving the final version of the manuscript.
Disclaimer
All statements in this report, including its findings and conclusions, are solely those of the authors and do not necessarily represent the views of the Patient-Centered Outcomes Research Institute (PCORI), its Board of Governors, or Methodology Committee.