
Abstract
Introduction:
International guidelines for best practice indicate specialised treatment is required for Juvenile idiopathic arthritis (JIA). While occupational therapy intervention for functional limitations in this chronic condition is conditionally recommended, the extent to which this is provided in public specialist rheumatology clinics in South Africa is unknown. The aim of this study was to determine which needs related to outcomes for occupational performance or functional status, condition-related factors and health-related quality of life, reported by children and adolescents with JIA were addressed by current occupational therapy services.
Methods:
The study used two descriptive, quantitative studies with limited samples of 37 clients with JIA attending specialist rheumatology clinics and nine occupational therapists who currently provide intervention for clients with JIA.
Results:
Functional deficits reported by 30–63% of clients with JIA were increased symptoms of active disease and difficulties with school activities. Occupational therapy services addressed condition-related factors and participation in personal management but not many related to the social, educational and psychosocial needs of clients with JIA.
Conclusion:
Occupational therapy services followed international guidelines but based on the reductionist biomedical model approach used within specialist services in tertiary hospitals, which limit context-based therapy for children and adolescents with JIA in the community.
Introduction
The chronic rheumatic disease in childhood, juvenile idiopathic arthritis (JIA) is an autoimmune disease of unknown aetiology with several different subgroups. JIA is characterised by chronic inflammatory arthritis of the joints (Petty et al., 2015). The typical indicators associated with JIA include physical symptoms such as pain, joint stiffness and swollen joints, which may result in joint deformity and growth impairments. Some psychological symptoms such as nervousness, anxiety, depression and concentration deficits are also reported (Eyckmans et al., 2011; Wells and Smith, 2015). These symptoms may persist into adulthood and affect the individual’s ability to engage in their everyday activities, which can impact health-related quality of life (HRQoL) (Listing et al., 2018).
Some advances have been made in providing specialised services for clients with JIA, at the tertiary level public hospitals in South Africa (Lewandowski, 2020) where intervention is based on the international treatment guidelines for JIA. These guidelines recommend a combination of multi-disciplinary services to address the needs of clients with JIA, including occupational therapy. However, evidence of best practice is mostly related to pharmacologic treatments and clinical remission (Klein et al., 2020; Ringold et al., 2019; Ringold et al., 2014). The American College of Rheumatology (ACR) only started to consider clinical guidelines for non-pharmacologic treatments for JIA in their 2021 project plan. For the first time, a rehabilitation professional has also been included on their core oversight team (American College of Rheumatology, 2021).
While the ACR conditionally recommends occupational therapy for clients with JIA who have or are at risk of functional limitations (Ringold et al., 2019), there is little research evidence of clinical guidelines for the profession. Aja et al. (2016) in a systematic review reported most occupational therapy intervention addresses condition-related factors such as pain, range of motion using splints and functional exercises. A number of authors have also described the role of occupational therapy in JIA in terms of standardised assessments, assistive devices, joint protection techniques and environmental adaptation (Rottermund et al., 2015; Van Oort, 2020). Van Oort (2020) however indicates conflicting evidence for psychological interventions for this condition.
While emphasis is placed on occupational therapy services for children and adolescents with JIA being holistic and tailored to meet individual occupational performance and condition-related needs (Rottermund et al., 2015; Ziff, 2016), this should be context specific. Occupational therapists need to be cognisant of the different disease presentation of JIA in the South Africa compared to other international populations (Scott and Webb, 2014). Achieving an integrated holistic occupation-based approach within occupational therapy practice may also be inhibited by the health service context. Limited intervention opportunities, particularly in tertiary care in South Africa (Department of Health, 2020) within the public sector were financial constraints result in a lack of resources and limited healthcare professionals, (Ngobeni et al., 2020) may also play a role.
Literature review
JIA is diagnosed in children under the age of 16 years who have chronic arthritis for more than 6 weeks resulting in the inflammation of multiple joints (Scott and Brice, 2015). Internationally in the past two decades major changes in the management of JIA have been achieved through the introduction of biological disease-modifying antirheumatic drugs (Ravelli et al., 2018). While these advances have reduced the level of disease activity, some children with JIA continue to experience articular and extra-articular damage and disability (Ringold et al., 2019). This may be the case for children and adolescents with JIA treated in the public sector in South Africa, since paediatric rheumatology was only registered as a speciality in this country in 2008. As a result, specialist teams are limited due to insufficient, appropriately trained human resources (Lewandowski, 2020), and specialised care is only offered in the 29 public tertiary hospitals in the country. Clients have poor access to these limited services, which is affected by poor referral pathways from lower levels of healthcare (Department of Health, 2020) resulting in late diagnosis, inadequate care leading to poor management and insufficient prevention of deformities (Aoust et al., 2017). The management of JIA in South Africa also needs to consider the local patient profile of children and adolescents who present with high functional disability, pain and joint limitations, impacted by comorbidities such as HIV and tuberculosis (Scott and Webb, 2014).
Although adherence to international guidelines for the pharmacologic management of JIA is emphasised in the rheumatology clinics in the public tertiary hospitals, recommended occupational therapy focuses on intervention of physical client factors (Rottermund et al., 2015; Ziff, 2016). Ziff (2016) indicated that individuals with JIA also experience activity limitations or participation restrictions, which result in psychosocial and HRQoL dysfunction and suggested that these aspects be addressed by occupational therapists. The determination of appropriate and holistic occupational therapy outcomes and strategies to promote and preserve the client’s current functioning to meet progressive developmental stages is thus a priority. Gentry et al. (2018) suggested that occupational therapists should play a role in ensuring independence in the home and school environment, manging virtual technology as well as referral to available community resources including those that support psychosocial adaptation.
Very limited research on evidence-based occupational therapy for JIA is available. A broad range of outcomes are rarely included in the current clinical guidelines (Ravelli et al., 2018; Ringold et al., 2019). It is, however, recommended that standardised assessment tools and clinical measures for physical, psychological, social functioning and quality of life (QoL) are utilised to improve evidence-based practice in occupational therapy (Brown and Wallen, 2002; Van Oort, 2020). Assessments, such as the Juvenile Arthritis Multidimensional Assessment Report (JAMAR) (Filocamo et al., 2011), has been recommended to evaluate the children’s, adolescents’ and parents’ perception of the outcomes of JIA for supporting treatment goals, to identify rehabilitation needs and for determining change. The JAMAR has been reported to have adequate face and content validity as well as reliability. The assessment tool has been used in various international studies in 52 countries (Morgan and Carle, 2020).
The purpose of this study was to determine which outcomes, indicate rehabilitation needs for occupational performance or functional status, condition-related factors and HRQoL, reported by children and adolescents with JIA (or their parents) attending the specialist rheumatology clinics, were addressed by current occupational therapy services.
Methodology
This study consisted of two parts. In the first part a survey, used the JAMAR, a standardised self-report questionnaire. This allowed cost-effective, time-efficient data collection while clients were attending clinic visits. Questions on the JAMAR cover perceptions of children and adolescents with JIA or their parents about the functional activity status as well as JIA disease outcomes such as pain, morning stiffness, disease activity and disease status of clients with JIA. HRQoL is also assessed in relation to satisfaction with illness outcomes as well as school-related issues.
In Part 2, a survey questionnaire was specifically designed, by the first author, to determine the current services offered by occupational therapists for children and adolescents with JIA, since no standardised survey was available. Open and closed ended questions were based on the role of the occupational therapist in the management of clients with JIA in accordance with international recommendations. Questions included information on the reason for referral to occupational therapy, assessments used, treatment focus, intervention provided as well as barriers related to offering holistic and integrated services.
Total population sampling included recruitment of all eligible clients with JIA and occupational therapists available at the study sites. In Part 1, the population included the limited number of 37 children or adolescents, recently (within the last 3 months) diagnosed with JIA and who had no comorbidities. They were between 3 and 16 years of age and attended one of two paediatric specialist rheumatology clinics at tertiary public hospitals in South Africa. Children and adolescents were excluded if they had previously been assessed with the JAMAR.
A total population of nine occupational therapists providing services to specialised paediatric rheumatology clinics in four tertiary hospitals, who were involved in the intervention of clients with JIA, participated in Part 2 of the study.
Ethics
Ethical clearance was provided by the Human Research Ethics Committee of the University of the Witwatersrand (M1121163). Permission to conduct the study was attained from the Department of Health, the Chief Executive Officer of each of the participating hospitals and Heads of Occupational Therapy Departments. An information sheet, which described the details and intention of the research, was provided to each client with JIA and their parents as well as the occupational. No names or identifying data were collected.
Research procedure
Part 1: Children and adolescents with JIA
Research data were collected using a demographic questionnaire and JAMAR (Filocamo et al., 2011). The questionnaires took approximately 15 minutes to complete.
Data collection
The data were collected weekly at the paediatric rheumatology clinics that were held at two research sites. Parents or caregivers of children and adolescents, who met the inclusion criteria, were invited to participate. Children and adolescents with JIA and/or their parents were asked to complete the JAMAR. The assessment is suitable for all ages and can be completed either by a child or an adolescent with JIA older than 7 years or by the parent as a proxy report for children under the age of 7 years. Although participants or their parents were asked to complete the self-report JAMAR independently, the first author was always available to assist with language issues and to explain questions if required, especially with younger participants.
Part 2: Occupational therapists providing intervention for JIA
Data for this part of the study were collected using the self-report survey. The survey questionnaire had undergone pilot testing by two experienced occupational therapists and revisions of the questionnaire included clarification of terms and the addition of options for treatment services.
Data collection
All occupational therapists working at four tertiary-level hospitals providing services at specialised paediatric rheumatology clinics were invited to participate. The survey questionnaire was distributed in hard copy to them. Once completed, the questionnaires were placed in sealed envelopes for collection for the next day.
Data analysis
Statistica v 13.3 was used to analyse data from both surveys. In Part 1, descriptive statistics and frequencies for outcomes from the JAMAR in relation to occupational performance or functional status, condition-related factors and HRQoL were determined. Reported outcomes were expressed as percentages to determine rehabilitation needs.
In Part 2, descriptive statistics were also used to analyse the data on occupational therapy assessments, treatment focus, treatment intervention and services offered. In Part 2, content analysis was used to categorise the responses from open-ended questions, and categories were then quantitatively analysed by frequency of response.
The frequency of outcomes indicating rehabilitation needs of the clients with JIA attending specialist at rheumatology clinics was aligned with the frequency of current occupational therapy services provided to address these outcomes for clients with JIA.
Results
Part 1: Children and adolescents with JIA
Of the 37 children or adolescents with JIA who participated in the study, 14 (37.84%) were males and 23 (62.16%) were females. The majority of the participants were Black African (81.08%), with the most common age groups being 11–12 years (18.92%) and 13–14 years (18.92%). Medical services provided by rheumatology specialists were attended by all participants, but with only between 31% and 46% of the participants at the respective hospitals being referred to occupational therapy.
The JAMAR
The following sections, which relate to occupational therapy assessment and intervention, were extracted from the JAMAR for this article.
Evaluation of functional activity
In Figure 1, the analysis of functional activity indicated that the most difficult functional activities were gross motor activities such as running on flat ground for at least 10 m, jumping forward and bending down to pick something up. The single most difficult activity was squats for which 38% of the participants scored some difficulty, 8% of the participants scored much difficulty and 3% of the participants scored severe difficulty. Difficulty was reported by 27% of the participants for resisted hand function such as opening and closing a tap or opening a previously opened jar, whereas 8% had much difficulty with this activity (Figure 1).
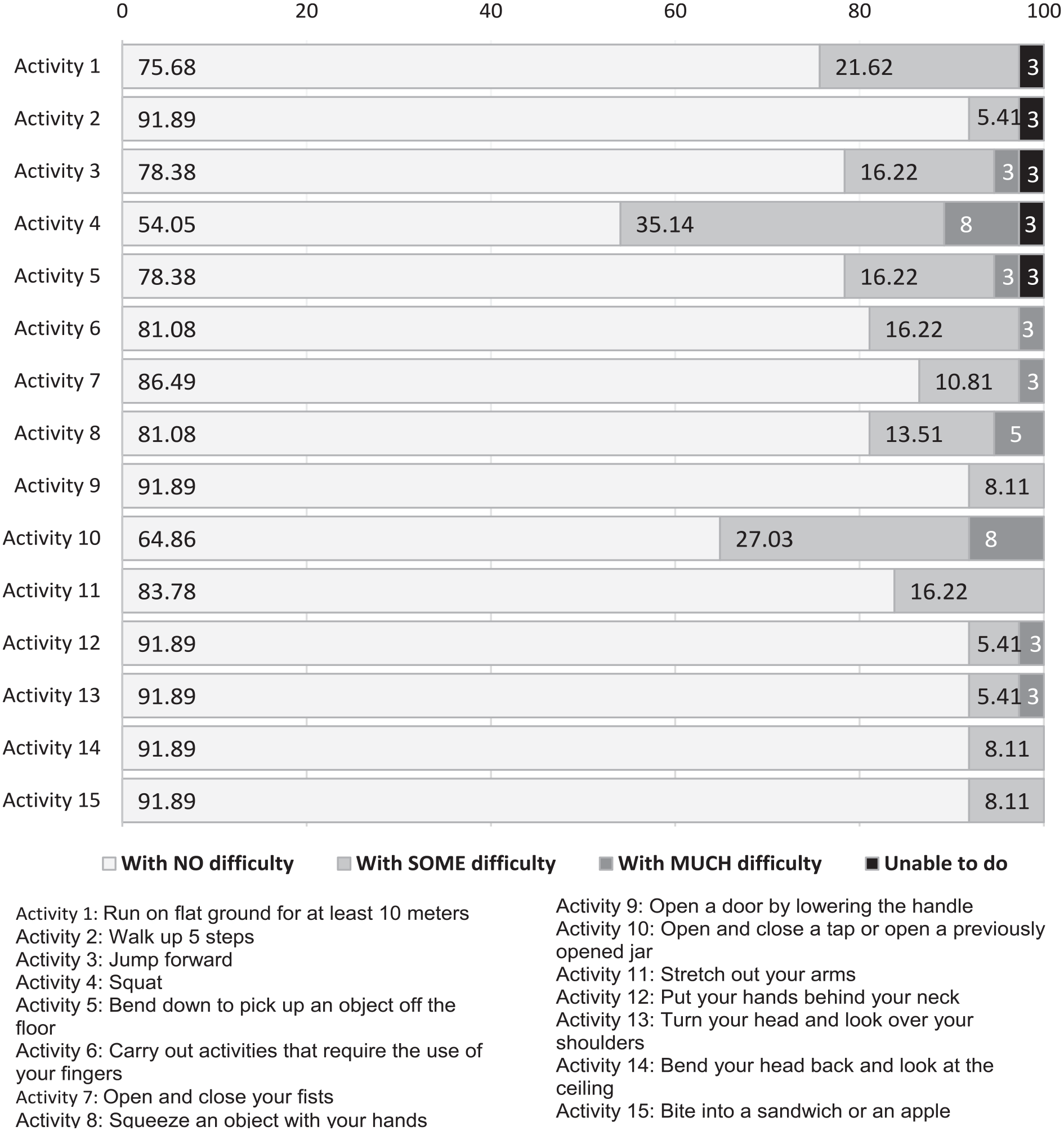
Evaluation of functional activity (n = 37).
Evaluation of disease activity
It was noted on the completed pain scale (on VAS from 0/10) that less than half (46%) of clients with JIA experienced no pain, whereas 18% of the participants rated their pain being mild (>3/10) and 5% of the participants rated their pain as severe (10/10) in the past week.
Two-fifths of clients with JIA or their parents responded that there was no joint pain or swelling on the day of their clinic visit. For those who reported joint pain and swelling on the day of the clinic visit, the knees, ankles and fingers were most affected. Nearly 90% of clients with JIA, however, responded that they had experienced joint stiffness lasting between 15 minutes and 2 hours in the morning in the past week.
The level of disease activity was reported to be 0 by 38% of clients with JIA or their parents, whereas another 33% rated disease activity as mild (1–4) and 29% rated the level of disease activity as severe (5–10). When considering the disease course since their first clinic visit, 59% reported the persistent disease activity, whereas 25% reported no change and 75% agreed that there has been improvement.
Quality of life
The evaluation of HRQoL indicated pain has the greatest effect with more than half of clients with JIA or their parents reporting that they sometimes experienced pain every day. QoL was least impacted by social participation as assessed by ‘has had any trouble getting along with other children’, whereas over 70% reported no difficulties with school activities and independence in personal management. Only one-fifth of clients with JIA or their parents reported difficulty remaining seated for a long time and even less reported numerous absences from school (Figure 2).

Evaluation of Quality of Life (n = 37).
Part 2: Occupational therapists providing intervention for JIA
Of the nine occupational therapists who participated in the study, eight stated that they treated an average of one to ten clients with JIA monthly, whereas one therapist treated 11–20 clients. Five of the therapists indicated that the majority of clients were between 11 and 18 years of age.
Current occupational therapy services
Reason for referral to occupational therapy
The most common reason for referral was for assistive devices (n = 8) followed by provision of splints (n = 7). No referrals were made for learning disabilities and psychosocial problems.
Assessments used
Seven therapists stated that they did not use any formal screening tools or standardised assessments specifically designed for clients with JIA. Two therapists at one hospital had created their own assessment tool.
Treatment focus and intervention provided
The occupations the therapists reported most commonly included in the treatment of clients with JIA, were personal management (n = 8) followed by education (n = 5). Social participation and leisure were the least common occupations addressed and were considered by only one therapist. Occupational therapy services offered included splints, assistive devices, pain management, functional exercise, home programmes and school-related activities. The six therapists who provided splints agreed that resting splints were most commonly irescribed followed by splints for wrist extension and swanneck deformity. Wheelchairs/seating devices and personal management assistive devices were prescribed by seven of therapists, whereas four therapists provided assistive devices to assist in the classroom and one therapist never prescribed assistive devices. The most common assistive devices made for clients with JIA were pencil grips (n = 5) followed by built-up handles (n = 4) and wash mitts (n = 3).
All the therapists reported using joint protection techniques to manage pain symptoms, with five preferring the use of heat packs and two wax baths. Therapists noted that functional exercises were most commonly used to address client factors such as range of motion (n = 8), muscle strengthening (n = 6) and endurance (n = 4). Between hospital visits therapists relied on home programmes, which commonly included joint protection principles (n = 8), and functional exercise programmes (n = 7). Play home programmes were the least used, whereas no home programmes to facilitate social participation and leisure were used (Figure 3). No referrals to occupational therapists offering care at a community level were reported.

Occupations focussed on in therapy for clients with JIA (n = 9).
Barriers related to offering holistic and integrated services
Barriers to offering rehabilitation services reported by therapists included the multidisciplinary team having a poor understanding of the activity limitations and participation restrictions associated with JIA. Of the nine therapists, six therapists noted that multidisciplinary team members did not understand the role of occupational therapy in this condition. Clients were therefore not referred, or not referred early enough to occupational therapy to prevent or reduce the disability and occupational dysfunction. Within the rehabilitation team, two participants perceived the understanding of the occupational therapy role was facilitated by the use of combined occupational and physiotherapy sessions.
Reported outcomes reflecting rehabilitation needs of children and adolescents with JIA addressed by current occupational therapy practice
Children and adolescents with JIA and their parents indicated that education (43%) was the most affected occupation requiring rehabilitation, followed by personal management (30%). They commented on deficits in social participation with both peers (24%) and teachers (5%). Intervention to address these needs were not reported in the occupational therapists’ treatment regime (Table 1), which prioritised personal management.
Condition-related factors reported reflecting rehabilitation needs for children and adolescents with JIA addressed by current occupational therapy practice.
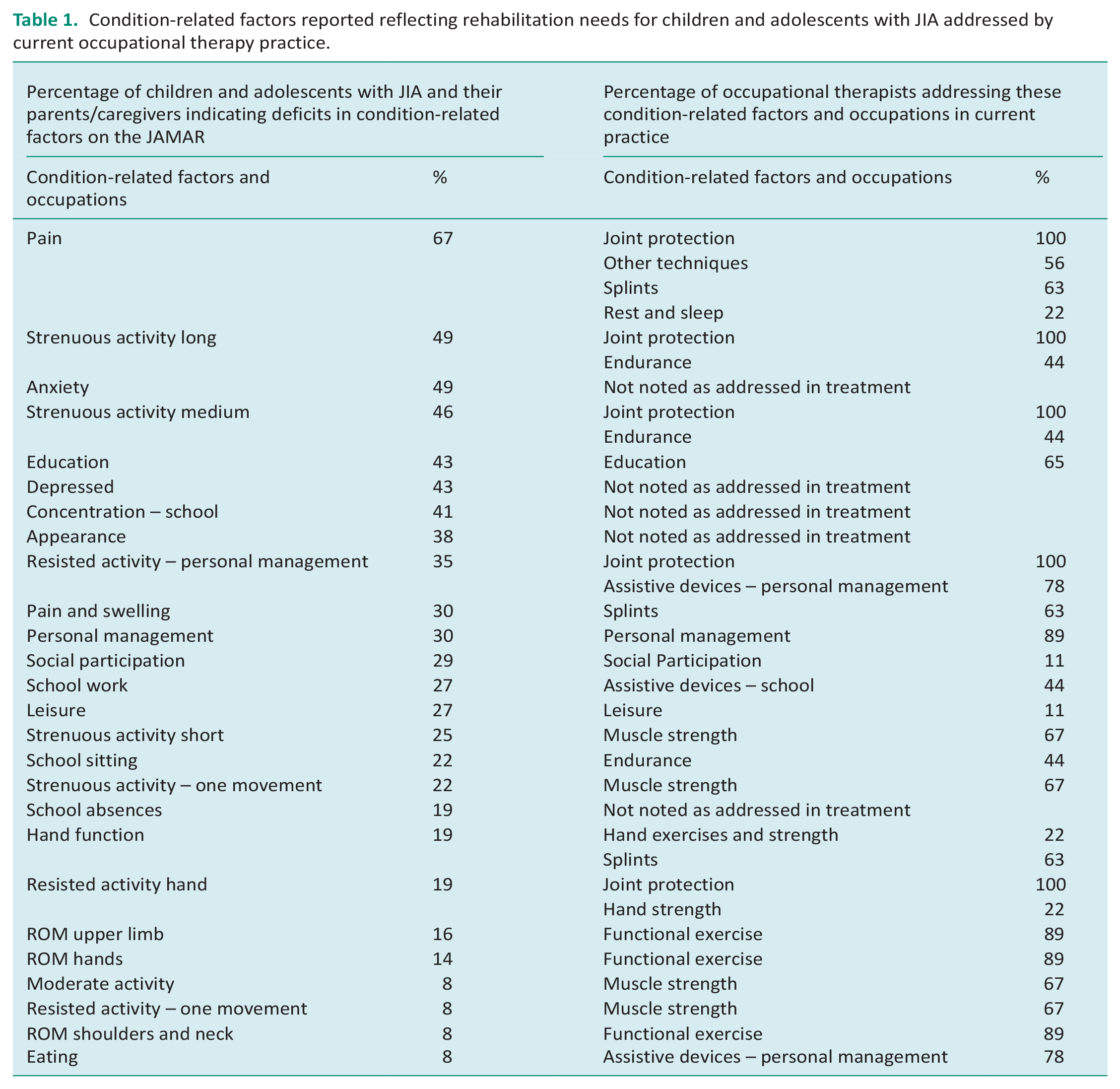
More than two-thirds of children and adolescents with JIA and their parents reported that pain was their greatest client factor deficit, whereas just less than half reported problems with long strenuous activity. While these deficits were addressed between 100 and 22% of the time by occupational therapy, anxiety, depression, concentration and appearance reported as a deficit by nearly half the clients with JIA were not addressed. Therapists focussed treatment on physical modalities.
Discussion
Children and adolescents with JIA (Part 1)
The majority of the children and adolescents with JIA in this study were between 11 and 14 years of age, which is supported by international literature that indicates the most common onset for the disease that occurs after 6 years of age, and most children who present for intervention are attending school (Martini and Lovell, 2010). The greater number of female participants was not unexpected since females have a higher predisposition to JIA (Scott and Brice, 2015). Although Caucasians have reported higher predisposition to JIA, the racial distribution of children and adolescents with JIA appeared to reflect the population groups who utilise the specialised public healthcare services in South Africa (Mhlanga and Garidzirai, 2020).
More participants (59%) in the current study reported active disease than 46.7% reported by Concha et al.(2021) in school going children and adolescents with JIA in Chile. This was possibly due to late referral and the higher incidence of disease activity reported in the South African population (Scott and Webb, 2014).
Even though more than half of children and adolescents with JIA in the current study reported active disease, with the exception of squatting and opening or closing a tap or a jar, it was reported that 75–92% of the participants had no difficulty with occupational performance. This supports the findings of van der Net et al. (2008) who indicated that although more than half of school going children and adolescents with JIA reported condition-related deficits, these do not correlate with their functional activities. These findings may reflect the ability of the children and adolescents to adapt or avoid activities to accommodate their limitations.
More than 50% of the children and adolescents in this study experienced school-related problems because of JIA. However, absenteeism from school was at less than 19%, which is similar to that reported in Nordic countries for children with JIA (Nordal et al., 2019). Activities requiring endurance were sometimes a problem for over 50%, whereas pain impacted the HRQoL for nearly 70% of the children and adolescents with JIA. As with other studies, social skills were the component least affecting HRQoL, whereas this was commonly impacted by feelings of nervousness, anxiousness, sadness or depression (van der Net et al., 2008; Ziff, 2016). This was supported by Ziff (2016), particularly in relation to decreased physical functioning and pain, which could affect the individual’s ability to cope as their physical limitations increase. This was particularly expressed in terms of limited leisure opportunities (Houghton, 2015).
Occupational therapists providing therapy for children and adolescents with JIA assessments (Part 2)
Although the institutions that participated in the study had access to multi-disciplinary services, in accordance with international guidelines, the approach to intervention at the tertiary hospital specialised rheumatology clinics in South Africa is predominantly curative rather than preventative and rehabilitative (Ziff, 2016). This may have impacted the services offered by occupational therapists since their perception is that the multi-disciplinary team members’ lack of understanding of their holistic and integrated role in the treatment of JIA, limited referrals for intervention. The majority of referrals were for splints and assistive devices. However, due to the higher levels of active disease and possibly the involvement of occupational therapists at the rheumatology clinics, the referral rate of 31% to 46% for rehabilitation services in the current study was higher than the 23% reported in a German study (Heinrich-Rohr et al., 2021) and the 7.8% in a study in Chile (Concha et al., 2021).
The occupational therapists confirmed that they did not use any screening tools or assessments specific to the assessment of JIA. This was attributed to the lack of comprehensive occupational therapy assessment tools for clients with JIA although Van Oort (2020) indicated a number of suitable standardised assessments that can be used with children and adolescents with JIA.
Occupational therapists described their prioritised role as addressing the physical client factors related to pain and strenuous or resisted physical activity. This is in line with recommendations reported in the literature (Rottermund et al., 2015; Van Oort, 2020; Ziff, 2016) and is consistent with the intervention aims described to improve function and mobility (Houghton et al., 2018). These client factors as well as HRQoL were identified as the outcomes most affecting function and the ability to lead an active lifestyle by children and adolescents with JIA and their parents. Intervention for functional participation in occupations was focussed on personal management with less emphasis on other occupations (Rottermund et al., 2015).
Outpatient therapy in the context of the tertiary hospitals is also usually limited to one session monthly or trimonthly when the child attends rheumatology clinic. The intervention therefore prioritised outcomes and related rehabilitation needs identified at the time of the visit. This may be impacted by the limited access to the child’s environmental context for therapists working at a specialist tertiary level and the inability of clients to access the hospital more frequently. In a country where 60% of people live below the low-middle-income-country poverty line (The World Bank, 2021) visits to the tertiary hospital, usually some distance from the child’s home, are not possible due to lack of transport and finances (Morris et al., 2021).
Reported outcomes reflecting rehabilitation needs of children and adolescents with JIA and current occupational therapy practice
The current occupational therapy services offered were not always consistent with the outcomes and rehabilitation needs as reported by JIA participants from the JAMAR assessment tool. Occupational therapists appear to have had to adopt a more reductionistic approach to the evaluation and treatment due to the restrictions imposed by the healthcare system within which they offer services.
The focus on intervention at tertiary hospital addresses clinical remission (Gentry et al., 2018), and referrals to occupational therapy appear to focus on immediate concerns in relation to joint pain, swelling and symptoms of active disease. Goals for improvement in client factors, reduction in disability and risk factors appear to have been prioritised in the limited time the occupational therapists have to provide intervention. They used a bottom-up biomechanical approach, which supports the deficits in pain, limited ability for resisted movement and range of motion, which could in turn affect the child’s ability to engage in activities (Secor-Turner et al., 2011). The full scope of occupational therapy services in terms of school assessments and psychosocial aspects, such as anxiety and depression, was not evident (Philpott et al., 2010) even though 19% of the children and adolescents with JIA reported issues with these components. The services the therapists provided were in line with the literature on the role of occupational therapy for children and adolescents with JIA, which also places limited emphasis on psychosocial intervention. Evidence for psychosocial intervention for this population is not clear, and peer group support, which has been reported as effective in addressing psychosocial issues in JIA, is not recommended as part of occupational therapy services by Van Oort, (2020).
The South African health service delivery policies advocate referral from tertiary hospitals to intervention in the child’s environment provided by ward-based primary healthcare outreach teams and integrated school health teams (Department of Education, 2001; Department of Health, 2020). The referral pathway to lower levels of care for more regular therapy is complex and not well defined with very few therapists working at the community level. Issues with referral pathways affect holistic intervention for clients in the confines of a symptom-based approach in a chronic condition such as JIA, for clients who attend specialist outpatient clinics at a tertiary hospital. Since no therapists reported referral to lower levels of service delivery and they therefore relied on home programmes to achieve most therapy goals. Referral to district or primary healthcare services for further context-based home and school-related intervention (Department of Health, 2020) may resolve these issues.
Almost half of the occupational therapists reported that they did not provide intervention for school-related occupations although the majority of clients with JIA were of school going age. The lack of referral to the Department of Education for occupational therapy services for children above the age of 6 years presents the greatest limitation. Even though occupational therapists are employed in some public special needs schools, this does not provide services for clients with JIA, who often attend mainstream schools. Children and adolescents attending mainstream schools rely on very limited occupational therapy input from a district team to provide support services. To address this gap in service delivery, the Education White Paper 6 policy highlighted the need for intersectoral collaboration between education, health and social services in assisting children and adolescents with disabilities to overcome barriers to learning by the provision of appropriate care (Department of Education, 2001).
Even, without this collaboration available occupational therapy services, should be extended to ensure problems experienced by clients with JIA in schools, such as physical symptoms, delayed developmental milestones and lack of psychosocial support, are addressed (Rottermund et al., 2015; Ziff, 2016).
Limitations of the study
Limitations of the study included the small sample sizes. These were dependent on the number of clients with JIA who attended the clinics, and only clients who met the inclusion criteria of having a recent primary diagnosis of JIA were invited to participate in the research study. Clients who had comorbid conditions and other rheumatic conditions were not considered. The small number of therapists who treated children with JIA also resulted in a small sample size meaning the findings cannot be easily generalised to other treatment contexts.
In order to compare the rehabilitation needs of children and adolescents with JIA international recommendations for occupational therapy and comments from the nine participants were used and may not clearly reflect the link between rehabilitation needs and therapy for condition-related factors and occupations in current practice.
Conclusion
This study highlights the provision of rehabilitation for children and adolescents with JIA at a tertiary level in terms of providing holistic occupational therapy intervention (Gentry et al., 2018) at this level of healthcare in South Africa. Most services, such as splinting, assistive devices, pain management and functional exercise, provided by occupational therapists in tertiary hospitals addressed physical client factors identified as outcomes needing rehabilitation by clients with JIA and their parents. Although occupational therapy services provided were in line with international recommendations for JIA, the holistic occupational therapy management consistent with the philosophy of the profession by the inclusion of psychosocial factors and school-related deficits and HRQoL could not always be accommodated in a tertiary healthcare setting (Gentry et al., 2018). Current services offered to clients with JIA may not be optimal due to a lack of focus on all occupations since some rehabilitation needs of the children and adolescents with JIA may not be addressed. Poor referral pathways to address more comprehensive intervention within the health and educational systems meant that community-based services were not accessed by these clients.
Key findings
Occupational therapy intervention for JIA in the South African public healthcare specialist context is constrained by a number of factors.
There is a need for researched clinical guidelines for a holistic occupational therapy intervention for JIA provided at a tertiary level.
Changes are required in in terms of referral pathways and access to occupational therapy at a community level.
What the study has added
While occupational therapy services in the South African public healthcare specialist context provide intervention recommended for JIA, these do not address all reported rehabilitation needs of children and adolescents with JIA.
Footnotes
Acknowledgements
None.
Research ethics
Ethical approval for this study was obtained from the Human Research Ethics Committee (Medical) of the University of the Witwaterstand, Johannesburg.
Consent
Parents or legal guardians provided signed informed consent and the children and adolescents provided informed assent for participation in the study. For the therapists, informed consent was indicated by the completion and return of the survey questionnaire. No names or identifying data were collected.
Patient and public involvement data
During the development, progress and reporting of the submitted research, patient involvement in the research was included in conducting of the research.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) declared no financial support for the research, authorship, and/or publication of this article.
Contributorship
As a postgraduate student, DM researched literature and conceived the study and was involved in patient recruitment and data collection. LJ was the academic supervisor directly involved supervised the project and was involved in protocol development, gaining ethical approval and assisted with the research process. DF completed the data analysis and with PdW revised and updated literature and conceived the first draft of the manuscript, as per university policy or the student. All authors reviewed and edited the manuscript and approved the final version of the manuscript.