
Abstract
Introduction:
Sensory approaches are often used by Occupational Therapists working with clients with a severe or profound and multiple learning disabilities (SLD/PMLD). The aims of this review were to synthesise the outcomes of sensory approaches for adults with an SLD/PMLD and describe the key intervention components.
Method:
A mixed methods literature review of three databases was completed to identify studies where sensory approaches were used for clients with an SLD/PMLD. Peer-reviewed research articles published between January 1990 and April 2021 were included. Data quality was assessed using the Mixed Methods Appraisal Tool. A convergent-segregated approach to synthesis was taken, including thematic analysis of qualitative data and a narrative review of quantitative data.
Results:
Eighteen studies were included. Positive outcomes were reductions in challenging behaviour, stress and improved engagement, attention and communication. Three themes emerged, suggesting important components of sensory approaches for clients with an SLD/PMLD: matching sensory stimuli to the needs of the individual, sensory integration therapists and caregivers as facilitators and increased intervention duration and frequency.
Conclusion:
Evidence suggests that sensory approaches support positive social, emotional and cognitive outcomes for individuals with an SLD/PMLD. Essential features of sensory approaches for this client group are sensitive use of sensory stimuli, skilled facilitators and more intensive intervention protocols.
Introduction and literature review
People with a severe learning disability (SLD) or profound and multiple learning disabilities (PMLD) have a severely limited ability to understand and communicate and a range of other disabilities restricting their participation with others and their environment. These disabilities often include movement, postural and sensory impairments, complex medical conditions (such as epilepsy and dysphagia) and behaviours perceived as challenging, such as self-injury (Doukas et al., 2017).
To overcome barriers to participation in everyday activities, people with an SLD/PMLD require specialist multidisciplinary health and social care teams trained to manage their complex needs (Doukas et al., 2017) and when this is not available, low expectations, discrimination and restrictive practices to manage behaviour persist (Mansell, 2010; McGill and Breen, 2020). The cultural shift required in health services supporting people with an SLD/PMLD is reflected in recent clinical guidance, core training standards and national initiatives such as STOMP (stopping over medication of people with a learning disability, autism, or both) and the Raising our Sights report (Mansell, 2010). In these key drivers of change, professionals are challenged to implement person-centred interventions, including sensory approaches, to enable people with learning disabilities to participate actively in all aspects of daily life (Doukas et al., 2017; National Institute for Health and Care Excellence, 2015, 2018).
The term ‘sensory approaches’ was adopted by Scanlan and Novak (2015) to describe a range of sensory interventions from multisensory rooms to sensory activities, sensory diets and specific sensory integration (SI) interventions, which share the common aim of providing sensory input to support emotional regulation and arousal levels. Although encompassed in this definition, SI offers a distinct intervention whereby trained SI therapists select activities with the ‘just-right challenge’ based on clients’ unique sensory integration needs to elicit adaptive responses (Bundy and Szklut, 2019). Proponents of SI call for researchers to make a clear distinction between SI and other sensory approaches (Schoen et al., 2020). In acknowledgement of this, the present review includes SI under the ‘sensory approaches’ concept but discusses SI intervention and outcomes separately.
Whilst there is limited research into the effectiveness of sensory approaches for adults with an SLD/PMLD, there has been research on the effectiveness of sensory approaches across the learning disability (LD) spectrum. There are, however, conflicting conclusions within this evidence base. Whilst some systematic reviews report that sensory approaches improve behaviour, mood and engagement (Breslin et al., 2020; Chan et al., 2010) others report no significant outcomes (Leong et al., 2015). In the context of specialist multidisciplinary teams, however, sensory approaches have been found to be critical components of multi-element positive behavioural support programmes for learning disabilities and challenging behaviour (McGill and Breen, 2020).
Occupational therapists who commonly use sensory approaches for adults with an LD to increase participation and social interactions (Blaskowitz et al., 2021) may be well-placed to deliver similar outcomes for adults with an SLD/PMLD. At the same time, there is a lack of good quality evidence to justify the use of sensory approaches or explain the mechanisms by which they affect this client group (Breslin et al., 2020). The Royal College of Occupational Therapists recently mandated that all OTs must critically consider the evidence prior to implementing sensory approaches (Royal College of Occupational Therapists (RCOT), 2021). There is therefore a strong justification for conducting research into sensory approaches for the SLD/PMLD population.
The aim of the review, therefore, was to assess the evidence for sensory approaches in the treatment of adults with an SLD/PMLD. The specific aims were: (1) to collate and describe the main outcomes of sensory approaches for adults with an SLD/PMLD and (2) to describe the key components and rationales underpinning these sensory approaches.
Method
Studies were included in the review if they satisfied the following inclusion criteria:
Peer-reviewed articles of primary research into sensory approaches written in the English language and published from the year 1990 to the present.
At least 50% of participants were over eighteen years old.
The study sample included individuals with an SLD/PMLD.
Interventions within the study had sensory strategies as the main component of the intervention.
Excluded studies were:
Articles or opinion pieces and grey literature without a rigorous research study design.
At least 50% of participants were under the age of eighteen.
Studies that included adults with an LD but did not specify the severity of the LD.
A search of the literature was completed up to the date of 6th April 2021 using CINHAL, PubMed and PsycINFO databases and key search terms pertaining to the concepts of sensory approaches and learning disabilities. The search terms were derived from key words and titles in articles retrieved in a preliminary scoping review of the literature and refined in consultation with a subject librarian and using database specific thesaurus terms (see Supplemental Appendix A for the full list of search terms).
Search terms used for Concept 1 ‘sensory approaches’ were combined with search terms for Concept 2 ‘learning disabilities’ using Boolean Operator ‘AND’ and the Boolean operator ‘OR’ was used to link search terms within each concept. The following search string was used to complete each search: (Sensory OR (all concept 1 terms)) AND (Learning Disabilit* OR (all concept 2 terms)) AND Adult*.
After an initial search (n = 395), filters were applied to include only journal studies from 1990 to 2021, with adult participants, published in the English language. Following the removal of duplicates (n = 140), 120 studies were reviewed. The independent researcher selected studies for inclusion in the final review in a two-step process. Firstly, the title and abstracts of the remaining studies were screened, and the exclusion and inclusion criteria were applied (n = 19). The full texts of the 19 remaining studies were then reviewed, resulting in exclusion of one study due to reporting the reinforcing properties of individual sensory stimuli rather than outcomes relating to a sensory approach (Matson et al., 2004). In total, 18 studies were included in the review (see Figure 1). Table 1 provides an overview of the included studies:
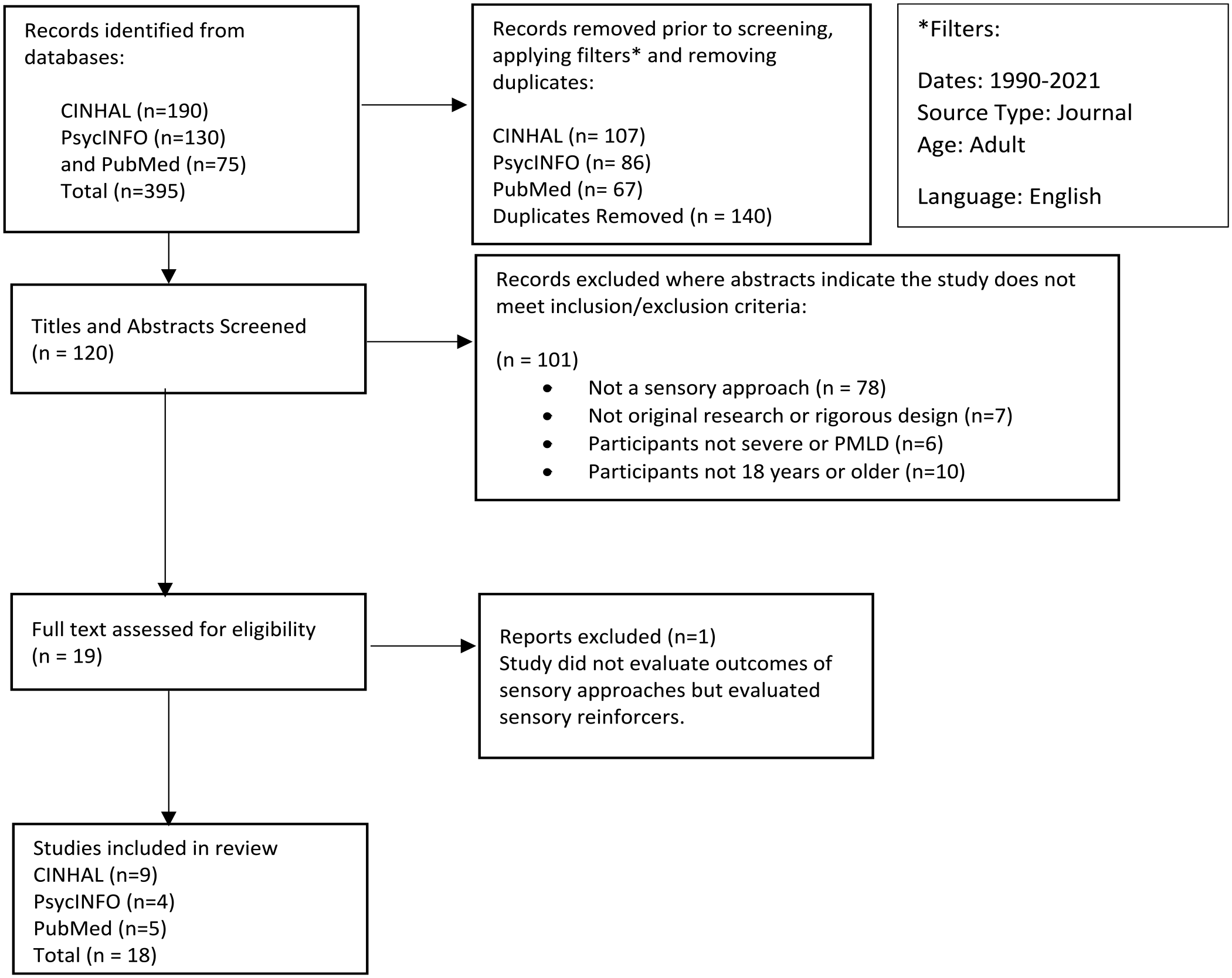
Study selection process.
Overview of included studies.
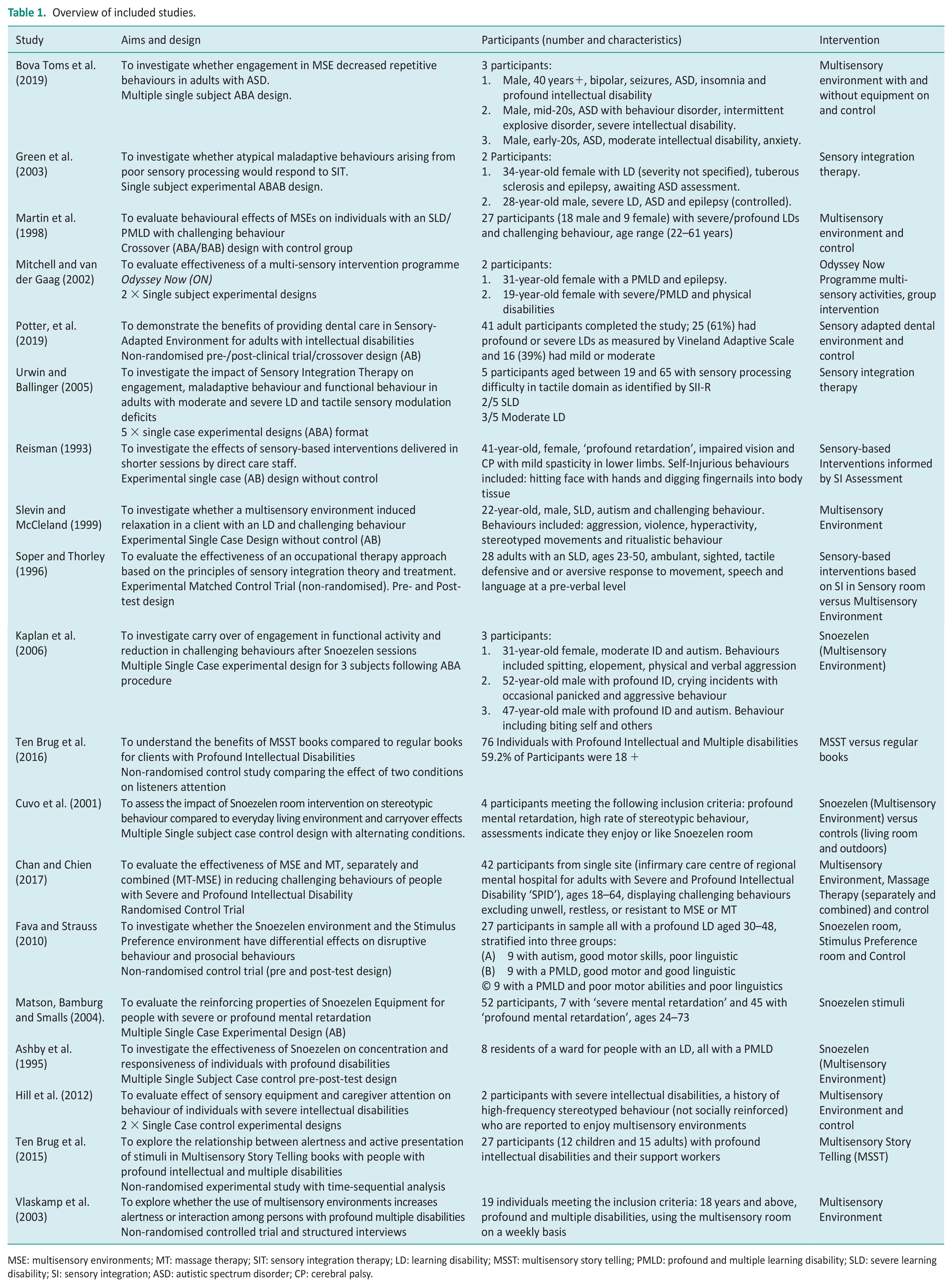
MSE: multisensory environments; MT: massage therapy; SIT: sensory integration therapy; LD: learning disability; MSST: multisensory story telling; PMLD: profound and multiple learning disability; SLD: severe learning disability; SI: sensory integration; ASD: autistic spectrum disorder; CP: cerebral palsy.
The quality of the included studies was appraised using the Mixed Methods Appraisal Tool (MMAT; Hong et al., 2018). Each study was categorised using the MMAT algorithm then critically appraised according to its design using the MMAT criteria. The studies were evaluated by comparing the ratings for each criterion, which informed interpretation of the results. Table 2 illustrates how many studies failed to demonstrate appropriate measures, complete outcome data or account for confounding variables. Since the aim of the review was descriptive rather than evaluative, no studies were excluded following critical appraisal.
Quality appraisal of review studies using the MMAT (Hong et al., 2018).

Data collection process
Qualitative and quantitative data were extracted from included studies using separate data forms developed by the researcher (see Supplemental Appendix B). For all studies, data extracted included details about the study aims and methods, participants and sampling, intervention approach, context and main outcomes reported by authors. For quantitative studies (and quantitative components of mixed methods studies), additional data extracted included more detailed information on intervention outcomes. For qualitative studies, additional data extracted included descriptions of intervention components and implementation.
Data synthesis
A narrative synthesis of both qualitative and quantitative outcomes, following guidance from Popay et al. (2006) and Heyvaert et al. (2017), was completed by the researcher in the following stages. Firstly, studies were clustered by intervention type into three main groups to aid data analysis: multisensory and sensory adapted environments (MSEs/SADEs), Multisensory Stories and Activity Programmes and sensory integration therapy (SIT). Quantitative data from the results sections of included studies were extracted and qualitised into textual descriptions. Simultaneously, qualitative data about the implementation and components of the interventions were extracted from the methods and results sections of each study. The data were then analysed thematically through coding and constant comparison of themes (Popay et al., 2006).
Results
The included studies were conducted in community residential settings (n = 8), inpatient settings (n = 6), day services (n = 3) and a clinic (n = 1). All studies included individuals with an SLD/PMLD, therapists and support workers. Eleven studies used MSEs/SADEs, four studies used SIT and three studies used a Multisensory Activity Programme or Multisensory Stories (MSSTs). No studies with a qualitative design were retrieved. Sixteen of the included studies had a quantitative design with the majority being experimental before and after case studies (n = 9), then non-randomised trials (n = 6) and a single randomised controlled trial (n = 1). There were also two mixed methods studies included.
Methodological quality
Overall, the quality of the studies and evidence included in the review was limited, in part due to the methodological challenges of evaluating complex sensory approaches and interpreting the responses of individuals with an SLD/PMLD. Table 2 provides an overview of quality findings for each study using the MMAT (Hong et al., 2018). Further detail on quality issues with included studies is provided in the discussion section.
Synthesis
Outcomes of sensory-based interventions
Challenging behaviour
Improvements in clients’ behaviours during or following sensory approaches were reported in eight out of the eleven studies of MSEs and SADEs. These included reduced frequency of stereotyped, repetitive, self-injurious, agitated and aggressive behaviours (Bova Toms et al., 2019; Chan and Chien, 2017; Cuvo et al., 2001; Fava and Strauss, 2010; Hill et al., 2012; Kaplan et al., 2006; Potter et al., 2019; Slevin and McClelland, 1999). Whilst overall improvements in behaviour were reported in most studies of MSEs and SADEs, several indicated that positive outcomes were absent for some participants (Bova Toms et al., 2019; Kaplan et al., 2006), inconsistent across sessions for others (Slevin and McClelland, 1999) and had limited carryover (Fava and Strauss, 2010). Moreover, Martin et al. (1998) found no significant impact of MSE on behaviour compared with a control condition.
All of the SIT studies found behaviour improvements during or following SI intervention, including reductions in the frequency, intensity or duration of screaming and shrieking, self-injurious, self-stimulatory and compulsive behaviours (e.g. PICA) and physically aggressive behaviours (Green et al., 2003; Reisman, 1993; Soper and Thorley, 1996; Urwin and Ballinger, 2005). Not all improvements in behaviour, however, occurred consistently across the SIT studies. Similar to the MSE studies, there were marked variations between individual client responses (Urwin and Ballinger, 2005). Green et al. (2003) also concluded that SI may positively influence challenging behaviour but has a limited impact on entrenched motor stereotypies.
A positive effect on behaviour was reported from staff interviews about the Multisensory activity programme, Odyssey Now (Mitchell and Van der Gaag, 2002). Absence of clear procedures for qualitative data collection and analysis, however, makes it difficult to determine the credibility of this finding.
Mood
Of the eighteen studies included, only three reported on mood outcomes. In two studies, an alleviation of physiological stress and anxiety was demonstrated through significant reductions in agitated behaviours, pulse rate and blood pressure following exposure to MSE and SADE (Potter et al., 2019; Slevin and McClelland, 1999). The highest quality evidence of the impact of MSEs on mood can be found in the randomised controlled trial by Chan and Chien (2017), where significantly lower occurrences of agitated (‘active-alert’) behaviours were reported in MSE conditions compared with controls. Interestingly, however, this study reported no significant differences in physiological stress measures.
Engagement
There was some evidence from studies that the engagement of people with an SLD/PMLD is enhanced by MSEs. Results should be interpreted cautiously, however, as there were limited reliable methods for detecting and measuring the subtle indicators of engagement in participants with an SLD/PMLD.
Ashby et al. (1995) and Kaplan et al. (2006) measured engagement effects by administering controlled functional and puzzle tasks before and after MSE sessions and showed improvements in performance from baseline after treatment. Cuvo et al. (2001) and Hill et al. (2012) both used operational definitions of ‘engagement’ and structured observations to show that MSEs are more effective at promoting engagement in people with an SLD/PMLD compared with a normal living environment. Difficulties controlling for confounding variables affecting engagement, such as caregiver attention, were reported in several studies. Hill et al. (2012) overcame this problem by evaluating high and low caregiver attention conditions across settings, showing that when attention effects are accounted for, MSEs retain their impact or ‘additive effect’ on engagement. Vlaskamp et al. (2003), by way of contrast, found no significant difference between activity levels in MSE versus normal living environments.
SIT studies demonstrated engagement outcomes by measuring smaller units of goal-directed activity, known as ‘adaptive responses’ in Ayers’ Sensory Integration Theory (Bundy and Szklut, 2019). In two SIT studies, Goal Attainment Scaling scores measuring functional and adaptive response outcomes were significantly improved after SIT, although not across the sample (Green et al., 2003; Urwin and Ballinger, 2005). Significant score improvements in The Ayers Scale of Adaptive Responses following SIT were also noted (Soper and Thorley, 1996). Reisman (1993, p. 409) also provided qualitative evidence from a single case study indicating that ‘[. . .] adaptive responses were elicited in social, motor and vocalisation activities immediately after the initial 5 minutes of sensory calming activities’.
In the Multisensory Activity Programme Odyssey Now, the main quantitative outcome reported was time spent engaging with people and objects (Mitchel and Van der Gaag, 2002). Authors of this study found that engagement increased to statistically significant levels for the first participant and was detected as a data trend only for the second.
Attention and communication
Attention and communication outcomes featured prominently in all three Multisensory Activity Programme and Storytelling studies. Following participation in the Odyssey Now programme, significant increases in communication behaviours such as eye contact, smiling, pointing, sharing and co-operating were reported (Mitchell and Van der Gaag, 2002). In the two studies MSSTs, the MSSTs were shown to improve foundational communication skills of alertness and joint attention, with the greatest impact found when storytellers presented stimuli interactively (Ten Brug et al., 2015, 2016).
Whilst communication outcomes were not the main findings reported in MSE and SIT studies, two MSE studies did report increased communication attempts during sessions such as making eye contact, smiling, responding through gesture, signs, or touch (Fava and Strauss, 2010; Hill et al., 2012). Qualitative descriptions in SIT studies, such as the observation, ‘The subject smiled, laughed aloud, maintained eye contact and imitated sounds and motions with the staff’ (Reisman, 1993, p.408), also provide some evidence that SIT may enhance communication.
Key components of sensory-based interventions
Analysis of qualitative data from all studies led to three themes describing the key components of sensory approaches for clients with an SLD/PMLD: the sensory environment, apparatus and stimuli; facilitation of sensory approaches and the dosage of sensory approaches (see Table 3). A narrative summary for each of these themes is presented, highlighting the similarities and differences across each of the intervention subcategories.
Themes and supporting evidence for components of sensory-based interventions.
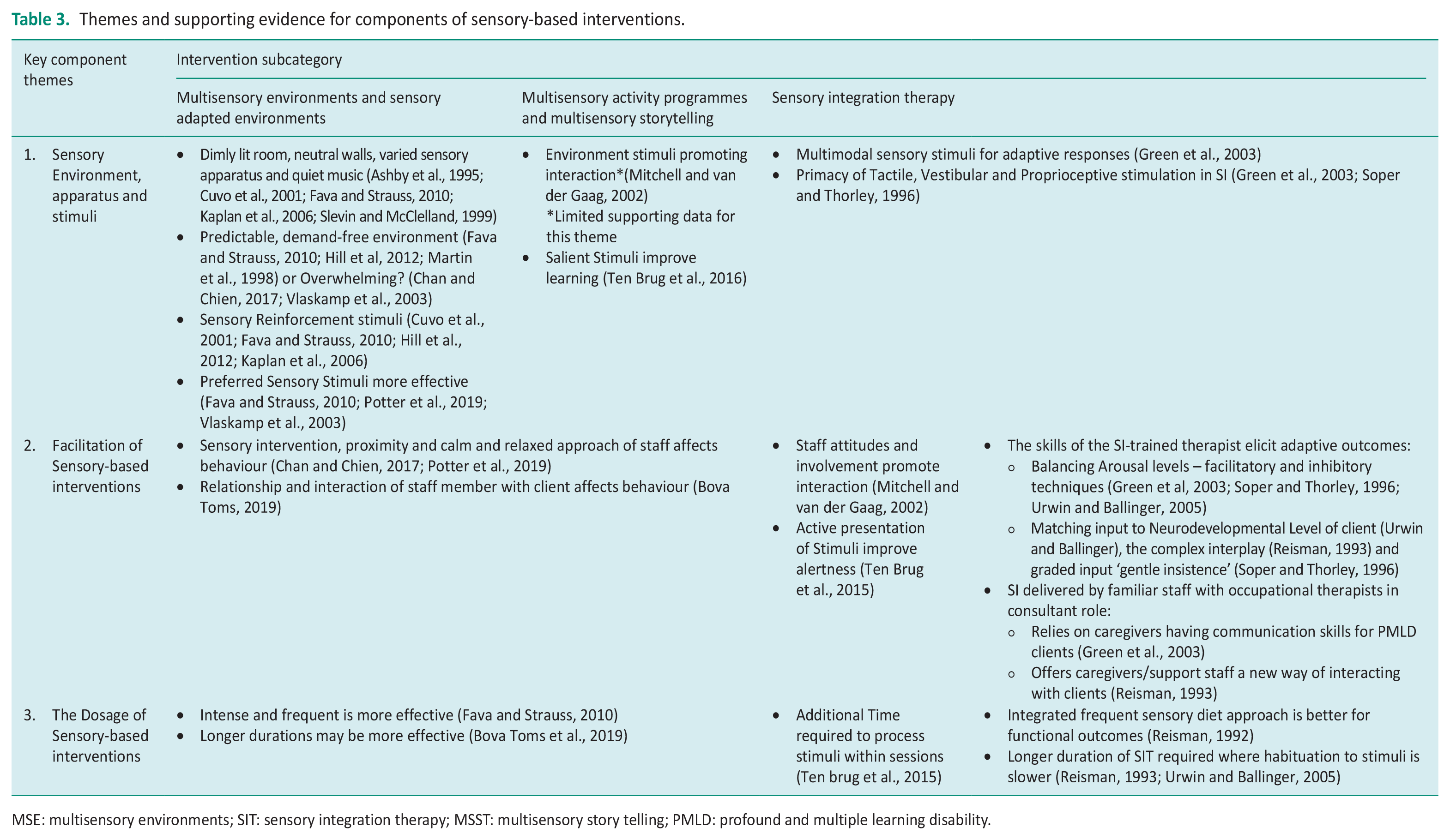
MSE: multisensory environments; SIT: sensory integration therapy; MSST: multisensory story telling; PMLD: profound and multiple learning disability.
The sensory environment, apparatus and stimuli
Common features of the MSE were dim lighting, neutral-coloured walls, a variety of specialist sensory apparatus distributed throughout the room and sometimes quiet ambient background music or nature sounds. Equipment offered opportunities for visual, tactile, proprioceptive and auditory stimulation and occasionally olfactory and vestibular stimulation (Ashby et al., 1995; Bova Toms, 2019; Chan and Chien, 2017; Cuvo et al., 2001; Fava and Strauss, 2010; Hill et al., 2012; Kaplan et al., 2006; Martin et al., 1998; Slevin and McClelland, 1999).
Theories on how the general MSE impacts on clinical outcomes varied across studies. Some authors suggested that the MSE elicits positive outcomes because it offers clients with an SLD/PMLD a predictable, demand-free environment in which to explore (Fava and Strauss, 2010; Hill et al., 2012). Conversely, others concluded that the MSE room is restrictive and overstimulating. Vlaskamp et al. (2003, p.141), for example, reported that the stimuli in the MSE led to participants, ‘cut[ting] themselves off from an environment experienced as overwhelming’. Chan and Chien (2017) concurred that the MSE is overwhelming but explain that this can be beneficial for individuals with an SLD/PMLD, as their passive response to the environment allows for ‘waves of alertness,’ promoting better attention overall.
Other studies hypothesised that better clinical outcomes may be attained if sensory stimuli within the MSE were tailored to the individual’s needs rather than presented as a general array (Potter et al., 2019; Vlaskamp et al., 2003). One study tested this idea empirically and found that a stimulus preference condition, where clients with an SLD/PMLD were supported to select stimuli, led to increased prosocial behaviours compared to the general MSE (Fava and Strauss, 2010). Other studies theorised that specific stimuli within the MSE provide sensory reinforcement for positive behaviours, by offering an alternative to self-stimulatory, repetitive and stereotypical behaviours (Fava and Strauss, 2010; Hill et al., 2012; Kaplan et al., 2006). For repetitive movements, however, Cuvo et al. (2001) suggest that the outdoor environment and physical activity may provide better reinforcement than the MSE.
Fewer of the SIT and Multisensory Activities studies discussed the sensory environment as a key intervention component, however, some highlighted that the types of sensory stimulation used may have affected outcomes. In SIT studies, multimodal stimulation – in particular, the skilful implementation of vestibular, proprioceptive and tactile stimulation input through specialist apparatus – was linked to positive, adaptive responses (Green et al., 2003; Soper and Thorley, 1996). In the MSST studies, Ten Brug et al. (2016, p.1052), attributed the improved attention outcomes of participants listening to MSSTs to the unique, ‘handpicked’, sensory stimuli chosen for the stories. Similar to the stimulus preference concept proposed by Fava and Strauss (2010), Ten Brug et al. (2016) explained that stimuli that are more salient or motivating to the individual, gained the most attention and likely resulted in better story apprehension.
Facilitation of sensory approaches
The skill of the therapist or facilitator, how they directed individuals to interact with stimuli, and interactions between facilitators and participants during sensory approach sessions were all noted to affect outcomes.
Facilitation was frequently described as a critical component within SIT studies, with positive clinical outcomes attributed partly to the application of SI skills and principles by SI-trained occupational therapists, which included: the careful use of facilitatory (alerting) and inhibitory (calming) techniques to balance arousal levels; matching sensory input to the neurodevelopmental level of the client and interpreting sensory responses and providing client-led intervention (Green et al., 2003; Reisman, 1993; Soper and Thorley, 1996; Urwin and Ballinger, 2005).
Whilst all four SIT studies asserted the importance of a SI-trained practitioner, perspectives on the level of training required and the role of these practitioners varied. Soper and Thorley (1996), for example, emphasise the importance of SI-trained practitioners providing intervention with the supervision of an experienced SI therapist. Reisman (1993), conversely, argues for a more pragmatic model of SIT, where SI activities are designed and overseen by SI-trained OTs but delivered directly by familiar support workers.
Although SIT studies focused on specialist SI facilitation skills, they also noted the positive influence that effective facilitator-client communication had on session outcomes (Green et al., 2003; Reisman, 1993). The importance of well-honed skills in responding to the communication attempts of individuals with an SLD/PMLD was also reflected across other studies of sensory approaches. Within multisensory programmes and MSEs, staff attitudes and their skills in presenting sensory stimuli interactively were linked to improved interaction, alertness and behavioural outcomes (Bova Toms et al., 2019; Mitchell and Van der Gaag, 2002; Ten Brug et al., 2015).
To a lesser extent, the effect of sensory activities and environments on caregiver or provider stress levels was also reported to affect outcomes. The sensory activity of massage therapy within an MSE, for example, was noted to have the potential to improve relationships between individuals with an SLD/PMLD and their support staff (Chan and Chien, 2017). Similarly, the calming effect of stimuli on patients with an SLD/PMLD in the SADE was hypothesised to improve the stress levels of the dental provider and subsequently improve patient interactions (Potter et al., 2019).
The dosage of sensory approaches
The dosage – referring to the length, frequency and overall duration of sensory approach sessions offered to clients – differed across studies and intervention subcategories.
In MSE studies, sessions lasted between 15 and 30 minutes but were offered at different frequencies: daily (Slevin and McClelland, 1999); three times a week (Ashby et al., 1995; Fava and Strauss, 2010); twice a week (Bova Toms et al., 2019; Chan and Chien, 2017; Kaplan et al., 2006; Martin et al., 1998) and weekly (Hill et al., 2012). The duration of MSE interventions ranged between seven to sixteen weeks in total, although in several studies overall duration was dependent on contextual factors and participant responses (Bova Toms et al., 2019; Cuvo et al., 2001; Kaplan et al., 2006).
In multisensory activity programmes, the number of sessions were fixed in all studies, with the Odyssey Now programme being offered over eight weeks (with no description of the frequency or length of sessions) and MSSTs being offered twice a week for five weeks.
For the SIT subcategory, there was greater variation in session length and intervention duration between studies, possibly reflecting the more individualised, client-led nature of SIT. Session durations ranged from 10 minutes to 1 hour and were offered once (Soper and Thorley, 1996), twice or three times a week (Green et al., 2003; Urwin and Ballinger, 2005) with the exception of Reisman’s study, where sessions were integrated into the clients’ daily activity schedules, making it difficult to determine session length and frequency. Reisman (1993, p.409) argued that distributing SIT sessions throughout the day in a ‘sensory diet’ is more effective for people with an SLD/PMLD because it prevents overstimulation and supports carryover effects in daily routines. Duration of intervention in the older SIT studies was long at seven and nine months, respectively (Reisman, 1992; Soper and Thorley, 1996) compared just four weeks in newer studies (Green et al., 2003; Urwin and Ballinger, 2005).
Across the three intervention subcategories, there was some consensus that a longer duration of sensory approach treatment may be beneficial, allowing clients with an SLD/PMLD habituate to and process sensory stimuli (Reisman, 1993; Ten Brug et al., 2015; Urwin and Ballinger, 2005) and adjust to sensory environments in order to maintain gains outside of sessions (Bova Toms et al., 2019; Fava and Strauss, 2010). Some studies also advocated that intense and frequent intervention produces enhanced behavioural and functional outcomes (Fava and Strauss, 2010; Reisman, 1993).
Discussion and implications
Results provide some limited evidence that sensory approaches could be beneficial in the care and treatment of adults with an SLD/PMLD. Potential outcomes of sensory approaches for this client group are reductions in behaviour that challenges, reduced signs of stress and agitation, increased engagement in activities during or immediately following intervention and increased signs of communication and attention within sessions. Reporting of these outcomes was rarely reliable, however, owing to observer bias and paucity of measurement tools sensitive enough to capture non-verbal responses. Moreover, outcomes reported did not apply uniformly to all participants and therefore results could not be generalised.
Notwithstanding these limitations, the studies suggest ways therapists can maximise the effectiveness of sensory approaches and give direction for future research.
Many studies within the review indicate that the success of sensory approaches depends on how multisensory environments, sensory stimuli and apparatus are selected and presented to individuals with an SLD/PMLD (Cuvo et al., 2001; Fava and Strauss, 2010; Green et al., 2003; Hill et al., 2012; Kaplan et al., 2006; Potter et al., 2019; Soper and Thorley, 1996; Vlaskamp et al., 2003). Not all behaviours are driven by sensory needs and certain repetitive or self-stimulatory behaviours warrant distinct forms of sensory input to elicit outcomes (McGill and Breen, 2020). Providing the appropriate type of sensory reinforcement for the individual’s need is an important component of effective intervention. Other reviews echo this theme, calling for better articulation of the underlying mechanisms of sensory approaches, aiding practitioners’ understanding of how to use sensory stimuli and who might benefit most from intervention (Bodison and Parham, 2018; Breslin et al., 2020). Prior to selecting sensory approaches for a client with an SLD/PMLD, therefore, it is recommended that therapists use standardised SI assessment tools to determine the person’s sensory needs and tailor therapy accordingly.
A further recommendation from the review is to consider using stimulus preference assessment tools with people with an SLD/PMLD to select the apparatus and stimuli used in sensory approaches. Choosing salient stimuli that motivate the individual with an SLD/PMLD, has been shown to enhance outcomes and hypothesised to be more effective than generalised sensory equipment provision. To implement this recommendation, therapists could use tools such as the multiple stimulus with or without (MSW/MSWO) replacement, consult and involve familiar caregivers of the individual in selecting stimuli or consider other ways to involve individuals with an SLD/PMLD to make choices.
It is also clear from the review that the skill of the facilitator significantly impacts on the outcomes of sensory approaches for people with an SLD/PMLD. SIT studies articulated the advantages of employing trained SI therapists to deliver or oversee sensory approaches because of their in-depth knowledge of sensory behaviour and unique skills in interpreting sensory responses of individuals with an SLD/PMLD. May-Benson and Kinnealey (2012) explained that SI skills are especially advantageous where clients are unable to learn about or self-regulate their sensory difficulties, which is frequently true for the SLD/PMLD population. Whilst the benefits of a SI-trained therapist over untrained facilitators were not specifically evaluated here, it does present an important direction for future research.
Several of the studies in the review not only advocate for SI therapist consultation but also point to unique skills and advantages of involving caregivers in sensory approaches for adults with an SLD/PMLD. At the time of Reisman’s study (1993, p.410), involving direct care staff in the delivery of SIT to individuals with an SLD/PMLD was a ‘new model’, which had the potential to ‘enhance the quality of treatment given by the staff whilst maximising scarce therapist time’. In recent years, key proponents of SIT have gone further, stipulating caregiver involvement as essential for developing goals that reflect and support daily functioning (Bundy and Szklut, 2019).
Whilst the review was unable to provide guidance on the optimal ‘dosage’ of sensory approaches, there was some agreement that the duration of sensory interventions and stimulus exposure would need to be longer, more frequent and intense for people with an SLD/PMLD than for other client groups to account for delayed processing and slower habituation. This finding echoes the recommendations made in a review of sensory stimulation in traumatic brain injury (TBI) settings (Padilla and Domina, 2016) and reflects similarities in the clinical presentation and sensory processing needs of people with an SLD/PMLD and TBI. These similarities suggest there may be particular benefits to the SLD/PMLD population to conducting ‘translational’ research across the disciplines of neuroscience and SI.
Limitations
There were several limitations impacting on the quality of all studies and the credibility of the findings presented. Many studies had small sample sizes, used convenience sampling or did not give adequate detailed descriptions of participants, limiting the generalisability and clinical utility of the findings. As a result of participant withdrawal for medical or ethical reasons, several studies also had incomplete outcome data, further reducing the reliability of the findings (Bova Toms et al., 2019; Reisman, 1993; Soper and Thorley, 1996; Ten Brug et al., 2015, 2016).
The validity and sensitivity of observational checklists and measures of participants’ responses was also a major limitation. Finding suitable measures and trained observers to sensitively interpret the responses of individuals with an SLD/PMLD is a challenge for researchers. The complex comorbidities of the SLD/PMLD population alongside the naturalistic settings in which sensory approaches are conducted also make it difficult for researchers to control confounding variables. Only a few studies mitigated the effects of confounding variables using control groups, observer blinding or sensitive interpretation of findings (Chan and Chien, 2017; Green et al., 2003; Potter et al., 2019). The designs of these studies would be beneficial to use as blueprints for future studies of sensory approaches.
There were also methodological limitations to the present review process. Guidelines for conducting reviews recommends at least two reviewers to minimise error and selection bias. Due to funding and time constraints, however, the present review was completed by one independent researcher. Another limitation was the small number of databases used, which may also have resulted in the omission of key studies. It would be beneficial for future reviews to complete more exhaustive searches for literature using other relevant research databases, hand-searching of key journals and screening of bibliographies to avoid overlooking potentially relevant studies. Finally, due to the paucity of studies including only adults with an SLD/PMLD, studies with heterogenous samples were included, which could reduce the validity of the findings.
Notwithstanding these limitations, the present study did identify common themes across a broad range of sensory approaches, which could inform how future interventions are delivered to adults with an SLD/PMLD. In addition, the study raises awareness of the methodological challenges and alternative approaches that can be used to evaluate outcomes in complex interventions with clients with an SLD/PMLD.
Conclusion
Sensory approaches are inherently complex because of the many mechanisms through which they effect change. Moreover, for individuals with an SLD/PMLD, it can be challenging to interpret non-verbal behaviours and responses to sensory approaches in order to evaluate their impact; the evaluation of sensory approaches in research with individuals with an SLD/PMLD is therefore a methodological challenge.
The present review collates evidence for using sensory approaches with individuals with an SLD/PMLD, highlighting their potential for improving outcomes for this client group. In spite of the limitations, evidence points to sensory approaches improving participation, communication and attention of individuals with an SLD/PMLD as well as reducing behaviours that challenge.
The review also highlights some essential features of sensory approaches that support positive outcomes for this client group, which are the use of salient sensory stimuli matched to the individuals’ unique profile; the input of a SI-trained therapist as session facilitator/consultant and consideration of higher ‘doses’ of sensory interventions for clients with an SLD/PMLD. Further research exploring these aspects of sensory approaches would be beneficial.
Key findings
For clients with an SLD/PMLD:
Potential outcomes of sensory approaches are improved participation, communication and attention, reduced anxiety and challenging behaviour.
Salient stimuli, experienced facilitators and longer intervention doses support outcomes.
What this study has added
The study has synthesised current evidence to support the use of sensory approaches in clients with a severe or profound and multiple learning disabilities and highlighted areas for future research.
Supplemental Material
sj-doc-1-bjo-10.1177_03080226231208717 – Supplemental material for Sensory approaches for adults with severe or profound and multiple learning disabilities: A systematic literature review
Supplemental material, sj-doc-1-bjo-10.1177_03080226231208717 for Sensory approaches for adults with severe or profound and multiple learning disabilities: A systematic literature review by Jennifer Humpheson in British Journal of Occupational Therapy
Footnotes
Research ethics
Not applicable.
Consent
Not applicable.
Patient and public involvement data
During the development, progress and reporting of the submitted research, Patient and Public Involvement in the research was included in the reporting of the research.
Declaration of conflicting interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The research was undertaken with funding granted through the National Institute of Health Research (NIHR) Integrated Clinical Academic Internship Programme. No other grants were received from any funding agency in the public, commercial, or not-for-profit sectors.
Contributorship
All aspects of the review, drafting and write up of the manuscript were undertaken by the named author.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.