
Abstract
Purpose:
This study aimed to evaluate the validity, reliability, and feasibility of the Persian version of the Relative Mastery Scale as a measure of the Occupational Adaptation Model in caregivers of people with multiple sclerosis.
Method:
In a cross-sectional study, after translation, face and content validity, the caregivers completed the Relative Mastery Scale and the Canadian Occupational Performance Measure. Expanded Disability Status Scale for people with multiple sclerosis was reported by neurologist. Also, convergent validity, internal consistency, test–retest reliability, and exploratory factor analyses were evaluated.
Results:
A total of 150 caregivers completed both instruments. Cronbach’s α = 0.852 and ICC = 0.838 were good. The convergent validity of the total Relative Mastery Scale score was confirmed with a significant correlation with Canadian Occupational Performance Measure (r > 0.67, p < 0.001) and Expanded Disability Status Scale score (r > 0.34, p < 0.001). The Persian-Relative Mastery Scale was found as a multidimensional instrument with three items that appeared to be redundant.
Conclusion:
The Persian-Relative Mastery Scale had acceptable reliability and validity for evaluating mastery in Persian-speaker caregivers.
Introduction
Multiple sclerosis (MS) is an inflammatory disease of the central nervous system. It is usually diagnosed in early adulthood when a person is in the productive phase of their life (Dobson and Giovannoni, 2019). Therefore, one’s life experiences can be affected, such as marriage, job choice, and social interactions (Vitturi et al., 2022). The progressive and unpredictable nature of MS is a key challenge for their caregivers and causes significant physical, psychological, and social burdens for caregivers (Motaharinezhad et al., 2015, 2020).
The challenges of unpredictability and the progressive nature of MS make it difficult for caregivers to prioritize occupations and disrupt the caregivers’ adaptation process. Based on the Occupational Adaptation Model (OAM), the adaptation process disrupted in facing some occupational challenges (Schkade and Schultz, 1992; Schultz and Schkade, 1992). Occupational challenges result from the interaction between a person’s desire for mastery, the occupational environment, and their needs for mastery, which normally occurs in the lives of all people and does not interfere with their ability to perform and complete occupations of desire (Schkade and Schultz, 1992; Schultz and Schkade, 1992). But when occupations change and mastery in previous occupations is disturbed, this challenge can affect people’s ability to adapt (Grajo, 2017; Schkade and Schultz, 2003). According to OAM, people vary in adaptive capacity, caring for a chronic condition, and their ability to adapt successfully (Motaharinezhad et al., 2020). The OAM is distinct from other models, and it underscores the importance of individuals adapting to challenges, contributing to holistic client care. Therefore, OA’s emphasis on adaptation aligns with the challenging nature of caregivers’ lives, making it a valuable guide for practitioners seeking dynamic and client-centric strategies in occupational therapy practice in this field.
The process of occupational adaptation was evaluated with relative mastery as a measurable outcome that has three components by which individuals evaluate their responses to occupational challenges: effectiveness, efficiency, and satisfaction with self and others (Schkade and Schultz, 1992; Schultz and Schkade, 1992). The first version of the Relative Mastery Measurement Scale (RMMS) was a 12-item instrument and was aimed to measure relative mastery (George et al., 2004). RMMS enabled clients to evaluate their state of relative mastery for a self-selected and a researcher-selected goal (George et al., 2004). Analyses confirmed the construct of relative mastery, with a single misfitting efficiency item (George et al., 2004). The item was improved in the new instrument, named the Relative Mastery Scale (RMS) (George-Paschal et al., 2022). Finally, RMS was introduced as a valid and reliable measure of occupational adaptation that supports application to monitor the progress of occupational adaptation across a variety of individuals (George-Paschal et al., 2022).
The RMS is not available in the Persian language. According to our knowledge, RMS has not been translated into any other language, and the present study is the first study that translated RMS into a language other than English and evaluated its validity and reliability. Examining caregivers’ occupational adaptation, particularly in the context of Iranian or Persian language users, is crucial for a comprehensive understanding of occupational therapy practice. In this cultural setting, caregiving roles often involve intricate dynamics influenced by cultural norms, family structures, and societal expectations. Exploring caregivers’ occupational adaptation sheds light on how they navigate and respond to the demands of providing care within this specific cultural and linguistic context. Therefore, this research aimed to translate and evaluate the psychometric properties of the Persian RMS and assess the feasibility of using the Persian version of the RMS to assess self-reported mastery in the caregivers of people with MS.
Methods
Study design and procedure
This cross-sectional study was approved by the Ethics Committee of Iran University of Medical Sciences with the number IR.IUMS.REC.1397.742. This study was completed in three stages: (1) Translation, (2) Validity testing, (3) Reliability and Feasibility testing of RMS in caregivers of people with MS.
Translation
In translation and cultural adaptation stage, the original English version was translated according to the IQOLA protocol. According to the recommendation of the World Health Organization, the IQOLA project was used to translate and standardize the scale (Aaronson et al., 1992). In general, this process is summarized in four stages: translating the English version into Persian (forward translation), evaluating the translation quality, translating the Persian version into English (back translation), comparing the obtained English version with the original version, and confirming the designer of the questionnaire.
Validity
Both qualitative and quantitative methods were used to check face validity (Waltz et al., 2010). For qualitative face validity, the Persian version of RMS was given to 10 experienced occupational therapists as well as 10 caregivers of people with MS to find the level of difficulty, the degree of appropriateness and ambiguity or the existence of insufficiency in the meanings of the words and the comprehensibility of the questions. Also, in order to check the content validity of the tool items in the caregivers of people with MS, 20 experienced therapists participated to establish the Content Validity Ratio (CVR) and Content Validity Index (CVI) (11 therapists for CVR and 9 therapists for CVI). The CVR is related to the validity of individual items. To know the content validity of the entire instrument, it needs to calculate a CVI (Waltz et al., 2010; Polit et al., 2007). For a convergent construct validity, RMS was analyzed for its correlation with Canadian Occupational Performance Measure (COPM) scores. While COPM may not be universally considered the gold standard, its focus on client-centered outcomes makes it a relevant benchmark for evaluating the convergent validity of other tool-based models in occupational therapy. Also, we hypothesized Expanded Disability Status Scale (EDSS) score in people with MS can influence the mastery of caregivers and that the RMS scores negatively and moderately but significantly correlate with the EDSS scores. EDSS is a method of quantifying disability in people with MS and monitoring changes in the level of disability over time and ranges from 0 to 10 in 0.5 that represent higher levels of disability (Kurtzke, 1983). People with MS with a score of 1.0–4.5 have a good and independent ambulatory ability, and a score between 5.0 and 9.5 refers to the loss of ambulatory ability (Kurtzke, 1983). EDSS score is reported by a neurologist.
Reliability and feasibility
Finally, for reliability, 10 days after collecting the questionnaire data, the participants completed the RMS again. A time of approximately 10 days was chosen between the two tests because the caregivers’ Relative Mastery was deemed to remain stable during such an interval, while the timing was long enough to cause the caregivers to forget their answers from the first occasion. After establishing the validity and reliability of a questionnaire, the next step involves the administration process for evaluating the questionnaire in a population (Creswell and Creswell. 2017), that in this study was performed through the monitoring of data collection and collecting feedback from caregivers involved in the study. Therefore for feasibility, we checked the administration process such as the ability to complete the questionnaire, the duration of completing the questionnaire, and the difficulty understanding of the questions with the caregiver’s comments regarding the tool and scoring process.
Participants and measures
One hundred sixty-seven caregivers of people with MS were recruited through the Rehabilitation Centers in Tehran, Iran. The caregivers became aware of the study objectives and methods via phone and had 2 days to decide on participation in this research. Finally, the informed consent was received from the caregivers in person. Seventeen caregivers did not return the informed consent form, so they were excluded from the study. One hundred fifty caregivers completed the RMS and the COPM. Finally, 51 caregivers of people with MS completed the Persian RMS again 10 days later to study its test–retest reliability.
Inclusion criteria specified that caregivers should be family members of people with MS. Furthermore, eligible caregivers were aged 18–60 years old. Caregivers were allowed to withdraw at any stage of the study.
In addition, people with MS under the care of caregivers should
- according to the McDonald Criteria have a confirmed MS diagnosis (Polman et al., 2005).
- have no significant cognitive impairment based on the Mini-Mental State Examination and get a score greater than 22 for cognitive screening (Cockrell and Folstein, 2002).
- have 18–60 years of age.
The RMS was developed as a quantitative instrument of the OAM (George-Paschal and Krusen, 2017; George-Paschal et al., 2022). The RMS measures the three properties identified for the adaptive response, including effectiveness, efficiency, and satisfaction for the occupational activity of clients (caregivers in the current study) in the face of occupational challenges (George-Paschal and Krusen, 2017; George-Paschal et al., 2022). The RMS consists of two parts. In part 1, six items were rated on a 5-point scale (−2 to +2), with −2 reflecting the lowest relative mastery rating and +2 indicating the highest relative mastery. A higher score indicates a more successful adaptation response. Part 2 includes three open-ended questions related to performance on the self-selected occupational activity in Part 1 that oriented clients to think and find strategies for occupational challenges. The validity and reliability of the RMS were reported as acceptable (George-Paschal et al., 2022).
COPM determines and evaluates the problems in occupational performance and one’s prioritization of occupational performance. According to this scale, the client ranks his/her occupations considering the importance in their life based on a 10-point scale. Then the person is asked to rate their performance in specific occupations, along with their satisfaction in their performance for each of these occupations. Finally, the performance scores are summed up and divided by the number of problems, from which the total performance score is obtained. Satisfaction scores are also summed up and divided by the number of problems, such that the total satisfaction score is obtained. Law et al. developed the COPM for the first time and its validity and reliability were reported as acceptable (Atashi et al., 2010; Carswell et al., 2004; Law et al., 1990). The RMS was considered for an overall goal (managing the challenges of caregivers for mastery in their daily occupations) by the caregivers that can encompass all of their daily occupations. In the same way, based on the COPM, the caregivers identified and rated their performance in 3–5 desired goals or occupations and their satisfaction with their performances.
Statistical analysis
Demographic data were reported using descriptive analysis (i.e., mean and standard deviation for continuous data, and frequency and percentage for categorical data).
Face validity was obtained quantitatively by determining the impact score. In this method, a survey was conducted on the importance of the items using a five-point Likert scale, including absolutely important (5 points), important (4 points), moderately important (3 points), slightly important (2 points), and not at all important (1 point). If the impact score of the item was more than 1.5, the item was considered appropriate in terms of face validity (Waltz et al., 2010). In content validity, the degree of necessity was measured for each item for CVR. Based on the table proposed by C. H. Lawshe, for 11 specialists, the CVR score must be higher than 0.59 to be considered an essential item (Waltz et al., 2010). In the evaluation of CVI, three states of relevance, simplicity, and clarity were evaluated for each item: scores above 0.79 are suitable, scores between 0.70 and 0.79 are questionable and need to be revised, and scores below 0.70 are considered unacceptable (Waltz et al., 2010).
Since the Kolmogorov–Smirnov test indicated the non-normality of the data, correlations between RMS and COPM scores were analyzed by calculating Spearman’s correlation coefficients. Correlation coefficient values <0.4, 0.4–0.69, and >0.7 between the RMS with COPM scores were considered weak, moderate, and strong correlations, respectively (Akoglu, 2018).
Intraclass correlation coefficient (ICC) with a 95% confidence interval (CI) was used to evaluate the test-retest reliability. Cronbach’s alpha was calculated to assess internal consistency. Values ⩾0.7 are acceptable for ICC and Cronbach’s alpha (Bobak et al., 2018; Koo and Li, 2016; Terwee et al., 2007). Also, the Corrected item-total correlation was used to examine the internal construct validity.
For factor structure, an exploratory factor analysis (EFA) was conducted for analysis of the relationships between variables of the Persian version of the RMS construct using principal component analysis with varimax rotation. The cutoff point for factor loading was determined at 0.4 (Schumacker and Lomax, 2004). Also with calculating the Kaser–Meier–Olkin (KMO), the sample size’s adequacy indicated the data’s suitability for factor analysis (Huck et al., 2012; Osborne and Costello, 2004).
Results
Translation
After obtaining permission from the designer of the questionnaire (Dr Lorrie George-Paschal) via email, the questionnaire was translated into Persian by translators 1 and 2, who had sufficient experience in translating English texts. At next stage, the emphasis was on the conceptual equivalence of the questionnaire’s words, phrases, and sentence and was confirmed the translation quality. In the next step, the Persian version was back-translated into English and analyzed by two translators 4 and 5. The final translation of the Persian version into English was sent to the designer to review. Finally, with the designer’s approval, the Persian version of the RMS was prepared.
Validity
Face and content validity
For the face validity, (qualitative method) of the Persian version of the RMS, 10 experienced therapists as well as 10 caregivers of people with MS reviewed the level of difficulty, the appropriateness, and the comprehensibility of the questionnaire questions through email.
For the quantitative method, based on therapists’ opinions, all items received a favorable impact score >1.5. Finally, all the items were understandable and clear, and 95% of the therapists and caregivers confirmed that the RMS has good face validity.
For content validity, the RMS was sent to the therapists via email and the necessity of the items and the relevance of the items were checked by 11 and 9 experts, respectively. According to Lawshe’s table, CVR > 0.79 was considered desirable. Also, based on the “relevance,” all the items were acceptable (CVI > 0.81), and no items were changed or removed during content validity.
Convergent validity
Characteristics of the participants
One hundred fifty caregivers of people with MS completed both RMS and COPM to assess the convergent validity of the RMS (Mean age = 42.75, SD = 11.31). Sixty-eight (45.3%) of the caregivers were female. The mean age of the people with MS under care was 38.54 years (SD = 9.34). The EDSS score in 108 (72%) of the people with MS was <4 and in 42 (28%) patients were between 4.5 and 8. Descriptive statistics for total and subscales scores of RMS are shown in Table 1.
Descriptive statistics for the total and subscales of RMS (n = 150).
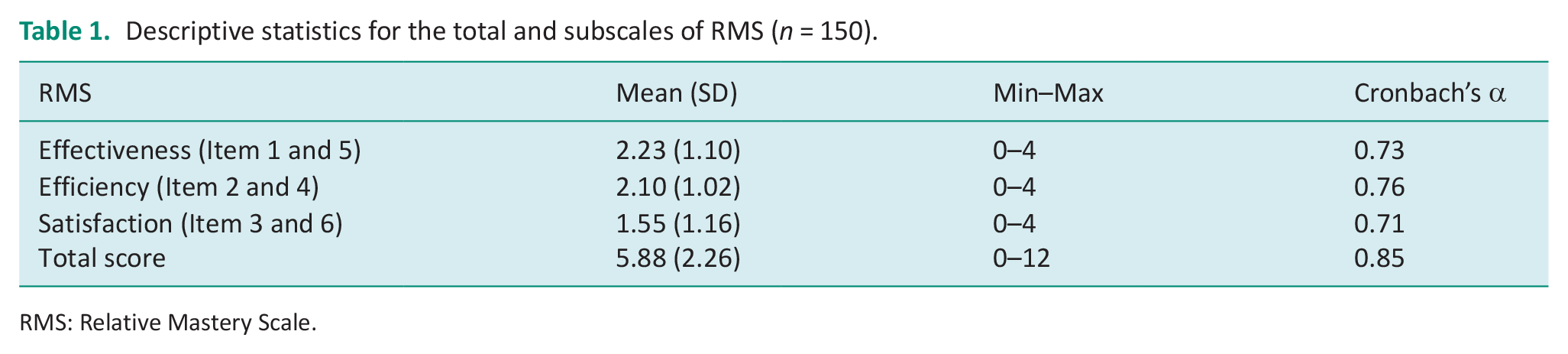
RMS: Relative Mastery Scale.
The Spearman’s correlation showed a significant and strong correlation between RMS score and the Performance (0.70, p < 0.01) and Satisfaction (0.67, p < 0.01) of COPM (Table 2). Also all subscales of RMS in the caregivers had a moderate and significant Spearman’s correlation with COPM scores except effectiveness and satisfaction subscales that had poor and significant correlation with the Performance (0.22, p < 0.01) and Satisfaction (0.28, p < 0.01) of COPM, respectively. Analysis by EDSS of the people with MS with RMS scores of caregivers indicated that the caregivers of people with MS with EDSS score <4 had a poor, significant, and negative correlation (−0.34, p < 0.01) and the caregivers of people with MS with EDSS score <4.5 had a strong, significant, and negative correlation (−0.66, p < 0.01) with RMS total scores. All subscales of RMS in the caregivers had a significant and negative correlation with patient’s EDSS score, except Satisfaction (−0.20, p = 0.31) did not demonstrate a significant correlation with patient’s EDSS score <4 (Table 2).
Spearman’s correlation coefficient of the sum score of RMS with the COPM (n = 150).

RMS: Relative Mastery Scale; COPM: Canadian Occupational Performance Measure; EDSS: Expanded Disability Status Scale.
Correlation is significant at 0.05 significant level (one-tailed).
Correlation is significant at 0.01 significant level (two-tailed).
Exploratory factor analysis
Based on the Kaser–Meier–Olkin (KMO) test (0.61) and the Bartlett test of sphericity (χ2 = 50.86, df = 15, p < 0.001), the sampling was adequate. Based on the Factor analysis and with an eigenvalue >1, two factors were extracted for the EFA, which together explained 54.9% of the total variance (Table 3 and Figure 1). Also, based on the varimax rotation method with removing of 3 items and item-total correlation <0.4 (Table 4), extracted one factor with items 1–3 explained 42.9% of the total variance (eigenvalues = 1.27). Factor loading for items 1–3 were 0.719, 0.774, and 0.677, respectively.
Factor loadings of Persian RMS.
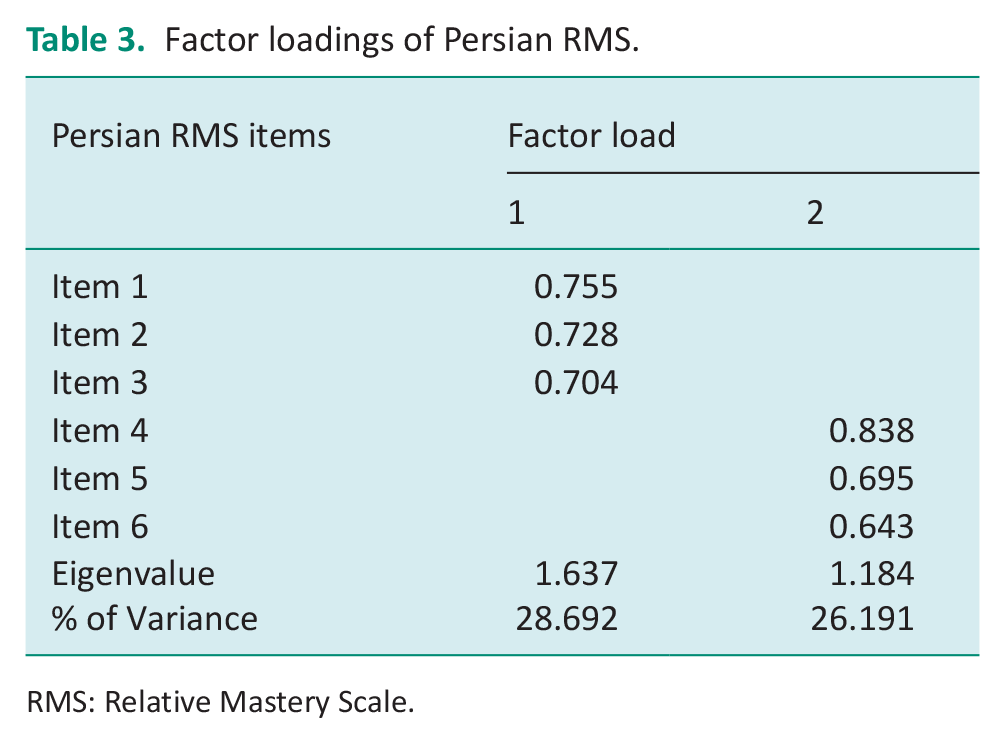
RMS: Relative Mastery Scale.
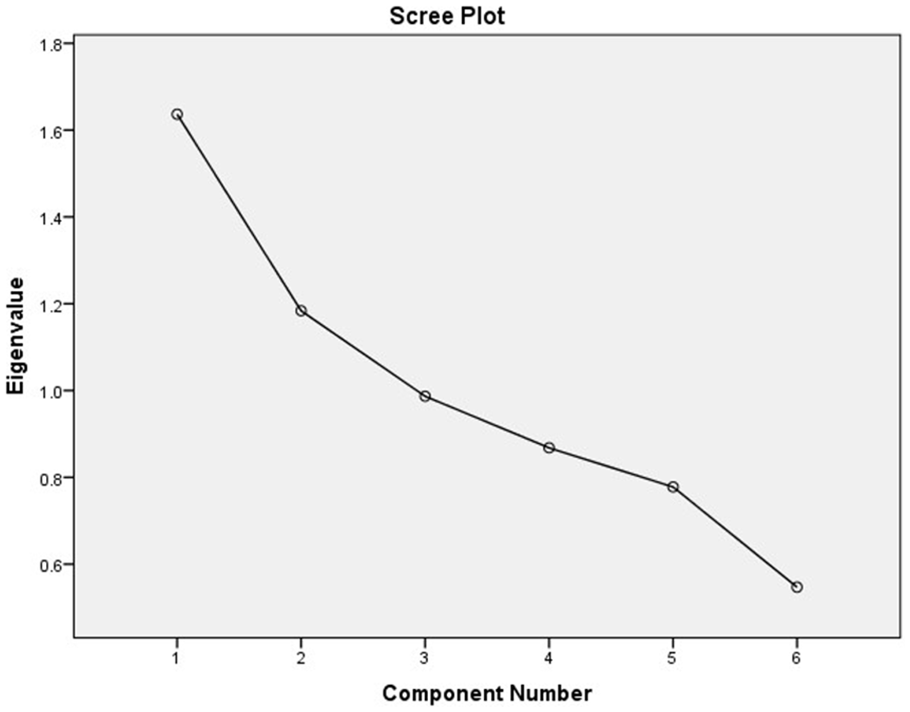
Scree plot of 6-item Persian RMS shows 2-factor with the eigenvalues >1.
Cronbach’s α if item deleted and corrected item-total correlation for Persian RMS (n = 150).

RMS: Relative Mastery Scale.
Item-total correlation <0.4.
Reliability and feasibility
Cronbach’s alpha coefficient for 150 caregivers who completed the questionnaire at one time was 0.852, which indicates excellent internal consistency for the total RMS score (Table 1). If an item was deleted, Cronbach’s alpha ranged between 0.715 (item 6) and 0.886 (item 1). The corrected item-total correlation for three Items of RMS (3–6) was <0.40, and when deleted the Cronbach’s alpha for internal consistency of RMS (3 items) was 0.789 (n = 150; Table 4). The cut-off for Item-total correlation was set at >0.40 (Ware Jr and Gandek, 1998). The questionnaire was completed after 10 days by 51 caregivers again, and the ICC for total score RMS was 0.838 (p < 0.001).
We recorded the time required to answer and score the RMS by chronometer. The average time was 12.47 minutes (ranging between 6 and 20 minutes). It appears this time is considered acceptable by caregivers and therapists. No participant had a time above 20 minutes that demonstrated the caregivers understood the RMS items well. Seventy-one caregivers completed the RMS in a range between 15 and 20 minutes. These participants required a longer time to understand and link the items with the goal. Therefore, it was need to spend more time with them to explain the concepts of the RMS. For 69% of the caregivers, the questions of the RMS were easy to understand and for 31% were difficult. 89% of the caregivers stated that the RMS questions raised their awareness about the management of care-related occupational challenges and prompted them to think about their responses.
Discussion
Developing and selecting appropriate tools for evaluation at the international level to examine various outcomes at personal and social levels is one of the important issues in research. Therefore, researchers seek tools that evaluate their desired concepts as accurately and comprehensively as possible. In occupational therapy literature and according to OAM, relative mastery is the primary measure of the state and process of occupational adaptation (Schkade and Schultz, 1992; Schultz and Schkade, 1992) and the RMS was developed as a quantitative tool for measuring the state and process of occupational adaptation. But it is available only in its original English version (George-Paschal et al., 2022). Therefore, the current study was the first to translate this tool into another language and evaluate the psychometric properties and feasibility of the RMS. This study was aimed to translate the RMS into Persian language and provide information about its reliability and validity based on the OAM concepts.
Translation
The translators in this study, who had sufficient and acceptable skill and experience in translating English texts into Persian and vice versa, improved the ease and satisfactory quality of the translation process in a reportable manner. Also, there were several stages of forward and backward translation, qualitative review of the obtained version and matching with the original version by the developer (George-Paschal et al., 2022), as well as following the translation process based on the IQOLA protocol confirms the quality of the translation version (Aaronson et al., 1992).
Validity
A separate analysis of RMS subscales showed that all subscales except Effectiveness and Satisfaction showed a moderate and significant correlation with COPM. The effectiveness subscale had a weak correlation with the performance. Perhaps this weak correlation can be attributed to the evaluation content of the RMS items in this subscale. For the effectiveness subscale, caregivers, in addition to scoring their performance, must also score the degree of achievement of the result they wanted for that performance. In COPM, caregivers only rate their performance level and do not evaluate the results (Carswell et al., 2004).
On the other hand, in COPM, caregivers evaluated their performance level in daily activities, while in RMS, they only scored one goal (management of caregiving challenges). The satisfaction subscale also had a weak correlation with the satisfaction score in COPM. Although the authors expected this correlation to be strong, this difference may be due to the evaluation of the level of satisfaction of others in this subscale of RMS, while again, in COPM, only the level of satisfaction of the individual is evaluated (Carswell et al., 2004). On the other hand, it seems that determining the level of satisfaction of others from another person’s performance can be influenced by some personal characteristics such as psychosocial status, attitude, culture, etc.
The correlation of RMS’s total score in the caregivers with EDSS score above 4.5 in patients under their care was strong, significant, and inverse. Still, the correlation was weak but significant in caregivers with patients with EDSS <4. The existence of such correlations is not surprising because caregivers who cared for patients with an EDSS above 4.5 were more involved in the care process so they had to spend more hours during the day involved in the challenges of caring for their patients (Motaharinezhad et al., 2020), which can affect their mastery. While patients with EDSS of <4 are independent in most daily activities and do not need much care.
The factor analysis of the RMS showed that the RMS might not be a unidimensional questionnaire. The corrected item-total correlation analysis revealed that three items of the RMS may be redundant, and it was only with the removal of three items that a single factor was achieved. From the implications of this finding is probably that three items of the RMS evaluate different constructs confirming the multidimensionality of the RMS and there might be more complexity or specificity in the relationships among items, indicating a more nuanced structure in the phenomenon being studied that in the current study is “mastery” in the caregivers of people with MS. The original English version applied Rasch analysis and factor analysis and reported that the RMS is unidimensional (George-Paschal et al., 2022) and the relationships among items had been more straightforward.
The differences in the dimensionality between the Persian version of the RMS and the original version could arise due to variations in sample characteristics, etc. (Tabachnick et al., 2013). It might prompt further research into why the factor structures differ and what contextual factors contribute to these variations.
Reliability and feasibility
The good internal consistency of the total RMS score with an alpha of 0.852 and all subscales (>0.7), which was acceptable, showed the appropriateness and necessity of the items and subscales. However, the RMS items in the original version had an excellent Cronbach’s alpha coefficient (0.94; George-Paschal et al., 2022). We predict differences in internal consistency between the current study and the original study could be influenced by various factors such as sample characteristics (community-dwelling adults in the original study and caregivers in our study), cultural or contextual differences, measurement variability (changes in how the tool is administered or slight modifications in item wording), and sample size (larger sample in the original study). However, assessing the context, methodology, and characteristics of each study is crucial in understanding why there might be variations in the internal consistency values between different research (DeVellis and Thorpe, 2021). Also, the retest value (0.838) for the test-retest reliability showed that the RMS is reliable and repeatable among the caregivers of people with MS in Iran. With the change of time, the items and concepts of the scale will be stable. The retest was not evaluated in the original English version of the RMS. One of the main challenges in the test-retest reliability in determining the reliability of tools is determining the appropriate time interval (DeVon et al., 2007). The usual time interval is between 2 weeks and 1 month (DeVon et al., 2007). The time interval between should be such that it is impossible to recall the instrument’s items and there should be no change in the measured phenomenon (DeVon et al., 2007). Therefore, it seems that a minimum time interval (10 days) was suitable in the caregivers of people with MS, so it wasn’t too long to change the master which could occur with the possibility of relapse of MS in patients under the care and the need for more care.
Also, this study showed that the Persian version of RMS is a feasible tool. Most caregivers experienced the scoring method easily. This can indicate the accurate translation and validity process of the RMS. However, a number of caregivers faced difficulty in scoring and relationship of items, which seemed to be due to unfamiliarity with some terms in the RMS. Therefore, the authors in this study suggested that the assessment of RMS should be administrated by an experienced therapist familiar with the concepts of the OAM as well as the challenges caused by MS disease. In addition, according to the caregivers’ point, part 2 of the RMS (open questions) made an indirect compulsion to think about successfully doing the occupational activity. The indirect guidance of this section in RMS made caregivers about seeking, modifying, and changing their attitudes or strategies to do their desired occupational activity. However, it seems that there is a need for more research to examine this issue.
Limitations
There are several limitations in the present study. First, we did not administer a Rasch analysis to investigate the dimensionality of the RMS. Future investigation is required to conduct a Rasch analysis of the RMS to determine the dimensionality. Second, no other language versions of the RMS were available to compare validity and reliability, such as factor analysis. This study was the first research on the validity and reliability of RMS in another language.
Conclusion
The present study showed RMS is a reliable and valid instrument for the evaluation of mastery in Iranian caregivers of people with MS. We tried in the present study to prepare RMS for use in education, practice, and research in Iranian society. Understanding the caregivers’ adaptation process using RMS is essential for tailoring interventions that align with the unique challenges they face. It allows occupational therapists to develop culturally sensitive and effective strategies that acknowledge the caregiver’s role in supporting individuals with diverse conditions and needs such as people with MS. Moreover, we believe considering the caregivers’ occupational adaptation in the Persian-speaking community offers insights into the cultural nuances that may affect communication and collaboration between healthcare professionals and caregivers. Recognizing these factors is fundamental for promoting effective partnerships, ensuring the delivery of client-centered care, and fostering positive outcomes within the Iranian or Persian language user context.
Key findings
The Persian RMS was feasible among Iranian caregivers.
Persian-RMS has demonstrated good internal consistency and test-retest reliability.
This study demonstrated good psychometrical characteristics for Persian-RMS as an occupation-based measure for Iranian caregivers of people with MS.
Footnotes
Acknowledgements
We gratefully acknowledge all the participants in this research who agreed to participate in this study and honestly provided their valuable experiences.
Research ethics
This study was approved by the Ethics Committee of Iran University of Medical Sciences with the number IR.IUMS.REC.1397.742.
Consent
In the current study, written consent was obtained from written participants.
Patient and public involvement data
During the development, progress, and reporting of the current research, Patient and Public Involvement in the research was included in the conduct of the research.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The Iran University of Medical Sciences funded the study.
Contributorship
F.M. and A.H. developed the Protocol/project, and wrote the main manuscript text. S.G. and L.L. analyzed data and prepared figure and tables. M.M. collected data and managed data analysis and all authors reviewed the manuscript.