
Abstract
Introduction:
Post-stroke depression is a frequent but under-diagnosed condition. Nevertheless, it impacts participation in activities of daily living (ADLs) and the rehabilitation process. The aim of this study is to analyze the influence of post-stroke depression on participation in ADLs and on occupational therapy (OT) intervention in adults.
Methods:
An observational study was conducted through a survey. The questionnaire covered OTs view about the influence of post-stroke depression on ADLs and occupational therapy treatment. Data collected by online questionnaire were analyzed through STATA®, using a mixed method. Quantitative data were analyzed through descriptive statistics. Qualitative data were analyzed by thematic analysis.
Results:
Sixty-three surveys were valid. Stroke adults manifest hopelessness toward the future, crying and nervousness (“often” / “always” >50%). They have often worse occupational performance than patients with stable mood (55.56%), especially in self-care activities (35.92%). The performance limiting factors are low volition (41%), reduced motor skills (30%), and reduced cognitive skills (19%). OT intervention with these patients aims to increase volition (21.30%), recover roles (16.61%), and improve self-care activities (14.08%).
Conclusion:
Mood disorders negatively affect participation in ADLs and OT intervention. This study highlights the importance of volitional factors in promoting occupational engagement and provides guidance for OT treatment. Further investigation through specific studies appears necessary.
Introduction
Depression is one of the most frequent and important neuropsychiatric consequences of stroke (Alajbegovic et al., 2014). Its cause is poorly understood, but the onset is known to be related to biological and psychosocial factors (Towfighi et al., 2017). Post-stroke depression affects about 33% of survivors within 5 years, but it’s often neither recognized nor treated due to diagnostic difficulties (Robinson et al., 2016). A literature review found that the frequency of depression ranges from 5% at 2 to 5 days after stroke to 84% at 3 months after stroke, generating higher states of disability (Hackett and Pickles, 2014). The greater severity of stroke and the lower degree of autonomy are the main risk factors for depression (Guo et al., 2022).
In Italy, stroke is the leading cause of disability and the second cause of death (Ministero della Salute, 2021). Motor and cognitive impairments limit participation in daily activities and make occupational therapy (OT) intervention increasingly necessary. A systematic review of the literature shows that OT intervention in stroke patients focuses on recovering autonomy in ADLs and counseling about assistive aids and technologies (Steultjens et al., 2003). This view, however, does not consider emotional aspects, which, together with motor and procedural factors, affect occupational performance (Kielhofner and Burke, 1980). Indeed, factors like cognitive impairments, lack of social or family support, and anxiety are all predictors of depression after stroke (Ayerbe et al., 2013 and Towfighi et al., 2017).
According to Torrisi et al. (2018), post-stroke depression and reduced autonomy seem to influence each other. A literature review revealed that the most consistent association with depression after stroke is severe stroke, early physical disability, and later disability (Kutlubaev et al., 2014). Indeed, there are higher levels of post-stroke depression in patients who are more dependent in ADLs (Ezema et al., 2019). Similarly, ADL performances of patients with post-stroke depression are significantly worse than those of patients with stable mood (Ezema et al., 2019). Despite these data, available evidence investigate the OT intervention in adults with post-stroke depression. Recent studies report findings where OT is combined with other treatments, pharmacological and nonpharmacological, to evaluate the effectiveness of these ones. (Maltseva et al., 2018; Zhang et al., 2021). Most notably, the first study featured only men, whereas the other was specifically about mirror therapy.
The aim of this study is to analyze the influence of post-stroke depressive symptoms on participation in ADLs through OTs’ views and investigate the occupational therapy intervention in adult stroke survivors with mood disorders.
Using the view of OTs, rather than testing patients directly, allows us to detect the point of view of a professional figure specialized in ADLs rehabilitation. An occupational therapist, indeed, considers the person as an occupational being embedded in his or her environment and can grasp the various aspects that affect their performance. In addition, through the experiences of OTs, it’s possible to focus on treatment and highlight any difficulties in the intake.
Materials and methods
Study design
An observational survey was conducted through a questionnaire.
Population of interest
The population of interest was Italian occupational therapists who are currently working in neurorehabilitation.
Occupational therapists were selected based by university education and number of years of experience in neurorehabilitation.
The questionnaire was sent to all therapists who were registered with the Italian scientific association (AITO). Sending the questionnaire to all occupational therapists nationwide was not possible because it is not possible to find all e-mail addresses (legal requirements).
All participants signed the informed consent and privacy policy required to participate in the study. Given the non-clinical population of interest, the active involvement of an ethics committee was not necessary.
Questionnaire design
A questionnaire was created ex novo through a topic-specific literature research and an active discussion by the authors.
Electronic databases searched in April 2022 were PubMed, Embase, PsycINFO, and Scopus.
The following topics were used as keywords: stroke, depression, depressive symptoms, autonomy, quality of life, and OT. The search strings are available in supplementary materials.
The identified articles were imported into Rayyan, a software for automatic review management, and submitted for review by the authors. The list of selected articles and the PRISMA flow diagrams are available in the Supplemental Materials.
Based on the selected articles and through a focus group, authors identified the following topics of interest for the questionnaire creation: post-stroke emotional state; relationship post-stroke depression and ADLs/quality of life; and relationship post-stroke depression and OT. The three authors conducted the focus group: one of them with <3 years of experience, the others with >10 years of experience in neurorehabilitation and research.
The final questionnaire consisted of 30 questions: 6 about participants’ personal information, 16 single-choice questions, 4 multiple-choice questions, and 4 open-ended questions.
Setting
The questionnaire was digitally transformed via the Google Forms platform. Participants were reached through the Italian Association of Occupational Therapists (AITO). The period for online completion was from 29 June 2022 to 31 July 2022. Before completion, therapists had to read the instructions to filling out the questionnaire. The responses obtained were collected, anonymously, in an Excel® file (Microsoft Office 2019).
Variables and outcome
The primary outcome of the study is related to how much, based on the therapist’s experience, patients with stroke outcomes with mood disorders have worse occupational performance in ADLs than patients with stable mood (question no. 13. of the questionnaire). This variable of interest is categorical (closed answer).
The influence of post-stroke mood disorders on OT intervention is a co-primary outcome (question no. 20 of the questionnaire). This variable of interest is qualitative.
Secondary outcomes with quantitative variables were the most frequent depressive symptoms in adults after stroke; characteristics of stroke patients with mood disorders, regarding age, gender, life roles, social environment, and work situation; quality of performance in ADLs of stroke patients with mood disorders; and aspects affecting participation in daily activities.
Secondary outcomes with qualitative variables were differences related to OT intervention in adult stroke victims with mood disorders; professional and personal difficulties experienced by occupational therapists during the treatment of adult stroke victims with mood disorders.
Bias
To minimize selection bias, we released the questionnaire through the Italian Association of Occupational Therapists (AITO). This allowed us to receive responses specifically from only occupational therapists working in Italy. To reduce the participation of occupational therapists who had never treated neurological patients, we included a series of initial selection questions (university education, years of experience, and clinical setting).
To reduce information bias, we tried to formulate the questions and answers as clearly as possible. We favored closed-ended questions to avoid distorting the result.
To reduce sample confounders, we formulated the initial questions considering all the characteristics of interest to those working in the neurological area.
To reduce reporting bias, the scientific article was written according to the guidelines in the STROBE Checklist specifically for cross-sectional studies.
Sample size of the study
The sample size of interest was calculated according to the primary outcome.
Following Bartlett’s article (2001), the type I error (Alpha) was set at 0.05, the standard deviation (SD) of the categorical outcome was set at 0.80, and the absolute error (d) was set at 0.20. The formula for estimating the sample size reported the need to include 62 subjects in the study.
The number of occupational therapists in Italy is small, about 2000. Currently, it’s not possible to clearly define how many occupational therapists work in the neurological field.
Statistical methodology
In order to ensure the generalizability, contextualization, and credibility of the study, a mixed method analysis was chosen.
Quantitative data were analyzed through descriptive statistics (median, SD, percentages, and frequencies) using STATA® 14.2 software (StataCorp LLC, College Station, TX, USA).
Qualitative data from the open-ended questions were analyzed by thematic analysis. This methodology was by topic according to Richards (2005). No coding software was used. Each individual author read the open-ended responses of the questionnaire and highlighted relevant themes. All authors met for active discussion of the themes and selection of the most relevant ones. The choice of themes was by majority vote.
The responses were subsequently stratified according to the educational qualification of the respondents to highlight any differences with OTs more experienced in neurology, neuropsychology, neurorehabilitation, and psychology.
Due to the type of population surveyed, the following confounders were taken into consideration: age, type of education, years of experience, and work setting. The specific objective of the study is not to report a risk factor or to give an indication for treatment: it was therefore decided not to use a risk adjustment model but to conduct a subsequent analysis for a subgroup, in this case educational qualification.
To reduce missing data, all questions concerning quantitative variables were mandatory. Questions concerning qualitative variables were not mandatory, in which case missing answers were considered relevant.
Results
Description of participants
Six hundred and sixty questionnaires were distributed. Sixty-three occupational therapists completed the questionnaire. The response rate was 9.5%. Table 1 shows the sample composition. The mean age of the participants was 32.6 years (SD = 6.83), ranging from 22 to 53 years. The responding occupational therapists had, on average, 7.17 years of experience in neurorehabilitation (SD = 6.22), with a range between 0.5 and 28 years. All participants had a bachelor’s degree in OT (100%). Fifty-four occupational therapists (85.7%) reported facility based as their main intervention setting, while nine indicated the home setting (14.2%).
Sample characteristics.

Descriptive analysis of the quantitative data
Table 2 shows the frequency of emotional states in adults with stroke. The most frequent post-stroke emotional states in adults are hopelessness toward the future, crying, irritation/nervousness, and loss of interest in activities (work or hobbies). All “often”/“always” responses above 50% were considered relevant here.
Emotional states in patients with stroke.
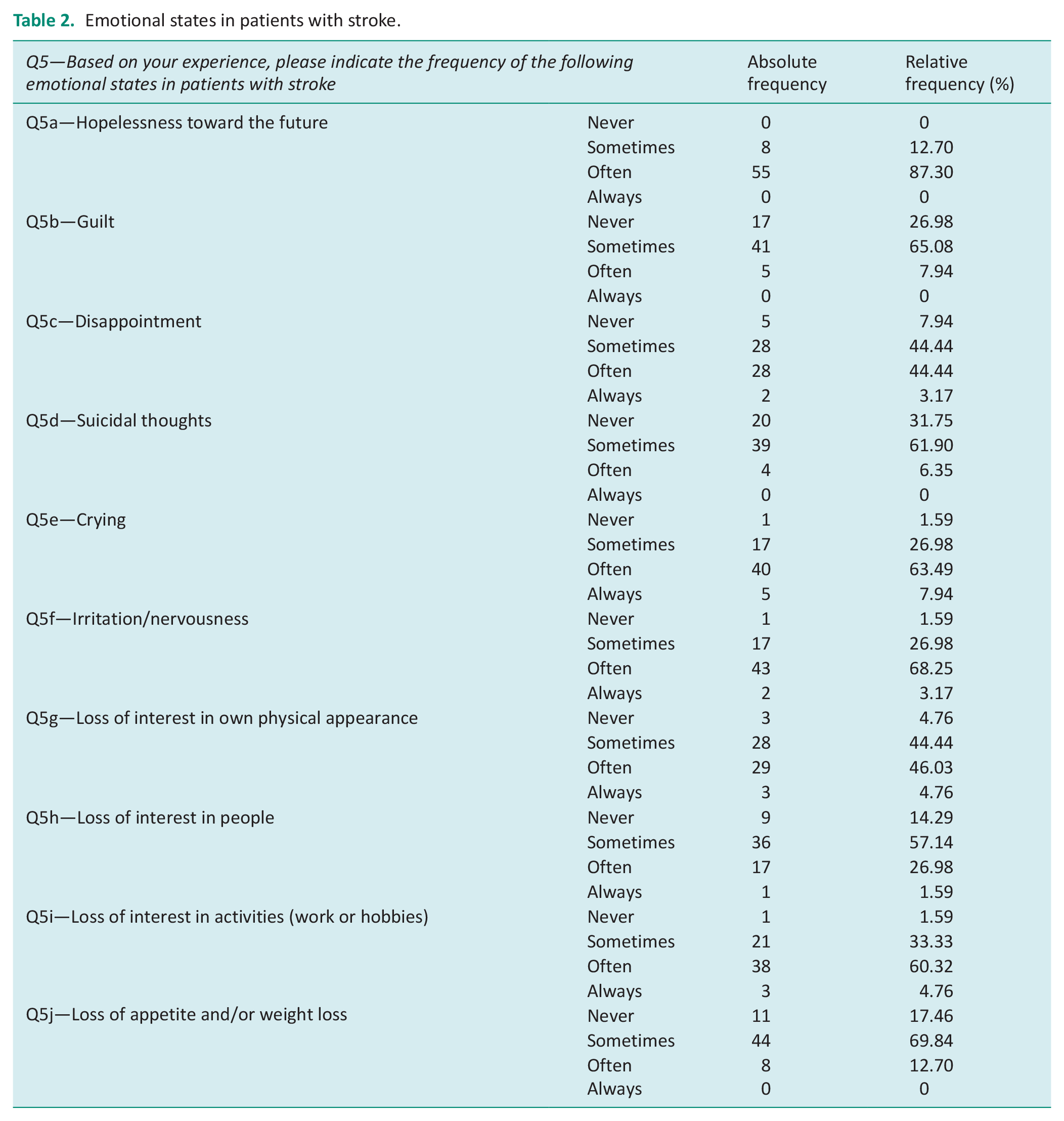
Table 3 describes the characteristics of stroke patients with mood disorders regarding: sex, age, roles, social environment, work, and performance in ADLs. In relation to sex and age (Q6–Q7), stroke patients with mood disorders are male and female with no significant differences (61.90%), aged 40–60 years (36.51%). These patients experience many difficulties in fulfilling role expectations (Q8–76.19%) or are unable (Q8–9.52%). The quality of their occupational performance (Q11) is “often” worse than that of patients with stable mood (55.56%). The activities in which performance is worst (Q12) are personal care activities (35.92%). The aspects that most impair occupational performance are (Q13): low volition (41%), reduced motor (30%), and cognitive skills (19%).
Post-stroke depression, ADL/quality of life and OT.
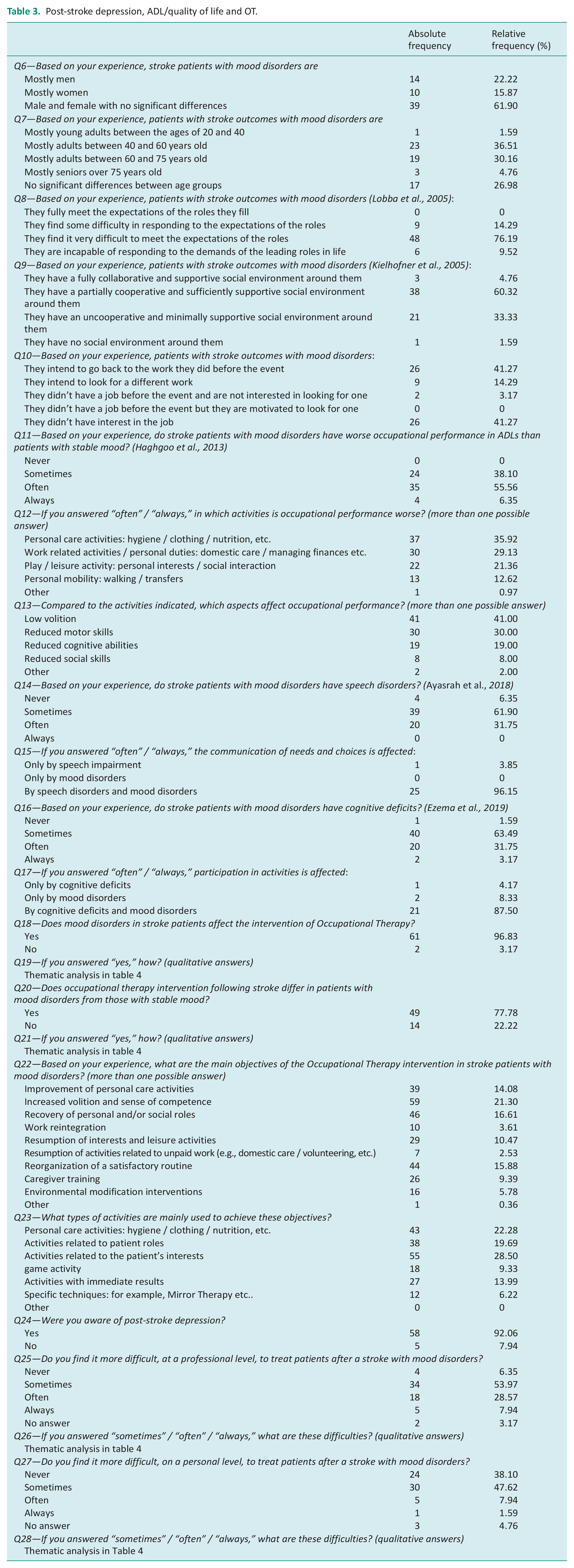
The characteristics of OT intervention in adults with post-stroke depression are shown in Table 3. According to the study participants, mood disorders affect the OT intervention (Q18–96.86%) and makes it different from that with patients with stable mood (Q20–77.78%). The main goals of OT intervention with these patients are (Q22) increasing volition and sense of competence (21.30%) and recovering personal and/or social roles (16.61%). The types of activities used for their achievement are (Q23) activities related to patient interests (28.50%) and personal care activities (22.28%). Almost all study participants, moreover, declared that they were aware of post-stroke depression (Q24–92.06%). Many participants, finally, reported that they “sometimes” experience greater professional (Q25–53.97%) and personal (Q26–47.62%) difficulties when treating stroke patients with mood disorders.
Thematic analysis of qualitative data
Thematic analysis was used to sum up the OT intervention-related responses. Each theme was divided into several sub-themes. The complete thematic analysis is available in Table 4.
Thematic analysis.

According to the participants, mood disorders in stroke patients affect two aspects of OT intervention (Q19): patient motivation (42) and therapeutic alliance (12). The main differences about the OT intervention with these patients are two (Q21): increased timing (32) and acceptance of discomfort (8). The professional difficulties experienced during treatment were summarized in two themes (Q26): difficulties in involving the patient in the rehabilitation project (29) and difficulties in goal setting (10). Finally, the main personal difficulties experienced during treatment were (Q28) the therapeutic relationship (14) and frustration and self-doubt (9).
General analysis of the subgroup “educational qualification”
Sixteen occupational therapists formed the subgroup “Educational qualification higher than Occupational Therapy.” Appendix 5 shows its composition. The average age of the subgroup was 33.56 years (SD = 8.56), ranging from 25 to 53. They had, on average, 7.5 years of experience in neurorehabilitation (SD = 7.7), with a range between 4.5 and 28 years. Fifteen occupational therapists (93.75%) reported facility based as their main intervention setting, while only 1 reported home-based (6.25%).
The subgroup reported that the most frequent post-stroke emotional states in adults are (Appendix 6): hopelessness toward the future, crying, irritation/nervousness, loss of interest in self-image, and loss of interest in activities (work or hobbies). All “often”/“always” responses above 50% were considered relevant here.
The subgroup reported that stroke patients with mood disorders are (Appendix 7): male and female with no significant differences (Q6–62.50%), aged 40–60 years (Q7–43.75%). These patients experience difficulties in fulfilling role expectations (Q8–75%). The quality of their occupational performance (Q11) is “often” worse than that of patients with stable mood (56.25%). The activities in which performance is worst (Q12) are personal care (31.03%) and work-related activities/personal duties (27.59%). The aspects that most impair occupational performance are (Q13): low volition (46.15%) and reduced motor skills (26.92%).
Appendix 7 describes the characteristics of OT intervention in adults with post-stroke depression according to subgroup. The whole subgroup (100%) claimed that mood disorders in stroke patients influence OT intervention (Q18). The following areas of influence emerged: (Appendix 8—Q19): patient motivation (10) and therapeutic alliance (4). Most of the subgroup (75%) reported that OT intervention after stroke differs in patients with mood disorders from those with stable mood (Q20). The following differences emerged (Appendix 8—Q21): increased timing (9) and acceptance and containment of malaise (1). The main goals of OT intervention with these patients are (Q22) increasing volition and sense of competence (16.87%) and reorganization of a satisfying routine (16.87%). The types of activities used to achieve them are (Q23) activities related to the patient’s interests (28.30%) and personal care activities (24.53%). The entire subgroup stated that they were aware of post-stroke depression (Q24–100%). Most of the subgroup reported that they “sometimes” experience greater professional (Q25–47.75%) and personal (Q26–50%) difficulties while taking care of stroke patients with mood disorders. The professional difficulties experienced during treatment were summarized in two themes (Table Appendix 8 – Q26): difficulties in involving the patient in the rehabilitation project (7) and difficulties in goal setting (4). Finally, the main personal difficulties experienced during treatment were (Appendix 8—Q28): frustration and self-doubt (4) and the therapeutic relationship (2).
Discussion
Responding occupational therapists confirmed the presence of depressive symptoms in adults with stroke. According to their view, depressive symptoms affect occupational performance in ADLs and influence OT treatment, causing difficulties among the occupational therapists themselves.
A significant finding of the present study concerns the heterogeneity of post-stroke emotional states. Alongside conditions of inertia in which there is a lack of motivation to do, there are feelings of irritation and nervousness, which complicate the clinical situation and subsequent intake. The available literature, while highlighting the presence of depression following stroke, does not elaborate on its peculiarities (Altindag et al., 2008; Ayasrah et al., 2018; Ezema et al., 2019; Haghgoo et al., 2013). Delineating the nature of signs and symptoms characterizing post-stroke depression, on the other hand, allows the occupational therapist to adapt the approach to the patient and modulate the intervention. As stated above, occupational therapists claim that the occupational performance in ADLs of stroke patients with mood disorders is often, or even always, worse than that of patients with stable mood. This result totally reflects what has been found in the literature (Altindag et al., 2008; Ayasrah et al., 2018; Ezema et al., 2019; Haghgoo et al., 2013). We should point out, however, that most of the occupational therapists responding to the questionnaire worked in the hospital setting. They are therefore more likely to see patients earlier after stroke than in the community. This aspect could influence their experience and, likewise, ADLs.
The results find worse occupational performance in activities related to self-care and work/personal duties, that is, life roles. A singular aspect, across all activity types, concerns personal mobility. Occupational therapists with specializations report that personal mobility of stroke patients with mood disorders is worse than that of patients with stable mood twice as often as occupational therapists with bachelor’s degrees. There is a positive correlation in the literature between lower levels of post-stroke depression and better walking skills (Altindag et al., 2008). Seizing this aspect, therefore, is important for teamwork purposes, especially for physical therapists involved in improving and restoring walk ability.
The results show that the aspects that impair occupational performance in stroke patients with mood disorders are, to a greater extent, low volition and reduced motor skills. This finding appears to be evident of what Kielhofner and Burke (1980), with MOHO, argue. According to MOHO theory, human action is primarily promoted by volition, a factor necessary to allow the person to choose what kind of occupations to pursue and with what engagement (Kielhofner and Burke, 1980). Occupational therapists interviewed report that the primary goal of OT is increasing volition and sense of competence. Low volitional levels result in patients not choosing the type of occupations in which to engage, because they don’t perceive themselves as competent and able to act on the outside world. Strengthening the volition system, therefore, is functional in improving other skills needed to increase participation in ADLs. Increasing volition and sense of competence, however, is not without its issues. The results show that the types of activities used during intake are those related to the patient’s interests. Reduced cognitive abilities, potential language impairments, and mood disorders, however, affect the communication of needs and choices, making it difficult for an occupational therapist to understand what the patient’s real interests and needs are. Moreover, this goal makes limited progress in autonomy recovery and lengthens the period. Much time, in fact, is dedicated to establishing the therapeutic relationship, which is hampered by the patient’s low motivation and compliance. This scenario generates feelings of frustration and questioning of their work by occupational therapists, who are, sometimes, struggling with the influence that the patient’s mood may have on them and individual experiences.
This study comes from a gap found in the literature regarding OT intervention in adults with post-stroke depression. The presence of depressive symptoms in stroke-affected adults and poor participation in ADLs is a known finding (Altindag et al., 2008; Ayasrah et al., 2018; Ezema et al., 2019; Haghgoo et al., 2013). However, this study is the first to focus on the occupational therapists’ perspective through a cross-sectional study and survey aimed at them. This modality allowed for an in-depth study of the characteristics of patients with post-stroke depression and their participation in ADLs, and focused on rehabilitation intake.
The survey also allowed occupational therapists to choose the type of activities in which patients with post-stroke depression experience the most difficulties. Studies in literature, in fact, often are limited to using Barthel’s Index to detect the patient’s status related to simple basic activities and personal care (Altindag et al., 2008; Ezema et al., 2019; Haghgoo et al., 2013). This study, on the other hand, includes activities from the three life spheres: self-care, work, and leisure.
The main limitation of this study relates to the sample composition, which is only partially representative of the entire population due to the low age and few years of experience in neurorehabilitation among the participants. Furthermore, within the sample, the ratio of occupational therapists with bachelor’s degrees to occupational therapists with specializations is 4:1. This type of selection bias, known as Neyman bias, may have generated skewed results (Heneghan and Spence, 2017). The main results subject to bias can be found in the modalities of TO intervention in stroke patients with mood disorders and the professional and personal difficulties experienced during intake, which would be overestimated. Finally, the primary outcome was based on a single questionnaire item (Q13). Choosing only one question to answer the primary outcome is surely a limitation, but it gave us more feedback from occupational therapists and clearer answers.
The findings are moderately useful for clinical practice. This research clarifies the type of patients with post-stroke depression, preparing occupational therapists for treatment. In addition, there are indications regarding goals and activities used during OT intake in patients with post-stroke depression. These aspects are necessary to trigger clinical reasoning and outline the rehabilitation intervention.
Conclusions
The aim of this study was to explore the relationship among post-stroke depression, performance in ADLs, and OT intervention in adult patients. The results showed that, following stroke, depressive symptoms arise and impair performance in ADLs. The most affected activities are those related to self-care and work/personal roles. A part of the sample reported that walking is also worse. OT intervention with these patients focuses on increasing volition and sense of competence, to enable occupational engagement. However, OT treatment generates professional and personal difficulties, such as increased recovery time, difficulties in the therapeutic relationship, and frustration.
One of the points highlighted by this study concerns teamwork. Higher levels of post-stroke depression, in fact, are associated with difficulties in personal mobility (Altindag et al., 2008) and speech impairment (Ayasrah et al., 2018). Therefore, it would be interesting to also investigate the characteristics of the intervention of physical therapists, speech therapists, and psychologists to identify a common and shared direction for the different health professionals involved in rehabilitation treatment.
Key findings
There is a relationship between post-stroke depression and performance in ADLs.
Volition plays a primary role in occupational engagement.
OT treatment of patients with post-stroke depression could generate professional and personal difficulties.
What the study has added
This study contributed to the field by exploring post-stroke depression, its impact on ADLs and volitional aspects, through the perspective of occupational therapists. Further research is needed to obtain stronger evidence.
Supplemental Material
sj-docx-1-bjo-10.1177_03080226241246138 – Supplemental material for Post-stroke depression, activities of daily living, and occupational therapy intervention: An observational survey
Supplemental material, sj-docx-1-bjo-10.1177_03080226241246138 for Post-stroke depression, activities of daily living, and occupational therapy intervention: An observational survey by Anello Sara, Diletta Maria Pisaniello and Pier Carlo Battain in British Journal of Occupational Therapy
Footnotes
Acknowledgements
The authors are grateful to the Italian Association of Occupational Therapists (AITO) and the University of Milan for supporting this project.
Correction (October 2024):
Article updated to amend first author forename/surname display.
Research ethics
Not applicable.
Consent
Data were properly anonymized, and a written informed consent was obtained at the time of original data collection. The participants authorized the publication.
Patient and public involvement data
During the development, progress, and reporting of the submitted research, Patient and Public Involvement in the research was not included at any stage of the research.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) declared no financial support for the research, authorship, and/or publication of this article.
Contributorship
All authors prepared the conduct protocol. AS searched the literature and, after a focus group with DMP and PCB, created the questionnaire. DMP participated in recruiting therapists and PCB in analyzing the data. AS wrote the first draft of the manuscript. All authors reviewed and edited the manuscript and approved the final version.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.