
Abstract
Introduction:
Occupational therapy has a central focus on occupation. This calls into question the role and value of anatomy education and knowledge holds for the profession. This research reports on the key findings of a larger, doctoral study which explores the role of anatomy within occupational therapy and examines curricula implications.
Method:
A hermeneutic, phenomenological approach was employed. Semi-structured interviews gathered data from participants in four categories (occupational therapy students, practitioners, lecturers, and profession experts). Thirty-two participants (eight participants per category) were interviewed. Reflexive thematic analysis was utilised. Data were analysed separately for each category and then blended to produce key findings.
Findings:
Challenges and complexities exist with the inclusion of anatomy education in occupational therapy curricula and there remains ongoing debate as to the core knowledge of the profession. Findings revealed continuing challenges with professional identity in medicalised settings and strong influences of the multidisciplinary team and the practice context.
Conclusion:
Occupation-centred anatomy education is suggested to equip students with a strong professional identity, which centralises occupation, whilst still meeting practice-based realities. Developing students’ lifelong learning skills is essential to ensure future occupational therapists take ownership of their learning needs to meet practice-based demands.
Introduction
This study explores the role of anatomy in occupational therapy education and considers its value within the 21st century contemporary paradigm. The study was conducted within the United Kingdom (UK) and as such will reference the professional and regulatory bodies of the Royal College of Occupational Therapists (RCOT) and the Health and Care Professions Council (HCPC). However, the topic is important within the wider, worldwide context of occupational therapy due to ongoing consideration on what should be included within higher education curricula and how the World Federation of Occupational Therapists (WFOT, 2016) Minimum Standards for Education should be interpreted. This article thus reports on the key findings of a larger, doctoral study. Detailed findings can be found in the primary author’s unpublished thesis (Fielden, 2025).
Education programmes should be underpinned by values and beliefs which are central to occupational therapy, in addition to the teaching of core knowledge and skills (RCOT, 2019). The move away from the profession being underpinned by the mechanistic paradigm to a contemporary one (Kielhofner, 2009) means that the profession should focus on occupation rather than underlying performance deficits. The WFOT (2016) makes clear that an occupational perspective must permeate all aspects of an education programme. Occupational therapy roles are varied (RCOT, 2019) and its diversity means that not everything can be covered in curricula. Continuing professional development (CPD) and lifelong learning is actively promoted within the health professions (Broughton and Harris, 2022) and thus skills and knowledge often develop post-graduation. This shift in focus along with curriculum capacity calls into question the role and value anatomy knowledge holds for occupational therapy.
Literature review
The study of human anatomy is a scientific discipline founded in medicine. Anatomy knowledge within occupational therapy is linked to the emergence of the mechanistic paradigm which was heavily influenced by the medical model (Kielhofner, 2009). Knowledge of anatomy (body structure and function) has long been a feature in occupational therapy education and historically the concept of occupation has been built on this foundational knowledge (Bagatell and Womack, 2016). WFOT (2016) indicates that essential knowledge for graduates should include the ‘relationship between body structures and function, as defined in the ICF (International Classification of Functioning, Disability and Health), and human capacity to participate in occupation’ (WFOT, 2016, p. 31). The current, contemporary paradigm within westernised occupational therapy in particular, has less of a focus on dysfunction and underlying impairment and embraces the core tenet of occupation (Kielhofner, 2009).
Occupational science has encouraged the profession to refocus on occupation, the fundamental core of the profession (Yerxa, 2000). Wilcock (2001) argued that the profession was founded on subjects such as anatomy, however, was not focused on occupation and humans as occupational beings. Whilst the importance of occupation and its centrality to the profession is not disputed, there are arguments suggesting that the focus on occupational science has come at the expense of subjects such as anatomy (Bagatell and Womack, 2016; Dove et al., 2022).
The WFOT minimum standards for the education of occupational therapists state that ‘10–30% of the programme is focused on knowledge supporting an understanding of body structures and functions, biomedicine, psychological and sociological concepts’ (p. 46). RCOT (2019) and HCPC (2023) stipulate that knowledge of underpinning sciences including anatomy need to be included within occupational therapy curricula. However, there remains limited curriculum guidance and competing curricula priorities means that designing anatomy content is complex. Delivery can be impacted by several factors, including the underpinning programme philosophy, lecturer experience and preferences, subject time allocation and resource availability (Schofield, 2017).
Internationally, studies have investigated what anatomy knowledge is necessary for practice (Schofield, 2017) and valued within the profession (Legleiter, 2023). Literature suggests that occupational therapists utilise anatomy knowledge to assess service user’s limitations and underpin interventions (Veazey and Robertson, 2023), understand how anatomical issues impact on occupational performance (Giles et al., 2021), guide clinical reasoning (Schofield, 2017), ensure safety in practice (Giles et al., 2021) and communicate with multidisciplinary team (MDT) members and educate service users (Carroll and Lawson, 2014). McAndrew and Kaskutas (2022) argue that subjects such as anatomy should be clearly linked to occupation to promote occupation-centred curricula. By redesigning an anatomy and applied biomechanics course the authors were able to make explicit occupation and link relevant anatomy knowledge. Although a small study at one university, results found statistically significant increases in student self-rated learning objectives, demonstrating anatomy and related subjects can be taught with a clear focus on occupation.
There is a paucity of literature on the inclusion and teaching of anatomy within occupational therapy education, with the majority from the United States of America (USA) (Berrios Barillas, 2019; Berrios Barillas and Lemley, 2021; Giles et al., 2021; Legleiter, 2023; Schofield, 2017; Veazey and Robertson, 2023), and others from Canada (Dove et al., 2024; Ho et al., 2024). Views on the importance of anatomy within occupational therapy curricula are supported within literature (Giles et al., 2021; Legleiter, 2023; Schofield, 2017). However, further research on the learning and teaching of anatomy is needed to ensure student learning outcomes are optimised (Dove et al., 2024). Dempsey et al. (2023) notes a lack of literature investigating anatomy education in occupational therapy. They suggest changes need to be made to how anatomy is taught to enhance student motivation, engagement and thus anatomy knowledge in the healthcare professions.
Literature considering anatomy within occupational therapy programmes within the UK specifically is sparse and research investigating the topic within occupational therapy curricula is needed. This study therefore considers ‘What is the role of anatomy education within the 21st century for occupational therapy programmes based in the UK?’
Method
Underpinned by a relativist, constructionist stance, a hermeneutic phenomenological approach was utilised to explore participant perspectives within education and practice settings. Hermeneutic phenomenology explicitly uses interpretation to explore lived experiences (Finlay, 2011). Interpretation aims to draw out implicit or hidden meanings occurring in context (Finlay, 2011). In hermeneutic phenomenology, it is vital to acknowledge researcher positionality. The primary author (K.F.) has been lecturing in occupational therapy at a UK higher education institution for the past 10 years, has had previous experience as a practicing occupational therapist and as an occupational therapy student. As an occupational therapist educated in Australia and currently working in UK higher education, the different emphasis on anatomy education within both countries was noted and thus motivated the primary author’s interest in understanding the role of anatomy education within education programmes. Reflexivity was essential in managing researcher preconceptions, which is outlined within Quality and Rigour.
Recruitment and participants
With ethical approval from the (University of Cumbria) (Ref: 19/66), a purposive sampling method utilised a variety of sources for recruitment:
Social media platforms X, Facebook and LinkedIn.
Invitation emails sent to occupational therapy departments within UK universities if email addresses were publicly available via the website.
Posting via social media pages of the previous RCOT Children, Young People and Families specialist section.
RCOT OT News magazine advertisement.
Advertising at the primary researcher’s own university student Blackboard platforms and emails to staff within the university’s occupational therapy department.
Inclusion criteria were
Eighteen years of age and over identifying with one of the four categories identified below.
Based in the UK.
Currently part of the occupational therapy community (student, practitioner, lecturer, or profession ‘expert’).
‘Expert’ was defined as those who are leaders in their professional field at a Level 7 or higher on the RCOT Career Development Framework (RCOT, 2021a). This could be but was not limited to: Associate Professor/Professor level in academia, and/or Band 8A and higher or equivalent in the health and social care services.
A larger sample size was needed to gather rich data, reflecting a range of experiences, whilst adhering to study timeframes. As such, eight participants per category were recruited (32 participants in total).
Data collection
Written, informed consent was obtained. Semi-structured interviews were all conducted by the primary author (K.F.) and lasted between 25.19–55.57 minutes. Interview questions were developed from both an initial scoping study and subsequent questionnaire, and apart from the addition of one question after the second interview ‘Why did you choose to study occupational therapy?’ participants were asked the same questions, with supplementary questions based on participant responses. Interviews were conducted online via Microsoft Teams in no set order regarding the allocated category. Interviews were audio recorded and transcribed verbatim by a professional transcriber. Recordings were allocated a pseudonym prior to being sent to the transcriber. Transcripts were redacted of potentially identifiable information. All participants were invited to review their own transcript and request for any other potentially identifying information to be redacted.
Data analysis
Reflexive thematic analysis was utilised as it works with a relativist-constructionist stance (Braun and Clarke, 2022). The primary author (K.F.) conducted the initial analysis which was then discussed with B.Y. and D.C. The notion of the hermeneutic circle (Finlay, 2011) was employed throughout the analysis. This involved the researcher moving back and forth between the words and sentences within the data extract itself and then considering the data extract within the context of the data item and then data set. Both ATLAS-ti and manual data analysis methods were used. Analysis progressed through the six phases of data analysis outlined by Braun and Clarke (2022) initially employing inductive coding and then progressing to a more deductive approach when integrating category findings. Coding was primarily at a latent rather than semantic level (Braun and Clarke, 2022).
Quality and rigour
Within hermeneutic phenomenology, researcher subjectivity plays an integral role in knowledge production; however, researchers should be aware of their own perceptions (Finlay, 2011). A ‘phenomenological attitude’ was employed by approaching the research with openness and empathy (Finlay, 2011). To maintain this phenomenological attitude, a reflexive journal was kept.
Power issues were considered due to the primary researcher’s role as a lecturer, especially when interviewing students. To limit the influence of power the participants were involved in the research on a voluntary basis with the right to withdraw. A pre-interview briefing reiterated that all opinions are valued with a reminder that both the participants and researcher were required to abide by RCOT’s 2015 Code of Ethics and Professional Conduct (now Professional Standards for Occupational Therapy Practice, Conduct and Ethics; RCOT, 2021b). Reflexivity was employed throughout data collection and analysis to consider power issues, and the primary authors own preconceptions. Interview questions were open-ended, allowing participants to discuss what was important to them, however followed a set schedule of questions. Use of pseudonyms and redaction of identifiable data within transcripts were also used.
Participants had the option of checking their transcripts for accuracy in the form of participant feedback. For interest’s sake rather than validating findings, participants had the opportunity to engage in the research process by obtaining their perspectives on the data analysis for their category. A paper trail was also kept for transparency.
Findings
Thirty-two participants participated, with eight participants per category. Tables 1–4 present participant demographic information collected. As this study reports on key findings of a much larger study, sample quotations from a limited number of participants are presented. Figure 1 presents a summary of the individual category overarching themes, key themes and subthemes. Figure 2 displays the blended thematic map which combines the key findings from all categories of participants. The blended themes specifically will be reported on. These include: ‘In The Club: The Power of Practice’, ‘The Push and the Pull: Debating Core Knowledge’, ‘The Great Balancing Act: Anatomy Education for Practice’.
Student demographics.
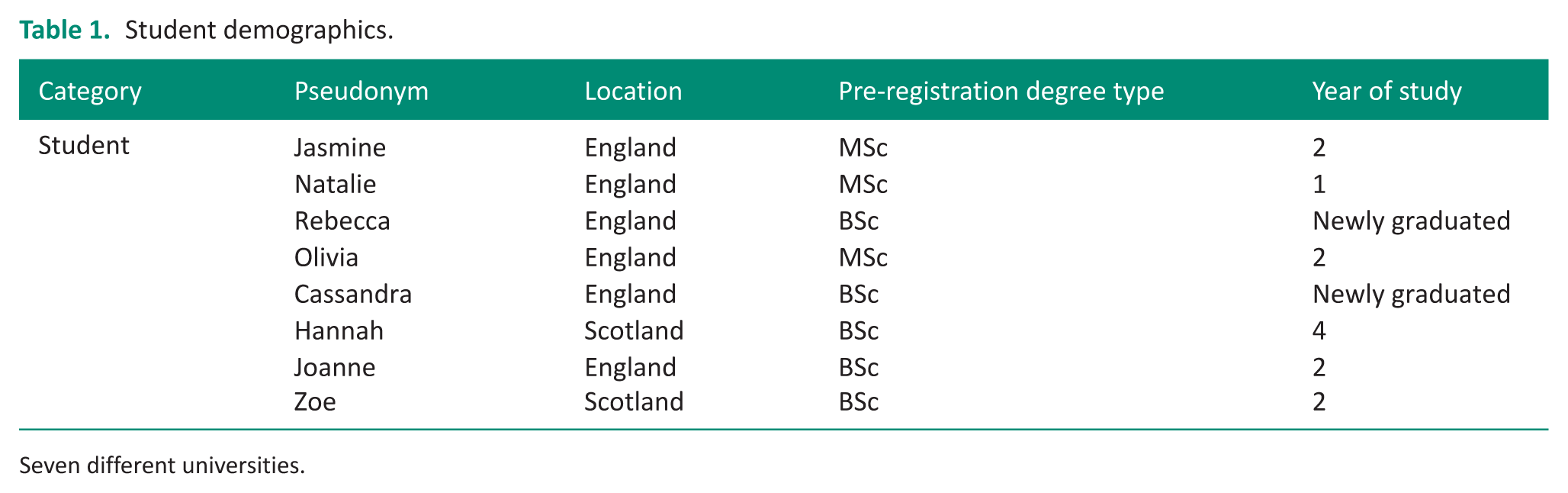
Seven different universities.
Practitioner demographics.
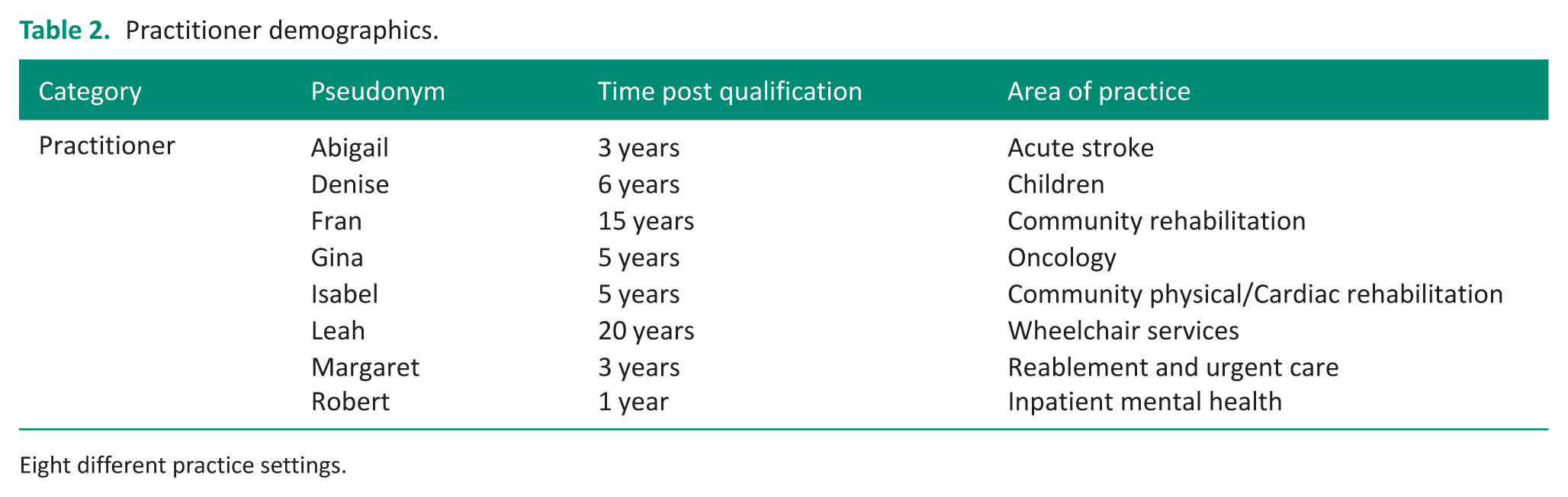
Eight different practice settings.
Lecturer demographics.

Six different universities.
Expert demographics.
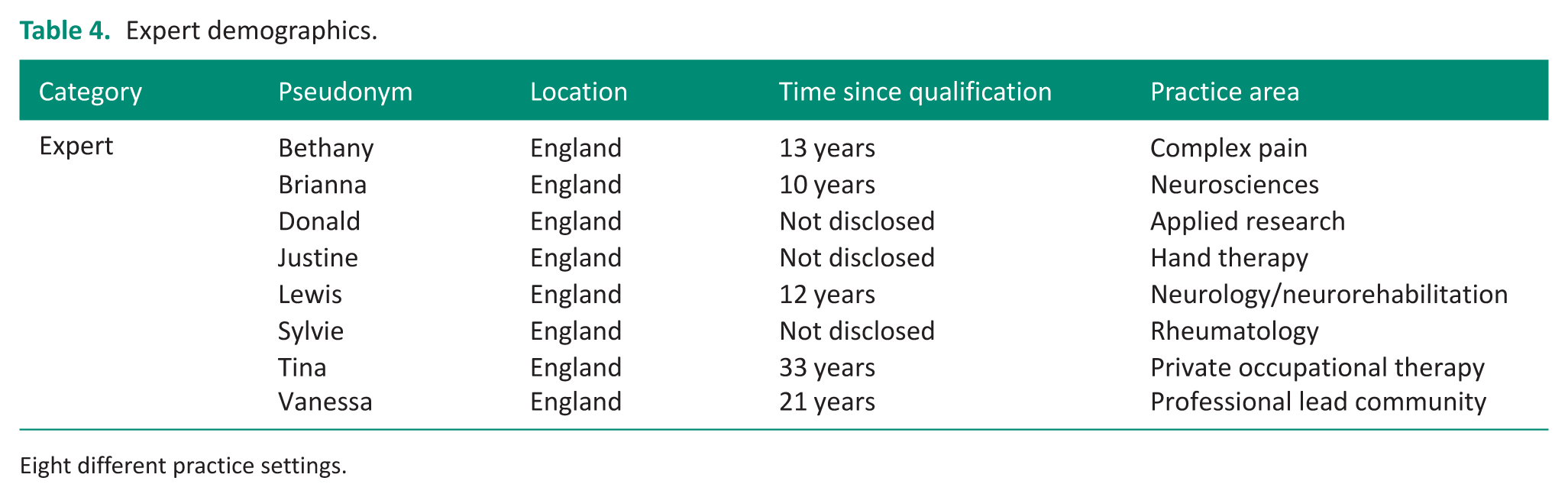
Eight different practice settings.
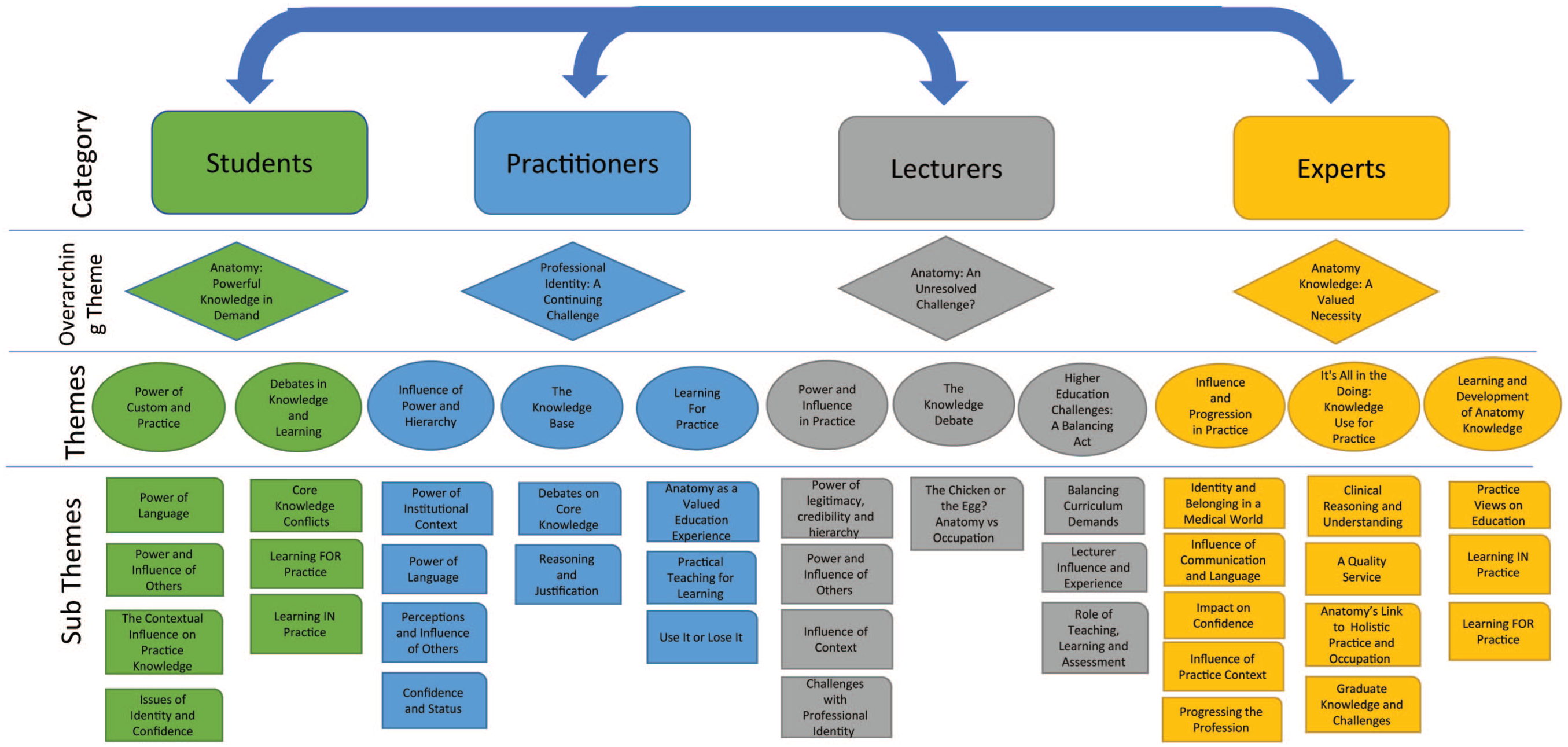
Summary of individual category findings, including overarching themes, key themes and subthemes.
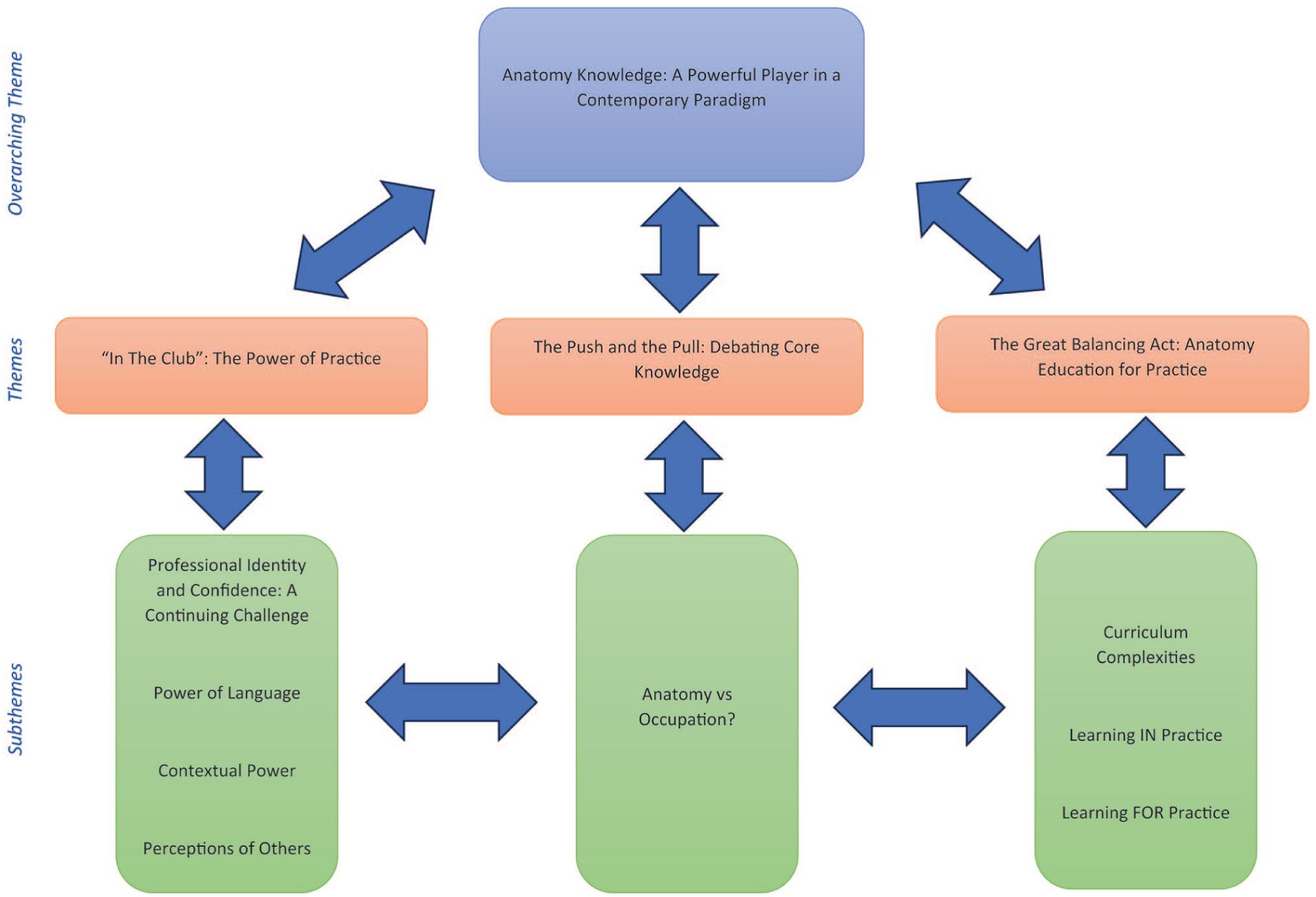
Blended thematic map combining key findings from all participant categories.
Blended theme one – ‘In The Club’: The power of practice
This theme explores the external influences which exert power on the value placed on anatomy knowledge. Factors are suggested to stem from the influence of custom and practice within traditional medical model dominated settings, where medical hierarchy and institutional needs often dominate. For students, anatomy knowledge was linked to confidence in practice, whereas practitioners viewed anatomy as knowledge which would enhance their professional identity. In contrast, the experts viewed this knowledge not only as a confidence enhancer but also as important for helping occupational therapists to advocate and progress the profession by entering into more advanced roles. Lecturers considered more explicitly the influence of the practice context as to whether anatomy knowledge was valued or not. Professional identity and lack of confidence was noted to continue to be a challenge in occupational therapy practice, particularly within medicalised contexts. Anatomy knowledge was often viewed as a ‘way in’ to enter an ‘exclusive club’, in this case the MDT. Lecturer Leanne voices this view:
. . .I think that [pause] there are people within health professions who very much like to have their own language; they like to be in a little bubble of ‘you know actually if you don’t understand this then you’re, you’re not in my gang’ um. . . that kind of status and hierarchy that that affords them. . . . . .I do feel a lot of its language. It’s about being able to converse and sort of enter discourse with those people in, in those terms, in that language.
MDT influence and perceptions of others on the role of occupational therapy was seen to drive the need for practitioners to understand and utilise anatomy knowledge. If they were not able to do this, credibility and respect was felt to be lacking and feelings of not belonging in this medical world were noted. Expert Vanessa considers that occupational therapists need to work at being seen as equals in MDTs and that anatomy knowledge assists them to be seen as scientific and credible within teams.
. . .I think OT always has, is always having to promote themselves and that you are part, you know, that you are. . . equally important in the MDT as sort of Physios and Medics and Nursing, so I think [pause] yeah, I think it’s just to promote OT that it is a science. . .
It was the knowledge of anatomy rather than that of occupation which promoted belonging and confidence within these teams, indicating anatomy knowledge may hold power over occupation-focused knowledge in medically dominated settings. . The power of anatomical language within these settings was notable and reflected in the data of all categories. The use of this discourse was viewed as the key in which to open the door to ‘the club’. Not being able to utilise or understand this language impacted on feelings of credibility and respect. Practitioner Fran articulates this view:
. . . if I could talk the talk, you know, even if it didn’t change my clinical reasoning at all, just being able to talk that medical lingo would, would give me a level of authority with other more medical professionals. . . I think I would, I would maybe have a bit more credibility. . .
Lecturer Martha, however, considers the risks associated with establishing one’s professional identity around anatomy knowledge. She considers that a reason for utilising this knowledge is due to uncertainty around one’s role and difficulties with articulating occupational therapy. Anatomy is seen as an easier body of knowledge to grasp than that of occupation and that this knowledge is used to strengthen professional identity. Martha suggests that the identity of an occupational therapist can then be lost.
. . .I hear this quite a lot, you know ‘oh I’m not sure how to explain occupational therapy’ which disheartens me, you know. And that, that’s where it comes from, isn’t it? ‘I don’t understand occupation, but I do understand anatomy, so I’m going to’, if you’re doing physical obviously, er, ‘I, I will build myself around this and the people will know who I am’, but they won’t know you as an occupational therapist’.
Blended theme two – The push and the pull: Debating core knowledge
This theme considers the value anatomy holds as essential, core knowledge within education. Data showed evidence of conflict and debate as to where anatomy knowledge sits with that of occupation-focused knowledge. There was evidence in the data that anatomy was viewed as foundational on which knowledge of occupation and its application can then be built. Student Rebecca likened the lack of anatomy to somebody removing the bottom rung of a ladder. This implies that this knowledge is foundational on which other knowledge is then built from and developed further. For Rebecca, limited anatomy education at university means that graduating occupational therapists are entering into practice without all the required knowledge needed.
It’s like someone took the first rung off the ladder and all the other rungs are there so you get to go on your placement; you get to do the application; you get to do the Moving and Handling but the bottom rungs gone off the ladder because they thought it was OK not to teach it.
For the majority of participants, this value reflected the nature of the practice setting. Practitioner Margaret suggests that anatomy is central to her practice in a physical health setting.
Erm, yeah, I think it should be at the heart of OT practice really. Erm, I think it should inform what you do I guess specifically in physical health, erm, otherwise I’m not entirely sure where you get your clinical reasoning from if you’re not using anatomy.
With a background in mental health, Lecturer Kathleen, however, holds an alternative view and considers that basic principles of how the body works is sufficient rather than an in-depth understanding. Whilst Kathleen’s is an outside view in the data, it is important to highlight alternative perspectives within the profession.
To be a good OT. You don’t need anatomy. You just need to know principles. You [don’t] need to know all the in, all the innovation and the, and the ins and outs of what muscle’s called what. You just need to know how the human body works, the principles of it, you don’t need to know anything else.
Others also considered occupation as core knowledge with anatomy knowledge viewed as a useful tool to then apply in practice. Expert Lewis considers how occupational therapists utilise their anatomical knowledge with that of occupational engagement and one is not separate from the other. Experts regularly linked anatomy knowledge to holistic practice.
Erm I see the Occupational Therapist’s role as providing the link and the expertise to link anatomy to participation and how people engage meaningfully in their everyday lives.
What was deemed core knowledge was often context dependent. Student Jasmine acknowledged the contextual influence in regards to depth of anatomy knowledge, but expresses that a basic understanding of anatomy is necessary for all occupational therapists.
. . .depending on where you’re going, you should specialise in whatever that is as, you know, you can’t take a scatter-gun approach to the knowledge of anatomy because there’s just too much um. Um however, I think everyone should have a basic understanding of the systems of the body.
Blended theme three – The great balancing act: Anatomy education for practice
This theme considers complexities and challenges of anatomy education within occupational therapy curricula. There was evidence of the challenge when meeting a wide variety of practice-based knowledge demands within curricula. Anatomy was considered important to include; however, the depth and extent of how this should be included varied within categories and often depended on the participants’ specialism. Student, practitioner and expert categories featured data calling for more taught anatomy at university, whilst the lecturer category reflected the complexities of balancing curriculum demands. What was notable within this theme was student ownership of learning and consideration of whose responsibility it is to develop this knowledge if taught anatomy at university does not meet the depth required for a practice area. Learning of anatomy was discussed within two separate areas, learning at university in preparation for practice and learning on the job and via CPD after graduation. Students overwhelmingly considered that more taught anatomy was required at university to prepare them for the challenges in practice. The complexity of learning anatomy was commonly cited, and participants expressed that support was needed to facilitate learning. Self-directed learning for anatomy was not looked upon favourably as Student Joanne noted:
My problem with self-directed anatomy is how do you know if you’re on the right track? How do you know if you’re reading and this is how you’ve understood it, if it’s correct? Cos it’s a complicated thing anatomy and physiology, really complicated. . .
However, their student status meant that they were yet to experience this knowledge developing and expanding in practice. Whilst practitioners considered anatomy as essential for inclusion in the curriculum and that more should be included, they took this one step further and discussed the importance of practical application of knowledge and integrating this knowledge with other modules. Their contextual experience meant that they were able to consider the importance of practical application of knowledge, as Practitioner Abigail notes:
I think it needs to be a balance because we are occupational therapists and occupation is at the heart of what we do, so that’s where I think the, the application of the knowledge maybe needs to be explored a bit more in the, these settings. . .
Experts discussed the importance of including a basic level of knowledge but considered the importance of CPD and learning on the job to develop specialist knowledge needed for practice as Expert Sylvie suggests:
. . .of course, a lot of the rest can be in-house training because that’s what happens when you go into the clinical, you know, when you’re starting your erm, er Band 5 post depends on where you, you know, it’s – I’m not saying that it’s all in the Degree but I think we need to give that basic knowledge to build their confidence. . .
Conversely, the majority of lecturers commented on complexity within curricula and the difficulties in trying to meet the requirements set out by the professional body in addition to practice-based needs and demands. Their experience as both practitioners and educators meant that they could see both sides of the coin. Lecturer Samuel summarises this challenge:
. . .when you send students out, er, they decry the lack of, er, anatomy knowledge and so on and so forth and are, you know, they think it’s disgraceful and everything else, er, and I’ve been part of that brigade as well. Erm, but I think one of the things I have learnt coming into higher, higher education is, you know, you can only, you can only teach so much. . .
Discussion and implications
Participant voices argue that taught anatomy in occupational therapy curricula is a highly important topic, linked to practice demands. Participants expressed the need for more taught anatomy within education programmes. However, this teaching and learning needed to be linked to practical application and practice-based realities. Understanding and use of anatomical knowledge and language, rather than occupation specific knowledge, was seen as vital for the profession to be deemed credible, particularly within medicalised settings.
There was evidence to infer that the value which is often placed on this topic within occupational therapy may feed into continuing struggles with professional identity, confidence and role clarity. Occupational therapists’ challenges of working within a dominant medical model is well documented in the literature (Britton et al., 2015; Molineux and Baptiste, 2011; Murray et al., 2021; Turner and Knight, 2015; Walder et al., 2021) and findings from this study demonstrate that there is a continuing struggle by occupational therapists to establish a strong professional identity. Findings suggest that the occupational therapist’s position, particularly within acute, physical health settings, was often viewed as lower in the hierarchy compared with other multidisciplinary colleagues. Anatomy knowledge was viewed as a way of strengthening one’s position and credibility within this hierarchy. Phrases such as ‘wishy washy’ and ‘airy fairy’ were used to describe occupational therapy, illustrating negative views of professional identity and a lack of confidence in some participants within their role. The profession’s struggles with professional identity have been well documented (Walder et al., 2021) and evidence within this study demonstrates that these struggles are continuing.
Reasoning as to why anatomy knowledge and the use of anatomical language in medicalised practice settings was needed, often linked back to the MDT. There was evidence that occupational therapists need to use this language to feel a sense of belonging within these environments. This supports Cole and Tufano’s (2020) suggestion that whilst occupational therapists continue to work within settings dominated by a medical model, then understanding the common language of the medical model is essential for the maintenance of professional relationships. For participants, this inclusion was important to then be able to practice with an occupational focus. However, it is suggested that this view runs the risk of further shifting the core focus of occupational therapy from occupation to anatomy, leading into a cycle of confusion for the profession.
These findings give support to literature which reinforces the importance of anatomy teaching and learning within occupational therapy curricula (Carroll and Lawson, 2014; Giles et al., 2021; Legleiter, 2023; Schofield, 2017). The demand for more anatomy teaching was prominent within the student, practitioner and expert categories and reflected participant experience. Students strongly felt that more taught anatomy was required in higher education, whilst experts considered that a basic understanding is necessary, with CPD important for enhancing specialism-based knowledge. Practitioners reflected on the need for anatomy teaching to be practically applied.
The complexity of balancing programme demands means that not everything can be taught. The wide range of practice settings occupational therapists work in adds to this complexity. It is thus argued that students must be introduced early on to vital lifelong learning skills. Lifelong learning and CPD are imperative for occupational therapists (Broughton and Harris, 2022), thus practitioners have a responsibility to further develop their anatomy knowledge should they require it. It is argued that curriculum standards, both within the UK and internationally, should consider providing additional direction for education providers. This should include guidance on anatomy curriculum content and clarity of the responsibilities of the education provider and learners in obtaining this knowledge.
It is suggested that using anatomy knowledge and language to align with dominate voices within medical settings potentially risks occupational therapists losing their unique, occupation-centred focus. Thus, it is argued that these findings need to be considered in light of literature which calls for occupation-centred education programmes (Di Tommaso et al., 2019; Hooper et al., 2015, 2020; Krishnagiri et al., 2017; Walder et al., 2021). Occupation-centred education is curricula which centralises occupation as the core of all learning and teaching (Di Tommaso et al., 2019) and can work towards strengthening professional identity (Walder et al., 2021). McAndrew and Kaskutas (2022) demonstrate feasibility when designing an anatomy module with occupation at the centre of teaching. Hooper et al. (2020) consider that occupation is the core subject of occupational therapy and other elements such as anatomy are identified as topics rather than a core subject. Occupation-centred curricula is one where topics are taught; however, occupation is centralised and is impossible to ignore (Hooper et al., 2020). It is therefore suggested that anatomy education has an occupation-centred focus so that the core construct of occupation when teaching anatomy is not lost. For example, one could analyse the occupation of drawing by examining the musculoskeletal anatomy of the upper limb which allows the person to engage in that occupation. This approach then aligns with the WFOT (2016) Minimum Standards for the Education of Occupational Therapists ensuring that all facets of a programme is linked to occupation. By centring occupation in anatomy teaching, it is argued that occupational therapists can then utilise their anatomy-based language and knowledge but also clearly articulate their unique, occupation-centred perspective.
From these findings, the following suggestions for occupational therapy education are made:
Anatomy remains an essential element within occupational therapy education programmes to ensure students have the knowledge and confidence for practice.
Students should be empowered to take ownership of their learning for future practice.
Education providers are encouraged to deliver anatomy content utilising an occupation-centred approach. Further research and guidance on how to design occupation-centred taught anatomy content is needed.
Professional bodies are encouraged to strengthen their guidance on anatomy inclusion within higher education curricula to ensure consistency in taught content.
Limitations
Recruitment was primarily via online platforms potentially limiting the range and diversity of participants. Participants were predominantly, although not exclusively, white British women educated within the UK from acute physical health backgrounds; therefore, findings should be considered with this in mind. These participants may have had a vested interest in the topic of anatomy whilst those working in settings where anatomy is not overtly considered may have felt that the study was not relevant to them. The voice of occupational therapists working in alternative settings is therefore suggested and thus is currently under investigation as a post-doctoral research project by the first author (K.F.).
Implications for occupational therapy
This study advances the profession’s understanding of why anatomy is often sought after knowledge in practice. It identifies underpinning reasons as to why struggles with professional identity persist in settings dominated by a medical model. It is therefore essential that curricula is developed which promotes a strong professional identity and empowers students to embrace lifelong learning and learning ownership. This study argues for the centralising of occupation in curricula with specific reference to the topic of anatomy. Consideration of how to design and deliver anatomy education which addresses practice-based realities whilst also adhering to the fundamental philosophy of occupation is needed.
Conclusion
This study explores the role of anatomy within occupational therapy education and considers its value within the contemporary paradigm. Anatomy is essential curricula content which ensures new graduates possess vital knowledge and confidence to meet practice-based realities. However, anatomy education must be underpinned by the core philosophy of occupation. The value of an occupation-centred approach to anatomy education has been discussed as a way of addressing this. This research has demonstrated that a dual focus on anatomy and occupation is essential within curricula to ensure graduates are able to meet practice demands, can explain their unique contribution within MDTs, and are confident professionals with a strong occupation-centred, professional identity.
Key findings
Challenges with professional identity continue in medicalised settings.
Ongoing debate on the core knowledge of the profession remains.
Anatomy knowledge and practical application is essential in curricula, however, needs to be foregrounded by occupation.
What the study has added
Occupation-centred anatomy education is vital within curricula to ensure new graduates possess essential knowledge which allow them to meet practice-based realities and equip them with confidence in medicalised settings.
Footnotes
Ethical considerations
Ethical Approval obtained via University of Cumbria’s Research Ethics Panel (Ref: 19/66) on 20.08.2020
Consent to participate
Written, informed consent was obtained from all participants prior to data collection
Author contributions
K.F. researched literature, conceived the study, gained ethical approval, facilitated participant recruitment, conducted the data analysis and wrote the first draft of the manuscript. B.Y. and D.C. provided supervision throughout. All authors reviewed and edited the manuscript and approved the final version.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research received funding from the University of Cumbria for the use of transcribers (0904-20)
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Patient and public involvement data
During the development, progress, and reporting of the submitted research, Patient and Public Involvement in the research was included in planning and progress of the research (small scoping study and questionnaire conducted in planning phase of the research)