
Abstract
Introduction:
The environmental and socio-economic realities of people with spinal cord injury (SCI) living in low-middle-income countries (LMIC) present challenges to engagement in meaningful occupations following discharge from rehabilitation. Participation depends on adaptation to occupational disruptions. The purpose of this study was to determine the disruption of occupational-identity, -competence and -settings among people with SCI in a LMIC. The association of occupational disruption and health-related quality of life (HRQoL) was also considered.
Methodology:
A cross-sectional quantitative study assessed 29 people with SCI, 4 months post-rehabilitation, using the Occupational Performance History Interview 2nd Version (OPHI II) and the European Quality of Life (5-dimensions and 3-levels) (EQ-5D-3L) survey.
Results:
Total interval key scores on a scale of 100 for occupational identity (49.97) and competence (51.21) were higher than those for occupational settings (38.62). Present functioning in occupational -identity and -competence was significantly lower (p = 0.001) than previously. However, HRQoL was most affected by pain and discomfort, with a low correlation between scores for mobility, usual activities and self-care and occupational disruption (r = -0.37–0.34, p ⩽ 0.05).
Conclusion:
Results suggest strengthening occupational therapy services post-discharge, with a focus on occupational settings disruption, particularly to support engagement in work and leisure, facilitating occupational identity and competence are required.
Keywords
Introduction
Spinal cord injuries (SCIs) result in permanent disability, challenging the ability of individuals to engage in everyday activities. The prevalence of secondary health conditions, such as pain, pressure sores, spasms, bowel and bladder problems, mental health concerns, as well as loss of roles and independence, all affect the health and well-being of people with SCI (Alves et al., 2023). While inpatient rehabilitation addresses some of these challenges, the reintegration into the home and community setting for a person living with SCI may present other activity limitations and participation restrictions and influence health-related quality of life (HRQoL; Alve and Bontje, 2019; Hossain et al., 2019). Barriers to participation or an individual’s involvement in life situations (World Health Organization, 2001) and reintegration into the family and community depend on dealing with a ‘new self’ disability (Joseph et al., 2016). Disruption in occupational identity and occupational competence of a person with a SCI affects adaptation to and acceptance of the injury. Adaptation is the process of constructing a new occupational identity and achieving occupational competence through meaningful, sustained engagement in daily life (Mohorič and Tavčar, 2024).
Kielhofner (2008) emphasized that the development of a positive occupational identity and occupational competence, established through interaction with occupational settings, is crucial to the adaptation process following a disability. Occupational identity and occupational competence are defined by Kielhofner in his seminal work on the Model of Human Occupation (MOHO; Kielhofner, 2008). MOHO describes the interaction between the human internal system, engagement in meaningful occupations (everyday activities) and the occupational settings within the environment using a dynamic open system model. Individual differences influence how people choose, participate in and maintain daily routines to achieve their sense of occupational identity and occupational competence by engaging in purposeful occupations that they want, need, or are expected to do in their daily life. This includes the ability to accept responsibility for life choices.
Thus, occupational identity is the cumulative subjective perception of who one is and wishes to become as an occupational being. Occupational competence represents more than occupational performance; it embraces perceived internal resources that enable the individual to use their occupational identity within culturally defined daily occupations (Kielhofner, 2008; Mohorič and Tavčar, 2024). All daily occupations take place in and are moderated by the occupational settings, which include spaces, resources and social supports in the home, work and leisure environments, which are mediated by cultural, socioeconomic and political elements. These factors constitute the context for performance, which must be considered as facilitatory or challenging to the adaptation to a SCI (Ishibashi et al., 2013; Walder & Molineux, 2017).
Research indicates that adaptation to SCIs in high-income countries with gross national income GNI > US$ 14.05, where the average person earns enough to enjoy a high standard of living and access to quality services like healthcare (Metreau et al., 2024) is facilitated by community accessibility, policies providing social security and insurance, telecommunication and transportation services. South Africa is a low-middle-income country (LMIC) defined by the World Bank as having a GNI of US$ 1.14–14.05, experiencing underdeveloped health systems, limited resources and higher burdens of disease complicating adaptation following an SCI (Metreau et al., 2024). Thus, adaptation to a SCI is impacted by resource-constrained occupational settings, which, when coupled with socio-economic hardship, present considerable challenges for people with SCI in coming to terms with their disability (Borg et al., 2020) and re-establishing engagement in their daily occupations (Alve and Bontje, 2019). The lack of services acts as a constraint, resulting in loss of employment, the risk of poverty, inaccessible homes, poor road access to homes, inaccessible public spaces and a lack of appropriate assistive (Joseph et al., 2016; Löfvenmark et al., 2016). In addition, cultural barriers to participation include stigma and negative attitudes to disability, resulting in social isolation and the injury being seen as a punishment or a curse (Löfvenmark et al., 2016).
As in HICs, barriers to participation after SCI are exacerbated by secondary health conditions and psychological distress affecting HRQoL, which may present as depression, loss of hope and feelings of failure. Although HRQoL has been related to self-efficacy, which enhances and is reinforced by occupational competence (Tan et al., 2020). The relationship between HRQoL and acceptance of SCI, which facilitates the creation of a new, positive occupational identity, is not clear (Van Leeuwen et al., 2012). Gurung et al. (2023) noted that the socio-structural and environmental factors also impact HRQoL and in LMICs, there is very limited access to health care for secondary health conditions due to a lack of personal resources, such as finances and transport needed to access services (Mohan and Deb, 2023), resulting in further disability or even death (Hossain et al., 2019). Reintegration into communities is influenced by the lack of access due to poor infrastructure, resulting in poor life satisfaction (Filipcic et al., 2021).
The purpose of this study was to determine the nature and extent to which people with SCI in a LMIC experience disruption in occupational identity, occupational competence and the effect of the occupational settings post-rehabilitation, as well as the association between these three variables and their HRQoL.
Methodology
Research design
This study used a quantitative cross-sectional design. Ethical clearance was granted by Faculty of Health Sciences, University of the Witwatersrand Human Research Ethics Committee (certificate number M231107). Additionally, permission was granted by the Gauteng Department of Health to conduct the research. Ethical procedures adhered to the World Medical Association Declaration of Helsinki 2024.
Population and sampling
The population for the study consisted of the people with paraplegia who received rehabilitation at Tshwane Rehabilitation Hospital, one of two public sector rehabilitation hospitals in South Africa. Inclusion criteria for the study comprised those who acquired paraplegia from a SCI at T4 or below, regardless of the cause, who achieved Landrum outcome Level 4 (community reintegration) or Level 5 (community reintegration and employment); (Landrum et al., 1995) on discharge and had been living in the community for at least 4 months before the data collection period. Exclusion criteria were SCI coupled with brain injuries and patients who were 3 months or less post-discharge from neuro-rehabilitation.
A review of the admission and discharge registers over 1 year before the data collection indicated a population of 78 possible participants between the ages of 18 and 60 years. Based on this population, a sample size of 35 participants was calculated to achieve a confidence level set at 90% with a 10% margin of error appropriate for small samples. Convenience sampling was used to recruit the participants. The confidence level was reduced to 80% due to the limited number of patients who could be traced, resulting in a final required sample size of 28 (Barlett et al., 2001). Sample selection bias resulted from the unavailability of potential participants and the use of one public sector rehabilitation facility servicing people with no medical insurance.
Those who agreed to participate were sent the approved information sheet explaining the details of the research. The participants then signed a consent form for participation and for the data collection session to be audio recorded.
Research instruments
Demographic questionnaire
A demographic questionnaire was designed specifically for this research to collect background information about the participants. This included age, gender, diagnosis, level of outcome at discharge, as well as the occupational and educational status of the participants.
The Performance History Interview–Version 2.1
The Occupational Performance History Interview 2nd Version (OPHI II; Kielhofner et al., 2004) was developed to gather information about an individual’s past and current occupational functioning and has an occupational competence, occupational identity and occupational setting scale. The OPHI II consists of three parts:
i) semi-structured interview, which explored the client’s life story,
ii) three evaluation scales, which measure the client’s occupational identity and occupational competence and the impact caused by their occupational settings and
iii) the narrative curve that outlines the client's life story over time and critical events (Hemmingsson et al., 2017). (This section will not be reported in this paper).
The tool has been standardised and includes semi-structured interview questions that enable the collection of qualitative information as well as three standardised scales (Kielhofner et al., 2004):
• The Occupational Competence scale, which was designed to measure the extent to which a client can sustain a pattern of occupational behaviour that is productive and satisfying (Kielhofner etal.,2004).
• The Occupational Identity scale that measures the extent to which a client has internalised a positive occupational identity (Kielhofner et al., 2004). This measures whether the client had values, interests and confidence; sees self in various occupational roles; and has a mental image of the kind of life they desire (Kielhofner et al., 2004).
• The Occupational Settings scale addressed the environmental impact on the person’s occupational life (Kielhofner et al., 2004). The tools have a four-point rating system with four indicating exceptionally competent occupational functioning; three indicating good, appropriate, satisfactory occupational functioning; two indicating some occupational functioning problems; and one indicating extreme occupational functioning problems (Kielhofner et al., 2004).
• The total score on the OPHI II for occupational identity, occupational competence and occupational settings scales is reflected as a client measure or total interval key score out of 100. These scores were accessed in the test manual for each participant, with scores of 50 or less (indicating the majority of scores as 1 or 2) considered as a clinically significant disruption in occupational functioning (Kielhofner et al., 2004).
The validity of the OPHI II scales was assessed using Rasch analysis with 151 raters and 249 participants receiving therapy for physical and psychiatric disabilities. The mean square fit statistic indicated no misfits for any items on the scales, indicating all items were valid indicators of the constructs. Validity measure of participants was indicated by 91% for the occupational competence scale, 92% for the occupational identity and occupational settings scales, with person separation indexes between 4.06 and 2.75 indications of the ability of the assessment to discriminate dysfunction. The ability of the raters to use the scale was confirmed by low rater separation scores of 1.28, 1.78 and 1.94 for the competence, identity and settings scales, respectively (Kielhofner et al., 2001).
The European Quality of Life
The European Quality of Life (5-dimensions and 3-levels) (EQ-5D-3L; EuroQol, 2025) is a versatile health-related QoL instrument that is widely used as a patient-report outcome measure (Devlin et al., 2020). The tool has been used internationally and has been translated into 176 languages, including South African languages (Marsh and Truter, 2021). It has been applied to and validated for spinal cord injury (Diop and Epstein, 2024). Thus, the EQ-5D-3L instrument was a viable option to measure HRQoL across different patient populations, including rural and urban populations in South Africa (Burnand et al., 2021). The tool consists of five dimensions (5D) for describing the health states: A: Mobility; B: Usual activities; C: Self-care; D: Pain and Discomfort, and E: Anxiety and Depression. The questions under each dimension are scored on a three-point scale of: No (1), Moderate (2) and Extreme (3) (EuroQol, 2025). Permission to use the tool was received from Euroqol.org.
The EQ-5D-3L shows moderate-to-good test–retest reliability, with intraclass correlation coefficients (ICC) commonly reported around 0.64–0.76 and Kappa values indicating acceptable stability. Convergent validity to the World Health Organization-5 Well Being questionnaire ranges from r = 0.61 to 0.24. A major limitation is a “ceiling effect” greater than 15%, which is commonly observed in the general population and less severe patients, where respondents cluster at the highest health state. The EQ-5D-3L is generally easy to understand, with low missing values (<3%) in the general adult population, with education level having a minimal effect (Janssen et al., 2013). The measure was also valid when used as a text message in a South African study, with acceptable agreement between the paper and text message (ICC = 0.84; 95% CI 0.78–0.89; (Burnand et al., 2021).
Research procedure
Potential participants were contacted by the first author to schedule an interview, which could be done either telephonically, online, or in person. All participants had an opportunity to review an information sheet about the study in the language of their choice before providing informed consent to participate. Face-to-face data collection was not always possible, as most participants had relocated to different provinces across the country. The structured interview included completing questions on the demographic questionnaire initially. This was followed by the presentation of each item of the three scales on the OPHI II. All interviews were recorded, taking between 28 and 50 minutes. The interviews were conducted in English, with the first author explaining or assisting with the explanations in the client’s home language if required. Finally, the participants completed the EQ-5D-3L survey in the language of their choice, either in a pen and paper format or as a survey on WhatsApp and returned it to the researcher.
Data analysis
The OPHI II scales were scored by the researcher from the recordings of the interviews as per instructions in the test manual. All data were manually extracted into an Excel spreadsheet. Data were analysed using STATISTICA 14.0 (TIBCO Software Inc, 2021) and the demographic information, OPHI II scales and the EQ-5D-3L scores were analysed descriptively. Friedman ANOVA was used to rank the scores for the OPHI II occupational identity scale, occupational competence scale and the occupational setting scale and the EQ-5D-3L. The frequencies of scores for these domains were used to determine the level of disruption based on the normative scores for the OPHI II. A McNemar's test was used to determine the change in the percentage of participants with disruption in occupational identity and occupational competence before and after the SCI. A Spearman’s non-parametric correlation coefficient was used to accommodate the small sample and ordinal data to determine the association between the occupational identity scale, occupational competence scale and occupational setting scale and the HRQoL scale. Significance was set at p = 0.05.
Results
Of the 72 potential participants, 28 could not be contacted, 15 refused the invitation to participate, so a sample of 29 participants was achieved, reflecting a 40.27% response rate. The youngest participant was 20 years old, with the oldest participant being 53 years old, while the mean age was 33.42 years. Most of the participants were males (79.31%; Table 1).
Demographics of the participants (n = 29).
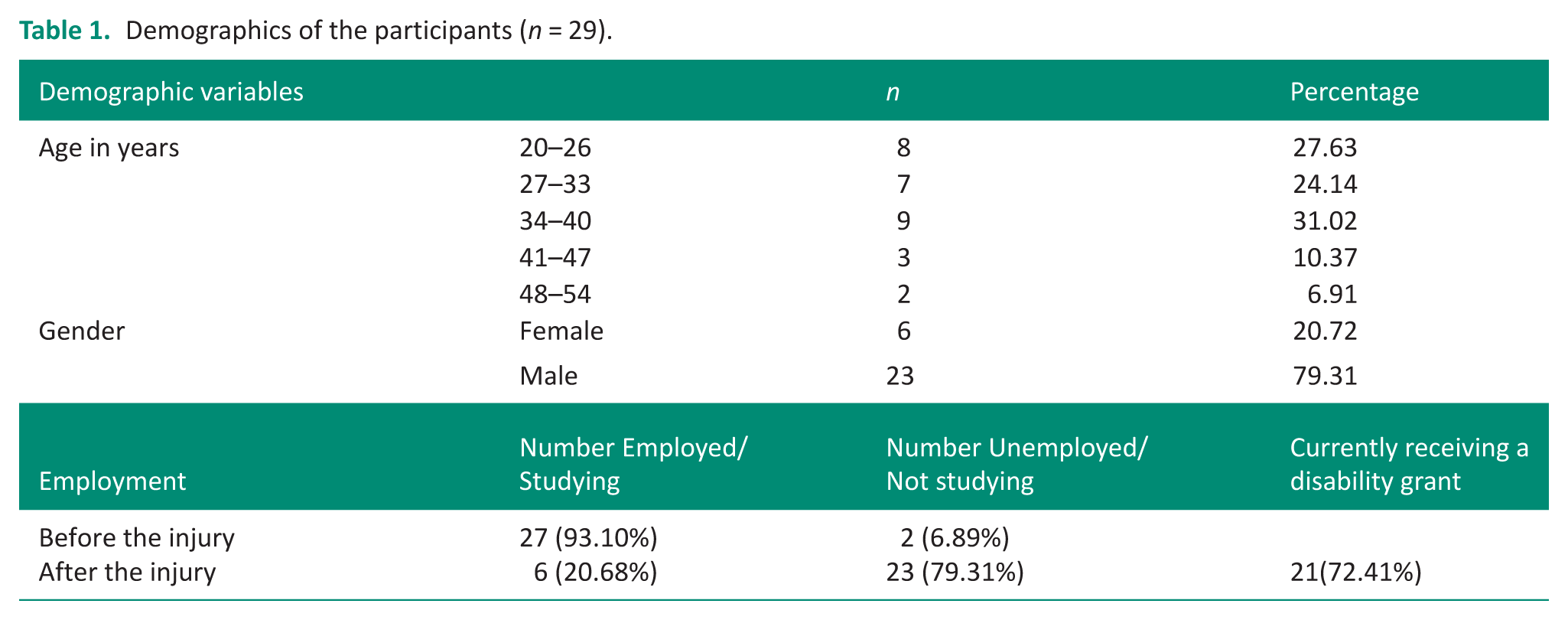
Most participants (89.74%) suffered a traumatic SCI resulting mostly from gunshots, motor vehicle accidents and stabbings, while the non-traumatic SCI were a result of TB spine. Twenty-three participants were discharged on Lundrum level 4 and the remainder on Lundrum level 5. Before their injury, over 90.00% of participants were employed or studying. After the injury, 79.31% were no longer working or studying, and over 70.00% were receiving a government disability grant of £104.00 a month. Those who did not receive the disability grant were foreigners or were formally employed, and thus, not eligible to receive the grant.
All participants reported needing transportation because the roads and the pavements were not accessible for wheelchair users. Following their injury, 69.24% relied on public transport, with most using e-hailing transportation, such as Uber, Bolt rides. Participants reported seldom using public minibus taxis, which although cheaper, were inaccessible. Only 30.82% had access to private transport, which included a family/relative or friend’s car that they relied on for transportation. None of the participants reported having an adapted car.
Occupational identity
The total interval key score (49.97) was on the cutoff score of 50, which indicates occupational disruption for occupational identity. These results indicated that some aspects of occupational identity were experienced as challenges (score of 2) and extreme challenges (score of 1) in five out of eight factors. These included Identifying a desired lifestyle, Has personal goals and projects, Has interests, Recognising their identity and obligations and Has commitments and values, which had a lower average rank on the ANOVA scores than other variables (Table 2).
Scores for occupational identity, competence and settings scales.
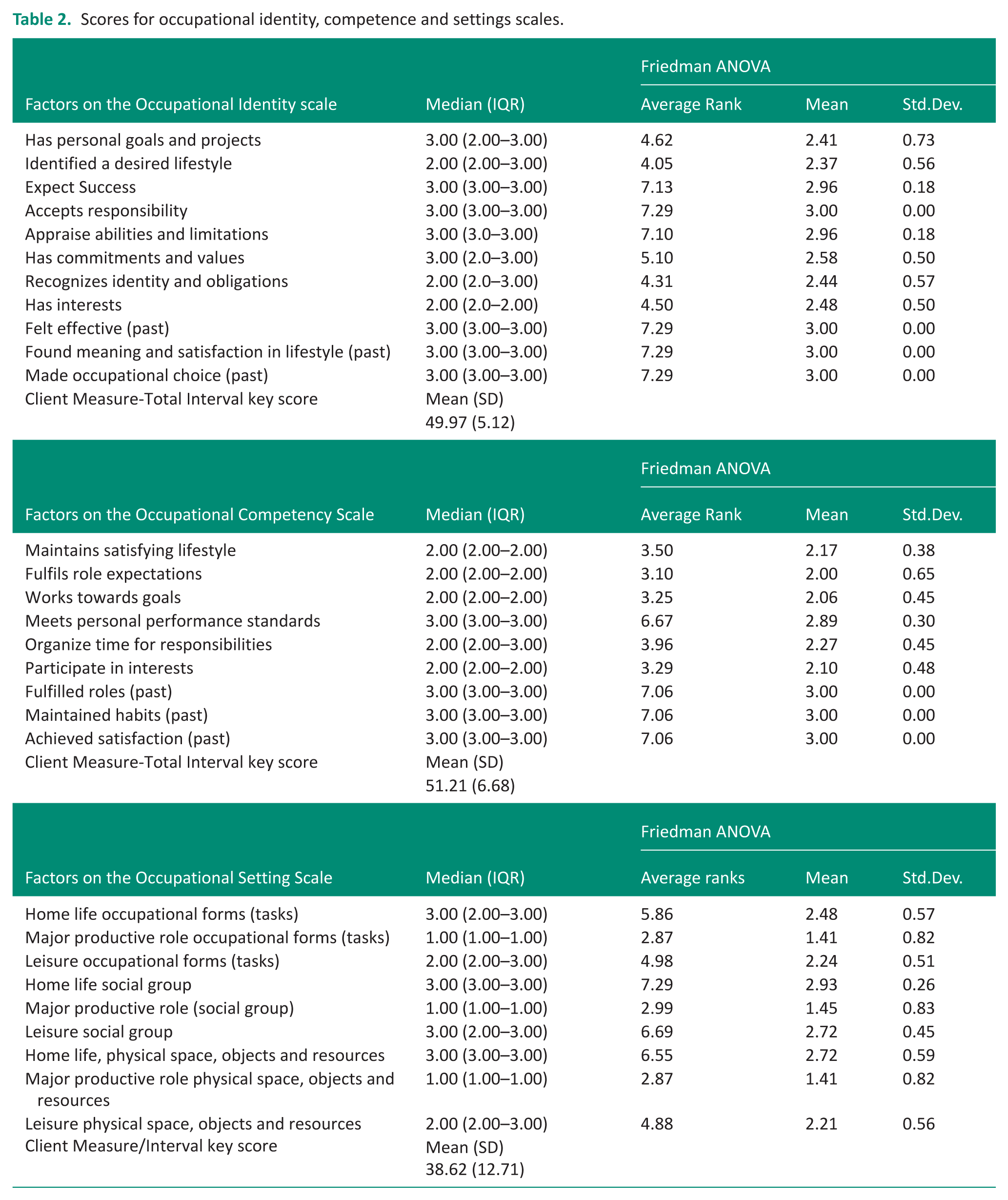
ANOVA scores indicated significant variance between the item scores (p = 0.001). Higher item rank scores indicating a higher median value for Felt effective(past), Found meaning and satisfaction in lifestyle (past) and Made occupational choice (past) suggest a consolidated occupational identity in the past.
Occupational competence
The occupational competence scores indicated that most participants experienced more occupational challenges and extreme challenges with five of the six occupational competence factors. ANOVA scores indicated significant variance between the item scores (p = 0.001) and lower rank scores for Fulfilling role expectations, Participating in their interests, Working towards the goals, Maintaining a satisfying lifestyle and Organize time for responsibilities were found (Table 2). Challenges with Meeting personal performance standards were reported less often and mostly related to their performance of their basic Activities of Daily Living (bADL).
For the past occupational competence of Fulfilled lives, Maintained habits and Achieved satisfaction, all participants had a score of 3. This represented average hardships expected as reported for occupational identity, with their perceived occupational competence as good, appropriate and satisfactory before their SCI.
Occupational settings
Table 2 reports on the challenges and functioning in the occupational settings. Participants reported fewer challenges for Home life social group and Home life physical space, objects and resources, with good social function in this setting and the ability to manage their social and mobility needs at home. In the work environment, extreme challenges were reported for Major productive role: physical space, objects and resources, occupational form and social groups since most had lost their jobs or not been able to return to work. Participants reported challenges for Leisure occupational forms (tasks) and Leisure physical space, objects and resources, but with good social function. Therefore, participants’ occupational settings did not support the reestablishment of occupational identity and competence related to work and leisure, since the total interval score was 38.62, indicating marked occupational disruption.
Occupational disruption
Just more than half (55.18%) of the participants had occupational identity disruption and a client factor/total interval key score below 50, indicating occupational functioning problems (Figure 1). There was a significant difference between the percentage of participants scoring above 50, indicating no disruption for occupational identity, reflecting past (100.00%) and present (44.83%) occupational identity (p = 0.001). A similar result was found for occupational competence, where a lower percentage of participants (37.83%) who scored above 50 for present, whereas 100% had scored above 50 in the past. Most disruption was identified for occupational settings, where 86.20% of participants achieved a client factor/total interval key score below 50.
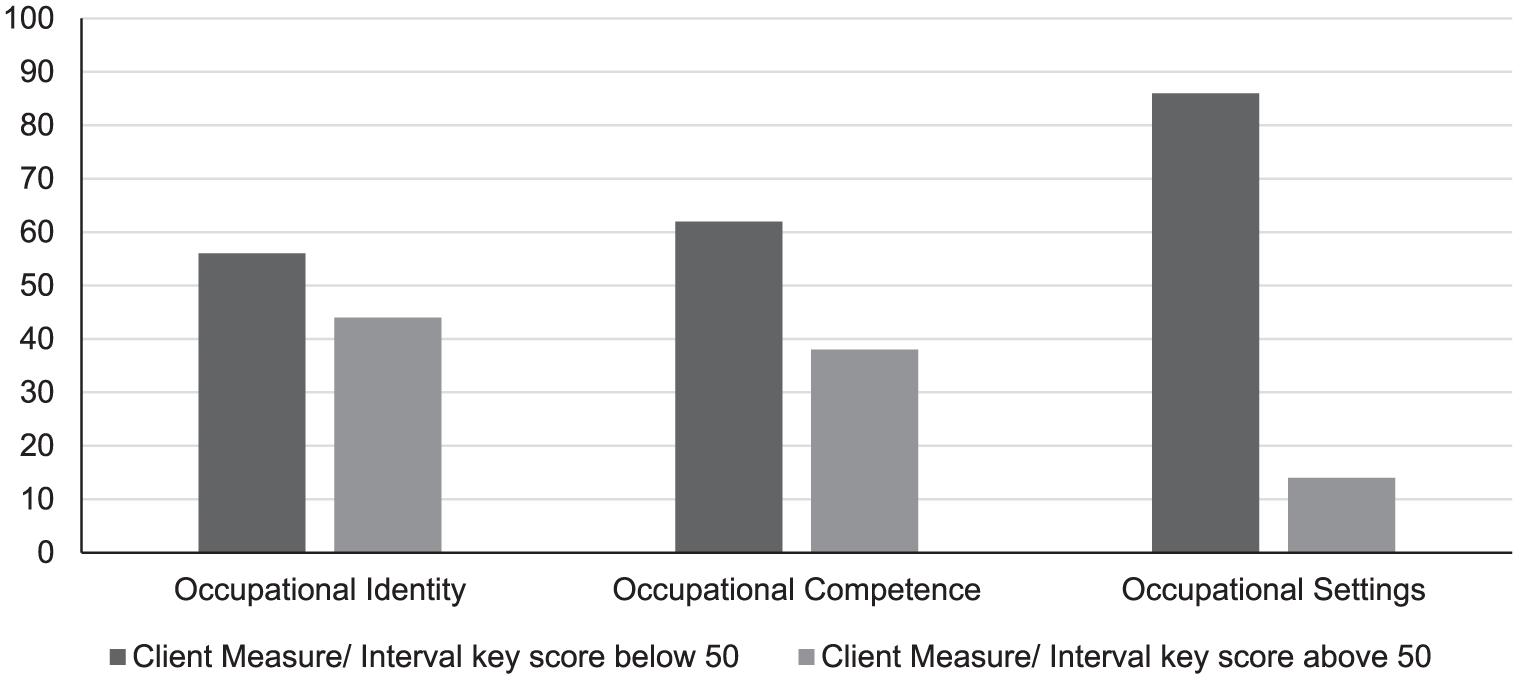
Percentage of participants with client factor/total interval key scores below and above the cut-off of 50 indication occupational disruption.
Quality of life
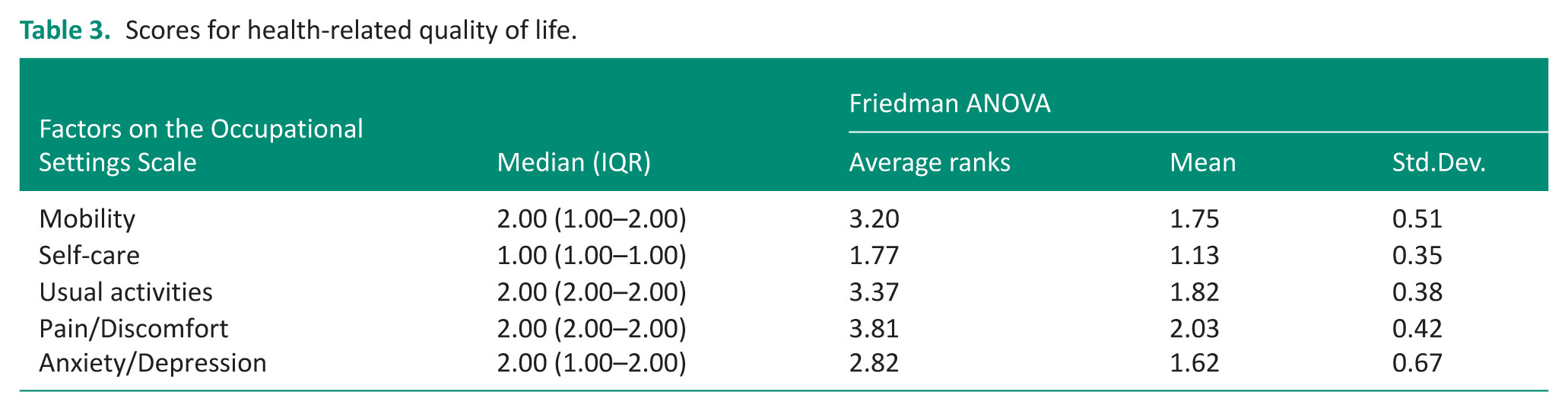
Table 3 describes the participants’ reported HRQoL dimensions on the EQ-5D-3L. The highest scores indicate poor HRQoL related to Pain and discomfort and Usual Activities. While participants reported that their self-care activities did not impact HRQoL. Mobility and Anxiety and depression had a moderate effect.
Scores for health-related quality of life.
There was no to little correlation between HRQoL and occupational competence, with significant low, moderately negative association between occupational identity and HRQoL. Lower occupational identity total interval key score scores were associated with higher EQ-5D-3L Mobility and Self-care scores, indicating poor HRQoL in these domains. The occupational settings total interval key score also had a low negative correlation with HRQoL usual activities (Table 4).
Correlation of occupational identity, competence and settings and factors related to health-related quality of life.

Significant ⩽ 0.05.
Discussion
This study determined the occupational identity, occupational competence and occupational settings as well as HRQoL in people with SCI post-discharge from the rehabilitation hospital. The sample for this study was reduced due to the difficulty of tracing discharged persons with SCI with the available hospital details, as well as no Spinal Cord Registry being maintained in South Africa (Nizeyimana et al., 2025). The sample consisted of more males within the age bands of 30–40 years, which is similar to samples of people with SCI reported in other South African studies (Joseph et al., 2017).
Before their SCI, the majority of participants reported having had average/normal occupational functioning as they had lived ‘normal lives’ and encountered ‘normal’ everyday challenges like everyone else (Oliveira et al., 2021). This is consistent with both the local and international literature that indicates post-SCI, their occupational identity and occupational competence, as well as the occupational settings were disrupted (Cotton, 2012). Seminal work by occupational science and occupational therapy scholars concur and confirm that both occupational identity and occupational competence are determined by participation in meaningful occupations (Laliberte-Rudman, 2002).
All participants scored three for their occupational identity, related to functioning that was appropriate and satisfactory, before their SCI, compared to the current hardship they were experiencing, with half the participants reporting occupational disruption. This is consistent with other findings for people with SCI in South Africa, where Nizeyimana et al. (2025) found 52% of their participants reported they were satisfied with themselves and their present condition. For participants who reported disruption in occupational identity, this was related to uncertainty about their futures, as most of their life goals and plans were reported to be on hold because of the limitations in access to work, finances and ability to participate in leisure interests. This concurs with the findings of Martin-Saez and James (2021) that uncertainty about the future is at the core of the occupational identity disruption process. Löfvenmark et al. (2016) noted that in LMIC such as South Africa, loss of employment is of greater concern, thus losing their identity in relation to this occupation, weakening their roles and obligations as a provider.
The participants did appear to have come to terms with some aspects of the reality of their disability. Little occupational disruption was reported for expectations of success and appraisal of abilities and limitations. Thus, indicating ‘behavioural engagement’ (Aaby et al., 2021) in meaningful and valued activities associated with acceptance, as well as appropriate and satisfactory occupational functioning at home and within a limited family sphere (Fekete et al., 2021). The results, however, indicate significantly lower than reported occupational competence after the SCI for roles, maintained habits and satisfaction in life. The disruption of occupational competence in a greater number of spheres than in occupational identity may result from the sense of oneself as an occupational being preceding acceptance and the development of competence, or the ability to perform altered but still valued occupations (Hansson et al., 2022). People with SCI were found to need support to improve their performance capacities and daily routines (Alve and Bontje, 2019) to address challenges with organising time for responsibilities. Due to the need for extended times and the assistance required when performing occupations, Barclay et al. (2011) reported that there was limited time for engaging in satisfying interests and activities post SCI. In this study, the participants reported challenges affecting their competence due to the inability to engage in occupations, mostly in their community for leisure, at work, as well as working towards goals for the future (Löfvenmark et al., 2016). An international study by Ganesh and Mishra (2016) found that both employment and physical activity were predictors of a satisfying lifestyle.
Consistent with this, participants reported that inaccessible and or unmodified occupational settings were one of the biggest challenges that contributed to their occupational disruption, impacting their occupational identity and competence. Over 80% of participants had occupational setting client measure scores of below 50. Most of the reported environmental facilitators were at home, with most barriers in their community domain, as well as within the work environment (Löfvenmark et al., 2016). Most of the participants reported having an accessible immediate home occupational setting with acceptable and satisfying home life, social group, physical space, objects and resources. This may be due to the lack of formal help in LMICs with informal care from family, leading to increased family relationship satisfaction (Fekete et al., 2021). Hall et al. (2021) indicated that since inpatient rehabilitation is focused on the physical and social micro-environments of the person, with less attention paid to participation in and accessibility in the broader community and work, adaptation to the home environment may be made easier.
Outside of the home, environmental barriers in South Africa, as reported by Bezuidenhout et al. (2023) impact occupational settings, which all influence the personal participation of people with SCI, in everyday activities. This includes a lack of ability to socialise due to a lack of access to built environments and poor resources in terms of transportation. Lijodi et al. (2025) support the issues with lack of access to space and resources and report in LMIC, public transport such as minibus taxis, which, along with many public places, are inaccessible to wheelchairs. The participants reported they required assistance with mobility in the public physical environment, such as on the pavements, roads and malls. There was a need to adapt the environment for accessibility to re-create occupational competence, in particular (Mohorič and Tavčar, 2024).
A major environmental barrier was inadequate finances related to loss of employment and the productive role. The ability of participants to return to previous work was limited since physical and manual/labour is the source of income for many people. However, labourers who sustain a SCI are mostly excluded from manual and construction work, and they are unable to find alternate work. Some participants in the current study were not reemployed since employers indicated the work or workplace was inaccessible for a person in a wheelchair (Nizeyimana et al., 2024). Nizeyimana et al. (2025) reported that 60% of people with SCI injuries treated in the public health system in South Africa received vocational rehabilitation as inpatients, but there was no follow-up on return-to-work in the community or workplace after discharge. Although the 2016 White Paper on the Rights of Disabled Persons in South Africa (Republic of South Africa, 2016) promotes vocational rehabilitation and states that employers should take on the responsibility for providing reasonable workplace as well as infrastructure accommodations according to the concepts of barrier-free access and universal design. However, the articles are not enforceable, as it is a policy discussion document that precedes the development of an Act. The lack of disability-friendly transport also often prevented participants from being able to access the workplace when work or other productive roles, such as volunteering, were available. This is complicated by LMIC not having affordable, accessible transport systems for persons with disabilities (Luke, 2024).
Participants also reported having lost their leisure interests and could not explore new leisure opportunities, although they could socialise with friends. The lack of transport and finances, as well as leisure resources in the community, also hindered most participants from continuing with their previous leisure interests and\or exploring new interests promoting physical health and leisure activity (Alve and Bontje, 2019). This is consistent with an international study by Skovbjerg et al. (2025), which found that the cost, time constraints, lack of accessible facilities or equipment and suitable activities were obstacles to engaging in leisure activities for people with SCI. Participants in the current study reported having to travel 40 kms to play wheelchair basketball.
The HRQoL findings indicated challenges with pain/discomfort, usual activities and mobility, reflecting those reported in the literature, which indicates secondary health problems that limit engagement in activities, which all affect HRQoL (Sturm et al., 2021). However, the occupational disruption assessed on the OPHI II appears to reflect the lack of adaptation to the disability, which may have little association with HRQoL issues (Khanzada et al., 2024). The low correlation to occupational identity total interval key score for present functioning and EQ-5D-3L Mobility and Self-care scores suggests that adaptation or self-efficacy is lower in participants who had challenges with caring for themselves and moving around once they are discharged from the inpatient facility to their home situation. Independence in mobility and bowel continence has been associated with better adaptation and greater participation in activities (Bezuidenhout et al., 2023). A lack of participation in work may account for the low correlation between the occupational settings total interval key score and HRQoL usual activities in a LMIC, as suggested by (Bezuidenhout et al., 2023).
The current study indicated that occupational therapists need to be aware of the occupational disruption that occurs once people with SCI are discharged from rehabilitation facilities, irrespective of whether they achieve Landrum outcome Level 4 or Level 5 during inpatient rehabilitation. Services to facilitate occupational engagement after discharge for people with SCI closer to home through referral pathways to local community-based rehabilitation services and SCI support organisations, community outreach, home visits and telerehabilitation should be routinely provided. An advocacy role for accessible transport, as well as with employers to facilitate the re-employment of people with SCI, should also be considered. This provides an opportunity for further rehabilitation in the community environment, with return to work being prioritized.
Limitations of the study
Limitations of this study are the small sample size, the use of convenience sampling and sampling bias, as potential participants could not be recruited into the study due to a lack of recent contact details and only patients who retained active cell phone numbers provided in their medical records and to the rehabilitation departments could be recruited. The small sample size may have resulted in a type II error due to insufficient statistical power. The sample was also biased to male participants, with little representation of these concepts in females. The use of an interview administered face-to-face, online or by phone and a self-report questionnaire may have resulted in recall bias in participants remembering previous sense occupational identity, occupational competence and activity participation. The data were collected from participants treated at a single site, as well as the time frame of 4 months following discharge from the hospital, limiting the generalisability of these results.
Conclusion
From this study, a clearer understanding was attained of the complex process of renegotiating an occupational identity and occupational competence following a SCI and the extent to which the occupational settings can both facilitate and hinder this process. This study found that most of the participants had disrupted occupational identity and occupational competence at four months post-discharge from a rehabilitation hospital. Before their injury, participants considered their occupational identity and occupational competence to be established. While adapting to their disability after being discharged, more than half the participants obtained client measure scores below 50 for occupational identity and competence. The occupational setting scale indicated the greatest disruption, with over 80% participants obtaining client measure scores below 50.
The participants’ HQoL also indicated challenges with participation in mobility and usual activities, as well as secondary health issues, although there was little correlation between HRQoL and occupational identity, occupational competence and the occupational settings. Thus, occupational disruption, which highlighted the participants’ struggles to adapt and to reintegrate back into meaningful and productive roles and routines, does not necessarily reflect the HRQoL issues that were raised.
This study has highlighted that an important first step in living with an acquired disability in the community is to navigate the barriers in their occupational settings to re-establish the person’s occupational identity and occupational competence. This study reported the challenging life situation following a SCI rehabilitation, confirming that people with SCI require further intervention in adapting their occupational settings to support the development of occupational identity and competence following a SCI. This should include planning for life after SCI and vocational rehabilitation (Hall et al., 2021). Future research should focus on the effectiveness of vocational rehabilitation and interventions to provide accommodations in occupational settings, in the short and long term, after discharge from rehabilitation facilities, to determine the time needed for their occupational disruption to be resolved or not, and how their occupational needs may differ at that stage.
Key findings
Post-rehabilitation disruption in occupational identity, competence and settings for people with SCI requires intervention to support adaptation
In LMICs, the occupational settings create the greatest challenge
HRQoL does not correlate with occupational disruption which
What the study has added
Disruption in occupational identity, occupational competence and occupational settings post-rehabilitation for people with SCI requires continued community-based rehabilitation to achieve change in occupational settings, particularly for work and leisure.
Footnotes
Ethical considerations
Ethical clearance was received from the Human Research Ethics Committee at the University of the Witwatersrand Certificate number M231107.
Consent to participate
Verbal informed consent to participate was obtained from participants.
Author contributions
LHL and PdW were involved in the conceptualization of the study and LHL developed the protocol that gained ethical approval and completed patient recruitment. PdW supervised the study and DF completed the data analysis. LHL wrote the first draft of the manuscript which was reviewed and edited by PdW and DF. All authors approved the final version of the manuscript.
Funding
The authors declared no financial support for the research, authorship and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Patient and public involvement data
There was no patient and public involvement in the development of this research.