
Abstract
Introduction:
Sensory approaches are increasingly used in mental health settings to support emotional regulation and offer alternatives to restrictive interventions such as seclusion. Occupational therapists are well positioned to deliver these approaches due to their expertise in sensory processing and occupational engagement. However, little is known about their use within seclusion, a highly restrictive environment with risks of sensory and occupational deprivation. This study explored occupational therapists’ experiences of applying sensory approaches in seclusion settings.
Method:
Semi-structured virtual interviews were conducted with occupational therapists working in mental health services where seclusion was used. Data were analysed using thematic analysis.
Findings:
Six occupational therapists participated. Three themes were generated: navigating risk through creative and flexible practice; occupational therapists as leaders in sensory-informed practice; and ward cultures that can undermine occupational and sensory needs in seclusion. Participants described adapting interventions to balance safety with meaningful engagement, promoting sensory awareness within teams and challenging cultures that prioritised containment over therapeutic input.
Conclusion:
Occupational therapists play a central role in delivering sensory approaches in seclusion but face environmental, cultural and organisational barriers. Collaborative, whole-team involvement and improved access to training are essential to support safe, consistent, and person-centred sensory practice.
Introduction
Occupational therapists have historically led in advancing the theoretical understanding and application of sensory approaches (Scanlan and Novak, 2015; Wiglesworth and Farnworth, 2016), recognising the impact of sensory processing difficulties on occupational participation (Champagne, 2020). This article does not examine Ayres Sensory Integration®, which is a specific, standardised, neurodevelopmental intervention for children with sensory integration difficulties (Parham et al., 2021). Instead, it focuses on broader sensory approaches utilised in mental health settings, which draw on sensory processing theory but are distinct in their purpose, application and evidence base. The growing use of these approaches reflects their potential to support individuals experiencing distress or emotional dysregulation, regardless of the underlying cause. In particular, they are increasingly considered as part of efforts to reduce reliance on restrictive practices such as seclusion and restraint (Barbic et al., 2019; Fredericks et al., 2025; Scanlan and Novak, 2015), as well as to promote emotional regulation and stress management (Fitzgibbon and O’Sullivan, 2018). Sensory approaches offer practical, person-centred strategies that can help individuals recognise and respond to their needs, supporting engagement in meaningful activity and participation in everyday life.
The sensory system is a component of the central nervous system that manages the collection and processing of information received through the eight senses (sight, touch, sound, taste, smell, vestibular, proprioception and interoception) from sensations inside and outside of the body (Fitzgibbon and O’Sullivan, 2018). The nervous system is interconnected to both emotional regulation and social behaviours and therefore, sensory approaches provide sensory input to this system to activate or deactivate the sympathetic (fight or flight) or parasympathetic (rest and digest) nervous systems (Fitzgibbon and O’Sullivan, 2018). Through this input, an individual’s neural activation is optimised which improves emotional wellbeing and overall functioning (Fitzgibbon and O’Sullivan, 2018; Sutton and Nicholson, 2011). It is essential for clinicians to understand the different senses and how different strategies can facilitate a change in emotional state through sympathetic/parasympathetic activation depending on what physiological change is required (e.g. alerting or calming; Fitzgibbon and O’Sullivan, 2018).
Popular sensory interventions within adult mental health inpatient settings include the use of sensory rooms, deep pressure strategies and sensory grab bags. Sensory rooms are dedicated spaces that contain items useful in providing sensory input to the various senses; for example, lava lamps (sight), aromatherapy oils (smell); rocking chairs (vestibular); stress-balls (touch); food items like herbal teas (taste) and calming sounds/music (hearing; Andersen et al., 2017; Fitzgibbon and O’Sullivan, 2018; Scanlan and Novak, 2015). International research across occupational therapy, nursing and psychology has increasingly examined the effectiveness of sensory rooms in adult inpatient mental health settings. Findings suggest that their use is associated with reductions in self-reported distress, anxiety and agitation, and with improved emotional regulation and perceived safety among service users (Andersen et al., 2017; Chalmers et al., 2012; Champagne and Stromberg, 2004). Deep pressure strategies describe the use of weighted items (blankets/vests) to provide proprioceptive input believed to have a calming and organising effect on the nervous system (Fitzgibbon and O’Sullivan, 2018; Wiglesworth and Farnworth, 2016). Sensory grab bags are transportable resources that are individualised and used for self-soothing in areas where sensory rooms may not be available (Andersen et al., 2017; Fitzgibbon and O’Sullivan, 2018; Scanlan and Novak, 2015). Studies highlight their value in promoting autonomy, choice and personalised coping strategies, aligning with recovery-oriented and trauma-informed care principles widely adopted across international mental health services (Andersen et al., 2017; Sutton et al., 2013). Emerging evidence within inpatient mental health settings indicates that these interventions may support reductions in arousal and assist with emotional regulation during periods of distress, though robust experimental evidence remains limited (Champagne, 2018; Novosel et al., 2019).
International and UK literature and national reports highlight the need for individualised sensory approaches in mental health settings to reduce distress and the use of coercive treatment methods (Care Quality Commission, 2020; Department for Education and Department of Health and Social Care, 2019; World Health Organization, 2019). This emphasis aligns with international evidence demonstrating that restrictive interventions should be avoided wherever possible and, when unavoidable, implemented using the least restrictive alternative, with attention to how service users experience and perceive restrictiveness (Lindekilde et al., 2024). Some studies report reductions in the use of restrictive practices, such as restraint and seclusion, following the introduction of sensory-based interventions, although the strength of evidence remains variable and context dependent (Lloyd et al., 2014; Wiglesworth and Farnworth, 2016).
Seclusion is the ‘supervised confinement and isolation of a patient, away from other patients, in an area from which the patient is prevented from leaving’ (Department of Health, 2015: 300). It is utilised as a last resort intervention in mental health settings to manage challenging or aggressive behaviours that pose a risk to self or others (National Institute for Health and Care Excellence, 2015). However, a paucity of evidence exists around the effectiveness of this controversial intervention in reducing these behaviours, with some studies suggesting that patients are more likely to experience negative physical and psychological effects following the use of seclusion (Brophy et al., 2016).
In addition to ethical and clinical considerations, there is growing recognition of the substantial economic burden associated with restrictive interventions such as seclusion and restraint. These practices require increased staffing, may prolong inpatient stays, and are associated with staff injury, legal risk, and wider organisational costs, making them highly resource-intensive components of mental health care (Chan et al., 2012; Luigi et al., 2026). However, a recent systematic review by Luigi et al. (2026), examining the economic evidence for interventions aimed at reducing aggression and restrictive practices in inpatient mental health settings, highlighted that relatively few studies report cost data. The review further emphasised the need for robust cost-effectiveness analyses and evidence of long-term clinical outcomes to better inform decision-making in this area.
While there is evidence highlighting the impact of sensory intervention in the reduction of distress and behavioural disturbance, (Adams-Leask et al., 2018; Novak et al., 2012; Sutton et al., 2013), there is very limited data that document occupational therapy interventions for patients experiencing sensory and occupational deprivation in seclusion (Jeffries, 2021). Occupational therapy is concerned with the negative impact of occupational injustice on health and wellbeing, (Whiteford et al., 2019) and therefore the profession plays a central role in generating opportunities for meaningful occupational engagement, particularly for patients in seclusion (Jeffries, 2021). The role of occupational therapy for patients in seclusion has been identified as an area requiring further research (Bowser et al., 2024; Link et al., 2024).
It is imperative that sensory interventions are carefully considered by occupational therapists in mental health settings, as extreme amounts of sensory stimulation could potentially trigger a negative reaction in persons already experiencing psychological distress and perceptual changes (Andersen et al., 2017; Brown et al., 2020; Sutton and Nicholson, 2011). Therefore, to effectively deliver sensory interventions, the healthcare professional must have an awareness of the concept of sensory overload (Scheydt et al., 2017) and be sensitive to everyone’s preferences and personal needs (Andersen et al., 2017; World Health Organization, 2019). Occupational therapists hold a significant role in spearheading sensory approaches in these settings and therefore this study aims to explore the experiences and role of occupational therapists working in this area, the different ways occupational therapy sensory interventions are delivered and highlight key barriers and facilitators in this setting. Hence, the question, what are the experiences of occupational therapists in using sensory approaches with patients in seclusion settings?
Methods
Study design
A qualitative study using semi-structured interviews and reflexive thematic analysis was used to explore the complex experiences of occupational therapists who work in seclusion settings. A reflexive stance was maintained throughout the research by using a reflexivity diary, peer debriefing, and regular supervision to consider the influence of the researcher’s social identity and ensure research quality.
This study was part of a wider project exploring the experiences of occupational therapists delivering interventions in seclusion while working as a member of the multidisciplinary team (MDT; Bowser et al., 2024).
Sampling and participants
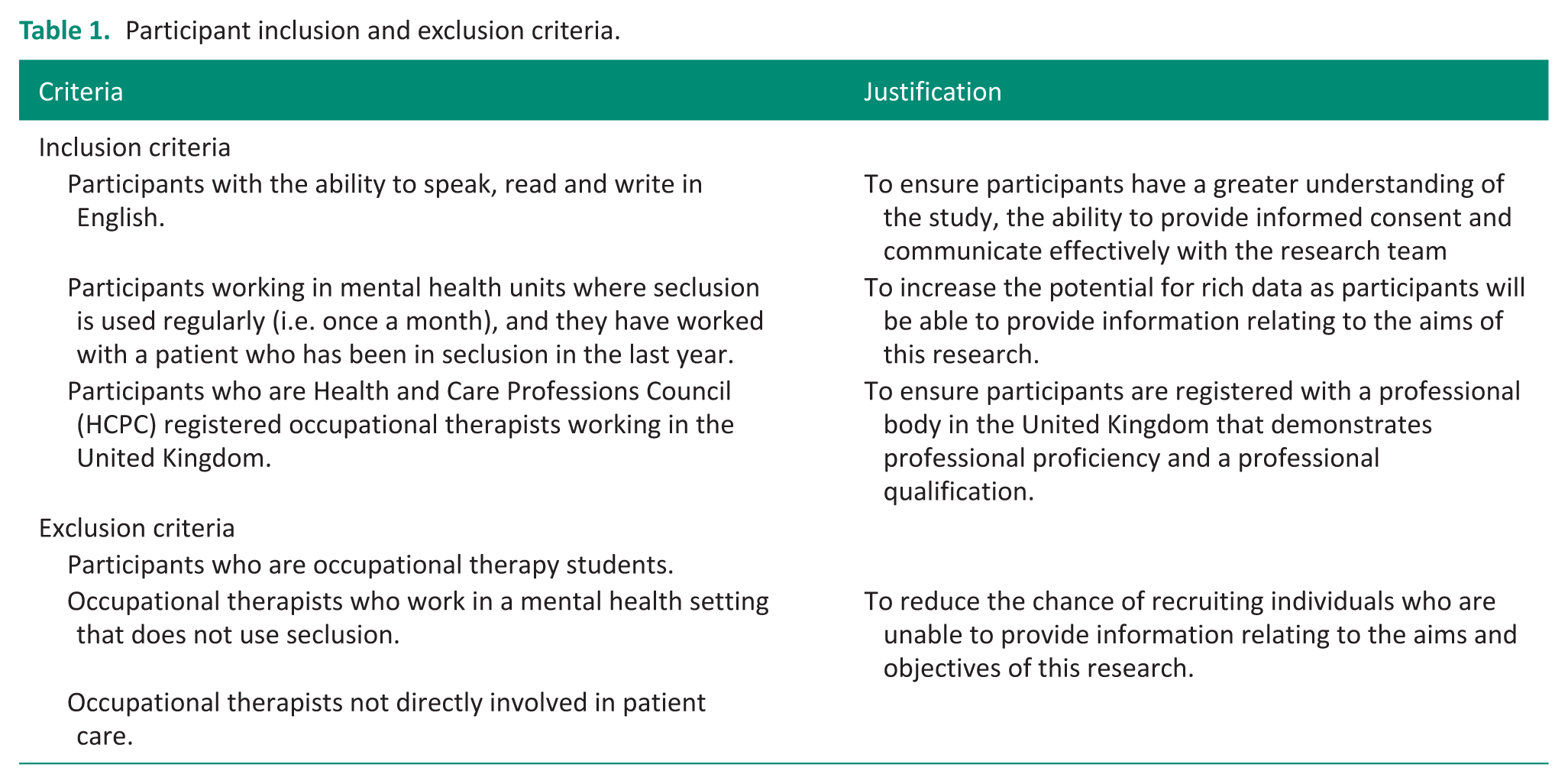
Ethics was approved by the University Ethics and Research Governance Online (ERGO2) System (70887.A4). Convenience sampling was used for recruitment. The study poster was advertised on specialist occupational therapy groups on social media. Snowball sampling was then used to generate recruitment of this hard-to-reach specialist population. The participant inclusion and exclusion criteria (Table 1) guided the recruitment.
Participant inclusion and exclusion criteria.
Recruitment
Interested individuals emailed the study address and were sent a Participant Information Sheet and consent form. After providing written informed consent, participants were contacted to arrange data collection. No incentives were offered. Participants were informed they could withdraw at any time, though data could not be removed once anonymised. Confidentiality was upheld by restricting data access to the research team and storing all data securely.
Data collection
Virtual interviews (40–90 minutes) were conducted and recorded via Microsoft Teams. A semi-structured schedule with open-ended questions guided the process. Participants were asked again for consent before beginning the interview (Braun and Clarke, 2022). A practice interview with supervisors tested the interview guide’s suitability, expected duration and the researchers’ interviewing skills.
Data analysis
Interviews were transcribed verbatim from the video recordings. Data were analysed inductively using reflexive thematic analysis to identify and interpret patterns in the dataset (Braun and Clarke, 2022), an approach well suited to complex, exploratory topics. A researcher not involved in the interview process completed the transcriptions to ensure all team members engaged fully with the data. Rather than conducting independent dataset checks, the team used supervision and collaborative discussions to deepen analysis, consistent with Braun and Clarke’s (2022) rejection of inter-coder reliability in reflexive thematic analysis.
Transcripts were read repeatedly to build familiarity, with initial ideas noted during early readings. Codes relevant to the research question were generated on the third reading across the full dataset. Codes were then reviewed collectively to identify emerging themes, which were refined in relation to the research question to move from surface-level patterns to more fully developed, interpretative themes (Braun and Clarke, 2022). Final themes were defined and named to articulate the narrative of the analysis.
Results
A total of nine individuals expressed an interest in the study; however, due to not meeting the inclusion criteria or non-completion of consent form despite follow-up, a total of six participants were interviewed. A smaller sample size like this is typical for qualitative research (Braun and Clarke, 2022). There was an equal representation of male (3) and female (3) occupational therapists, and they worked in both Child and Adolescent Mental Health Services (CAMHS) and Adult Services (see Table 2).
Participants demographics.

CAMHS: Child and Adolescent Mental Health Services.
Had recently changed roles.
To contextualise the findings, it is important to note differences in how participants defined seclusion and high-care settings. Some saw no distinction, while others viewed high-care as less restrictive but still limited in furnishings and access to risk items, functioning as a low stimulus space for de-escalation. Some participants reported that their high-care area included a seclusion room, with interventions delivered through the hatch or, when appropriate, in the wider high-care space. One participant described feeding under restraint occurring in high-care but still legally classed as seclusion because the young person was locked in and unable to leave. In this study, the terminology used by each participant is retained, but analysis focuses on data relevant to the research question using the Department of Health (2015) definition of seclusion.
Not all participants had access to traditional sensory resources. As outlined in Theme 1, risk levels often prevented their use. Participants drew instead on their knowledge of sensory processing and emotional arousal to make appropriate, creative substitutions. The literature similarly makes no distinction between everyday items and specialist sensory resources for achieving affect regulation (Fitzgibbon and O’Sullivan, 2018).
Three themes were generated to describe occupational therapists’ experiences of using sensory approaches with patients in seclusion settings and are presented below:
Theme 1: Navigating risk through creative, flexible occupational therapy practice
All participants spoke about risk being the barrier to interventions in this environment. It was inferred that seclusion paved the way for the wider team to become anxious and more risk-averse leading to additional challenges when planning interventions in this setting. Most participants in this study said they did not enter seclusion while a person was in there but used the hatch to deliver interventions: I haven’t ever entered the seclusion . . . it’s always been through the hatch or . . . the window. (Zara)
Participants acknowledged this was not an ideal approach, but it was a starting point to developing rapport and delivering therapeutic interventions: he [was] still quite disinhibited at that point. . . so a lot of their [the OT] work was just about kind of going to the hatch for sort of 5-10 minutes, saying hello, orientating him to time, place, person. So, they became sort of that familiar face. (Alice)
Participants spoke of the need for therapeutic input to continue by adapting sessions to meet the environment’s risks. The consideration of tools/equipment used during interventions was particularly important due to the potential risk that the item could be used as a weapon or something to self-harm with. Some participants felt that even if the item was beneficial to the person, the MDTs’ view of risk led them to compromise and find alternative items: I find myself. . ., as a matter of care, . . .explaining my thought process as to [the equipment chosen for the session]. . . people have different opinions on that and sometimes you do have to compromise. (Matt)
However, Michael felt that by framing something as a sensory approach, the MDT felt it was ‘worth the risk’ as it could be beneficial for the person.
All participants viewed risk as an opportunity to make innovative adaptations to sessions that would still consider the potential risk(s). All participants felt that occupational therapists led as positive risk-takers on the team: we’re more of the risk taker. . . the positive risk takers. (Stephen)
Participants spoke both explicitly and implicitly about their core occupational therapy skills in activity analysis to grade and adapt their interventions accordingly. All participants emphasised the need to individualise and be flexible with their sessions, rather than a prescriptive ‘one size fits all’ approach: . . . our profession is underpinned by creative thinking. . . . we’re effective problem solvers, aren’t we? . . .But again, you know, we use activity as a therapeutic tool. And so, it’s about kind of thinking about how we can grade activities from a security perspective, but also how can we keep it enjoyable and meaningful for the patients. (Alice)
Most participants mentioned that traditional sensory approaches/resources required additional considerations for use in seclusion due to ‘increased risk with [these] items’ (Michael). However, all participants were able to provide examples of how they were able to adapt and find alternatives to their sensory approaches to still meet that individual’s sensory needs while also being mindful of risk: . . . things like making a hand scrub that’s edible so that they get the sensory smells of it. . . but it’s like sugar and bananas, so they can eat it and it’s not going to cause any damage. (Zara)
Participants provided examples that demonstrated their creativity in planning sensory interventions that met the individual’s unique needs, sometimes with items outside the realm of traditional sensory resources. In these instances, the balance between security and therapy had been considered and reflected in the choice of tools used to deliver sensory input: I’ve done sensory sessions in high care where I’ve got cotton pads [with] like essential oils and kind of going right, which ones do you like? (Matt)
Sophie discussed how she was able to provide sensory input by using everyday objects and activities in innovative ways despite a lack of ‘traditional’ resources: I used to think. . . it’s all about sensory rooms and sensory items and then. . . . someone told me once, and I completely agree, that there are sensory elements in everything. . .So for example, if we’re doing our stretching and kind of more sports stuff and that’s going to give us that heavy work feedback and. . . proprioceptive feedback. . . (Sophie)
Theme 2: Occupational therapists as leaders in sensory-informed practice
Participants described that sensory approaches and knowledge were mostly spearheaded by the occupational therapy department. Participants recognised the positive shift in recent years of offering occupational therapy staff sensory training and creating advanced clinical practitioner roles within the department to provide specialist support in this area.
Stephen spoke about sensory awareness becoming part of the ward culture for the wider MDT to address their own needs: to try and. . .help the stress levels of the nurses, they’ve asked for their own little sensory grab bags. . .(Stephen)
Sometimes other professions provided inappropriate sensory items to patients and with a ‘one-size fits all’ approach that did not consider the individual’s sensory preferences or needs: giving them a fidget toy. . .that’s seen as . . . the easy option. . .for some of the professionals that we work with. . . you often see that some of the things . . .are given out are kind of inappropriately (Michael)
Michael also discussed the importance of balancing patient’s wishes with the clinician’s clinical reasoning. He spoke of an incident that occurred whereby a patient had requested a weighted blanket, citing it had worked for them in the past; however, this intervention was not clinically indicated as appropriate for this individual by the sensory practitioner who was concerned that it could be a potential method for self-harm: and it did transpire that this was a, a method of eliciting behaviour where he could self-harm. He wanted to .. smother himself with the . . . weighted blanket. (Michael)
Sensory approaches were inferred to be suitable for everyone it an assessment of the person’s preferences and sensory processing needs informed interventions: I think if it doesn’t work, you’re not using the right approach. I think it will work for everyone. You just need to find out what their sensory needs are. (Matt)
However, some participants highlighted two other patient populations that sensory interventions may not be suitable for: individuals with a diagnosis of autistic spectrum condition (ASC) and individuals with a trauma history. These groups required further consideration to avoid inadvertently causing further harm by providing inappropriate interventions: . . . in general, it’s an all-rounder. We do get a lot more [ASC] young people so obviously you do have to be a little bit aware of – cause some people can have quite strong reactions to something they don’t like . . .or the other risk of having lots of things around it can be over-stimulating especially for someone with [ASC]. . . (Stephen) one of the patients I worked with . . . he had a horrific history of . . . abuse . . .and he associated the smell of. . . burning toast with his historical trauma. . . I suppose just from a trauma perspective you had to be mindful of how you delivered the session . . . because you didn’t wanna . . . retraumatize him inadvertently. (Alice)
All participants experienced the positive impacts of sensory interventions on patients’ emotional regulation and felt approaches could be used in de-escalating situations to prevent/reduce seclusion and restraint. Occupational therapists sensory-aware approach on the ward allowed them to lead reflection within the team on whether ‘challenging/aggressive behaviours’ were potentially unmet sensory-seeking behaviours or a presentation of over-arousal on the ward: . . .a lot of the patients who have challenging behaviours, it is more to do with. . . their sensory needs and them not being met then them. . .just being challenging . . . It is more around sort of your sensory seeking behaviours or being over aroused and things like that. (Alice)
However, Alice highlighted the danger of being pigeonholed by the MDT as wholly sensory practitioners: we’ve got to be mindful of kind of role blurring because first and foremost, we are occupational therapists. . . (Alice)
Theme 3: Ward culture undermining occupational and sensory needs in seclusion
All participants experienced a ward culture that did not always recognise the importance of continued occupational engagement in seclusion environments. For example, Stephen highlighted this stance ultimately conflicted with the professional paradigm and occupational theories of occupation being integral for health: Because there. . .used to be the kind of rationale . . . that if someone’s in high-care,. . . you weren’t to engage with them anyway, they should just be kind of left. Which obviously goes against OT principles. (Stephen)
There were mixed views from participants about the MDTs’ understanding of sensory needs, especially in the sensory-deprived restrictive environments of seclusion: a patient [would] often put his hand out of the hatch and try and grab people or grab things. . . but I felt that was more of a sensory thing . . .the consultant saw. . . it as a risk . . .but I think that the sensory aspect of it was never considered and there was a lot of [sensory-seeking] behaviour. (Zara)
The wider team often believed patients were in these environments ‘for a reason’ and required minimal input/stimulation while there. Participants felt this view was particularly harmful, given occupational therapy’s core understanding of the impact of the environment on a person’s health. Restrictive, low stimulus environments like seclusion presented major risks of sensory deprivation and had the potential to inflict further harm: . . .assumption is that someone’s done something that they require seclusion. They must need a low stimulus environment when actually what we are kind of seeing is that that that’s actually quite detrimental and it makes them worse so, what the hell are we doing. . . Isn’t it funny that this is how we think we’re helping people by shutting them away in a room? . . . it’s not good if you leave someone without that stimulation. (Matt)
Occupational therapy sessions were viewed by participants as important as other treatment modalities (e.g. medications) in fostering recovery. Many participants felt it was part of their role to promote the value of occupational therapy, particularly in challenging the ward’s attitude of leaving an acutely unwell person(s) in ‘solitary confinement’ (Matt) to consider and atone for their actions with minimal stimulation. Some participants spoke of the need for wider organisational changes like environmental modifications and development of policies to mandate occupational therapy input in seclusion to prevent further harm from sensory deprivation.
Discussion
This article explores occupational therapists’ experiences of using sensory approaches with patients in seclusion settings in the United Kingdom. Although research in this specific area remains limited, the findings of this study broadly support the emerging evidence base.
Participants embraced their role as ‘positive risk-takers’ within the MDT, advocating for meaningful occupational participation even within restrictive environments. This echoes Royal College of Occupational Therapists (2018) guidance, which encourages occupational therapists to support autonomy through balanced and considered risk-taking. The findings suggest that services may need to review their policies to ensure that positive risk-taking is supported rather than constrained by overly risk-averse cultures. Participants’ examples of creatively adapting interventions also highlight the relevance of core occupational therapy skills such as activity analysis, grading and environmental adaptation in maintaining therapeutic engagement in seclusion. This aligns with Link et al. (2024), who described similar adaptive practices driven by least restrictive principles.
Participants also reported that they were frequently regarded as the ‘sensory experts’ within the MDT. This perception is consistent with occupational therapists’ expertise in sensory processing theory and its functional implications (Craswell et al., 2020; Fitzgibbon and O’Sullivan, 2018; Wiglesworth and Farnworth, 2016). However, the study highlights variability in access to specialist sensory training across services. Limited training opportunities may contribute to inconsistent practice, supporting the argument for dedicated investment in specialist sensory education and the development of a core competency framework for sensory approaches in seclusion.
All participants described clear therapeutic benefits of sensory interventions, particularly in supporting emotional regulation, reducing distress and contributing to the prevention or de-escalation of crisis situations. These findings are consistent with evidence that sensory modulation can reduce anxiety, aggressive behaviour and the need for restrictive practices (Barbic et al., 2019; Dawson et al., 2025; Dike et al., 2021; Fredericks et al., 2025; Novak et al., 2012). Given these benefits, services should consider integrating sensory modulation as a first-line de-escalation tool and ensuring the availability of safe, appropriate sensory resources including sensory rooms, sensory kits and everyday items that can be used creatively within risk parameters. Establishing pathways for early sensory assessment, especially for individuals likely to experience dysregulation, may also support least restrictive care.
Although participants noted an increasing awareness of sensory needs within the MDT, they also identified ongoing gaps in colleagues’ understanding of how to implement sensory approaches safely and effectively. This aligns with Scheydt et al. (2017), who reported that staff often struggle to recognise sensory needs or the risk of sensory overload. Sensory training for the MDT, embedded sensory strategies in routine assessment processes, and shared care plans incorporating personalised sensory regulation techniques may help address this gap.
Participants also described a need to advocate for occupational engagement and challenge ward cultures that prioritised containment over therapeutic input during seclusion. This reflects the profession’s wider responsibility to address occupational deprivation and occupational injustice (Whiteford et al., 2019). Occupational therapists may therefore need to take an active role in educating colleagues about the role of occupation in emotional regulation and recovery, and the risks associated with sensory- and occupation-deprived environments.
At the same time, several participants expressed concern about being perceived solely as ‘sensory practitioners’. They emphasised that sensory work must be situated within the broader occupational therapy process, supporting occupational performance, participation and recovery (Machingura et al., 2022; Wallis et al., 2018). Maintaining clarity of professional identity requires therapists to articulate how sensory needs relate to occupational goals, and to ensure their practice remains occupation-centred even when delivering sensory strategies.
Finally, participants recognised that occupational therapists cannot lead sensory approaches in seclusion in isolation. Effective implementation requires shared ownership within the MDT, alongside co-developed protocols, collaborative risk assessments and joint decision-making around intervention options (Wright et al., 2020). Leadership support is also essential for embedding sensory approaches into everyday practice and ensuring sustainability, consistency and alignment with evidence-based and least restrictive care.
This study highlights several important areas for future research. First, there is a clear need to explore the perspectives of service users who experience sensory approaches while in seclusion. Understanding how individuals perceive the impact of sensory interventions on emotional regulation, distress, safety and dignity would provide a crucial complement to practitioner-focused evidence and strengthen the person-centred evidence base.
Further research is also required to evaluate the effectiveness of sensory approaches in seclusion more systematically. Quantitative and mixed-methods studies examining outcomes such as duration and frequency of seclusion, rates of escalation, and use of additional restrictive practices would support clearer conclusions regarding their role as first-line de-escalation strategies.
Given the variability in access to specialist sensory training identified in this study, future research should investigate how different models of sensory education and competency development influence confidence, consistency and risk-taking across services. The development and evaluation of a core sensory competency framework may help to standardise practice and improve safety and effectiveness.
The findings also suggest the importance of examining MDT understanding and ownership of sensory approaches. Research exploring how MDT members conceptualise sensory needs, and how shared training and collaborative protocols influence ward culture and decision-making, would inform more integrated and sustainable implementation.
Finally, further investigation into organisational and cultural factors is needed, particularly how policies, leadership and risk management frameworks enable or constrain occupation-centred and least restrictive practice in seclusion. Research in this area would support occupational therapists’ advocacy efforts and contribute to addressing occupational and sensory deprivation within highly restrictive environments
Limitations
Recruitment of this population proved challenging, likely reflecting clinicians’ limited time and a perception that participation would offer minimal benefit, as reported elsewhere in the literature (Meyer et al., 2022). As this study was conducted as an MSc research project within a restricted timeframe, only University Ethics approvals, not UK National Health Service (NHS) ethics approval, were sought, which meant that participants were not recruited directly from the NHS. This resulted in recruiting participants through social media advertising and word of mouth. These strategies may also have inadvertently excluded potential participants who were highly relevant to the research questions. Furthermore, the small sample size and limited geographical spread across the United Kingdom restrict the breadth of perspectives captured. As such, the findings may not fully represent the diversity of experiences across different clinical settings and regions (Beach et al., 2017).
This article formed one of three contrasting strands within a collaborative group research project, requiring careful coordination to ensure consistency in data collection across researchers. Although the three areas of focus were closely aligned, each researcher brought distinct professional backgrounds and research interests to the project (Mulvihill and Swaminathan, 2022). Consequently, individual researchers may have prioritised their own phenomenon of interest during data collection. To mitigate this risk, researchers engaged in ongoing reflexive practice and participated in regular supervision, which supported the critical examination of assumptions, decision-making and data collection processes. Despite these measures, there remains the potential that attention to one area of focus may have diluted the depth of data obtained across the other strands, resulting in the loss of some potentially important insights.
Conclusion
This study provides important insights into the experiences of occupational therapists using sensory approaches with patients in seclusion settings, highlighting both the potential and the complexity of delivering therapeutic input in highly restrictive environments. The findings emphasise that occupational therapists play a central role in recognising and responding to the sensory and occupational needs of individuals in seclusion, often acting as ‘positive risk-takers’ who creatively adapt interventions to ensure safety while enabling meaningful engagement. Participants demonstrated that sensory approaches can support emotional regulation, aid de-escalation and help reduce reliance on restrictive practices, reinforcing their therapeutic value within mental health care.
However, this study also reveals considerable challenges. Ward cultures that prioritise containment over engagement, limited access to specialist sensory training and inconsistent understanding of sensory needs across MDT all influence the quality and availability of sensory interventions. These barriers not only inhibit the effective use of sensory strategies but can also contribute to occupational and sensory deprivation, with potentially detrimental consequences for patient wellbeing. The findings underscore the importance of embedding sensory awareness and occupation-focused practice across the whole MDT, ensuring that sensory needs are recognised as integral to emotional regulation, safety and recovery.
Occupational therapists in this study negotiated tensions between their professional identity and being perceived solely as sensory practitioners. Their accounts highlight the need to maintain clarity about the place of sensory work within the broader occupational therapy process and to promote the value of occupation within seclusion, where meaningful engagement is often overlooked. The findings therefore support continuing advocacy, education and organisational change to ensure that sensory approaches are used safely, ethically and effectively, and that occupational therapists’ expertise is fully understood and utilised.
Overall, this study contributes to the emerging evidence base by illustrating how occupational therapists adapt, innovate and lead in the application of sensory approaches within seclusion settings. It reinforces the need for consistent training, supportive organisational cultures and collaborative MDT practices to sustain least restrictive, person-centred care. Further research exploring the experiences of service users themselves would provide a crucial next step in understanding the impact and effectiveness of sensory approaches in seclusion and informing future developments in practice.
Key findings
Occupational therapists used creative, flexible strategies to deliver sensory interventions safely within seclusion.
Ward cultures often limited occupational and sensory engagement, requiring therapists to advocate for least restrictive practice.
Effective sensory approaches depended on multidisciplinary collaboration and consistent access to specialist training.
What the study has added
This study provides evidence that occupational therapists play a central, creative and advocacy-driven role in delivering safe, least restrictive sensory approaches in seclusion, highlighting training needs and organisational factors essential for effective practice.
Footnotes
Acknowledgements
Thank you to all the occupational therapists who participated in the interviews.
For the purpose of open access, the author has applied a Creative Commons attribution license (CC BY) to any Author Accepted Manuscript version arising from this submission.
Ethical considerations
As the study does not involve patients in the NHS, ethical approval was sought from the university of Southampton ethics committee via the ERGO2 online process (approval number 70887). Approved 2023.
Consent statement
All participants gave written consent for their anonymised information to be shared.
Author contributions
AB, LM, and MDH researched literature, conceived the study, and developed a protocol. BH and RW gathered data. All authors conducted data analysis and wrote and edited the manuscript, approving the final version for submission.
Funding
The authors declared no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Patient and public involvement data
During the development, progress and reporting of the submitted research, Patient and Public Involvement in the research was not included at any stage of the research.