
Abstract
This study explores reflective functioning (RF) in foster carers using the Parent Development Interview. A mixed-methods design was employed in eliciting personal accounts of fostering by carers alongside an assessment of their RF. Results suggest that the carers displayed varying levels of RF and specifically that the elements of reflection that may be most salient for effective fostering – developmental, systemic and attachment-based thinking – were uncommon among the sample. Given the importance of foster carers’ potential to redirect the lives of children and enhance healthy attachment strategies, therapeutic and training packages that might increase RF are considered.
Introduction
Studies of looked after children have shown how it is possible to reshape their attachment strategies from insecure to more secure levels. Using the Child Attachment Interview (Target, Fonagy and Shmueli-Goetz, 2003), Briskman and colleagues (2010) found that 40% of the children who were assessed as insecurely attached to their birth mothers went on to form secure attachments to them. Research has demonstrated that success in trying to revise insecure attachment strategies varies. A cluster of important findings have suggested that only carers who were securely attached in relation to their own parents positively evolved the attachment strategies of the children in their care (Caltabiano and Thorpe, 2007; Dozier, et al., 2001; Kaniuk, Steele and Hodges, 2004; Pace and Zavattini, 2010; Stovall and Dozier, 2000). Dozier and colleagues (2001) also highlighted that children in care have an increased risk of developing disorganised attachments when their caregivers have insecure attachment strategies or dismissing and anxious states of mind. It seems that when child insecurity is met with carer insecurity, combined with any pre-existing vulnerability resulting from the child’s prior experiences, there is an increased risk of disorganised attachment. While the degree to which caregivers are able to regulate and organise their feelings about their relationships with their own parents is important in determining a child’s attachment security (Fonagy, et al., 1991; Main and Goldwyn, 1998; Main and Solomon, 1990), it is acknowledged that many other personal, relational and contextual factors can play a varying role in the formation and transmission of attachment styles. These include maternal mental health, child temperament, socio-economic status and social support (Fonagy and Target, 2005).
Extensive research has investigated the mechanisms by which attachment strategies are transmitted from caregiver to child (van IJzendoorn, 1995). It is increasingly appreciated that a parent’s capacity to reflect upon the child’s internal experience is crucial to passing on a secure attachment. Known as reflective functioning (RF), this capacity is said to involve both a self-reflective and an interpersonal component in which the parent must grasp the complex interplay between their own feelings (mental states) and their child’s inner experience. A parent’s capacity to hold in mind a representation of their child as having feelings is thought to allow the child to notice and explore their own internal experience via their parent’s representation of it (Fonagy, et al., 2002; Gergely and Watson, 1996).
Slade and colleagues (2003) developed and validated a measure of RF, the Parent Development Interview (PDI), and used it in a study of birth parents (Slade, et al., 2005). This study found that those with a high RF were more likely to be securely attached to their own parents and have children who displayed secure attachment strategies. Likewise, birth parents displaying low RF were likely to be classified as insecurely attached to their own parents, also reflected in the insecure attachment strategies revealed by their children in foster care. Kaniuk, Steele and Hodges (2004) identified similar patterns relating to capacity for RF and attachment transmission in a sample of adoptive mothers. Maternal behaviour appeared to play a mediating role through which RF was translated within the relationship. Grienenberger, Kelly and Slade (2005) found that mothers with high RF scores were unlikely to exhibit significant disruptions in affective communication. It is thought that an understanding of their child’s distress must be demonstrated by behaviourally communicating this in ways that are congruent with the child’s internal experience (Fonagy, et al., 1998).
Currently little is known about the RF capacities of foster carers. Some may have developed high capacities in this respect while others may struggle owing to their own early experiences. It is conceivable that without the capacity to find emotional meaning in children’s behaviour, foster carers will be unable to offer a flexible repertoire of responses, provide for the child’s psychological development or even maintain the foster placement. Given the relatively high number of foster placements that break down, work in this area is urgently needed. With increased understanding of the role of attachment in foster care, support packages and targeted training can assist carers in their challenging role.
Aims
The aims of our study were: (1) to assess the levels of RF capacity in a sample of foster carers providing long-term therapeutic care, to explore differences in their ability to reflect on their own mental states (RF relating to self and RF related to the child) and to chart the types of RF they employ; and (2) to explore carers’ accounts of fostering, encapsulating themes relating to their understanding of the child and their relationship.
Method
A mixed-methods design was chosen using the PDI. As will be explained, this was chosen because it directly assesses RF within a current parent–child relationship.
Interviews were undertaken with 12 foster carers. The analysis of the PDI consisted of two parts: quantitative assessments that measured the carer’s capacity for RF and its use and nature (a unique feature of this study was to assess separately RF related to self and RF related to the child); and a qualitative thematic analysis of the foster carers' responses in the PDI.
Sample
Foster carers were recruited from the South West (UK) region covered by a private sector fostering company offering long-term ‘therapeutic care’ for ‘hard-to-place’ children, who were unable to secure or maintain placements with local authority carers. Training and continuing support for the carers was provided by therapeutically trained staff employed by the agency. This included an overview of attachment theory and internal working models, but with no specific focus on mentalisation and RF. As with many such training programmes, the focus was on the child’s attachment disturbances with less emphasis on the carer’s attachment history and self-awareness. Attendance at sessions was voluntary and in some cases participation was triggered by problems or potential placement breakdown. The agency was concerned about improving this process and fully supported the research.
Letters of invitation were sent out to carers who were currently offering a long-term placement to a young person who had been in care for at least six months. Twelve carers volunteered for the study, a 90% acceptance rate, and all participated in the research (10 females and 2 males). They had been fostering for between six months and 15 years. All had English as their first language and had children of their own, some of whom had left home. There was a mixture of single carers and those in a relationship. The looked after children were aged between three and 16 years (4 females and 8 males). They had been in their current placement for between six months and seven years.
Carers were seen once in their homes and the interviews were audio-recorded. Following the PDI interview, a letter summarising the main themes and recommendations emerging from the data was sent out to all participants to check that the information was accurate and the clinical recommendations relevant.
Measures
The Parent Development Interview
The PDI is structured to assess a caregiver’s representations of the child, their self as a carer and their relationship with the child. It explores the carer’s ability to consider both their own and the child’s emotional experience and feelings. Other questions focus on their relationship with the child, including what makes it pleasurable or difficult. Carers are also asked to describe themselves as carers and express their feelings on matters such as neediness, guilt, anger and joy. Finally, they are asked about how their own childhood family experiences have affected their parenting.
Each coded question on the PDI is assessed for RF under four broad categories:
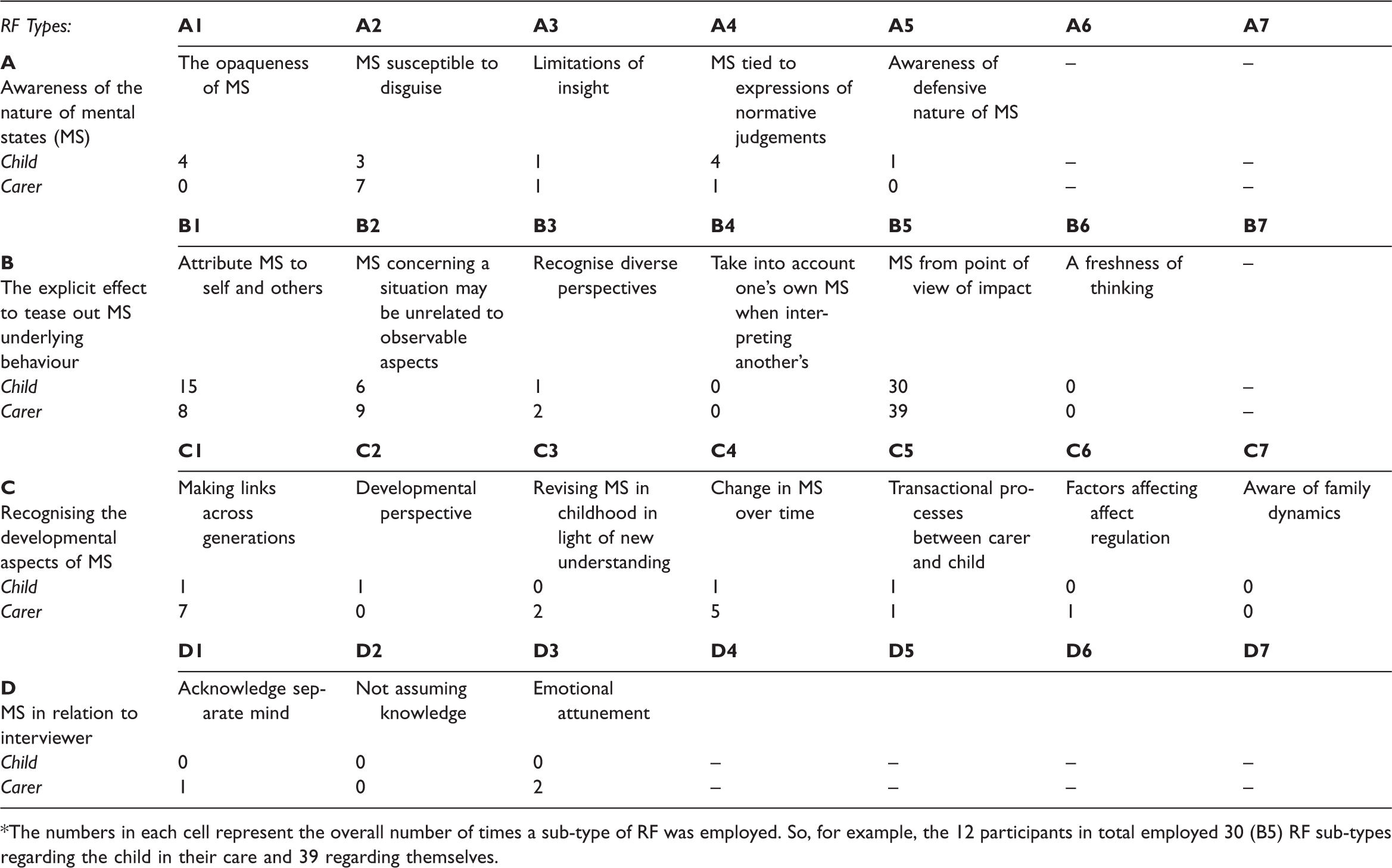
awareness of the nature of mental states – that they may be opaque and susceptible to defensive process; the relationship between mental states and actions; developmental aspects of mental states; evidence of reflection in the process of the interview. Profile of four categories of RF and their corresponding RF types for carers and children.* The numbers in each cell represent the overall number of times a sub-type of RF was employed. So, for example, the 12 participants in total employed 30 (B5) RF sub-types regarding the child in their care and 39 regarding themselves.
Each category has within it various sub-categories of types of RF and these are further divided according to whether they relate to the self (carer) or the child (see Table 1). From this information, an RF overall score is determined for each interview.
In addition to the PDI items, 18 questions charted the background characteristics of the carers and their history and experiences of fostering. Information was also requested about the young person’s care history, behaviour in placement and contact with birth family.
Analysis
The analysis adopted a novel coding approach that specified and separated RF related to self and RF related to the child and explored the differences and connections between them. An additional quantitative analysis of the breakdown of types of RF seen in the data was also undertaken. Finally, a thematic analysis of the content of the interview was conducted.
To do this, an overall RF score was allocated to each interview, along with additional scores for RF related to self and RF related to the child. RF profiles of each carer thus showed the quantity and range of varieties of RF revealed by interviews (see Table 1). Scores range from −1 (negative, hostile or bizarre RF) to +9 (full or exceptional RF). A score of 5 represents average or ordinary capacities in a non-clinical population and to achieve this there must be explicit evidence of at least one of the four categories awarded as a type. Scores above 5 thus indicate clear evidence of mentalising capacities and more sophisticated use of RF.
A thematic analysis was conducted on the PDI interviews, which followed a six-step approach as outlined by Braun and Clarke (2006). Four superordinate themes were subsequently generated.
The authors are qualified to administer and analyse the PDI and the interviews were independently analysed to increase inter-rater reliability. An independent thematic analysis of the interviews was also conducted separately by the authors. No substantive disagreements were found in either exercise.
Results
RF scores
As Figure 1 shows, the RF scores among the sample ranged from 3 to 7. While these differences may not appear huge given that a score of 5 represents average or ordinary reflective capacities in a non-clinical population (Slade, et al., 2003) and that the full gamut of possible scores was −1 to +9, it is important to stress that qualitatively these differences are highly significant. An RF score of 7 shows considerably sophisticated skills whereas a score of 3 indicates a very fundamental level marked by infrequent reference to and connections between states. This finding is surprising as the sample comprised therapeutic foster carers who provide long-term placements intended to promote positive changes in the children.
Profile of RF scores for each foster carer.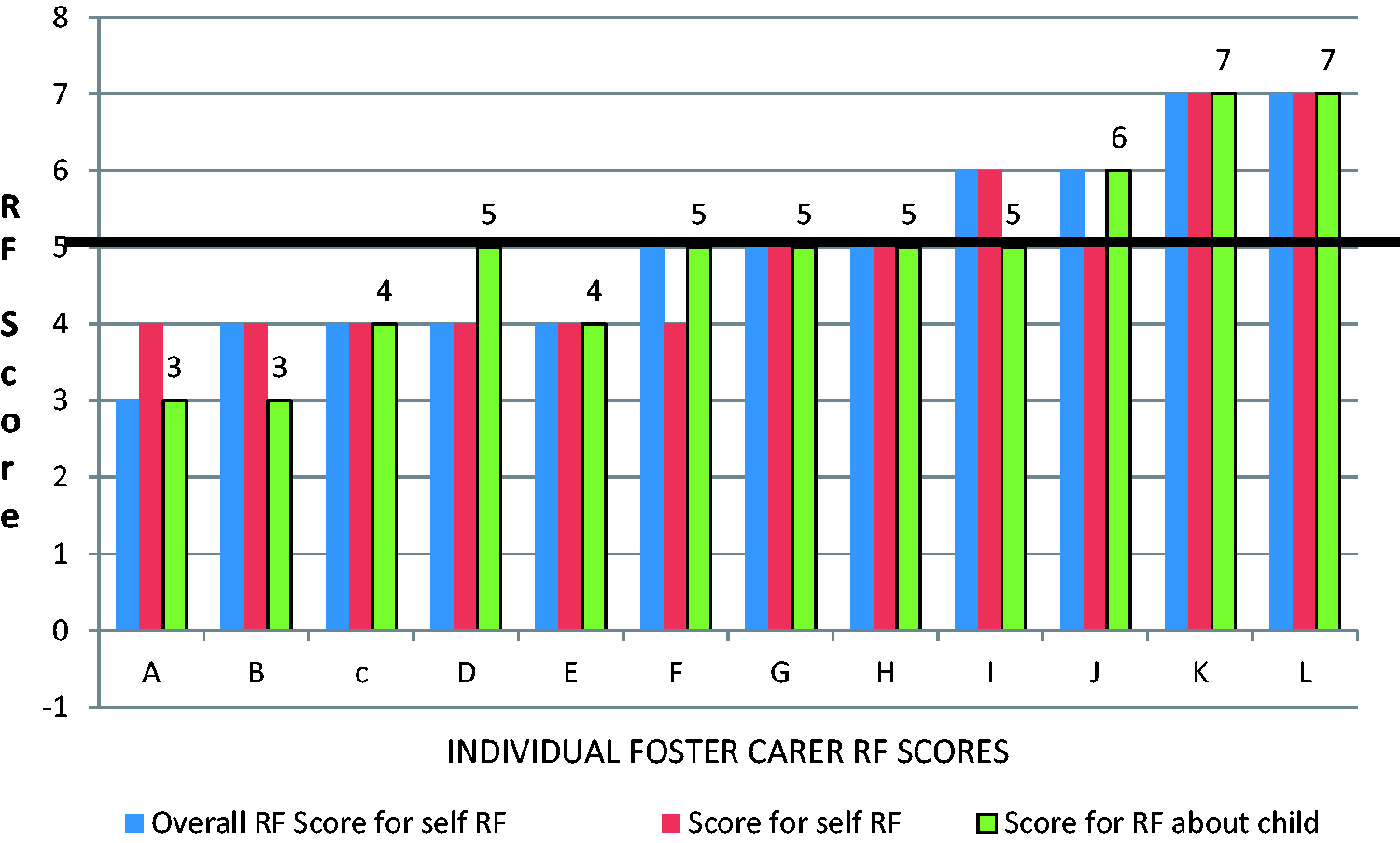
Although the sample size is small, a correlational analysis indicated that there was no significant relationship between carers’ RF scores and child or carer variables (age, gender, relationship status, length of time fostering). Some carers also showed different capacities for RF relating to self and relating to the child, with half the sample showing variation between the two scores. These variations were seen across the sample and did not simply relate to the carer’s overall level of RF.
RF types
The range and frequency of different ‘types’ of RF are shown in Table 1. The first column shows the four main types of RF (A, B, C and D) and next to these in the adjoining seven columns are the sub-types. Under each sub-type, RF scores are given regarding the foster carers’ use of these in relation to their own internal states and those applied to those of the child they look after.
Awareness of the nature of mental states (A types)
It can be seen from Table 1 that for RF type A, awareness of the nature of mental states, carers employed a wider range (all five sub-categories) of RF types related to the child, compared to those related to themselves (3). However, across the whole sample there were only five occasions when carers acknowledged that certain mental states are developmentally and psychologically expected (A4). There was a general trend that the higher the reflective capacities of the carers, the increased quantity of A types were expressed in relation to the child: Example: I think he was feeling worried or nervous, but I can’t be sure; it’s hard to know for sure. (Type = A3)
The explicit effort to tease out mental states underlying behaviour (B types)
This was the most common type of reflective thinking recorded. In particular B5, which concerns intentionality and making links between mental states as shaping actions (e.g. ‘I felt frustrated so I think that made her feel a bit nervous’) was by far the most common form of RF. Carers seemed to have an equal capacity for reflecting on the mental states underlying their own and their children’s behaviour. There was a general trend that the higher the reflective capacities of the carers, the increased amount of reflections they made about the mental states underlying the children’s behaviour. Example: He’d trashed his room, but I think he wanted me to see just how angry he was with the whole thing. (Type = B1)
Recognising developmental aspects of mental states (C types)
C types were more common in the higher RF scoring participants and limited or absent among carers assessed as having lower RF capacities. Analysis suggests that carers had a greater ability to reflect on the developmental aspects of their own mental states than those of the child. Example: In the past he used to struggle with feelings of jealousy, but more recently that’s less of a problem. Don’t get me wrong, he still wobbles but he manages himself better now. Maybe he’s feeling a bit more settled. (Type = C4)
Mental states in relation to the interviewer (D types)
This was found to be a rare type of RF but was more common in the profiles of higher scoring participants. It involves the capacity to hold in mind the listener’s mental state, orient them towards understanding the accounts being offered and comment on their possible reactions and interpretations. Example: I’m sorry; it’s quite a story to get your head around. It’s probably a bit shocking for you to hear first off. I forget this. (Type = D3)
Thematic analysis
In addition to the PDI analyses, four themes were extracted from the interviews:
1. Still struggling to cope with aversive early relationships and experiences
The majority of the carers noted difficult primary relationships or traumatic incidents in their own childhood and suggested that cultural or societal trends may have influenced their upbringing and their parents’ behaviour. They described how opportunities had been lost, relationships remained unrepaired and resolutions in understanding left unresolved: I did patch things up with my dad, and then blow me down, he went and got Alzheimer’s and it just threw me, completely threw me. And I always think to myself [starts to cry] … I always think I wanted to ask so much about my mum and I just didn’t have the time to do it. It was like ‘Oh God’ … It was like he had the last say … I just thought I was so angry with him to think that he could take it all with him and not share any of it and I was really annoyed with him. You do get really and emotionally like, up with it all and I had a flash … She’s just a young girl who just wants to be loved [crying] I am sorry … I can really relate to the whole rejection thing with her … so I am very honest with the girls. I know how tough it is.
2. Struggling to manage difficult needs and feelings
All of the foster carers said how much fostering had dramatically changed their lives. Many noted that they had not anticipated how significant its impact would be and how it was not possible to prepare for such a change: Honestly, if I knew the depths I had to go into and the alterations to my life, I wouldn’t have done it. I really wouldn’t have done it. You can’t really prepare − you can try, but they can’t prepare you for everything that is involved, the total disruption to your life. Sometimes he knows when I feel sad and has got this way of, not saying are you feeling sad, but he’ll come in and say, ‘Are you alright?’ and I’ll say ‘Yeah, fine.’ And really I’m not, but I’m trying to convince him that I am, I’m trying to hide it, because I don’t want to affect, or I don’t want to put onto him how I feel. Um. I think with him, emotionally, seeing me cry upsets him more than he lets on. Very often he just ignores me. I get a little bit upset sometimes, when I tuck him into bed he won’t say goodnight. I know I should get used to it after all these years, but it does hurt.
Developing an understanding of the child
Carers reflected on the struggles and limitations of understanding the child and acknowledged that there were aspects of his or her behaviour or history they did not know about or were not sure of. They drew upon several strategies to try and make sense of the children, including alluding to the child’s temperament and diagnosed conditions. Interestingly, ideas from attachment theory rarely featured in trying to understand a child and specific examples of how his or her past linked with present feelings or behaviours were infrequent, usually only occurring in the higher scoring transcripts: But with fostering you get a 13-year-old child that you haven’t got a clue what has made them really. You have got a little bit here and a little bit there but it is mostly about their behaviours and things to be worried about … but nothing about the background and what made that child that child. You have to sort of pick away at the person don’t you? And find out what makes them tick really and they pick away at you, testing you and see what makes you tick. I used to think there was one way of bringing up children and that was my way and sometimes that just hasn’t worked with her for whatever reason and you have to look at different tactics … when it’s somebody else’s children you feel more duty to try different things.
4. What is possible?
Carers spoke of a deep love and genuine desire to make a difference to the lives of the children they looked after. A majority recognised the requirement to adjust their hopes and goals to realistic levels and longer-term timeframes: I would say I’ve probably been pulled up a few times about setting my standards too high. Um, I’ve slightly lowered my standards believe me, but I have to have my own personal standards; me, I came into fostering to change the world, I wanted to change all these young people that came into care. He wants to get rid of the memories, the demons inside his head, but will he ever get rid of them? … Actually get him to a place where he feels comfortable with himself … because he knows that he’s not comfortable with himself sometimes. I don’t know if he will.
Discussion
The range of overall RF scores from 3 (showing little evidence of the awareness of mental states) to 7 (sophisticated thinking about the feelings underlying behaviour) indicates that while no individuals showed an extreme result, skills varied considerably among the participants. Since RF is positively correlated with secure attachment, this finding suggests that some carers may struggle to develop this type of functioning with the children they are looking after. Moreover, given the ages of the children, opportunities for making a positive impact on a child’s attachment stance are likely to be further reduced since early strategies become increasingly cemented as he or she gets older. Higher levels of RF in carers would maximise the chance of change and help promote well-being within the placement. This variation in RF capacity is surprising given that these carers were designated to provide therapeutic foster care.
What is new about this study is the separating out and independent assessment of RF related to self and child. Findings indicated that these scores can differ, with half the sample showing variation between the two domains. This could mean that there are two separate branches to RF that operate by related but distinct mechanisms. Current literature suggests that a caregiver’s development of self-related RF is a prerequisite to thinking about their child (Koren-Karie, Oppenheim and Getzler-Yosef, 2008), but surprisingly, this study revealed that some carers demonstrated higher levels of child RF than self RF. This extends Koren-Karie and colleagues’ work by suggesting that what is most beneficial is a balance between RF towards self and RF towards child, rather than one being a prerequisite for the other. Such a balance reflects a more relational rather than linear approach to the processes involved in child–carer interaction. Further research in this area is warranted, especially given the potential significance for clinical practice and theoretical understanding.
There were wide variations in the use of different types of RF, with B types (teasing out the mental states underlying behaviour) employed most often, regardless of the carer’s overall RF score. Here B5, which concerns the more immediate reflection on how mental states and actions are linked, was by far the most common. Other types were expressed much less frequently and were especially rare in carers who showed lower overall levels of RF. In particular, it is significant that RF related to less immediate factors, such as the child’s developmental history; or recent events at school and elsewhere, were relatively seldom considered. This suggests that carers might need support to enable them to employ more developmental skills and in so doing would benefit from having more information available on the child. However, this could pose a dilemma for agencies since they recognise that information which appears overly negative or which is clumsily presented may well deter potential carers.
It is possible that the particular RF patterns captured in this sample relate specifically to the fostering population. For example, all carers used more C type explanations and a wider range of C types (recognising developmental aspects of mental states) about themselves than they did about the child. This indicates a better recognition of the developmental aspects of their own mental states than those of the young person in their care. Looked after children often do not operate at their chronological age, displaying the cognitive and psychological abilities of much younger children. It is also unlikely that the child has grown up with the carer; unable to rely on direct experience, carers have to develop an understanding from external sources of information that are harder to internalise. It is conceivable that these factors make recognising the development of their child’s mind more challenging and limit the type of reflection available to the carer. Certainly this hypothesis is consistent with themes emerging from the analysis that emphasise the complexity and obstacles of ‘developing an understanding of the child’. Again, this also may be linked to the frequency of (B5) RF, which concerns the more immediate connections between mental states and actions.
The profile of RF types used showed that carers employed a wider range and increased frequency of A types (awareness of the nature of mental states) about the child than they did about themselves, with the exception of noting that their own mental states were susceptible to disguise (A2). It was noticeable that this pattern also connected with the theme ‘struggling to manage difficult needs and feelings’, which arose from the thematic analysis. Carers commonly identified that in order to protect themselves and the child emotionally, they had to hide, minimise or ignore their own needs. When considering the potential consequences of this coping strategy, it is important to note that none of the carers acknowledged that their interpretation of an event might be distorted by their own feelings (B4). This suggested that carers had a lack of awareness of how their own internal states or histories could interplay within and crucially misrepresent their current relationships.
The carers’ understanding of the effect of their own histories on their parenting may be even more vital in long-term therapeutic foster care. The theme ‘still struggling to cope with aversive early relationships and experiences’ suggested that many carers still had difficulties related to their own early relationships. This is consistent with previous research suggesting that adopters are more likely to have experienced loss or trauma compared to other parents (Bates and Dozier, 2002; Kaniuk, Steele and Hodges, 2004; Steele, et al., 1999). This is significant because a child’s behaviour or feelings may activate unresolved or poorly integrated issues in the carer. Where this happens, RF is likely to be blocked, resulting in both carer and child having a poor sense of safety within the relationship. Carers spoke of how their own negative experiences allowed them to feel a deeper empathy for the child, for example, that they had been through the ‘same experiences’. However, it may also be important to help carers recognise that such a sense of personal identification with the child’s painful experiences cannot only generate compassion but also lead to over-identification in which they miss important differences between the child’s and their own experiences.
Clinical implications
A further examination of the particular types of RF used by foster carers showed that they did not often consider that a child’s feelings could be unrelated to immediate external circumstances (B2) and most often focused on current intentionality in terms of what mental state might have shaped current actions (B5). The lasting effects of trauma and loss can be difficult to recognise and painful to sit alongside and attend to. Carers need to be supported to understand the long-term consequences of trauma for a child. Failure to notice that responses are unrelated to the present moment could risk a response that does not meet the child’s needs. Carers do demonstrate a general understanding of the lasting effect of a child’s past, as captured in the theme ‘What’s possible?’, but advancing this capacity by thinking more specifically about the trauma experienced and how it manifests in daily life could give them more confidence to react in attuned ways. Excessive or misattribution of traumatic states can be detrimental for guiding the child’s development too. In this respect, guidance that distinguishes between behaviours that are indications of traumatic states and ordinary ‘naughtiness’ that benefits from clear boundaries and consequences would be helpful.
Training in systemic thinking might also have some benefit. There was an overall lack of systemic and relational thinking contained in the transcripts. Carers displayed very little expressed understanding of the transactional processes between parent and child (C5) or the recognition of family dynamics (C7). Nor did they show knowledge of their role as regulators of the child’s feelings (C6). All parents have a crucial part to play in helping children to trust in relationships and to learn appropriate ways of managing their emotions. Encouraging carers to think from a relational perspective would strengthen their capacity for these essential tasks.
Foster carers further indicated that while they consistently minimised their own needs, they recognised the importance of developing and nurturing a reciprocal relationship. The acknowledgement that attachment needs are mutual has significant implications. Carers who do not feel they are appreciated or receive positive feedback from the child may feel less connected to him or her, possibly leading them to reject the child. It was noticeable that the lowest RF scoring carers spoke of their child ‘not giving back’. The RF types displayed by carers may vary according to the particular child but we would suggest that the capacity for RF should be viewed and interpreted at a relational level.
Clinical use of the PDI in foster care
The PDI is an extensive interview and its use in its full form might be prohibitive in many fostering contexts. In this research and in our own training we found that it was possible to employ parts of the interview to gain an overall indication of RF and also to allow a separate consideration of self and other RF. Using parts of the PDI in various aspects of the fostering process might be helpful in several ways:
Recruitment
The PDI includes questions regarding the potential carer’s own attachment history. For example:
How do you think your experiences of being parented affect your experience of being a parent now? How do you want to be like and unlike your mother/father as a parent? How are you like and unlike your mother/father as a parent?
If the applicant has children of their own, parts of the interview regarding the relationship and their understanding of the child’s perspective can be employed, as can questions requiring consideration of the child’s mental states (see below).
Training
The above three questions could be developed further but need to be extended to include exploration of the carer’s understanding of the child’s mental states. For example:
Describe a time in the last week when you and (your child) really ‘clicked’ and a time in the last week when you weren’t ‘clicking’. How do you think (your child) felt? When your child is upset, what does he/she do? How does that make you feel? What do you do?
These questions could be developed into considerations of typical case scenarios so that the carers do not feel personally threatened by the questions. Video sequences could be used to illustrate these scenarios and to ask the carers what they think the carer and the child are experiencing and what they might feel and think if they were one of them. The training could also include explorations of specific problematic issues, such as anger, lying and withdrawal, in terms of mental states involved in the carer and the child.
Ongoing support and problem consultation
Continuous support could focus on specific examples of problems that carers have been experiencing and be explored in terms of considerations of mental states for them and the child. An approach that we have found helpful is to analyse problems by exploring specific relational sequences (tracking) in terms of actions, thoughts and feelings for both parties. This can be undertaken in one-to-one situations or group support so that carers assist one another to consider such problematic cycles in terms of alternative mentalisations and responses to the child. Importantly, this invites the carers to consider their own role in triggering and maintaining problematic patterns.
Although skills such as RF are usually learned in early childhood, it is possible to nurture and develop them in later life (Gullstad and Wilberg, 2011). The focus of such training would be to enhance RF scores by encouraging and actively advancing attachment, developmental and systemic thinking. Carers would be encouraged to be accepting and curious about the connections between the child’s past traumas and current feelings and behaviours. They could also be helped to reflect on the impact of their own well-being and histories on how they view and interact with the child.
In conclusion, the value of this study lies in its use of an innovative approach to the assessment of RF among a special population. We acknowledge that the sample size was small but suggest that the findings raise a number of important questions that merit further study.