
Abstract
The number of UK children seen with complex behaviour difficulties where there is a history of exposure to alcohol and/or drugs prenatally appears to be increasing at an alarming rate. Community paediatricians work with vulnerable children and also act as medical advisers to adoption panels, so they have a unique overview of the unmet needs of looked after children affected by Foetal Alcohol Spectrum Disorders (FASD). This article reports on two simple audits of children seen in a community paediatric clinic setting. The first audit counted the number of children seen during a period of two-and-a-half years between April 2010 and August 2013, where there was a clear prenatal history of alcohol exposure. This audit also specifically looked at how many of these children might have Foetal Alcohol Syndrome (FAS) or FASD. Seventy-two children were given such a diagnosis within the time frame. The second audit reported on children looked after and children put forward for adoption during a 12-month period from January 2013 to December 2013. It reported a history of prenatal exposure in 55 out of 160 health assessments for looked after children (34%) and in 34 out of 45 medicals for adoption (75%).
Background
In recent years the number of children seen with complex behaviour difficulties where there is a history of exposure to alcohol and/or drugs prenatally seems to be rising at an alarming rate. The prevalence of Foetal Alcohol Spectrum Disorders (FASD) in the UK population is unknown but estimates for Canada and the USA suggest rates as high as 1:100, with the prevalence of Foetal Alcohol Syndrome (FAS) at 1:1000 (BMA Board of Science, 2007; Chudley, et al., 2005; May and Gossage, 2001). Looked after children (LAC) are a particularly vulnerable group for whom the likelihood of prenatal alcohol and substance exposure is greater than for the general population. Those with FASD should be identified early so that an accurate assessment, appropriate support and advice for carers, early intervention for challenging behaviours and support for learning difficulties can be offered.
When FASD are suspected, the community paediatric department is often the first place that a referral for assessment is sent. There is little evidence in the UK that these departments have a clear understanding of the magnitude of the problem or the ability to assess and manage the rapidly increasing numbers of affected children (Elliott, et al., 2006; Eustace, Kang and Coombs, 2003; Mukherjee, Hollins and Turk, 2006a). There are no FASD prevalence studies in the UK and so doctors are unable to inform the health commissioners of the services needed to provide an adequate level of care. Until we start to recognise FASD and collect prevalence data this situation will not change.
Community paediatricians work with vulnerable children, including those looked after, and also act as medical advisers to adoption panels. Therefore they have a unique overview of the unmet needs of children at risk in their locality (Gahagan, et al., 2006). This article reports on two simple audits of children seen in a community paediatric clinic in the UK city of Peterborough. The first audit counted the number seen during a period of two-and-a-half years between April 2010 and August 2013, where there was a clear prenatal history of alcohol exposure. This audit also specifically looked at how many of these children might have FAS/FASD. The second audit reported on children looked after and children put forward for adoption during a 12-month period from January 2013 to December 2013.
Peterborough, in the east of England, has a high level of social deprivation; it also has seen a large increase in population in the last few years. According to demographic data gathered by the Peterborough Children's Trust Partnership Board (2010), the rates for childhood poverty were significantly higher than the rest of the UK: in eight of the 24 local authority districts, the poverty rate was over 30%, with the highest reported at 35%. The average rate for the UK was 21.4%.
Peterborough City Council statistics for 2012 record a population of 186,400. There were 3300 live births per year, 14,700 children under five and 34,600 children aged 5–19. Since 2004, there has been a large increase in the number of migrants, particularly from Eastern Europe, and the population has risen by 12.3%.
Before the audit started in 2010, only two children diagnosed with FAS were recorded on the community child health system and none with FASD. Documentation of possible pre-birth exposure to alcohol and drugs was patchy and rarely linked to the presenting problem for the child. Some clinicians were more likely to record this information than others; in many cases, despite the information being available, it was not documented at all in the child’s records. Professionals from all disciplines referring children for assessment provided inconsistent information on substance misuse in birth mothers and when mentioned, it was often part of a picture of domestic violence rather than specifically around any prenatal exposure experienced by a child.
The gold standard for making a diagnosis of FAS/FASD
The gold standard for assessments leading to diagnosis in the USA and Canada (Astley, 2004; Chudley, et al., 2005) always involves a multidisciplinary team. This is because there is no one test for FASD. Such a team would include a paediatrician, one or two psychologists, a speech and language therapist, an occupational therapist, a social worker and a family advocate. Before clinical assessment, time is taken to review a child’s clinical records and collect pertinent background information. The clinical assessment is then carried out over several hours, after which a comprehensive report with diagnostic information, advice and recommendations is made. A feedback session for carers and professionals is also offered.
Like most community paediatric departments in the UK, resources and staff are limited and access to this level of multiagency assessment is simply not available. It was therefore impossible for the department to replicate this standard of assessment.
For the purpose of the audits a diagnosis of FAS was made using the standard US and Canadian criteria (Chudley, et al., 2005):
growth deficiency before and after birth – weight and length/height below the 10th centiles;
1
FAS facial phenotype – short palpebral fissure length (distance between the inner and outer canthus of the eye), smooth or flat philtrum and thin upper lip as ranked on a lip-philtrum guide; central nervous system structural/functional abnormalities in three or more domains – this includes microcephaly, neurological signs, deficits in cognition, academic achievement, executive functioning and poor working memory, and difficulties in social communication, abstract reasoning, adaptive behaviour and attention deficits; a confirmed history of prenatal alcohol exposure.
FASD was diagnosed if the child did not have all the facial features and/or growth was not affected, but did meet the other criteria. Assessments for cognitive functioning were not available for every child and executive function testing was hardly ever an option. Central nervous system functional abnormalities were therefore assessed on clinical assessment using standard developmental assessment tools or if there was evidence of attention deficit. Occupational therapy assessments were available, but speech and language assessments were not. The audit method required an identified problem in three or more areas of cognitive functioning to make a diagnosis.
Assessments for children thought to have FASD are often requested in a piecemeal fashion, with paediatricians asking for sequential assessments with little opportunity for joined-up thinking between the different professional groups. Not surprisingly, the process took a long time and it was very difficult for children’s carers to understand the process and when and how a diagnosis could be made.
Audit 1
This retrospective audit was carried out on children who had been seen in the city’s community paediatric clinics between April 2010 and August 2013. In all cases, the children had been referred for an assessment of complex behavioural difficulties. Also included were looked after children who had been referred for statutory health assessments where behavioural difficulties were noted at the time they were seen. In most cases, the information on prenatal alcohol and/or drug exposure came to light only during the assessment, though in a few cases the information was provided as part of the request for assessment. Simultaneously, to increase local knowledge and awareness of FAS/FASD there was a programme of intensive training for local multiagency groups, including health professionals, social workers, teachers, drug and alcohol teams, foster carers and prospective adopters. It was clear that towards the end of this audit, when some index cases had been identified with FAS/FASD, their siblings or similar cases known to professionals were more likely to be referred directly for assessment and advice.
Number of children identified as having a diagnosis of FAS/FASD between April 2010 and August 2013.
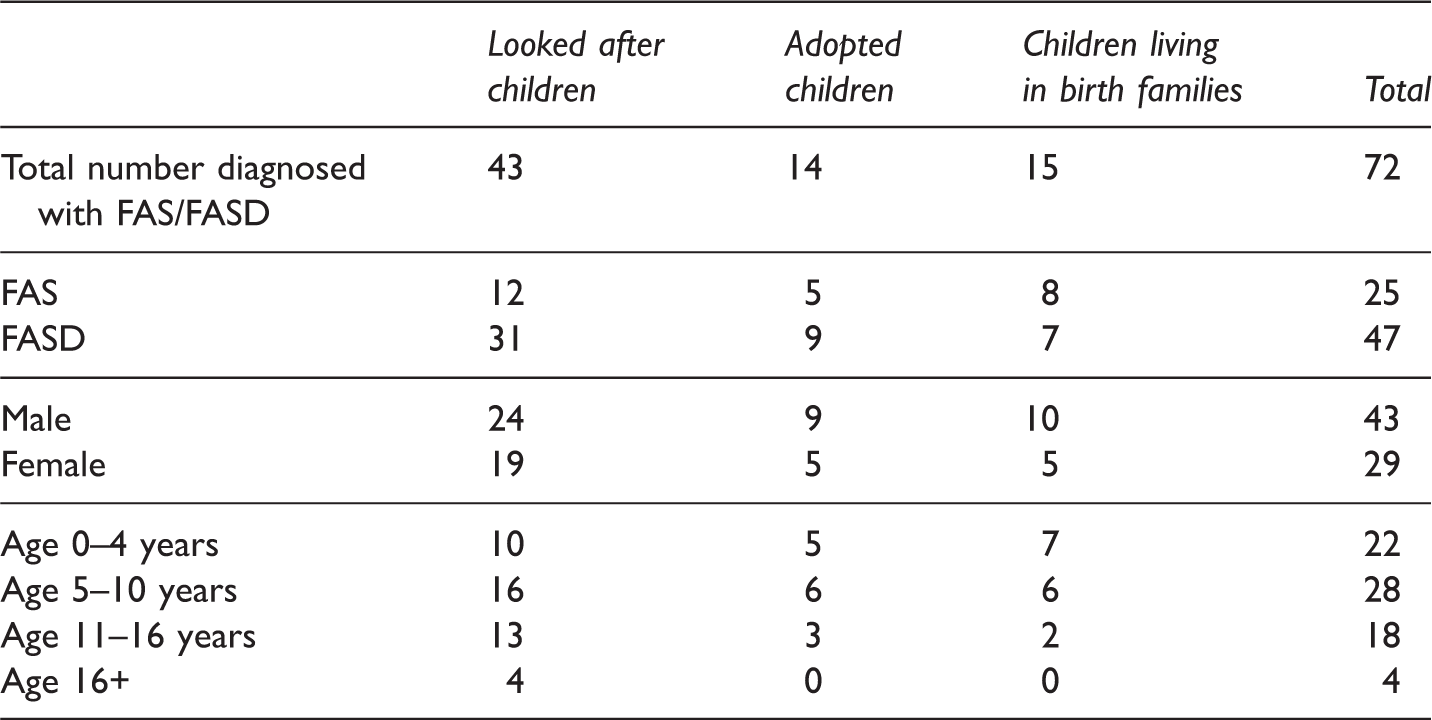
Forty-three of the children (60%) were looked after by the local authority; 14 were adopted and of these, six were given a diagnosis before the adoption order was made. In eight cases the diagnosis was made after adoption, when the child was presenting with difficulties. In most of the latter group the adoptive parents had no prior knowledge of possible long-term problems. For adopted children there is an emotional impact from being diagnosed with FAS/FASD many years after adoption. For parents it was usually a relief to know ‘what was wrong’ with their child as they were often given numerous conflicting explanations for their child’s difficulties. However, the realisation that they had adopted a child who was likely to have continuing long-term needs was very hard for most parents to come to terms with, especially when they looked at the impact on their whole family.
Fifteen children were seen who were neither in the care of the local authority nor adopted but living with their birth families. Three resided with their maternal grandmothers, five with birth fathers, four with birth mothers, two with an aunt and one with a maternal cousin. These families did not have the assistance of children’s services or adoption agencies and often struggled to receive adequate understanding and support. In four cases, the children continued to live with their birth mothers who still had their own issues with drug and alcohol use. For all these children it was not easy to pick out specific alcohol-related neurodevelopmental difficulties. This was due to other complications, a fluctuating level of care, inadequate behavioural management and unresolved attachment issues, or in many cases a combination of all these factors. Nevertheless, it is important to recognise that the children themselves had intrinsic and specific neurodevelopmental difficulties due to alcohol induced brain damage as well as to the detrimental environments in which they were growing up.
Children identified during the audit period April 2010 to August 2013 as having a history of Neonatal Abstinence Syndrome (NAS).
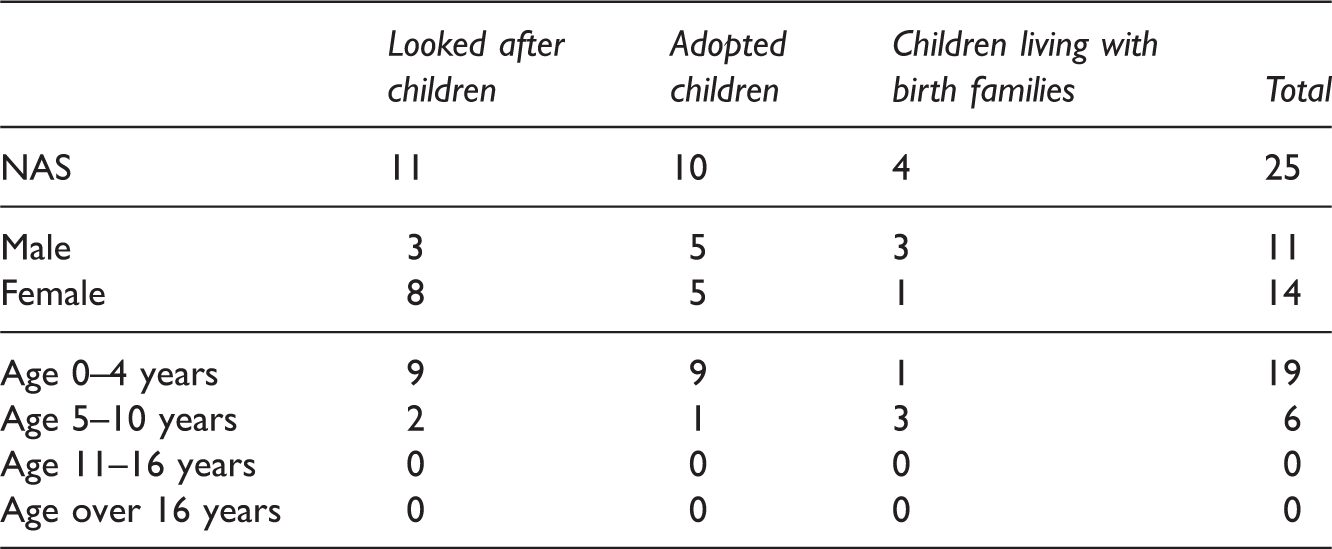
At risk but no diagnosis
At risk: children who had documentation of exposure to drugs and/or alcohol in the prenatal period but were not presenting with challenging behaviours.
Of the adopted children, nine had a history of NAS treated after birth but at the time they were seen were not presenting with any other problems. An additional nine had a clear history of drug use in pregnancy but were not clinically treated for NAS after birth.
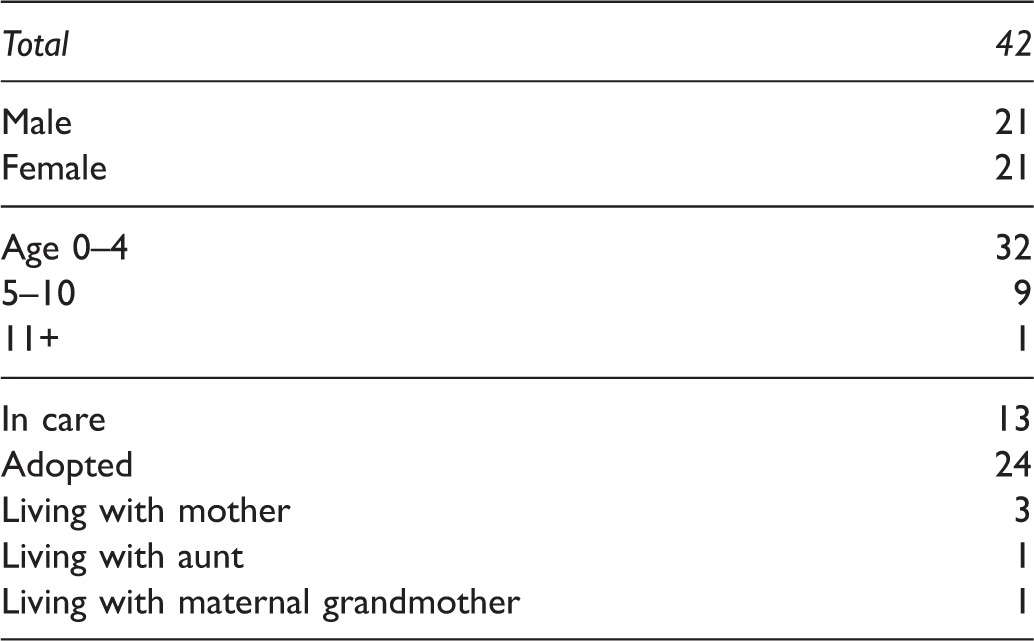
Thirty-two children (76%) were still under the age of four. However, they may develop problems in later life as FAS/FASD often present for the first time in primary school, at transition to secondary school or even at school leaving age.
Overall findings
This first audit was a retrospective assessment of how many children were noted to have a history of prenatal alcohol and drug exposure and to see how many were diagnosed with FAS/FASD. As it was a retrospective study, it would be difficult to give this number as an exact percentage of the total numbers of children assessed in the department. However, as an approximation, the community paediatric department received 2049 new referrals and 158 referrals for initial health assessment for children taken into care. Three per cent of all those seen had a diagnosis of FAS/FASD and for the looked after children it was 27% (43 cases out of the 158).
The number of children identified as being at risk increased steadily during the course of the audit. It is relevant that it also took place alongside an intensive training programme across a range of different agencies about the risks of drug and alcohol use in pregnancy. At the end of the audit period, most health professionals and social workers had changed their approach and were actively seeking information on prenatal alcohol and drug use as part of their initial assessments.
As this audit had found very high levels of affected children in the looked after and adopted populations, a second audit of looked after children (LAC) health assessments and adoption medical assessments was carried out for a 12-month period between January and December in 2013. The aim was to count the number of children seen where there was a clear history of prenatal alcohol and/or drug exposure documented in the prenatal period and measure this as a percentage of the total number of children assessed.
Audit 2
The second audit looked at initial and review health assessments carried out by community paediatricians during the 12 months. If a child was seen more than once during 2013, the case was only counted once and information on exposure to alcohol and drugs was only recorded as one event. Children and young people seen for health assessments by the specialist nurses mostly involved uncomplicated review visits and they were not counted.
A total of 160 assessments were recorded in the year. Of these, 88 were initial assessments for children who had recently come into care and 72 were review assessments seen by a paediatrician, as they were noted to have complex needs. The age range of the majority of children was between birth and 16 years, with just three young people over 16.
A summary of the main clinical health needs and any neurodevelopmental difficulty was documented for each child. Risk factors such as significant maternal health illness were noted as well as child abuse, if it was deemed to be significantly contributing to the child’s behaviour. A record was made where it was known that maternal drug and alcohol use was a significant factor in the prenatal period. When it came to older children, it was often difficult to find the evidence of prenatal exposure in the clinical records.
Results
Conditions identified in children seen for LAC health assessments in 2013.*
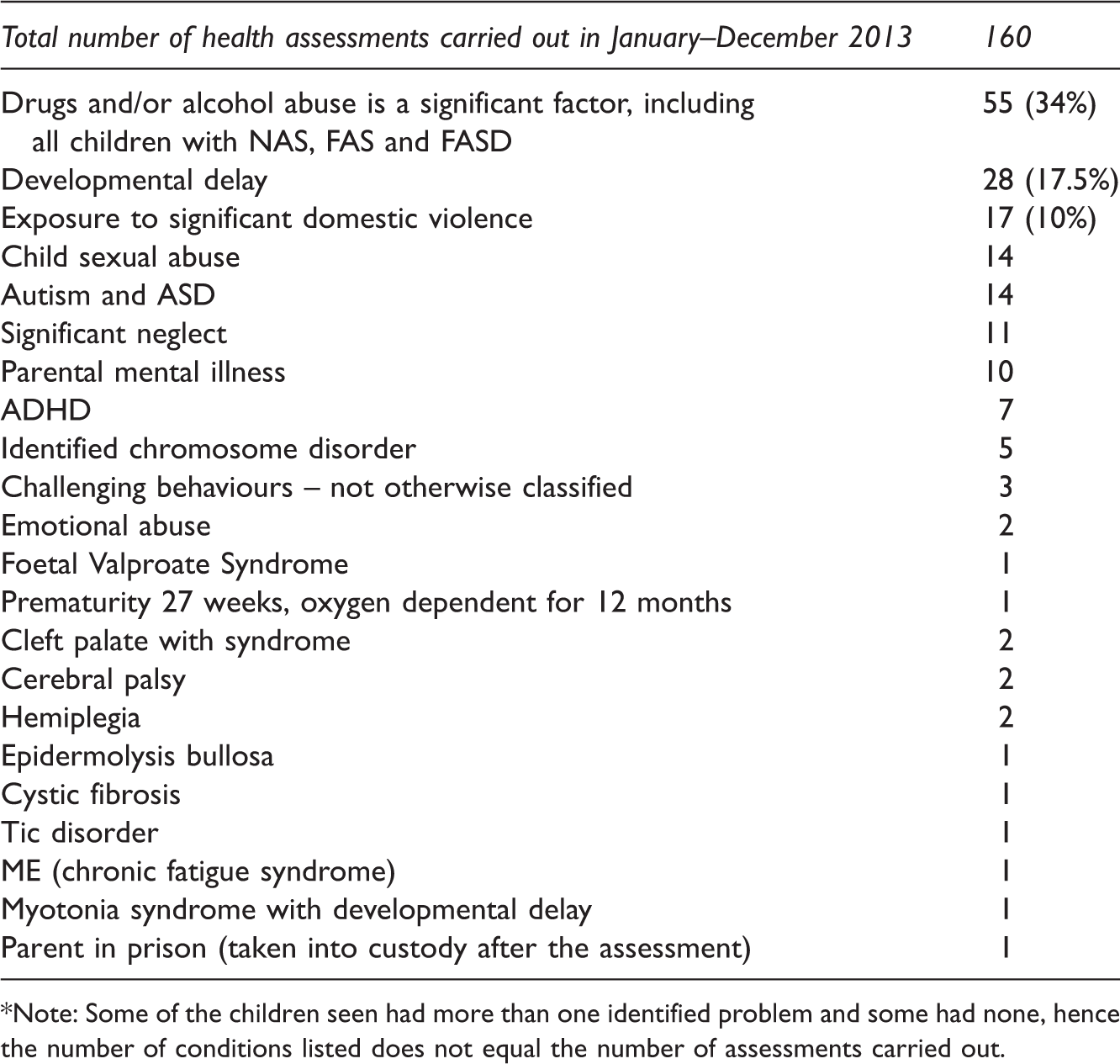
*Note: Some of the children seen had more than one identified problem and some had none, hence the number of conditions listed does not equal the number of assessments carried out.
It was noted that for 55 (34%) alcohol and/or drug use was noted to be a significant factor that needed to be considered as part of the ongoing assessment for the child. In 2013, this was by far the most significant health concern for children looked after and dwarfed all other health needs. All these children need long-term specialist follow-up, a situation which is neither available nor resourced at present.
Adoption reports
All adoption reports prepared and written in 2013 were audited, 45 of them specifically for the purpose of adoption. Some of these children also would have been seen as looked after children and so counted in the group above.
Among the 45 reports, 34 children (75%) had a positive history of exposure to alcohol and/or drugs in the prenatal period. While the number of reports written is not high, all of these children were under the age of five years, with the majority under two. Clinical symptoms often are not present at such a young age and physical characteristics may not be evident.
Consideration must be given to what advice and information is given to potential adopters and adoptive parents need access to assessment and long-term support, if appropriate at any time in the future. This finding is especially relevant to adopters proposing to adopt young children or babies, since few of them will have developed problems at the time of being placed (Autti-Rämö, 2002; Mukherjee, Hollins and Turk, 2006b; Mukherjee, et al., 2013; O’Leary, 2004; Riley and McGee, 2005; Sood, et al., 2001).
Conclusions
This article reports the findings of two community audits that identified children with documented prenatal exposure to alcohol with or without drugs.
During the timespan of the first audit, 72 children were given a diagnosis of FAS/FASD based on the best clinical evidence available at the time. Before, there had been only two recognised cases of FAS and no cases of FASD recorded in the community child health system. This is equivalent to about 3% of all referrals and 27% of referrals for looked after children.
The second audit revealed that 34% of children coming into care, 75% of whom were being put forward for adoption, had prenatal alcohol exposure. These are children at high risk of neurodevelopmental disorders and FASD.
Access to cognitive, behavioural and executive functioning assessments plays a key part in making a diagnosis of FAS and FASD, yet these are not widely available to most community paediatricians working with vulnerable children. It might be suggested that not being able to match the criteria for a ‘gold standard’ assessment partly could be to blame for the under-reporting of cases and lack of interest shown by other health agencies.
Vulnerable children presenting with difficult and challenging behaviours are likely to have more than one problem. There is a high rate of other developmental disorders such as attention deficit hyperactivity disorders (ADHD) and autistic spectrum disorders (O’Leary, 2004; Riley and McGee, 2005; Welch-Carre, 2005). Attachment disorders are also likely to be a significant factor. Whereas previously many challenging behaviours or disrupted placements have been put down to attachment alone, it is now becoming apparent that children may well have undiagnosed FASD.
This small audit revealed that around 40% of babies with symptoms of neonatal drug withdrawal also had evidence of FASD. More work needs to be done nationally to follow up these children, so that appropriate pathways of care can be set up. Many of the young babies with NAS are being adopted and potential adopters need to be given the correct information and advice at the outset of placement to ensure they are able to meet the child’s needs. A number of infants with NAS are discharged home with their birth mothers who are on drug programmes. These children must be identified as being more likely to have additional needs and it should be recognised that emerging behavioural problems cannot simply be attributed to the level of parenting, and appropriate assessment for neurodevelopmental difficulties needs to be offered.
Since the audits, changes to how children are assessed have been made locally and the training programme has continued to raise awareness. This has resulted in more children being referred for assessment and the information regarding prenatal exposure to alcohol, drugs and other substances being requested at a much earlier point prior to referral.
The most obvious difficulty in trying to persuade health commissioners of the need to fund services for assessments and management of cases of FAS/FASD is the lack of clarity regarding the number of children affected. It has wrongly been assumed that this is a rare disorder and that no additional support is needed to manage them. This is the first time that the workload which this population of children is generating, both now and in the future, has been documented. Our audits clearly show that exposure to alcohol and drugs in the prenatal period is one of the biggest issues facing health and social care. The UK urgently needs a statistically accurate prospective prevalence study to plan clinical services for the future for the nation’s most vulnerable children.