
Abstract

Why promote young children’s mental health?
Mental health promotion has been defined as ‘the prevention of mental illness and promotion of positive mental health’ (Friedli and Parsonage, 2007). Half of mental health problems start before the age of 14 (Kim-Cohen, et al., 2003) and one in 10 children and young people aged 5–16 suffer from a diagnosable mental health disorder (Green, et al., 2005). There is a considerable body of evidence to suggest that various psychiatric conditions can be prevented through effective early interventions and the promotion of mental well-being, which is particularly important in childhood and adolescence (Campion, et al., 2012). Promotion and prevention interventions make a strong case for policy investment (Knapp, McDaid and Parsonage, 2011) and have been shown to be cost-effective (Adi, et al., 2007).
NICE (National Institute for Health and Care Excellence) public health guidance also highlights that ‘children’s social and emotional well-being affects not only their mental health but also their physical health and can determine how well they do at school’ (NICE, 2008).
Looked after children
Statutory guidance from the Departments of Health and Education (2015) indicates that local authorities have a duty not just to treat but also to actively promote the mental health of looked after children (The Mental Health Foundation, 2002). Research has found that many mental health initiatives that work with the general population are also likely to be effective with this group (NSPCC, 2014). Education has been shown to play a key role in preventing mental health problems among looked after children (Department for Education and Department of Health, 2015), so schools provide an ideal forum for prevention and early intervention initiatives.
A Northern Irish initiative
We report on an evaluation of an initiative aimed at promoting mental health in primary schools called ‘Healthy Me’. This is a bespoke mental health promotion programme developed in Northern Ireland (NI) as a collaboration between the third sector provider AMH MensSana (the health promotion arm of the Action Mental Health), the Royal College of Psychiatrists (NI) Public Engagement Committee (RCPsych NI) and Step 2 CAMHS in the Southern Health and Social Care Trust.
The ‘Healthy Me’ programme emerged from the recognition of an unmet need in local primary schools. It was developed using modified elements of the secondary school mental health promotion programme run by AMH MensSana and drawing on existing evidence-based initiatives to promote emotional health and well-being among the 7–11 age group. The core features of the programme are shown in Figure 1.
What is the ‘Healthy Me’ programme?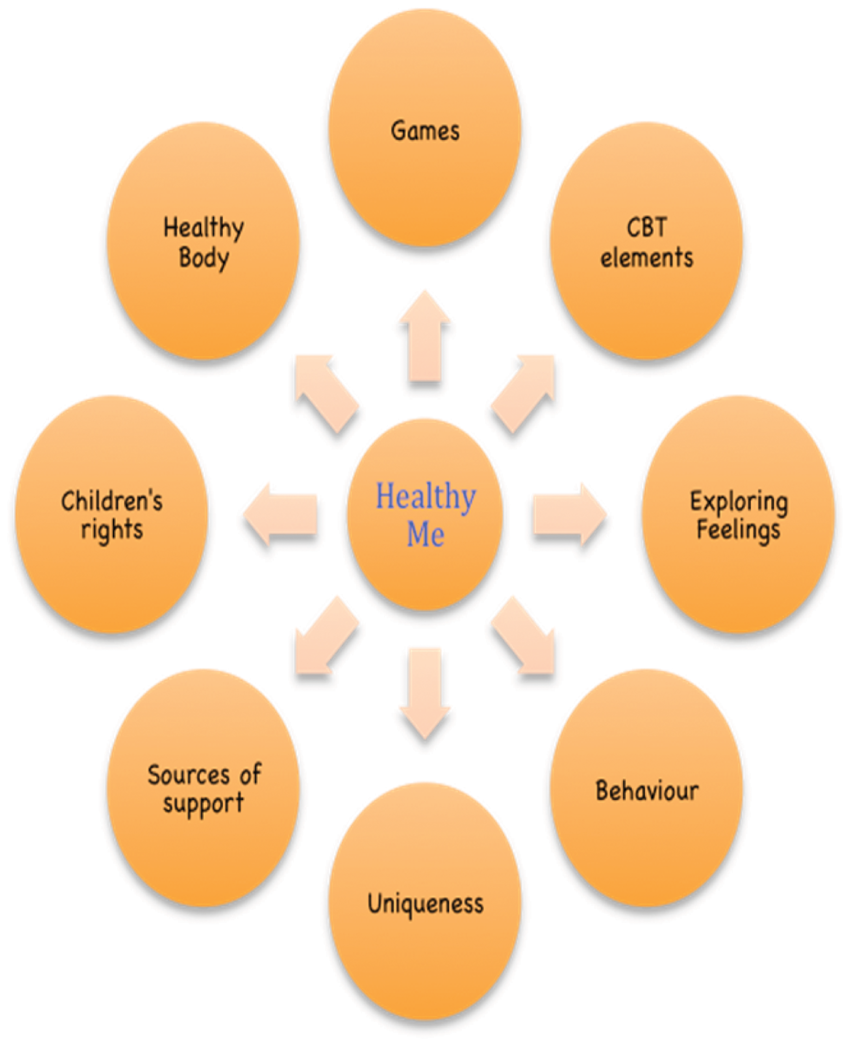
The programme is delivered as a three-hour interactive workshop with a powerpoint presentation to Year 6 and Year 7 pupils (ages 9--12). A bespoke workbook was developed to be completed by the children over the ensuing number of weeks. The following topics are covered using a mixture of games, small-group activities and discussion:
What is health? Healthy body, healthy minds Recognising and understanding feelings Coping strategies and accessing help Helping children understand their rights as per the United Nations Convention on the Rights of the Child (UNCRC).
Aims of the programme
To promote:
awareness of emotional well-being and positive mental health; parity of mental health with physical health; Help-seeking behaviour. To provide teachers with basic training in promoting social and emotional well-being
This universal health initiative aims to promote a positive whole-school ethos that avoids stigma and discrimination in relation to mental health and to catalyse a culture change where social and emotional difficulties are concerned. Transition from primary to secondary school is a particularly stressful time for children and it was hoped that targeting the programme at all Year 6 and Year 7 (Primary 6 and Primary 7 in NI) children would help them to cope.
Aims of the programme evaluation
To determine the feasibility of delivery, positive and negative aspects, and inform changes before a wider roll-out. To evaluate the effectiveness of the programme using qualitative and quantitative analysis of outcomes.
Before and after programme data on the children’s knowledge of aspects of physical and emotional health were collected using unvalidated structured and semi-structured questionnaires designed by the programme’s creators. Similarly structured questionnaires were also used to evaluate the children’s and teachers’ thoughts about it (see Appendices 1 & 2).
The participants
The programme was delivered to 267 pupils from five primary schools in the Southern Education and Library Board area with a mix of Catholic and Protestant ethos. One school had a large population of black and minority ethnic pupils with many non-English speakers; sessions in this school were punctuated by the sound of children translating in a variety of different languages for their friends. The cohort included children with learning difficulties, some requiring classroom assistant support.
A Medical Research Council decision-making tool indicated that this evaluation did not require formal research ethics council approval.
The evaluation
Evidence for mental health promotion interventions in schools indicates that one-off workshops do not constitute an effective way of influencing children’s mental health and well-being in the longer term (Weare and Nind, 2011). Post-workshop consolidation is necessary to stop the positive impact of the programme from diminishing over time. The ‘Healthy Me’ workbook and the creation of wall displays after the workshop were thus considered to be essential towards helping to consolidate children’s learning. Figure 2 provides an overview of the steps involved.
Structure of the programme.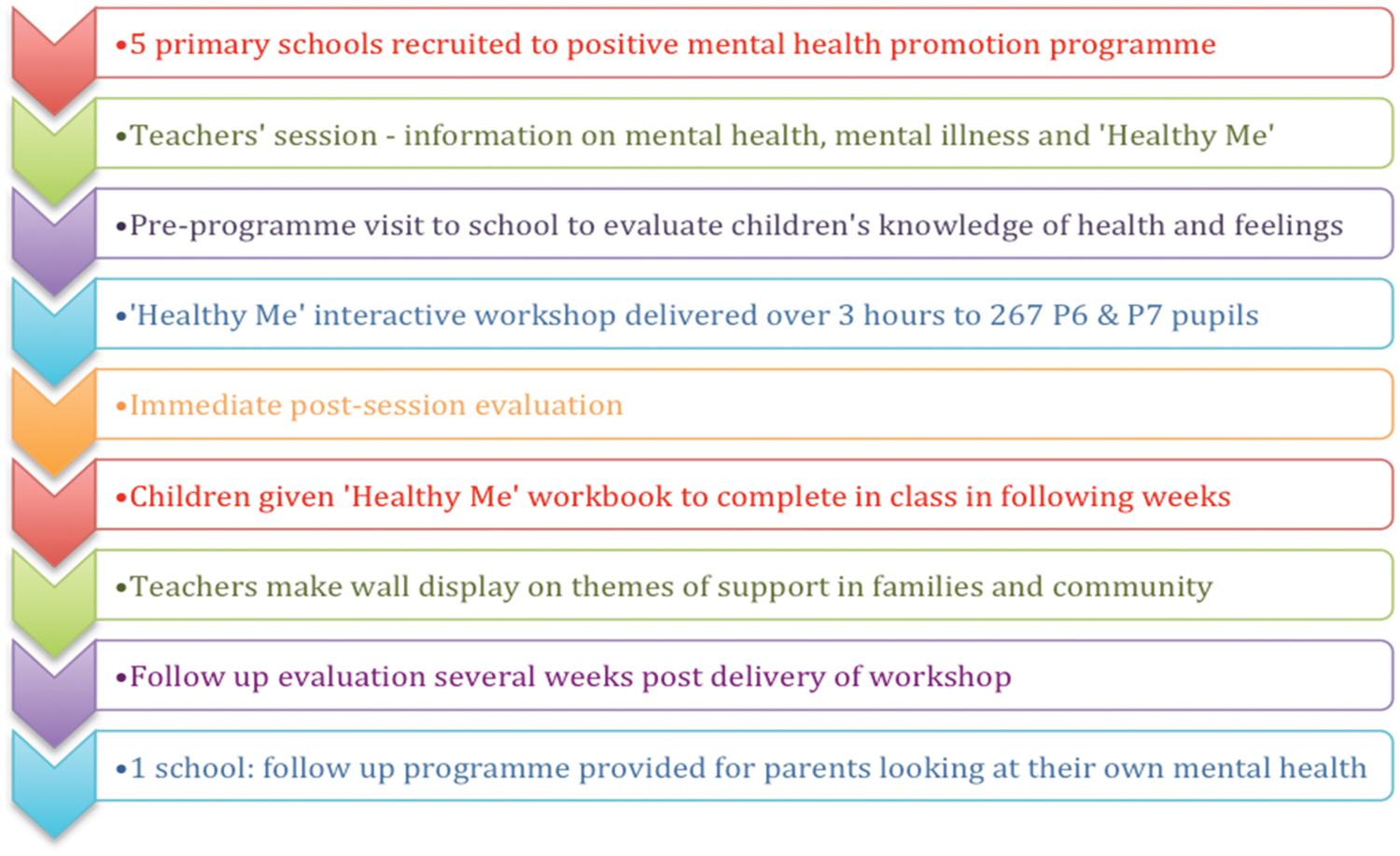
Results
Questionnaires assessing the children’s knowledge of physical and mental health were completed by 261 pupils before and three weeks after delivery of the programme. The children (49.4% boys and 50.6% girls) were aged between 9 and 12 years with the majority (87%) aged 10–11.
Figure 3 shows the percentage change in children’s knowledge of what it means to be ‘healthy’. There was a significant rise (p < 0.001) in recognition of mental health as a part of health (44.9% prior to session, 68.8% post session), reflecting an increased parity between mental and physical well-being.
Change in children’s knowledge of what it means to be ‘healthy’ (%).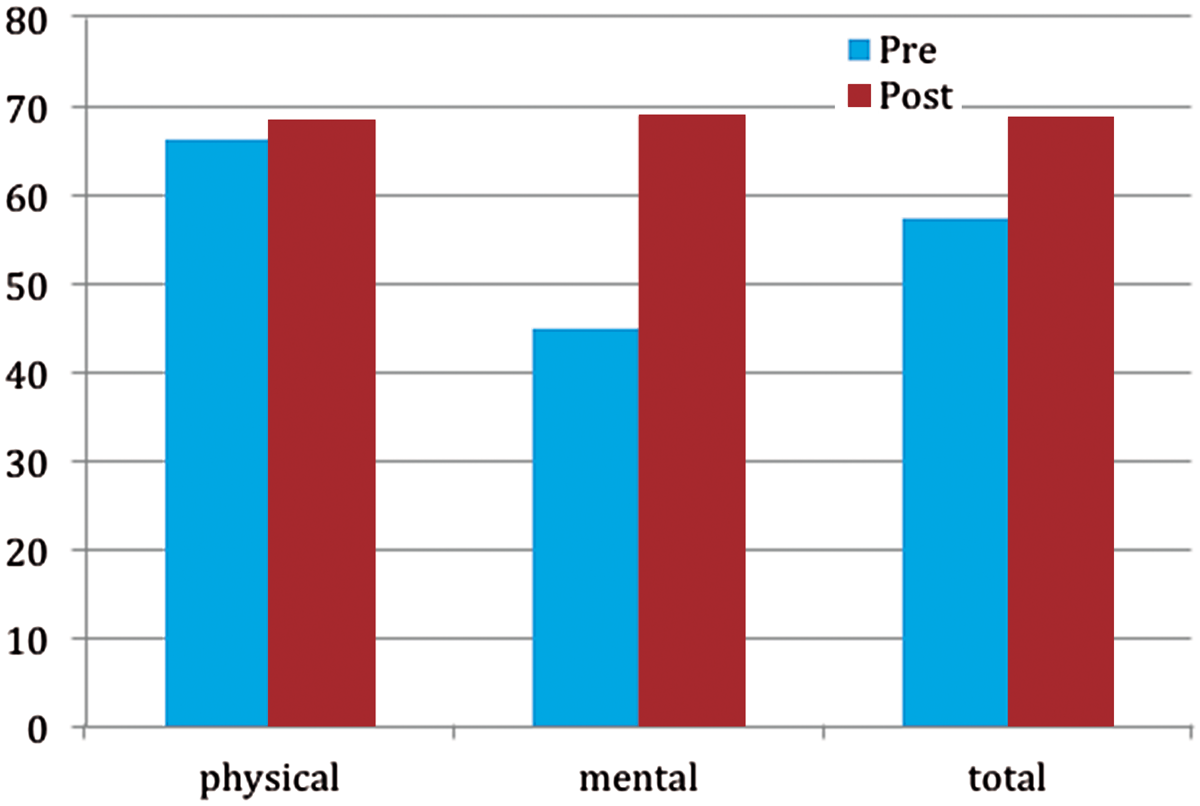
Via free text, children were also asked the question: ‘What can you do to stay healthy?’ Their answers were then coded into the five subgroups (see Figure 4).
What can you do to stay healthy?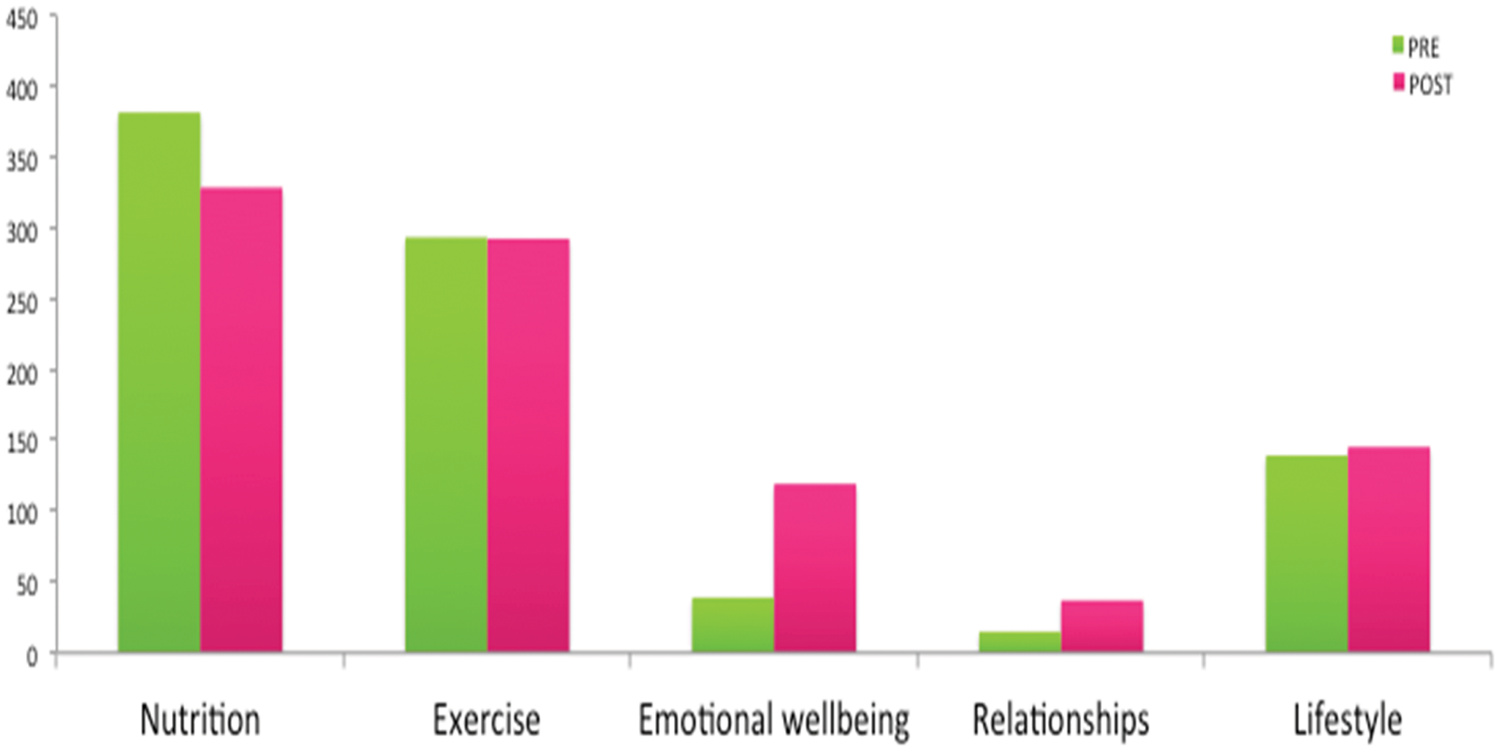
It is clear that before the session the children on the whole had good knowledge of the impact of nutrition and exercise on overall health – around a third were aware of the importance of lifestyle factors such as smoking – but very limited knowledge of the effects of emotional well-being or positive relationships on overall health. The children’s awareness of the significance of these last two areas showed the biggest increases (p = 0.001 emotional well-being and p = 0.042 positive relationships).
Feedback from the children
Zero to 10 likert-scale questions were used to assess the children’s enjoyment of, interest in and learning from the programme. Mean fun score was 9/10, mean interest score was 8.6/10 and mean learning score was 8.8/10. Clearly a very high percentage of children found it both fun and interesting, and learned a lot. Unsurprisingly, the interactive elements of the programme were the most enjoyed, with games being the favourite aspect for 21% of children and music the most popular for 12%.
Only 26 out of the 263 children highlighted something they did not like and out of those the most frequent response was that they would have liked more games.
Positive comments included: I loved every moment of it. I liked everything because I thought it was very interesting. I learned stuff, I had a great time and I understood everything. Thanks for the good time. I learned brilliant stuff so I am happy.
These show that the material was pitched at the right level. The comments seem to reflect what we know about children: they learn better when they are enjoying themselves.
Teacher’s evaluation
Feedback from teachers (%).
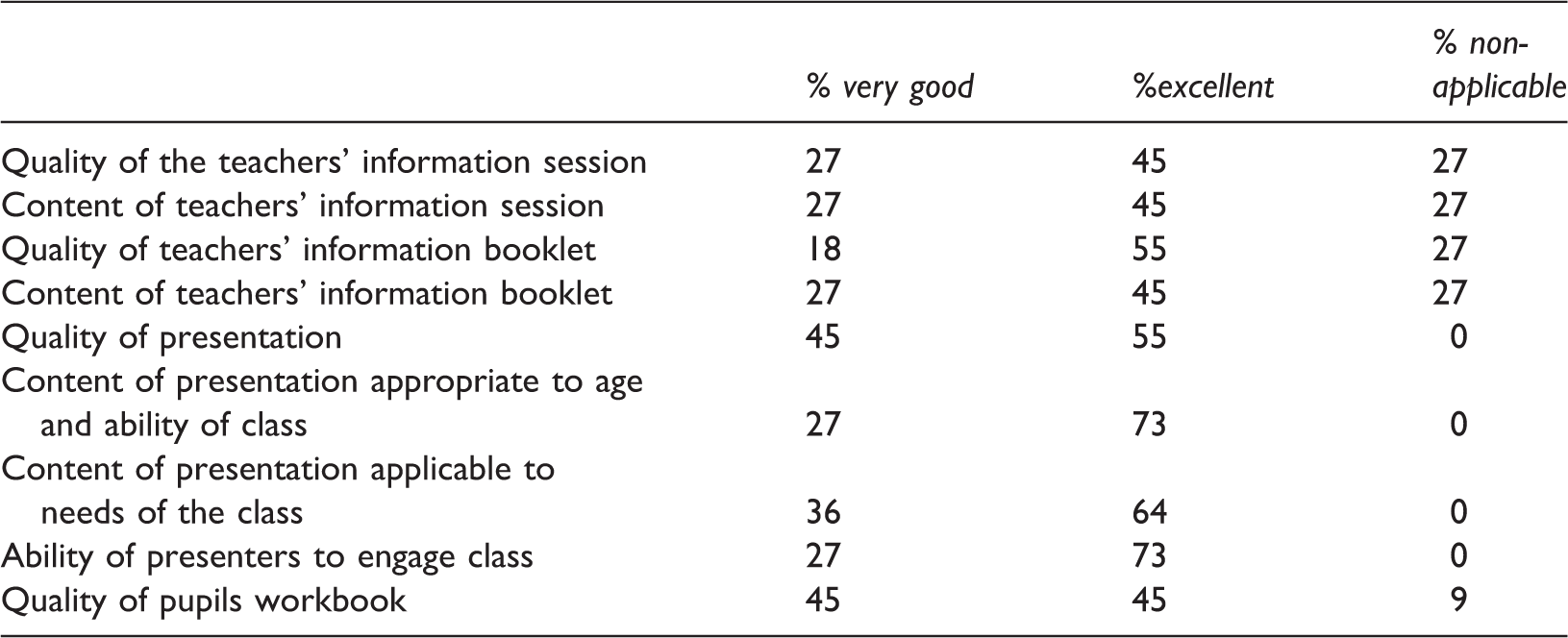
Among the comments were: General behavioural change – I haven’t needed to talk to the children as much about behavioural issues such as how they treat each other since. [They’re] more chatty about things to do with mental health. As a school [we are] very mindful of these things. [The programme] reinforced everything we try to do. The children have been coming in and talking to me about things that have happened in the playground . . . told me about someone being upset and said, ‘We tried to say to her to tell someone.’
All teachers said they would recommend the programme to other schools. It is clear from these comments that the children are reflecting on their own mental health needs and those of the class.
No negative effects were noted. Teachers said that they were glad the presentation did not mention mental illness as such but had a positive mental health message, and it was noted that the children did not perceive stigma around mental health at primary school age.
In terms of suggestions for improving the programme, comments were divided into the following themes: length of the session – aim to break it up; have a follow-up session to consolidate learning; include more activities and games; and develop the workbook. Including a parents’ session as standard could further strengthen the messages children are learning in school.
Conclusions
The ‘Healthy-Me’ programme was found to be feasible to deliver in a primary school setting and easily incorporated into the Personal Development and Mutual Understanding (PDMU) section of the curriculum.
Feedback from pupils and teachers was overwhelmingly positive, both in terms of enjoyment and usefulness of the programme.
The programme was found to be enjoyable and effective by a diverse range of children, including those from minority ethnic groups, with special educational needs and/or children with already identified social and emotional difficulties.
Children’s improved knowledge of the important aspects of physical and mental health after the programme was found to be sustained at follow-up several weeks later.
This was a brief programme with short-term outcomes, there was no control group, the data collected were mainly qualitative and outcome measures were not validated.
Evidence from systematic reviews of mental health promotion in schools indicates that for interventions to be most effective they need to be long term and embedded within the school curriculum, and that regular ‘booster sessions’ help to overcome the problem of diminution of effects over time (Weare and Nind, 2011). The longitudinal outcomes of this programme are not known. In addition, further work is needed to determine whether this universal prevention initiative is as effective for specific groups of children such as those who are looked after.
AMH MensSana have continued to run this programme within the Southern Trust area and plan to expand into other Trust areas in the near future. A Medical Research Council and NHS health research authority decision-making tool indicated that as a service evaluation project, this did not require formal research ethics council approval.
Footnotes
Acknowledgements
We would like to thank the following: Dr Hilary Boyd and Dr Peter Sloan for supervision and support; Cherith Edgar, Patricia Harte and Colin Loughran from AMH MensSana, Step 2 CAMHS SHSCT and the RCPsych NI Public Engagement Committee; and all the teachers and children who took part in the ‘Healthy Me’ programme.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.