
Abstract
The quality of the caregiver–child relationship is key to the well-being of children but assumptions based on research in western countries about the benefits of different types of substitute care may be questionable when applied elsewhere. This study assessed the quality of caregiver–child relationships and their association with child abuse in foster and residential care in Nigeria. The findings are relevant to European and North American countries as 4% of those looked after and 6% of care entrants in England are of African heritage and it is too easy to draw wrong conclusions about the care they might have received in their own countries. The study scrutinised 314 children aged 7–17 years from foster (157) and residential care settings (157) and assessed the caregiver–child relationship using the Positive Relationship Scale. The child abuse measure covered physical, sexual and emotional components and aggregated these into a single score. The subsequent analysis explored differences in child abuse between foster and residential care and the significance of other factors influencing levels of child abuse. It was found that the children in residential care had more positive relationships with caregivers than did those in foster care, even though abuse occurred in both settings. There were no gender differences in experiences of child abuse in either setting but children under the age of 12 were significantly more likely to have been abused while in care than those over this age. For children in residential care, age was the most significant factor associated with abuse. As these findings provide a perspective on children in substitute care in a West African city, they may be useful to social workers elsewhere who are responsible for children of African heritage, as they suggest that abuse often occurs in foster homes and that child–carer relationships in residential establishments can be good.
Keywords
Introduction
Child protection is a priority policy area for many human rights organisations and advocacy groups. While details of abuse and neglect are often poorly documented, the available data suggest that the rate of child abuse in Nigeria is substantial, with many children suffering from various forms of maltreatment, including physical, sexual and psychological abuse as well as neglect (Bowman and Brundige, 2014; Chinawa, et al., 2014; Ebigbo, 2003; Makinde, 2015; Obidigbo, 1999; Okeahialam, 1984). The problem is exacerbated by poverty, lack of education and employment opportunities, as well as absent or weak legal frameworks for action against perpetrators (Bowman and Brundige, 2014; Secker, 2013). Looked after children, that is those cared for or raised by non-biological parents in foster care or residential homes, are particularly vulnerable, socially and developmentally (Tarren-Sweeney and Vetere, 2013). Such children will have already experienced a lack of parental care due to their parents being dead, mentally or physically ill, disabled or unwilling to care for them (Eloundou–Enyegue and Stokes, 2002). This potential for maltreatment suggests the possibility of further long-lasting damage to their psychosocial development.
The quality of caregiving relationships in foster and residential homes is often deficient as some caregivers are insensitive in their interactions with the children (Hermenau, et al., 2015). In addition, the quality of the relationships and the attachments between caregivers and children can significantly affect children’s experience of harmful situations. Studies have shown that a positive and open relationship with child care providers serves as an important protective factor for young children (Joseph and Strain, 2004). Secure attachments are conducive to healthy child development and abuse and neglect are more likely when these attachments are weak. For example, Alexander (1992) found that the consequences of insecure parent–child attachments were various – rejection, role reversal and fear or unresolved trauma – and that these characteristics were frequently found in the dynamics of families characterised by sexual abuse.
Currently, there is limited empirical data from developing societies on the implications of attachment theory, particularly among older children, with respect to caregivers’ relationships and how they relate to children’s experiences of the care they receive.
Rules guiding child placement differ from country to country but, generally, at the core of those regulations is the well-being of the child. In Nigeria, for example, in addition to the formal structures for child adoption and placement in substitute care, kinship relationships are informally appropriated by extended family networks to ‘foster’ or give away for ‘fosterage’ within the kinship structure and even across family boundaries (Isiugo-Abanihe, 1985). Poor relatives often get more well-to-do family members, who often reside in cities, to care for their children, while richer relatives utilise the same familial dynamics to get young people to live with them. Sometimes, these fostered children assume the role of domestic workers and, in exchange, are provided with education and apprenticeships (Case, Paxson and Ableidinger, 2004). Other reasons may be the death of biological parents who could or could not have had a filial relationship with the family now assuming the caring duties. This system, though informal, is almost ubiquitous in Nigeria and other West African countries (Isiugo-Abanihe, 1985) and has been credited with a significant level of success. In terms of placement in residential care, there is also an informal mechanism (quite distinct from the formal process) through which children are admitted into establishments. In many cases, philanthropic individuals or organisations, such as the church, set up children’s homes and admit orphaned and abandoned children at the discretion of the homeowners. In these processes, there is an absence of any formal and standardised assessment of the child’s needs; instead, emphasis is placed on what the adult family members and homeowners consider to be right for the child. Also lacking is a mechanism for monitoring outcomes for the children.
The current study compares the quality of caregiver–child relationships in two types of child care settings – foster and residential care – and explores its significance for the prevalence of abuse.
Methods
This study scrutinised 314 children aged 7–17 years living in foster and residential care in Ibadan, Nigeria. From a list of all 28 registered child care establishments in the city at the time of the study (obtained from the Oyo State Ministry of Women's Affairs and Social Development, and the Department of Child Welfare), seven homes were randomly selected and all children (n = 157) who met the age range and other criteria described below were included. The selection of fostered children was carried out from public secondary and primary schools in Ibadan through a two-step process. This involved a random selection of secondary and primary schools from five local government areas out of the 11 in Ibadan and then identified the children in foster care enrolled in those schools, 157 in all (79 secondary and 78 primary).
Caregiver–child relationships were measured using the Positive Relationship Scale (PerformWell, 2015). The instrument is a six-item scale which measures children's relationships with their primary caregivers (whether a foster parent or biological parent/family member or someone affiliated with their residential home care provider). Each item in the scale has a five-point Likert score with numeric values from nought to four, giving a maximum score of 24. Higher scores imply better positive relationships. The internal reliability of the instrument among the population in the foster care setting was high (Cronbach alpha = 0.849) but slightly lower for the residential population (Cronbach alpha = 0.768). Child abuse was measured by asking the children about the kinds of abuse they had experienced. There were eight questions covering physical, sexual and emotional abuse. A score of nought was given when a child had never experienced any abuse and a score of one was given when any mention was reported. Child abuse variables were then aggregated into a single measure. Other variables perceived as potentially influential, such as the socio-demographic characteristics of the children and the duration of the child’s stay in foster or residential care, were then added to the analysis.
Children were included in the study on the basis that they were apparently healthy with no learning difficulties. Ethical approval was obtained from the University of Ibadan/University College Hospital Ibadan Institutional Review Committee (IRC) and permission was obtained from the principals of the selected schools. Informed consent was obtained from foster carers and heads of the residential homes. In addition, each child gave assent after the purpose of the research was explained to him or her prior to enrolment.
Data entry and analysis were performed using the IBM SPSS version 20 and descriptive analysis was used to present all the variables. T-tests were employed to explore the differences in child abuse scores between the two types of care settings and the Mann Whitney U test was used to examine the difference in positive relationships when the data failed to meet the requirements for parametric statistical methods. In addition, the association between the presence of positive relationships and child abuse was further explored by multivariate analysis that measured the impact of independent factors on the child abuse identified. Statistical significance for all analyses was set at p < 0.05.
Results
Socio-demographic characteristics of the children.

Comparison of positive relationships between children in foster and residential care.

Comparison of child abuse between children in foster and residential care.

Bivariate test for factors related with child abuse between children in foster and residential care.

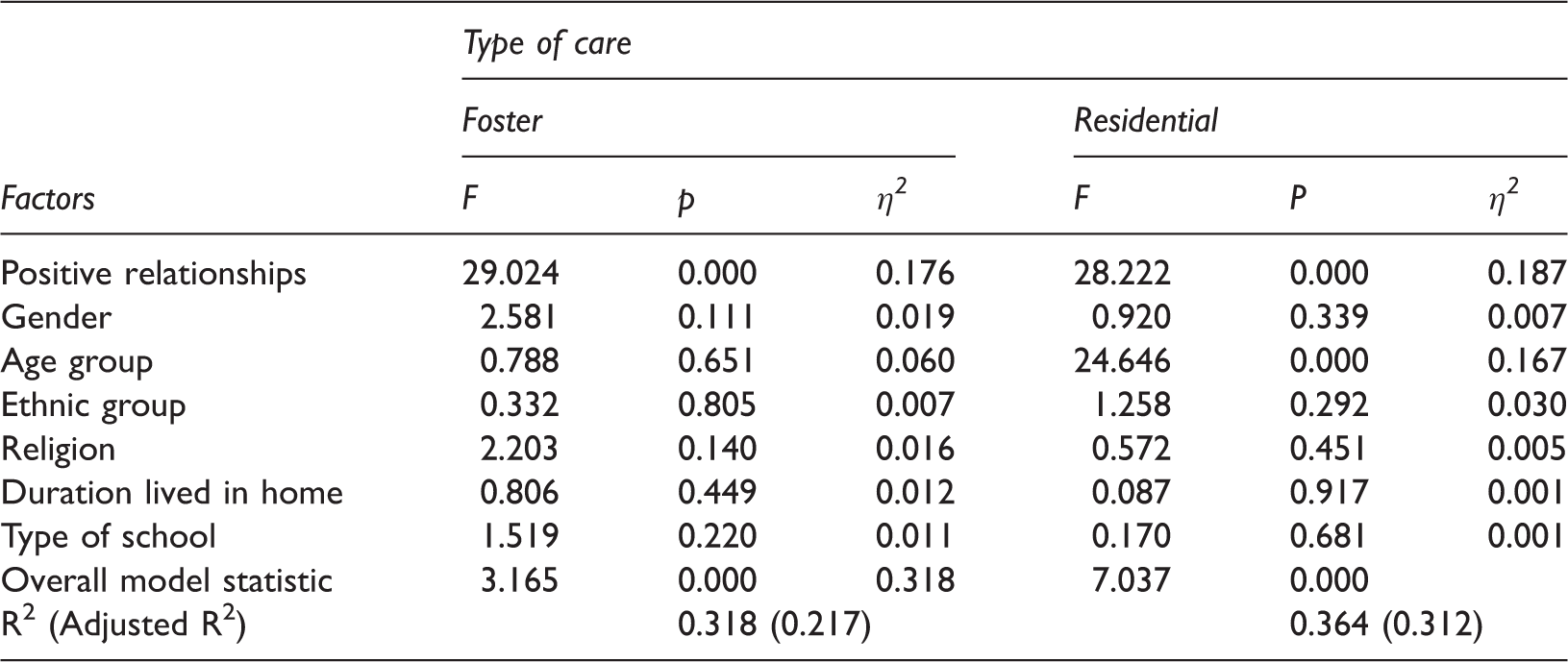
ANCOVA for factors related with child abuse for children in foster and residential care with positive relationship as a covariate.
Discussion
The aim of this study was to compare the quality of caregiver–child relationships and its impact on child abuse among children living in foster and residential homes in Nigeria. A key finding from the study is that the quality of caregiver–child relationships is apparently better in residential care than in foster homes. This finding contradicts much that is reported in the literature on different types of care, which generally concludes that children living in foster care have better social well-being and are more satisfied with their experience than those placed residentially (Nelson, et al., 2007; Rosas and McCall, 2009; Wilson and Conroy, 1999). Consequently, practitioners (even non-Africans) in Western countries often rely on the African family-centred social reality to assign children (those of African origin for non-African practitioners) to kinship-based foster care.
Yet, this is not an exceptional finding as Akeju (2015) found that foster children feel a lesser sense of belonging when their foster carers have their own children living in the home. Thus, it is likely that if foster children perceive that they are not receiving equivalent love, care and support as the carers’ own children, their relationship with caregivers will become strained (Baer and Martinez 2006; Tarren-Sweeney, 2013). Also, foster carers who have their own children living with them may tend to treat them more favourably and the animosity generated by this can be enormous, leading to deterioration in the carer–child relationship. The children in residential care, in contrast, will not have had this experience. In addition, there is a cultural tradition in Nigeria that if someone is a success or a failure, people always ask, ‘Whose child is that?’, not ‘Who raised that child?’. This might explain why some foster carers may not be fully committed to the care, love and support of the children who live with them. Moreover, some children who are fostered often function as domestic workers who perform all the household chores. This makes fractious relationships more likely.
The better relationships with caregivers found among children in residential care can also be attributed to the fact that staff in the homes are guided by rules and are expected to have an open and trustful relationship with those whom they look after. These rules are provided in the code of conduct for caregivers enshrined in the guidelines for protection of children in formal care in Nigeria (NAPTIP, 2009). The policy, which is mandatory for all formal child care providers, offers effective protection for children. In addition, residential staff are more likely to be trained in child care and this may influence their responsiveness and the quality of their interactions. On the other hand, when care is arranged informally there is a lack of monitoring and an increased risk of maltreatment. Thus, there is a need to establish the cultural sensitivity that will ensure good practice in these situations as informal foster care is often preferred to promote continuing contact with the birth family, if this is deemed to be desirable (Roby, 2011). Conversely, the results of the research indicate that child abuse occurs wherever children are placed – in residential care, foster homes or with relatives – and in formal as well as informal settings. The findings also support the notion that open relationships between caregiver and child serve as an important protective factor for young children. The environment that is created is auspicious for the bonding that underpins safe and secure relationships.
The evidence from this study on the significant impact of positive relationships reducing the risk of abuse for children in two different care settings provides valuable information for welfare organisations as it shows that maltreatment by caregivers can be reduced by promoting positive and healthy caregiver–child relationships, and by taking account of the significant factors highlighted in the research. There is a constant debate in the western social work literature over which type of care ensures the best outcomes for children. A review of the evidence in support of residential child placement in the UK by Clough, Bullock and Ward (2006) concluded that there can be no list of circumstances where residential care should automatically be the preferred choice; it is helpful in certain situations, such as when a child prefers it to any kind of family arrangements or when they have abused other children. By implication, therefore, foster care with family arrangements are usually the preferred option. Similarly, in most African settings, because of the importance placed on familial linkages, family and kinship care are usually the first consideration before residential care and even for practitioners in non-African settings, the common practice has been to place children of African origins in kinship foster care (Vecchiato, et al., 2013).
Although this study is specific to Nigeria, international migration means that social workers and carers in many European countries, North America and Australasia have to deal with an increasing number of children from West Africa. As stated earlier, in the UK 4% of children and young people in care at any one time and 6% of annual admissions are of African heritage and these figures are almost certainly higher in cities (Hayden and Jenkins, 2015). Whereas children of ‘African origin’ is a broad term, there is a substantial risk that when assessing these children's needs, British social workers may make unjustified assumptions, such as that past residential care has automatically been bad while foster care has always been good, whereas this might not be the case. Hence, social workers may miss some negative experiences in foster care and ignore some positive ones in residential settings.
The study has a number of limitations. The measures of abuse and of care provider–child relationships were all based on self-report. Also, it is uncertain if the positive relationship scale is valid for children as young as seven (the lower age limit in this study) as the scale was originally designed for use with teenagers. Moreover, the sample was relatively small. The method of recruiting foster carers through schools may have biased the sample given that in most cases, children who live outside of their homes have limited access to education. Neither did we examine whether the children in foster care had kinship ties with their carers, which could influence the quality of caregiver–child relationships. Finally, the study did not explore if cultural norms differ from the questions used to evaluate abuse; for example, the use of ‘time out’ may be a cultural norm for disciplining children but may be reported as physical abuse.
Nevertheless, in conclusion, we show that in Nigeria child abuse occurs in residential and foster care but that the quality of caregiver–child relationships is better in residential homes and has a mitigating effect. At the international level, social workers who deal with children of Nigerian heritage or origin (perhaps, West African also) may find these findings useful in understanding the cultural and social context from which those children come.
Footnotes
At the time of the study,