
Abstract
This article discusses the rationale for mindfulness as an intervention in addressing parenting stress in adoptive parents and describes the process of its implementation in a voluntary adoption agency. Burgeoning interest in mindfulness in the public and scientific domains, alongside the presenting needs of adoptive families, has led to an appreciation of this intervention to meet the particular needs of adoptive parents and their children. The theoretical and research grounds for it are outlined before a description of the service is provided and supplemented with data from staff and parent groups receiving Mindfulness Based Cognitive Therapy (MBCT). In the manner of ‘practice what you preach’, staff as well as adoptive parents participated in the training. Adoptive parents demonstrated improvements in mindfulness and compassion; staff showed positive changes in self-compassion. There were also improvements in parenting stress for adopters. These results suggest this was a promising intervention for both the families and the agency and indicate an ongoing commitment to using it alongside other treatments. Further pointers to future service delivery, implementation and research are outlined.
Keywords
Introduction
Service context and development
Adoptionplus is an English voluntary adoption agency which, in addition to providing adoptive placements, offers psychological, neurodevelopmental and paediatric occupational therapy assessment, Dyadic Developmental Psychotherapy and Theraplay. In seeking to offer interventions informed by research rationales, this article describes the process of using a well-described and widely used intervention, Mindfulness Based Cognitive Therapy (MBCT), to address a key element of presenting difficulties for adoptive parents: parenting stress.
The rationale
Research has consistently reported on the increased challenges and stress experienced by adoptive families (e.g. McKay and Ross, 2009), and among the parent population, adoptive parents may be a particularly vulnerable group. In a UK survey using a psychometric measure of parenting stress, Harris-Waller, Granger and Gurney-Smith (2016) found higher rates of parenting stress for adoptive compared to non-adoptive parents, to a clinically significant degree. For example, 70% scored within the ‘very high’ category for stress and had lower levels of mental well-being (Glossop, 2013). While interventions for adoptive parents have sought to positively influence the understanding and skills of parents (Rushton and Dance, 2006), there is not necessarily any corresponding improvement in parenting stress. For instance, the Fostering Attachments Group developed by Kim Golding has in some evaluations included established measures of parenting stress. Despite showing positive changes in parenting skills and understanding across a number of studies (Golding and Picken, 2004; Gurney-Smith, et al., 2010; Linares, et al., 2006; Rushton, et al., 2010), only one has shown positive changes in parenting stress (Laybourne, Andersen and Sands, 2008). Given the significance of such stress on outcomes for parent–child relationships, these findings highlight that in the field of adoption, the need for an intervention that not only helps parents ‘think differently’ but also ‘feel better’ may meet a potential gap in the provision of comprehensive adoption support.
Mindfulness, parenting stress and adoption
On top of the day-to-day demands of adoptive parenting, the nature of domestic adoption in the UK, often featuring older children with longer care histories, may increase the likelihood of adoptive parents developing stress (Barratt, 2009; Bird, Peterson and Hotta Miller, 2002; Mainemer, Gilman and Ames, 1998). This profile is characteristic of the children referred to Adoptionplus. More recent investigations demonstrate strong relationships between the degree of child-related difficulties, including externalising problems and attachment-related issues, and the level of parenting stress experienced by adopters (Glossop, 2013; Harris-Waller, Granger and Gurney-Smith, 2016). Additional diagnoses such as foetal alcohol spectrum disorders (Phillips, 2015) and post-adoption depression (Payne, et al., 2010) can be a further source of stress and demands. Exposure to sustained difficulties of emotions, behaviour and attachment in their child may lead to ‘blocked care’ for adoptive parents. This refers to a model developed by Hughes and Baylin (2012) whereby the capacity to have rewarding, engaged, open and co-regulating relationships is compromised at a psychological and neurobiological level. In seeking to develop practice that would assist with these presenting difficulties directly, Adoptionplus set out to consider interventions with an evidence base that might promote well-being and address stress symptoms in adoptive parents.
There is widespread interest in mindfulness in both the public and scientific domains, yet very little of what is described applies to adopters. Nevertheless, mindfulness interventions such as MBCT (Segal, Williams and Teasdale, 2013) have been shown to be consistently effective in reducing symptoms in specific populations affected by stress, depression and anxiety (Grossman, et al., 2004; Hofmann, et al., 2010; Williams and Penman, 2011). Furthermore, there is evidence of parent populations showing changes in both parent and child variables (Harnett and Dawe, 2012). As an intervention, MBCT does not require there to be a ‘problem’ in order to be effective; depending on the individual circumstances, it thereby offers a preventive and health-giving intervention or ‘treatment’. In these respects, the rationale for adoptive parents referred for help was considered promising.
Mindfulness is described as deliberately focusing attention on feelings, thoughts and bodily experiences in the present moment, with an attitude of non-judgement and acceptance (Kabat-Zinn, 1990). It also has been extended into the parenting domain by the term ‘mindful parenting’ (Hughes and Baylin, 2012) – that is parenting characterised by lowered stress, rewarding interactions, an ability to read the underlying needs of the child and a capacity to remain close and to be aware and resolved about the meaning of the relationship. In the mindfulness literature, the model of mindful parenting described by Duncan, Coatsworth and Greenberg (2009) has been operationally defined by behaviours such as a sensitivity to the child’s cues, a non-judgemental acceptance of the self and child, with greater compassion for both, and better self-regulation of immediate emotional states in favour of longer-term goals that sustain the relationship. The theoretical concept of blocked care referred to above offers some justification for not only helping parents with their stress but also cultivating a stance of openness and engagement with their children. Mindfulness may help parents to accept difficulties (including their own) as they are, reduce stress and change relationships while improving the capacity for choice rather than the reactive behaviours seen in blocked care. This may also be associated with more distal outcomes such as placement stability. Within their model of mindful parenting, Duncan and colleagues also identified the role of compassion, defined by Gilbert (2005:1) as ‘being open to the suffering of self and others in a non-defensive and non-judgemental way’. Our own research demonstrated that levels of mindfulness in adoptive parents were closely related to lower levels of parenting stress (Glossop, 2013; Gurney-Smith, Glossop and Granger, submitted). Although we did not find the same for self-compassion, there was a trend in this direction.
On the basis of these theoretical foundations and research findings, Adoptionplus sought to determine if MBCT might offer some promise to adoptive parents who are vulnerable to experiencing stress.
Implementing mindfulness in the agency
A service proposal was written, highlighting the rationale on the theoretical grounds outlined above, on the basis of need in a vulnerable population and the wish to innovate in the field of adoption support. The proposal sought to employ a fully qualified mindfulness practitioner to deliver MBCT one day a week. We did not wish to change the programme of MBCT given its impressive evidence base but simply to present to potential participants the reasons why it may be helpful. Hence, we prepared an information sheet to explain the elements of mindful parenting and how the intervention might help with parenting stress. A commitment to evaluating the group was made to ascertain whether this intervention was helpful and to inform decisions on whether it would continue to be offered longer term within the service. In order to practice what we preached and embed mindfulness as an intervention within the service, we educated staff who would be working with families who might require or had received mindfulness training and offered MBCT to all the therapists in Adoptionplus. Aside from this principle, we recognised the well-documented risk of ‘compassion fatigue’ among therapists (Weiss, 2004) and that a mindfulness-based stress reduction programme had been found to be helpful in this regard (e.g. Shapiro, Brown and Biegel, 2007).
The course we delivered, as described in this article, follows the eight-session manualised intervention provided over as many weeks, minus the day of silent practice, described in Segal, Williams and Teasdale (2013). This is briefly outlined below.
The first four sessions help teach participants the basics of mindfulness: developing awareness of body sensations and the activity of the mind. Bringing the mind back to a single focus is a skill learned through repeated practice and doing it every day at home is actively encouraged. The fourth session focuses on how mind wandering can allow negative thoughts and feelings to escalate, and when such lack of awareness can lead to reactive responses. Sessions five to eight move on to how to relate to negative thoughts and feelings by accepting their presence. The penultimate session encourages awareness of warning signs of unhelpful stress levels and identifies strategies and specific actions for the individual to improve well-being. The required skills and knowledge can only be acquired through direct experience and an enquiry after each mindfulness practice facilitates greater reflection on this. The whole MBCT course is underpinned by an attitude of compassion, modelled by the facilitator in the practice guidance, where acceptance of mental activity and body sensations, just as they are, is encouraged.
We now report on the delivery of two groups of MBCT at Adoptionplus, first with staff and second, with adoptive parents.
Method
MBCT for staff and parents
Eleven members (eight female, three male) of the therapy team attended a dedicated staff group. At a separate time, once recruited, mindfulness was also delivered to 17 adoptive parents (six adoptive fathers and 11 adoptive mothers). The parents were invited to take part and recruited based on an assessment of their family’s needs, or for prospective adopters, during their preparation training once they had been approved but were awaiting a match. All participants, including staff, consented to the use of their questionnaire data for publication. For both groups, widely used measures were completed to determine mindfulness and self-compassion before and after MBCT, and for adoptive parents, an established measure of parenting stress was also taken. These three measures are listed below.
Mindfulness
Mindfulness Attention Awareness Scale (MAAS) (Brown and Ryan, 2003). The MAAS is a 15-item questionnaire using a six-point Likert scale assessing mindfulness in relation to attention and awareness of the present moment. This scale is scored by averaging scores across all 15 items on the questionnaire, leading to a range of scores between 0 and 5.
Self-Compassion
The Self-Compassion Scale-Short Form (SCS-SF) (Raes, 2010) is the shortened version of the Self-Compassion Scale (Neff, 2003). It comprises a 12-item questionnaire, using a five-point Likert scale that measures six components of self-compassion – self-kindness, self-judgement, common humanity, isolation, mindfulness and over-identification – and provides a total self-compassion score.
Parenting Stress
The Parenting Stress Index/Short-Form-Fourth Edition (PSI/SF) (Abidin, 2012) is the short version of the Parenting Stress Index (Abidin, 1983) comprising 36 items over three subscales: Difficult Child, Parent–Child Dysfunctional Interaction and Parental Distress.
Results
MBCT for staff
Mindfulness and self-compassion for staff (n = 11).
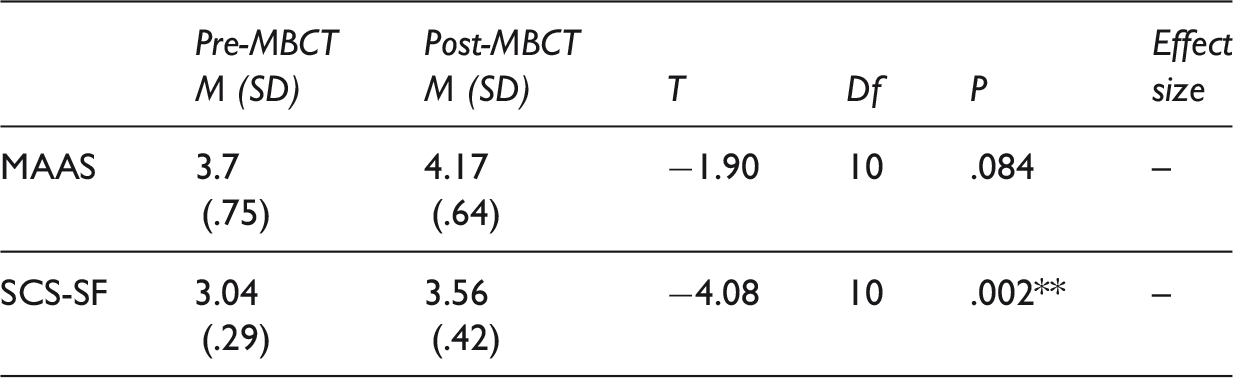
Note: * = p < .05, ** = p < .01. SD appear in parentheses below means.
A statistical analysis was then employed to assess whether there were ‘before and after’ changes. Using t-tests, for the staff group the mean total score for mindfulness (MAAS) increased by 0.47 from pre-training (M = 3.7, SD = .75) to post-training (M = 4.17, SD = .64); (t(10) = −1.90, p = .084), but this was not statistically significant. The mean total for compassion (SCS-SF) increased by 0.61 between pre-training (M = 3.04, SD = .29) and post-training (M = 3.56, SD = .42) and was significant (t(10) = −4.08, p < .01). These results with staff were seen as promising and gave further confidence to the agency in using MBCT with adoptive parents.
MBCT for adoptive parents
Mindfulness and self-compassion in adoptive parents (n = 17).
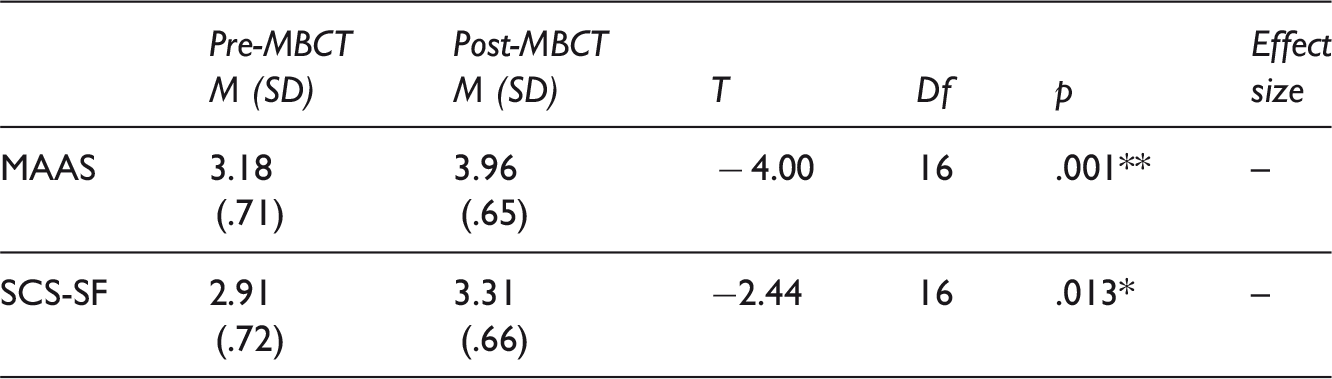
Note: * = p < .05, ** = p < .01. SD appear in parentheses below means.
Parenting stress (n = 7).
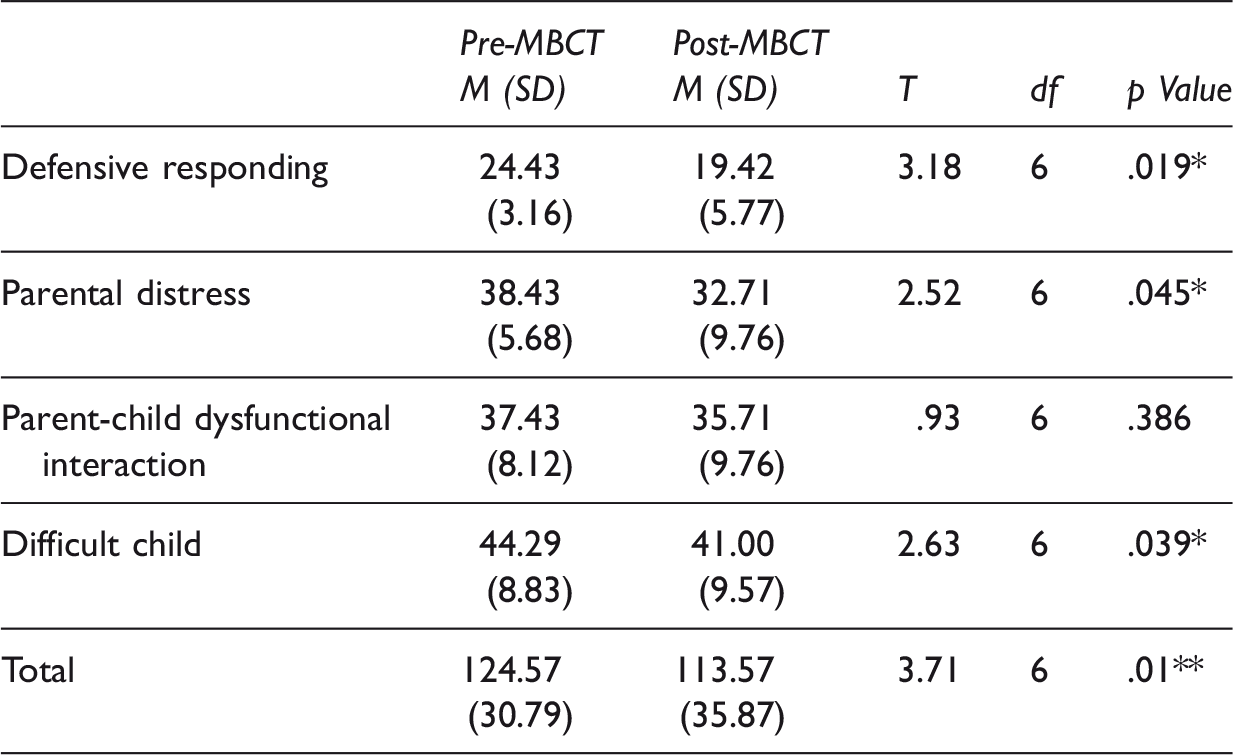
Note: * = p < .05, ** = p < .01. SD appear in parentheses below means.
Discussion
This article has described the rationale, development and a ‘before and after’ evaluation of MBCT for adoptive parents and therapy staff in a voluntary adoption agency. The decision to evaluate the groups was seen as critical to the development of the service within the agency but also of potential interest to the wider literature in seeking to assist parenting stress in adoptive parents and to share the practice of service development of a new intervention. The evaluation in and of itself is limited by the small numbers involved and the absence of a control group. Future research seeking to be definitive about the effectiveness of MBCT would tackle this question quite differently (e.g. by using a control group) and although the results are of interest, this was not the prime intention of this article. Nevertheless, at a service level, the results gave enough confidence to the agency to see MBCT as a viable, ongoing therapeutic intervention alongside others, such as Dyadic Developmental Psychotherapy, under the umbrella of ‘adoption support’. Based on these findings, a decision was made by the Board at Adoptionplus to continue offering MBCT for parents, and we intend to monitor the effectiveness and report on this with greater confidence as the numbers of participants grow. Indeed, we intend to continue to collate data on an ongoing basis in this way and the use of longer-term follow-up data may allow a better method of tracking changes, particularly when parents are faced with attachment-related difficulties that tend to have a chronic course. We did not complete full demographic data on the participants as this was not an evaluation study and given the early stages of this research, we would see fuller reporting in this way as being helpful for interpreting these preliminary findings in context. Further research to gain the qualitative experience of participants’ adoption support would also help determine the extent of its validity for parents.
It was promising to find that MBCT had the expected positive effects on self-compassion for therapy staff consistent with those reported for other therapists (Shapiro, Brown and Biegel, 2007). However, the effect of MBCT on mindfulness scores was insignificant. This may be due to staff having scored relatively highly on the mindfulness measure at baseline or to the possibility that some staff members had previous experience of mindfulness. Given that the mean mindfulness score for staff was higher post-intervention, and the significant positive effect of MBCT on self-compassion, these data suggest that MBCT may produce some benefits for staff. Since completing this exercise, new staff are now offered this programme; also short mindfulness exercises have been used prior to team supervisions to give staff the opportunity to be aware of anything influencing their capacity to make observations (i.e. to be present) about their work. This also recognises the importance of a culture in the agency whereby ‘well-being’ is important to staff and families alike. Maintaining this approach requires ‘buy in’ from the service at all levels and the use of formal measures, although requiring resources to collate and analyse, helps to ensure that the benefits can be made tangible if staff are to take time away from families.
For prospective and adoptive parents, we saw improvements in mindful attention and awareness and self-compassion. This finding only supports the wide application and acceptability of MBCT across groups but at a service level meant that it was flexible and wide-reaching as well as effective. Additionally, for adoptive parents, we saw improvements in parenting stress overall. Despite tentative evidence that parenting stress reduced, we were aware that it still remained within the high range. Knowing whether this led to a functional difference, for example in parenting behaviour, would be of interest and would need further testing. Qualitative research would assist with understanding mechanisms of change and how this may relate to the task of adoptive parenting or preparing prospective parents for this important change.
In finding an effective and cost-efficient intervention for parenting stress, MBCT benefits from being group based and widely available. Mindfulness may enable greater awareness and positive change in parents before addressing difficulties originating in their child and so inform what therapies are needed next. This particularly may be the case for interventions like Dyadic Developmental Psychotherapy (Hughes, 2009) or Theraplay (Booth and Jernberg, 2009), which encourage openness to the attachment relationship. It could be a way of addressing cases of blocked care that can blindsight practitioners or lead to ineffective child-centred treatments rather than helping to reduce a significant factor in parenting capacity so common in adoption due to the nature of the children’s difficulties (Harris-Waller, Granger and Gurney-Smith, 2016). It would be interesting to see whether MBCT assists with all origins of blocked care, be these childhood in origin or due to child-specific factors. It is now being offered in this way at Adoptionplus where parenting stress is high as a precursor to other treatments where that is seen as clinically appropriate.
Understanding parenting stress in adoption over an extended period of time requires greater research attention to be paid to its probable role in the risk of family breakdown and quality of parenting. In this way, as mindfulness is essentially a health enhancing and potentially symptom reducing intervention, it is flexible across the entire adoption process from assessment to post-placement support. It is of key interest to Adoptionplus as an adoption agency that uses evidence-based approaches to identify the resilient and reflective parents who are probably required of the later placed adoptions that are characteristic of those made by the agency (Golding and Gurney-Smith, 2015). Such measures of the potential for resilience, as in the capacity to regulate stress in oneself as a parent and distress in one’s children, may be informed by an understanding of compassion and mindful awareness as defined and measured using the questionnaires in this study. Taking this further to preparation training, it may also be possible that reported changes at a neurobiological level in the literature, including lowered amygdala firing (Desbordes, et al., 2012), may make mindfulness a deeply preparative tool for prospective adoptive parents. This may have some validity as preparation groups can only really provide an off-line understanding of the parenting task as there is no child present, whereas mindfulness has the capacity to help develop and practise the stance required even before a child is placed. More research would be needed to justify this approach, particularly using longitudinal methodology to determine if mindfulness as a preparatory course leads to different parent and child outcomes.
Developing innovation in adoption requires governance, an understanding of how to apply evidence from other populations and additional resources of time and expertise in evaluation supported from across the service and organisation. This was the case here. From an initial research study examining parenting stress (Harris-Waller, 2012) to an exploratory study of the role of mindfulness (Glossop, 2013) supervised by the lead author of this article, a staged approach to the application of a new treatment to a new population was rationalised. This process takes time and may be at odds with the pressing needs of the population being investigated. The agency has a positive view of research and a learning culture, so time was permitted and allowed to ensure this could be achieved. The requirement to monitor effectiveness was conducted here to inform whether this approach worked for families and the agency. Done reasonably well, it also may add in a modest way to the development of the evidence base in adoption support that is generally limited and lacking at present. This will take time and steady evaluation. For Adoptionplus, MBCT demonstrated enough promise in targeting stress and mindfulness to the extent that it is now part of an array of interventions within the agency. More broadly, with such a strong evidence base in other populations, MBCT offers much potential promise to the world of adoption support as there has been a gap in provision to date. As such, it is worthy of consideration alongside other interventions for adoptive families where parenting stress is found to be high.
Footnotes
Acknowledgements
The authors would like to thank all the participants for their agreement to use their questionnaire data in this study.