
Abstract
As foster and kinship carers are central to the lives of looked after children, it is important to recognise their unmet needs and the impact of these on the caring task. This article explores these issues by applying a hierarchy of needs to the foster and kinship care context, drawing on the perspectives of those involved. A group of Australian foster carers (n = 52) and kinship carers (n = 16) were interviewed using the CUES-C, a 13-item questionnaire that collects both qualitative and quantitative responses with regard to carers’ perceived needs and satisfaction. Thematic analysis was undertaken and participant responses were coded and organised according to the updated hierarchy of human motives proposed by Kenrick and colleagues (2010), based on Maslow’s (1943) widely used hierarchy of needs. The findings support Lyubomirsky and Boehm’s (2010) conclusion that parenting may interfere with the capacity to meet our other human needs and so has significant implications for the form of intensive parenting practised by foster and kinship carers. It was found that without the provision of timely and holistic supports and intervention, the two-way relationship between the needs of looked after children and their carers may create a feedback loop where stress and trauma can be endlessly amplified, to the detriment of both parties. The evidence highlights the importance of addressing both the needs of carers and those of the young people they look after, and suggests some basic improvements that could ease the burden of care and simultaneously increase satisfaction in the caring role.
Introduction
Foster and kinship care are the most important forms of out-of-home care in most economically developed countries. It is also well established that the children concerned will be more likely to have complex needs related to their behavioural difficulties, emotional and mental ill-health than most other children in society (Milburn, Lynch and Jackson, 2008). But it is also the case that their carers will have needs of their own that must be met in order for them to survive and it is this side of the equation that this study seeks to explore.
In this article, foster care is understood as the temporary care of children whose parents are unable or unwilling to look after them by accredited voluntary carers, while kinship care is provided by relatives or a member of a child or young person’s social network. In Victoria, Australia, it is a legislative requirement that options for placing a child in kinship care be thoroughly explored before other placement options (Department of Health and Human Services, 2017). This may be formal, mandated by a court, or an informal, private arrangement. Foster carers and statutory kinship carers are eligible to receive a modest allowance towards covering the cost of providing care. Informal kinship carers are not.
A growing body of research indicates that the well-being of foster and kinship carers plays an important role in social, emotional and behavioural outcomes for young people in care, with depression among carers particularly linked to poorer outcomes for children (Garcia, et al., 2015). Statutory care services have been shown to fail in properly recognising the importance of carers, with an inadequate focus on attachment and placement stability and the significant barriers to gaining access to supporting services (York and Jones, 2017). Given the critical role played by carers in achieving positive outcomes for looked after children, this article seeks to explore the concept of need in the context of the carer household and in so doing, understand the relationship between the needs of carers and their capacity to meet the needs of looked after children. Drawing on the perspectives of carers, two key questions are addressed:
What unmet needs do foster and kinship carers experience? How do these unmet needs impact on their caregiving role?
These questions are explored by analysing the perceived needs and satisfaction of carers through the use of the Carers’ and Users’ Expectation of Services-Carer (CUES-C) questionnaire and considering the results in the context of human needs theory. Questions were adapted to a minimal degree to acknowledge the unique relationship between these carers and the children they look after. We believe it may be the first time the CUES-C has been used specifically with foster and kinship carers.
Needs theory
The American psychologist Maslow (1943) identified five sets of basic needs which he set out in hierarchical order (see Figure 1). They include physical and non-physical elements and goals which humans are innately driven to attain in order to sustain their growth and development as people. He posited that when the most fundamental goal or need is realised, the next most pressing one emerges, and so on, potentially leading to self-actualisation and fulfilment. His theory was criticised for its lack of empirical support (Wahba and Bridwell, 1976) and for perceived cultural bias (Hofstede, 1984). Hofstede, for example, argued that placing self-actualisation needs above broader social needs reflected an individualistic, western values system which was not universally applicable. These concerns were later addressed in a 123-country study which largely validated the needs described in Maslow’s original theory, although it suggested a less hierarchical organisation than Maslow had originally described (Tay and Diener, 2011).
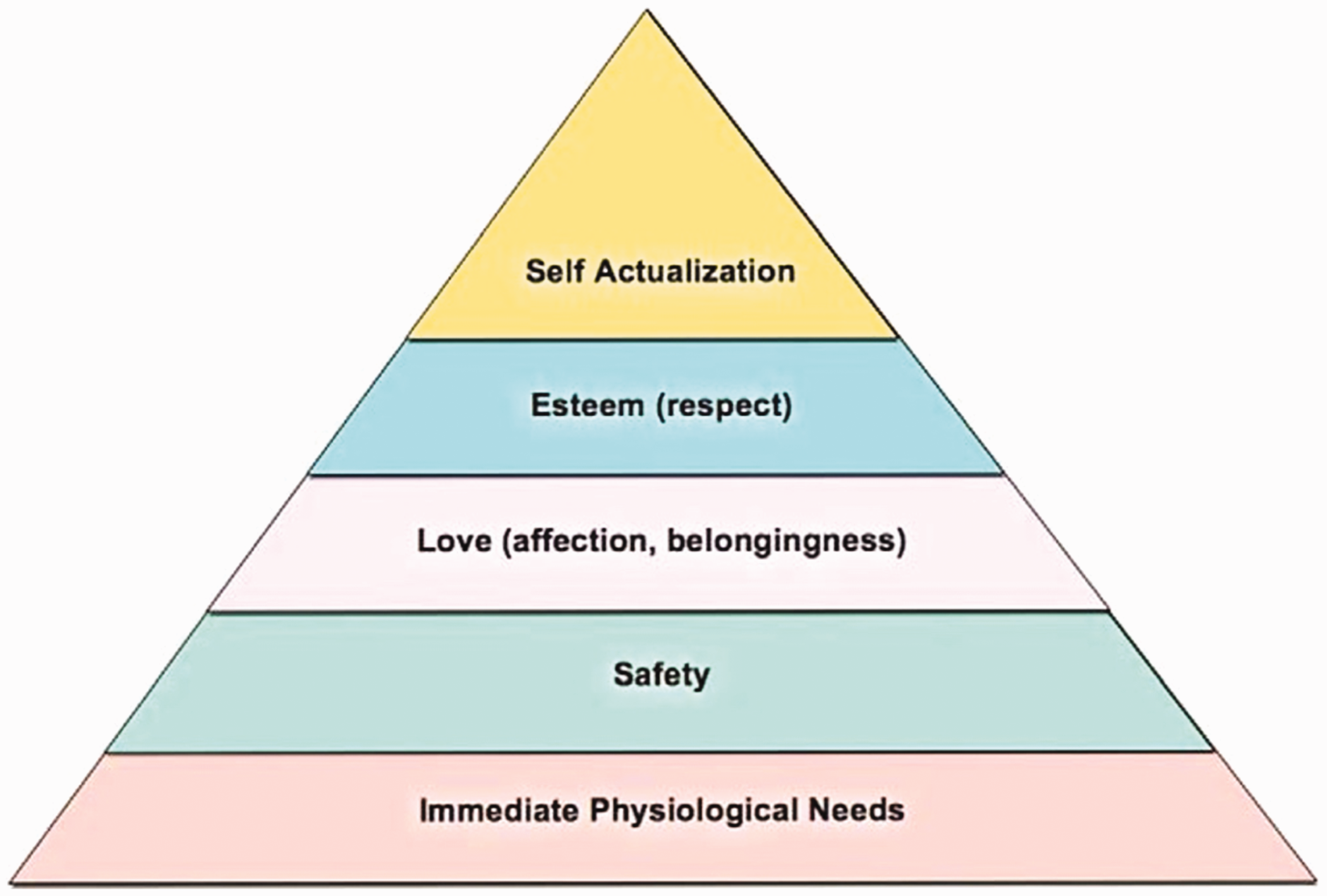
Maslow’s classic hierarchy of needs.
In 2010, Kenrick and colleagues revised Maslow’s theory, placing an emphasis on parenting and reproduction due to consideration of the biological framework of life-history theory. They posited that although self-actualisation may be of ‘considerable psychological importance’, it does not represent a functionally distinct human need. Their revised pyramid subsumed self-actualisation within the status/esteem level, with mating-related motives moved to the top of the new pyramid and comprising three types of reproductive goals: mate acquisition, mate retention and parenting (see Figure 2).
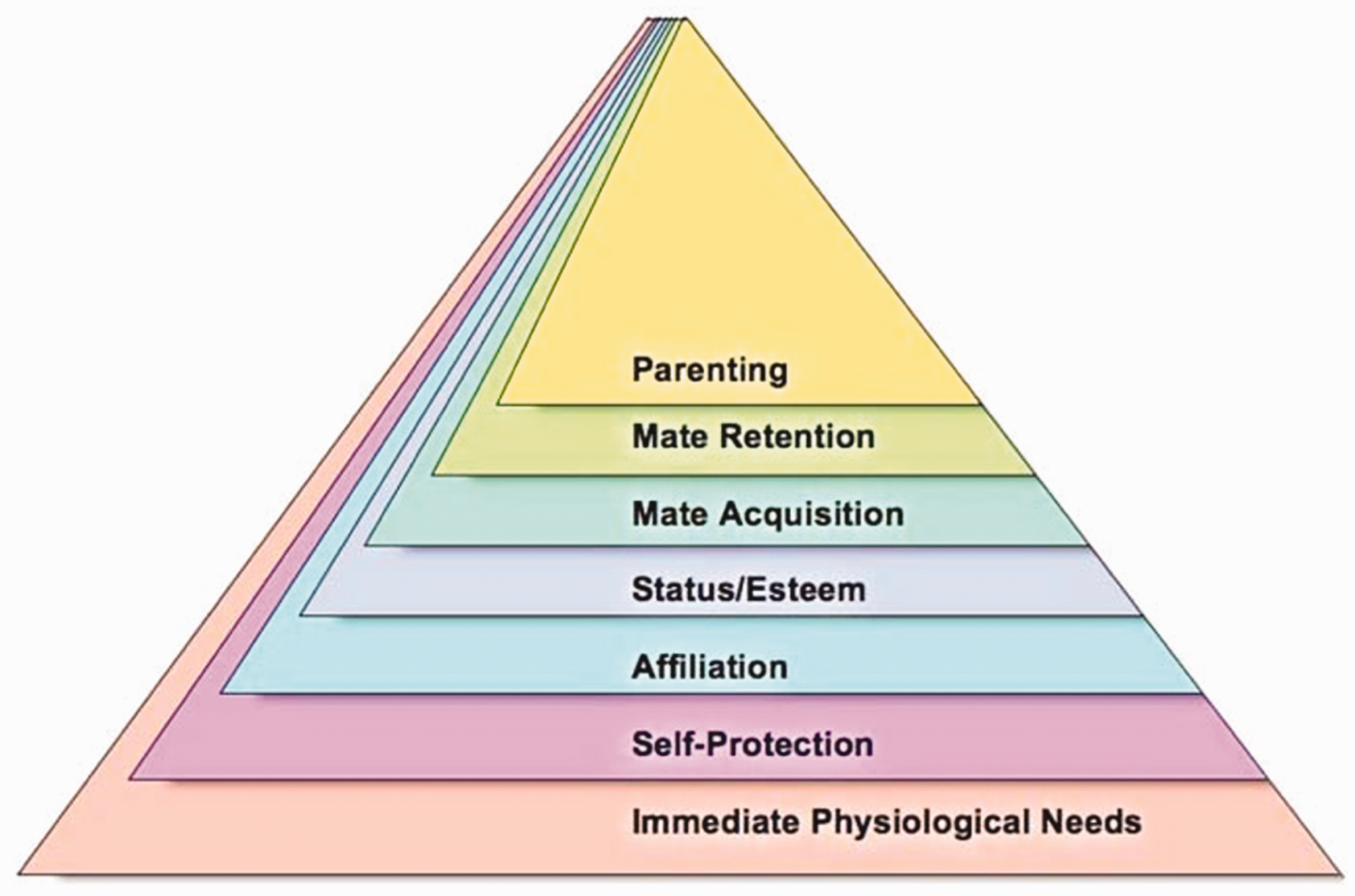
Kenrick and colleagues’ updated hierarchy of needs (2010).
Kenrick’s hierarchy assumes that parenting is more complex than the state of simply being or becoming a biological parent and involves supporting the physical, emotional, social and intellectual development of children (Brooks, 2012). Hence, it is broader than a heteronormative view of ‘traditional’ or nuclear family’ parenting. Kenrick and colleagues (2010) argue that human beings have a need to parent. For some people, this may mean practising parenting through caring for extended family, mentoring, teaching or fostering, but all adults, regardless of gender or sexuality, will experience this need in some form (Kenrick, et al., 2010). However, Lyubomirsky and Boehm (2010) are more sceptical and argue that while happiness in humans has been shown to stem from our needs being met, parenthood has also been associated with decrements in well-being. They posited that parenting may interfere with our capacity to meet lower level need, although short-term costs are eventually outweighed by long-term benefits (Lyubomirsky and Boehm, 2010). It is unclear, therefore, whether foster and kinship carers receive the same long-term benefits as biological parents.
Over the last 75 years, Maslow’s theory, with the aforementioned revisions and additions, has been applied to a broad range of contexts. These include feminist theory, conflict theory, management theory and even social media use. However, the explicit use of human needs theory in social work literature has only recently become influential (Dover, 2013).
Need in caregiver–child relationships
Parents who are healthy and well have been shown to be more able to effectively meet the needs of children in their care, suggesting an interplay between caregivers’ needs and their capacity to care. For example, depression in parents has been linked to problematic parenting and reduced capacity to respond to children’s needs, which can undermine the child’s development (Cicchetti, Rogosch and Toth, 1998; Lovejoy, et al., 2000). Importantly, a bidirectional relationship has been established between the behaviour of children and parental stress (Neece, Green and Baker, 2012). Children who are not having their needs met may exhibit challenging behaviours which, in turn, impact on parental stress, reducing the carer’s capacity to care, and so on.
In addition to the value of the carer‒child relationship itself, a number of studies have demonstrated that carers often act as powerful drivers of access to services (Fergeus, et al., 2017). Their expertise in understanding the needs of the individual child (Minnis and Del Priore, 2001) makes them important agents of change when it comes to improving the emotional well-being of the child they care for. While the literature confirms a general association between the quality of care provided and the health and well-being of the children (Fergeus, et al., 2017), the importance of foster and kinship carers in creating the conditions critical to positive childhood development tends to be poorly recognised. Consequently, a perspective that combines the hierarchy of needs and the understanding of need in the child‒carer relationship provides a fruitful conceptual framework through which to explore these critical issues.
Method
This endeavour was undertaken as part of the Ripple Project, a five-year National Health and Medical Research Council (NHMRC) funded study of approaches to improving the mental health of looked after children and ethical approval was granted by the University of Melbourne Behavioural and Social Sciences Human Ethics Sub-Committee (Ethics ID: 13406740). The study explores the questions previously posited by applying theories of human need to the context of the carer household, drawing on data gathered for the larger research programme.
An initial decision was made to adopt a broad perspective of the concept of need in relation to the carer household through the use of a combination of inductive and deductive thinking and reasoning, drawing on the expertise and experience of our research team. It was also decided that a mixed-methods design was appropriate as it provides the opportunity for both statistical analysis and in-depth contextual exploration of the issues.
Sixty-eight carers (52 foster carers and 16 kinship carers) were recruited through community service organisations (CSOs) which were partners to the Ripple Project in Melbourne. Eligible carers registered with these CSOs were approached by a caseworker known to them and asked if they would consider taking part in the study. To be eligible, carers had to be actively providing care for one or more children. It proved harder to recruit kinship carers due to the smaller number of such placements administered by CSOs in Victoria. A variety of household structures were represented within the sample, including one- and two-carer households, households including carers’ biological children or looked after children only, and some with multiple generations under one roof.
Carers participated in a structured interview using the CUES-C, a 13-item questionnaire. The CUES-C measures a range of domains to assess carers’ perceived needs and satisfaction (Lelliott, et al., 2003). It has been shown to have satisfactory psychometric properties and high acceptability among carer groups (Harvey, et al., 2008), as well as moderate test-retest reliability (Lelliott, et al., 2003). It has previously been used to identify the unmet needs of carers in the mental health sector (Coker, et al., 2016; Drapalski, Marshall and Seybolt, 2008; McAuliffe, Andriske and Moller, 2009).
Carers were asked a series of questions to which they could respond using a three-point scale. For example, they could answer a question such as ‘To what extent do you have information about the condition of the child in care?’ or ‘To what extent is your relationship with the child in care strained?’ by responding ‘a lot’, ‘a little’ or ‘not at all’. Participants were also asked to rate their perceived level of need using another three-point scale. For example, carers were asked if they would like more information about the condition of the looked after child, and more support in maintaining a good relationship with him or her, and could respond to these questions with ‘yes’, ‘unsure’ or ‘no’. Open-ended responses to each question were also recorded, providing substantial qualitative data under each domain.
Thematic analysis
This study followed the six phases of thematic analysis outlined by Braun and Clarke (2006), including familiarisation with the data, generating initial codes, searching for themes, reviewing themes, defining and naming themes and producing the report. A theme represents a level of patterned response or meaning within the dataset (Braun and Clarke, 2006). Qualitative responses of carers were thematically coded in this manner and organised according to the updated hierarchy of human motives proposed by Kenrick and colleagues (2010), based on Maslow’s (1943) hierarchy of need. Through the process of searching for and reviewing themes, the research team agreed that this framework, representing a holistic view of human need, provided an appropriate basis for analysis.
Sub-themes were based on the strength of engagement among participants, including the number of different carers who articulated a sub-theme, and the number of individual occurrences of the sub-theme across the data. These are detailed in the results section. The interpretation of data and the compilation of themes and sub-themes were discussed and agreed by all authors (Lincoln and Guba, 1985).
Limitations
As previously stated, the data analysed in this study were collected using the CUES-C. These structured interviews had the potential to limit the scope of themes arising from the data, given their focus on specific domains. Interviews were not audio-recorded and the reliance on notes taken by researchers during the interview process may have resulted in loss of nuance in some instances. While the quantitative data provided good descriptive evidence and trends, the cell sizes in different domains, particularly in relation to differences between kinship and foster carers, did not lend themselves to statistical analysis.
Results
Most carers responded to each question in the CUES-C, with the exception of the one regarding participants’ relationship with their spouse. This question was not relevant to a number of participants due to their relationship status. Once the total sample is divided into the responses from kinship and foster carers separately, the numbers are small. However, trends do appear and these are reported where relevant. Thematic groups were formed based on Kenrick and colleagues’ (2010) hierarchy of fundamental human motives: physiological needs, self-protection, affiliation, status/esteem, mate acquisition/retention and parenting. Where appropriate, numbers are provided to indicate the strength of the theme alongside the qualitative data from carers.
Foundational needs (physiological and self-protection)
Physiological needs are the physical requirements for human survival. If they are not met, the body will cease to function properly and will eventually fail. These needs include shelter, food, water, oxygen and sleep (Maslow, 1943). Many participants commented on challenges in meeting their physiological needs, making observations such as ‘Stress weighs heavily on my body. I’m often eating on the run or not eating properly. I’m not taking the time to drink plenty of water’ (Carer 42), and ‘Mental stress is making me lethargic’ (Carer 184). Many spoke about the physiological impacts of stress, including a number of carers who talked about sleep, a key physiological need, and the difficulties they had achieving good quality sleep due to stress and worrying about the needs of a child in their care. In one carer’s words: ‘She is really acting out and it is stressing me out. I think about it a lot at night in bed’ (Carer 222).
The ‘self-protection’ group of needs includes personal security, financial security, health and well-being (Kenrick, et al., 2010; Maslow, 1943). These needs are considered to be among the most basic, second only to fundamental physiological ones. They incorporate foundational needs related to health and security. When asked about these, there were many similarities and some differences in the responses of foster and kinship carers.
The significant emotional and physical impacts of caring were described by many participants. Carers, particularly foster carers, described high levels of stress, exhaustion and a lack of energy. Some mentioned symptoms such as high blood pressure. While some participants related this to specific issues, such as a child ‘acting out’, others attributed this to their caring role overall. Many stated that they did not have enough time to exercise and maintain physical fitness, making remarks such as ‘I don’t have time to go to the gym as regularly as before I took on the caring role’ (Carer 884). The quantitative data supported the open-ended comments from carers. While the sample is small, it is worth noting that only 33% of kinship carers (n = 4) reported feeling as well as they would like emotionally, compared to 63% of foster carers (n = 33). This is supported by a number of studies which have concluded that grandparent carers are more likely to exhibit symptoms of depression, more prone to depression and more likely to remain depressed than foster carers (Garcia, et al., 2015; Poitras, et al., 2017).
The time for self-care and looking after themselves was generally limited for the carers in the sample. A minority, including 20% (n = 3) of kinship carers and 30% (n = 15) of foster carers, felt that they had a lot of time for themselves but in contrast, 40% of kinship carer participants (n = 6) and 16% of foster carers (n = 8) said that they had no such time. Twenty percent of kinship carers (n = 3) and 9% of foster carers (n = 4) said they could not take a break when they wished to. One kinship carer stated that they only got ‘a break’ when they went to work (Carer 565).
A foster carer described the benefit of respite care: Our emotional well-being has improved a lot since having better access to respite so we can take a little bit of time for ourselves. (Carer 275) [Young person] had a psychotic episode…I’d called [agency]. The young person ‘wasn’t a physical danger’ so I was told to call back in the morning. I felt very unsupported. (Carer 314)
Forty-four percent of kinship carers (n = 7) talked of experiencing financial hardship.
For example: …payments don’t cover what it actually costs to look after a child, and you want to give them the best. We’ve had to borrow off family and get loans to pay for everything. (Carer 892)
The trend in the data showed that kinship carers reported more emotional impacts and foster carers more physical impacts deriving from their caring role. Overall, participants recounted significant difficulties in having their ‘self-protection’ needs met.
Affiliation, status and esteem
Maslow’s (1943) third proposed level of human need related to social belonging. Kenrick and colleagues (2010) reclassified this need as ‘affiliation’, arguing that different types of human relationships are worth clearly distinguishing in a hierarchy of motives. The need for affiliation is particularly important given a growing evidence base detailing the health and well-being impacts of loneliness, including findings by Holt-Lunstad, Smith and Layton (2010) that it greatly increases the risk of mortality. Carer 884 was one of many participants who reflected on the need for affiliation, commenting that ‘it would be good to have a community of carers to bounce ideas off and to have as support’. Seventy-five percent of participants (n = 50) reported being able to maintain satisfactory relationships with their family and friends while caring. Others told of significant problems. One stated that their brother had a significant accident a year previously, but that they had been unable to visit him interstate as they were ‘not allowed to take the kids across the border’ (537). Another said, ‘I can’t fix my family at the moment. I will probably regret that one day’ (Carer 565).
Participants spoke about a range of motivations for commencing and continuing to provide foster or kinship care. Carer 884 expressed altruistic motives, asking ‘if it wasn’t for me, where would these boys be?’, while Carer 326 was one of those who expressed that caring met a need to parent felt by himself and his partner: ‘We had an empty house when our children left home. We had a feeling of loss of purpose and fulfilment.’ Although motivations differed somewhat between foster and kinship carers and within these groups, meeting the needs of a child and/or meeting a need within the carer themselves were those most commonly expressed.
Needs relating to status and esteem can be divided into elements that contribute to self-esteem, such as achievement and mastery, and those which give rise to gaining the esteem of others, including reputation and dominance (Kenrick, et al., 2010). Participants reported many challenges in having these needs met, with one asserting that ‘decisions are made on statistics rather than our input as carers’ (Carer 132). Many foster carers in particular agreed with this sentiment, expressing a feeling of marginalisation from decision-making for the children in their care. Some participants stated that they had little or no rights in this regard and expressed a desire to be listened to, taken seriously and treated with respect. One carer expressed their frustration, stating: ‘My house is not seen as mine. I need to be treated with more respect and privacy’ Carer (923). Another described their own experience of the Department of Health and Human Services (DHHS) as ‘disrespectful’, saying that they have ‘had to fight for every bit of support that [they were] guaranteed’ (Carer 175). Others felt isolated in decision-making, having to make complex decisions without adequate professional input or support.
Twenty-nine percent of participants (n = 19) stated that they did not have enough information about the condition of the child in their care, with many also describing a lack of basic information regarding the child’s legal situation, medical history and support network.
In the words of one carer: We need to know everything about a young person. A young person who was taking medications and had panic attacks – I was given no information about this prior to being responsible for him. (Carer 135) The case manager had information for the wrong child at the start of the placement. We were told they would get back to us with the right information but they never did. (Carer 869)
Accessing appropriate information continued to be a challenge for many participants when children in their care experienced health or well-being issues. One carer stated that they were not apprised of details due to ‘privacy concerns’, while many felt that they were not given adequate practical information on how to support looked after children with their health or well-being from day to day: One child…we took him on but were never given information regarding his background – there was no support. He was very violent. We later learned of his background of violent sexual abuse. He ended up murdering someone. (Carer 687)
Carer 649 described one such case: Some kids come straight from court with no information at all. What if that young person has a history of sexual assault? I need to know because my grandkids come here on the weekend.
The need to parent
Kenrick and colleagues (2010) concluded that parenting is among the highest-order human needs. They posited that the need to parent has a close relationship with Maslow’s (1943) need to self-actualise, as reproduction and other forms of parenting are ‘not ultimately about self-gratification, but [involve] a considerable diversion of resources away from selfish goals and toward other human beings in our social networks’ (Kenrick, et al., 2010: 312). This can result in detriments to other aspects of quality of life. As Carer 42 described: ‘The kids’ needs are more important than mine, and I easily get distracted by that.’
Sixty percent of kinship carer participants (n = 9) identified that their relationship with the child in care was ‘a little’ strained. One stated that it caused her significant emotional stress but that she ‘wouldn’t have it any other way. I want them here’ (Carer 649). Foster carers were less likely to report a strained relationship with the child in care, although 10% (n = 5) spoke of the relationship being strained ‘a lot’. Carer 577 said that he ‘would love to have [his] old life back, but [he] couldn’t imagine life without [young person]’. Some participants described a strong parental connection to the children and young people in their care and some did not, but the majority expressed a view that they were the people who best understood the needs of the child. One described it in this manner: ‘None of them [case workers] know her. I don’t want them to plan her life without asking me first’ (Carer 544).
Forty-two percent of kinship carers (n = 4) and 53% of foster carers in our study (n = 24) reported short-term detrimental aspects in their caring role related to their ability to work or participate in education and training. One woman, a PhD candidate, described her story: ‘It’s been pretty exhausting. I’ve had to curtail my research programme. It’s dragged out, I’ve lost interest’ (Carer 89). Another participant said they had given up their full-time paid employment due to their caring role (Carer 902).
Discussion
Other researchers have provided some important contributions towards understanding the carer experience through examining carer strain (Farmer, Lipscombe and Moyers, 2005), carer dissatisfaction (Maclay, Bunce and Purves, 2006) and carer retention (Colton, Roberts and Williams, 2008). This study has sought to expand these ideas and make a contribution through the application of a hierarchy of needs to the foster and kinship care context, thus improving our ability to explain how carer needs may impact on their caregiving role.
All children placed with foster and kinship carers will have lived through a significant period where their needs were not being met, some for many years. The experiences of children prior to entry to care relayed by participants were sad, often violent and deeply traumatic. As a result of experiences like this, looked after children are more likely to have major needs related to their behavioural difficulties, emotional and mental ill-health than most children (Milburn, Lynch and Jackson, 2008). In large part, the burden of meeting these needs falls to their new primary carer. Participants in this study – both foster and kinship carers – reported a lack of information and understanding about the carer role prior to its commencement. Some continue to be surprised and alarmed by the demands made of them, describing a range of detrimental impacts.
Foster carer participants in this study expressed motives related to altruism or a desire to parent to be the primary drivers behind their decision to provide care. The foster care literature supports these findings, explaining that people choose to become foster carers for a range of reasons. But two comprise the overwhelming majority of their motivations: it is a ‘good thing to do’ (altruism) and it provides ‘an opportunity for children to be part of the family’ (parenting) (Peake and Townsend, 2012: 10). Conversely, kinship carers are motivated to care primarily for reasons of family loyalty, commitment and attachment to the child (Department of Communities, 2011), which were echoed by participants in this study.
Our findings support Lyubomirsky and Boehm’s (2010) conclusion that parenting may interfere with the capacity to meet our other human needs, and suggest implications for the form of intensive parenting practised by foster and kinship carers given the complex needs involved. The motivation of participants in this study to become and remain carers stemmed from need, whether their altruistic desire to meet the needs of children or their own personal need to parent. Their days consisted of meeting the physical, emotional, social and intellectual development needs of children, some almost to the exclusion of all else. The act of meeting one need at times caused a significant barrier to their capacity to meet another.
While meeting most human needs results in happiness, our findings support the conclusion that meeting the need to parent can also be associated with decrements in well-being (Lyubomirsky and Boehm, 2010). This can be partially explained by the bidirectional relationship between the behaviour of children and parental stress described by Neece, Green and Baker (2012). The more children exhibit behaviours designed to have their needs met, such as an infant crying, the more stress a parent may experience. Looked after children may have more immediate and complex needs than their peers. Participants in this study described behaviours that could reasonably be expected to place them at greater risk of experiencing parental stress than other parents, which may, therefore, have impacted on their ability to meet the needs of children in their care. Many explicitly described this inter-relationship between their needs and the needs of looked after children.
Carers who took part in this study told of both stress and satisfaction. They listed in detail a range of negative personal outcomes which they attributed to their caring role and their exposure to the challenging behaviour and complex circumstances of looked after children. For the majority of carers, providing foster or kinship care was associated with negative outcomes in every category of need except the need to ‘parent’. Many detailed frequent and significant impacts on areas of life ranging across every part of the needs hierarchy including sleep, nutrition, finances, physical and mental health, and intimate and other social relationships. Two in three carers recounted major areas of unmet need in their personal lives, while the remaining third could reasonably be described as having most of their needs met to an adequate and sustainable standard. Importantly, many participants primarily ascribed the negative impacts of caring not to the challenging behaviours of the children in their care, but to high levels of dissatisfaction with the DHHS and its management of the care system. This echoes Randle and colleagues (2017) who found that many carers are dissatisfied with factors which are within the control of foster care agencies. This included failure to provide timely and appropriate information about looked after children, inadequate financial support and a lack of help in dealing with crises.
Use of the CUES-C provided rich qualitative information, supported by quantitative results that significantly assisted with interpretation and analysis of data. Implementing the survey through a structured interview format meant that participants were supported and encouraged to work through the multiple domains, often engaging in a conversational style, and valuable data were gathered as a result. We believe the CUES-C may be appropriate for further use with foster and kinship carers.
Overall, the results of this study present a mixed picture. On the one hand, many participants described stress, frustration and even despair. But on the other, they often also spoke about their commitment to their role as a carer. It seems clear that the opportunity to parent looked after children provides fulfilment for many carers. However, choosing to become a foster or kinship carer can also result in a range of negative impacts on more foundational needs. In order to fulfil their caring role, carers’ needs often go unmet. Given the link between diminished carer well-being and poorer outcomes for looked after children (Garcia, et al., 2015), this is of grave concern. Without the provision of timely and holistic supports and intervention, the two-way relationship between the needs of looked after children and their carers may create a feedback loop where stress and trauma can be endlessly amplified, to the detriment of both parties. The evidence from this study supports the importance of addressing both the needs of carers as well as those of the young people in their care, with some basic improvements noted that could ease the burden of care and simultaneously increase satisfaction in the caring role.
Carer recruitment and retention is a major problem in many jurisdictions, no doubt significantly impacted by the inability of systems to effectively address unmet carer needs. A range of practical measures are necessary in order to facilitate the capacity of carers to appropriately meet the needs of the children in their care and ensure that the caring role remains attractive. Participants told us that foster and kinship carers must be adequately reimbursed to meet the full cost of care and also be recognised as respected members of the care team. Some found respite of value. Others raised the importance of timely and accurate information and advice. Participants particularly wished for their expert knowledge of looked after children and their critical role in meeting their needs to be recognised and appreciated.
Conclusion
This article has discussed the application of theories of human need to the context of the carer household, providing an overview of the relevant literature and drawing on the perspectives of foster and kinship carers to understand how unmet needs may impact on carers’ caregiving role. This process has shed new light on the complexities of the carer–child relationship through the examination of carer needs. A number of research implications arise as a result, including the potential for the application of needs theory to other complex and critical human relationships, as well as the development and evaluation of interventions involving foster and kinship carers. In addition, there is potential for further examination of particular categories of need and their interactions within the relationship between foster and kinship carers and looked after children, in order to better understand and address unmet need within the context of home-based care.