
Abstract
This article compares the needs and background characteristics of children who became looked after by an English local authority between April and July in 2019 and the same three months in 2020, with the aim of identifying any impact of the Covid-19 pandemic which broke out in March 2020 and continued for some months thereafter. It scrutinises the two cohorts, comparing children's age, gender, ethnicity, entry to care with siblings and reasons for admission. Differences attributable to the pandemic were found.
Introduction
The impact of Covid-19 on families, communities and society has been well documented. The English City of Derby saw a significant increase of 30% in the number of children becoming looked after during the second quarter of 2020 (April, May, June) compared to the same three months in 2019. Over the past five years, the local year-on-year increase of children entering care has been 8% – around twice the national average. Some of this reflects a rise in numbers of unaccompanied asylum seeking children (UASC), although their numbers have reduced significantly in the last year.
The population of the City of Derby is younger, more ethnically diverse and more deprived than the average for England as a whole. The last Census recorded a population of 257,000, of whom 25% were from a minority ethnic group. In addition, the city is one of the 20% most deprived areas of England with a Deprivation Index of 27.79 (Ministry of Housing, Community & Local Government, 2019). Life expectancy for both men and women is lower than the national average and levels of health and inequality are generally higher. The children becoming looked after and originating from the city are predominantly White British (63%), male (57%) and aged 10 to 15 years, and enter care mostly as a result of ‘abuse and neglect’.
This health note explores the potential reasons for the 30% increase of children entering care in Derby City in the second quarter of 2020 and assesses its impact on services. The main factors for consideration are whether the local authority’s thresholds for taking action have changed during the Covid-19 pandemic, the impact on social care caused by difficulties in arranging visits between families and children, the lack of contact with teachers and other professionals due to school closures, and the changes that have occurred in family dynamics.
Method
We used data from the weekly report submitted by Derby City Council to the local health provider, Looked After Children, Derby and Derbyshire Clinical Commissioning Group (CCG). This records all new ‘care episodes’. The reporting system has been implemented and led by the Designated Nurse since 2018 and was created to improve the flow of information between the local authority and the local health provider. It has led to a significant increase in Initial Health Assessment (IHA) compliance.
The study samples collected consisted of 46 children for the second quarter of 2019 and 66 for the same period in 2020. For each cohort, data from the local authority and the electronic patient health record were analysed using the ‘starting care episodes’ as a criterion for inclusion. This comprises all admissions into care notifications as well as child protection information and statutory IHA details. (All looked after children are subject to this statutory assessment within 20 working days.)
The following information was collated:
age of the child becoming looked after; gender; ethnicity; sibling groups; ‘abuse and neglect’ as a reason for entering care; number of children with a child protection plan in place.
Findings
The study findings are outlined below.
The changes in the age bands between 2019 and 2020 are shown in Figure 1. There is a reduction in the number of children under one year coming into care (from 27% to 21%) and an increase for those aged between one and 15 years; this is especially marked for the two- to three-year-old group. In contrast, there is a reduction in those aged over 16 entering care as well as for UASC.

Ages of the children entering care between April and June 2019 and 2020 (shown as percentage for each cohort).
Of particular interest is that the percentages for children aged 10 to 15 have remained consistently high in comparison to all other age groups, both locally and nationally. It is difficult to explain this but it may be linked to an increase in socially unacceptable behaviour and willingness of older children to disclose abuse and neglect and reveal acute stress within the family home. In addition, the higher percentage for the 2020 group may be related to young people not being in education, having the perceived freedom to socialise without the restraints of school routine and general difficulties in controlling anti-social behaviour among adolescents.
Within both cohorts all the UASC were aged 14 years or above; they are analysed as a separate group as many of their needs and current situations are different from their peers. Also, as noted above, their number has significantly decreased in the last year as a result of changes within the immigration process at the point of entry (Home Office, 2019).
Figure 2 shows that there were significantly more males entering care in the second quarter of 2019 compared to 2020. However, comparisons between the two cohorts are somewhat distorted by the number of UASC in the 2019 sample (15% of the total) as most of them are male. The gender distribution of the 2020 cohort is more in line with national statistics and the historical pattern for Derby City. The decreasing numbers of UASC entrants is linked to the improved assessment of age at the point of entry and fewer young people arriving in the city stating they are under 18 years old. On entry to England, if a young person appears to be under 25 and there is doubt about their true age, they are dealt with according to the age they give; if this is under 18, they are accommodated as looked after children in the geographical area of entry or through the UASC transfer scheme (Home Office, 2019).
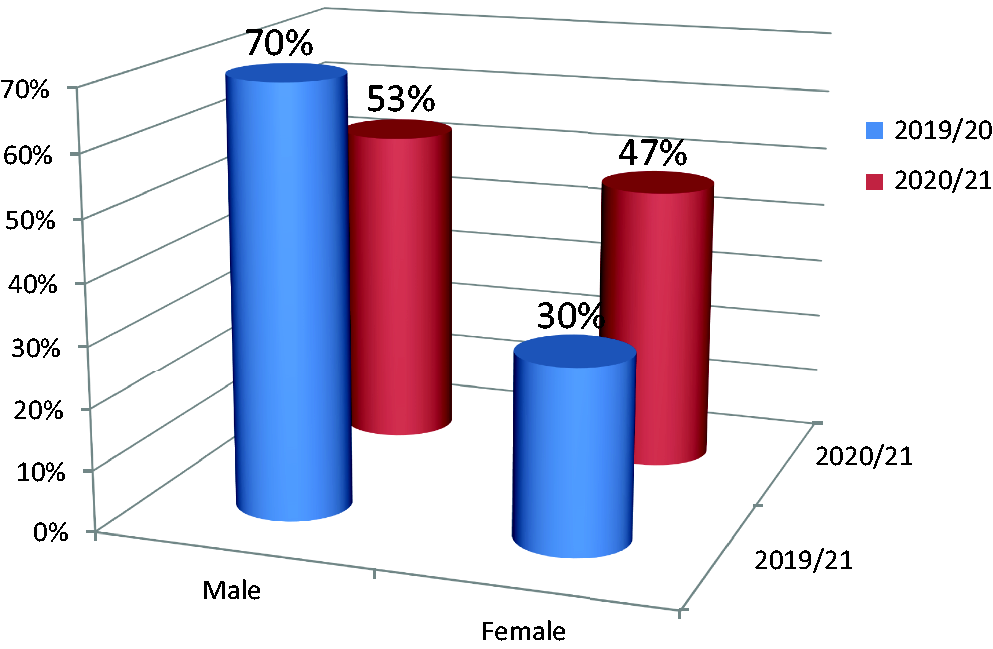
Gender comparisons between entrants for the 2019 and 2020 cohorts.
The main ethnic group is unchanged between the two cohorts and remains predominantly White British (Figure 3). Between 2019 and 2020 there is a drop in the number of children entering care with a reported ethnicity of Asian, Black, Dual Black/White, Dual Other and White Non-European but the reasons behind this downward trend are unclear. The reported data of Dual Asian/White ethnicity has shown a rise of 4% and for Gypsy/Roma a bigger rise of 10% which links to the subsequent analysis of sibling groups. (There is a correlation between Gypsy/Roma ethnicity and the increase in sibling groups entering care in 2020.)
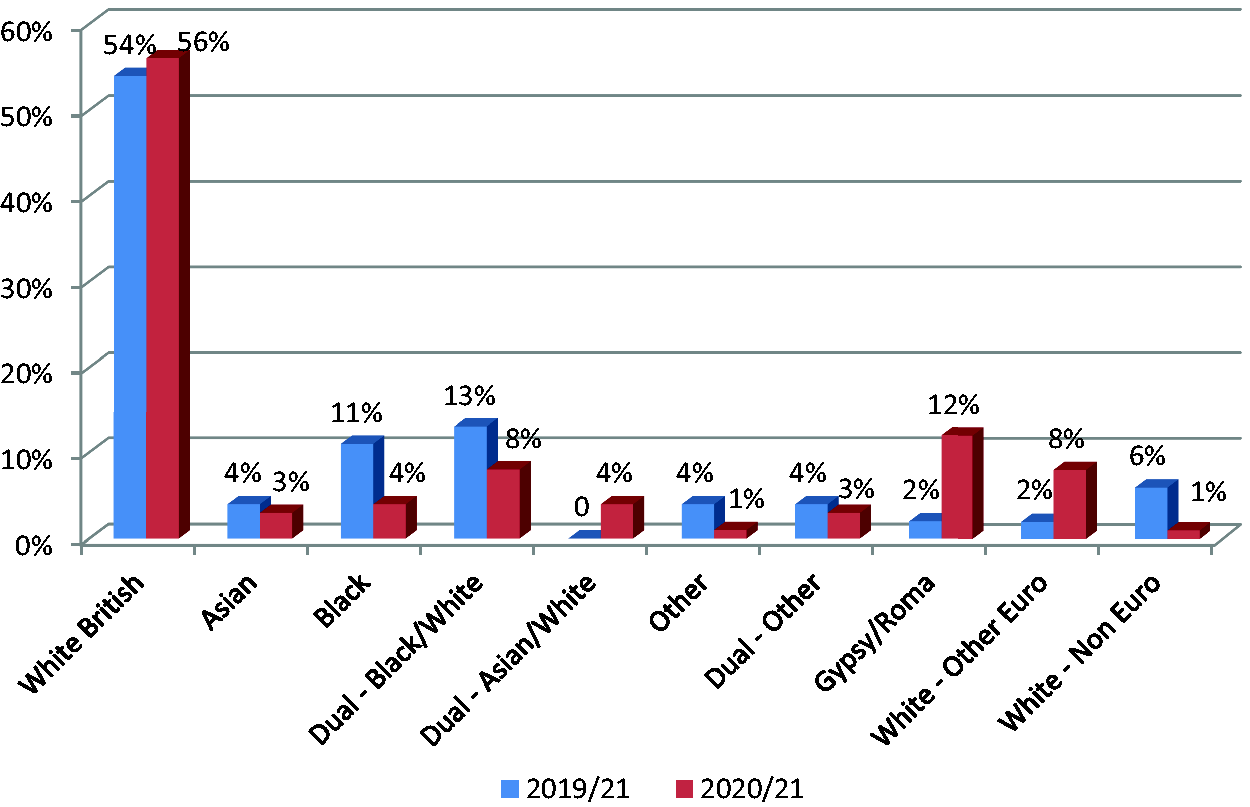
Ethnicity comparisons between the 2019 and 2020 cohorts.
The data in Figure 4 indicate a significant increase over the study period in the number of sibling groups of three or more children, with a notable growth of 18% for groups of four. This has had a substantial impact on the ability to place siblings together and affects the capacity of the health system to undertake IHAs within statutory timescales.

Sibling group size comparisons as percentages of the two study cohorts.
Figure 5 further analyses this increase by showing that the highest rise is for sibling groups of four (200%), followed by groups of three and seven children (100%).
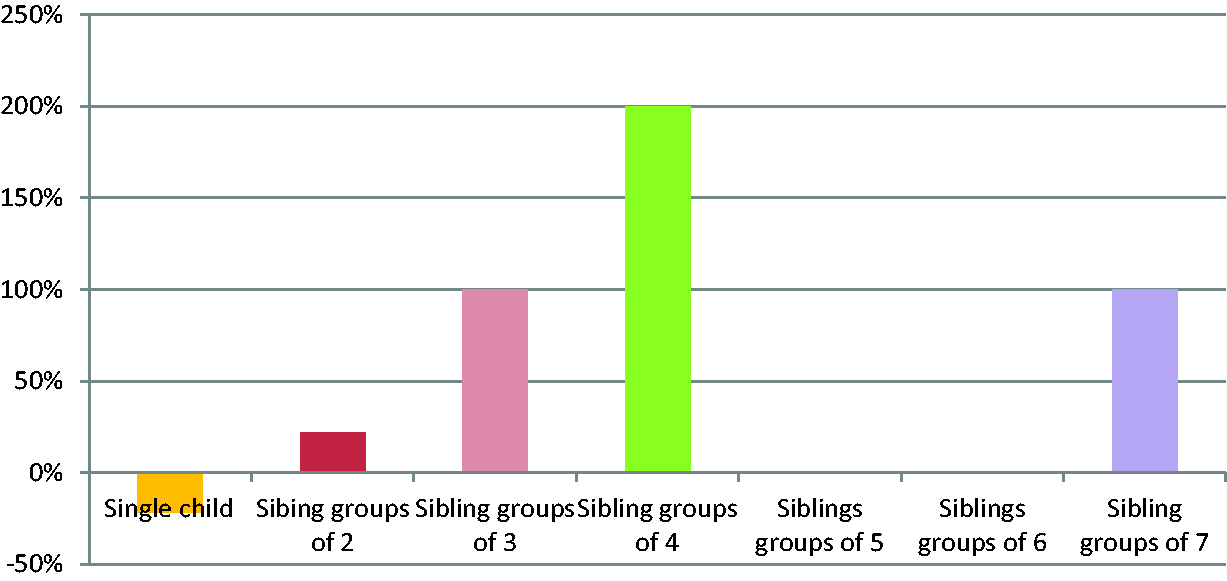
Percentage increase of sibling groups as a comparative cohort in 2019 and 2020.
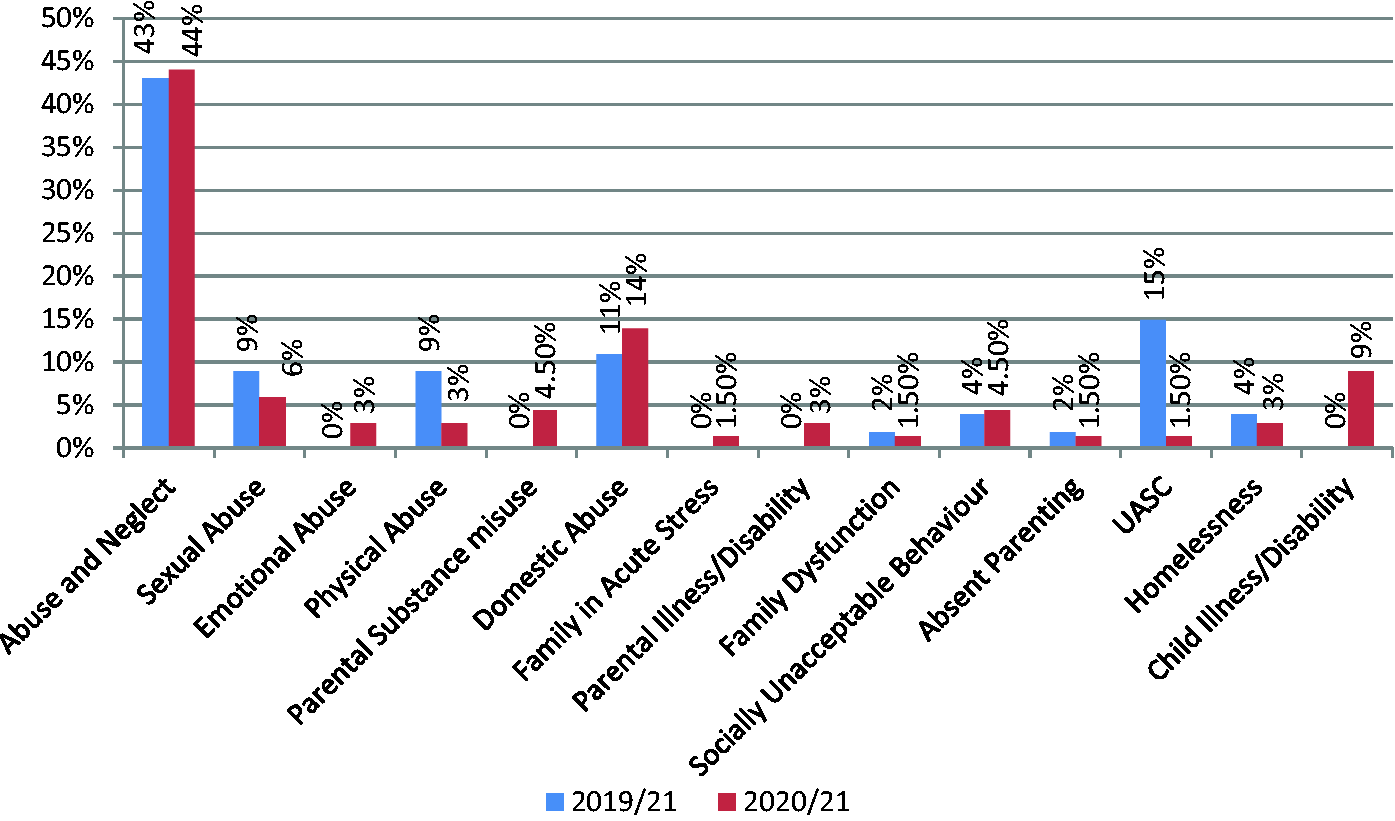
More contrasts between the two cohorts emerge when the reasons for becoming looked after are examined. Details can be seen in Figure 6 and can be summarised as follows:
The categories of abuse and neglect remain stable as the most common reason for becoming looked after. Physical and sexual abuse show a decrease; this may be related to a lack of disclosure opportunities and/or lack of contact between children and professionals. Being involved in or witnessing domestic abuse incidents within the home environment has increased as a reason for entry. This may stem from pressures within the family unit exacerbated by the pandemic, such as financial issues related to lack of work or furlough, or tensions caused by spending unusually long periods of time together. The number of families where acute stress is cited increased from 0% to 1.5%. Again, this may be linked to the environmental Covid-related factors encountered by families. Interestingly, the incidence of children coming into care as a result of homelessness has decreased, perhaps as a direct result of the pandemic hotel schemes to reduce the number of people living with no fixed abode. Parental illness and/or disability has shown an increase of 3% over the year; this deterioration in parents’ mental and emotional health and well-being, linked to the impact of lockdown, social isolation and emotional pressures of the pandemic, clearly has a negative impact on their ability to care for their children. Percentage comparison between the 2019 and 2020 cohorts for the reasons for entering care.
Finally, when comparing the two study cohorts, little difference was found in the numbers of children entering care with a child protection plan (9% and 8% respectively).
A weakness of this study is that it is difficult to determine how far the pandemic has affected thresholds for action and the evidence from this survey is mixed. There are certainly forces likely to increase admissions to care, such as pressures on families and reduced controls over adolescents’ behaviour, but on the other hand, use of new communication technologies has eased some aspects of providing preventive and support services.
Overall summary
It is clear from this comparative study that the number of children entering care in Derby City during the second quarters of 2019 and 2020 increased by 30% and that the young people concerned are predominantly aged between 10 and 15 years, male, of White British ethnicity, belong to a sibling group of two or more and are looked after because of abuse and neglect.
There has also been a rise in the number of children aged two to 15 years entering care because of domestic abuse in the family home, family pressures, parental illness/disability and child illness and/or disability. Some of this increase can be attributed to the national lockdown that has made services less available, stretched resources and damaged family relationships and finances.
The financial costs of providing services have also accelerated over the two time periods, affecting the ability and capacity of social care and health services to meet statutory requirements, find placements that keep siblings together, facilitate timely health assessments and ensure that the features of high quality care are maintained.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.