
Abstract
This report, the second of three, discusses the nature of a recent turn in health geography towards a posthuman theoretical orientation. This is an ontological turn that challenges basic categories leading to the understanding that health is not solely a human condition, but one created within assemblages of multiple human and nonhuman actors and forces. This is a turn concerned with the immediate and processual emergence of health, hence one that recognises the critical roles of pre-personal and more-than-representational events and forces. These facets are explored along with the extent to which the new ‘posthuman geography of health’ is a departure, and the forms of enquiry and ethics it brings forth.
I Introduction
Something is clearly happening to a substantive part of the sub-discipline of health geography, not so slowly and quite surely. Following two decades of humanistic inquiry placing human subjects firmly at the forefront of studies – exploring the meanings, attachments and identities they attribute to health and place (Kearns, 1993) – in the past ten years a new turn has commenced. With regard to how this turn might be categorised, ‘post-humanistic’ is an accurate descriptor, reflecting its theoretical departures and breadth and alignments with broader trends in the parent discipline (the term ‘more-than-human’ preferred by certain scholars).
As a theoretical orientation and mode of thinking, posthumanism rejects humanism’s ‘common sense’ views on the ‘self-evident’ primacy and uniqueness of the human in life, and with this the idea of a largely autonomous and fully reasoning human subject that culture layers onto (Duff, 2018). Instead, posthumanism recognises that humans are not contained or coherent entities but instead only ever exist and operate within distributed, expansive processes. It recognises that all things, human and otherwise (such as health), are produced through relations between a range of biological/natural and material/technological actors, including through the excessive vital forces that both exist within these actors and emerge during these relations (Duff, 2018).
Beyond addressing the shortfalls of humanism, other factors have led to the emergence of posthumanism in health geography which are to do with the world beyond books. Posthumanism is also an emerging societal condition; a regrouping and reorientation of cultural forces in the world (academic posthumanism hence being a theoretical orientation that considers this condition and these forces; Duff, 2018; Whatmore, 2006). It is argued that under changes the posthuman condition has heralded, it increasingly difficult to separate the human and nonhuman and their agency in relation to health (Duff, 2014; Whatmore, 2006). As Andrews (2018) explains, these changes have occurred in two realms in particular: modes and forms of health consumption, and parameters of human life and health.
With regard to consumption, drawing on the ideas of Nigel Thrift, scholars have noted that we live in a rapidly reconstituting world in which categories such as sexuality, gender, race, age and class are no longer the only conduits for health-related experiences. A world in which consumption has moved further to the foreground at an ever accelerating pace (Andrews, 2018). Human bodies move within an increasing range of environments and in relation to an increasing range of objects, with health consequences. Technological hardware (such as smartphones and tablets) and software (such as social media) give humans new forms of knowledge and awareness on health that bridge space and time and become obsessions in themselves (e.g. Simpson, 2017). New affective sensory pastimes entice human bodies into them, ranging from health activism to holistic and fitness lifestyles (e.g. Lea et al, 2015). Public health and health care organisations engineer root textures to their advice and care, adding multiple aesthetics and distractions that play to multiple senses and emotions (e.g. Solomon, 2011). The proposition follows that humanism is not best placed to engage this faster moving sensory world of health consumption which is arranged and experienced differently and where the subject/self is under constant manipulation by affective forces. Indeed, that the stabilities humanism attributes to people, health and place no longer exist to the degree that they once did, and therefore that we need a new research lens that is able to bring all this into much sharper focus (Duff, 2014).
With regard to human life and health, acknowledging the pathbreaking work of Donna Haraway in his assessment, Duff (2014) suggests that there have been fundamental changes in recent years. First, under technological innovation (such as bio-technology, nanotechnology, medical robotics, cell harvesting, pharmaceutical development and virtual reality) – not to mention numerous technologically-produced contaminants invading human bodies – previously firm distinctions between phenomena (such as cells vs society, nature vs culture, natural vs artificial, medical vs economic, medical vs social) are increasingly breaking down. Life itself becoming a ‘natural resource’ to be used and improved (Whatmore, 2006). The point here is that humanism has only served to sustain such dualisms, for example by informing the either/or positions of supportive transhumanism (informed by secular humanism) or sceptical bioconservativism (informed by religious humanism). Duff posits that if human life is itself being reconceived, then research approaches need to be developed that redraw boundaries between phenomena, that are more aware of the many commonalities and relations between them, and that more generally are better equipped to deal with these fusions of science, the body and society, and the highly politically charged climate that results (Andrews, 2017; Whatmore, 2006). Second, although what health is has long been debated, in the 21st century it has become even more of a complex question because many moral, bio-psychological, cultural, political and technocentric interpretations come into play. Indeed, policy, practice and academic efforts are increasingly made to expand thinking on health, but they have resulted in the production of numerous sub-classifications that, although incorporating both body and mind, possess their own definitional and implementation challenges. Moreover, that each capture only a fraction of real human experiences (e.g. wellbeing, wellness, holism, happiness, quality of life, functioning, fitness, resiliency, precarity, security, thriving) (Andrews, 2017; Duff, 2014). Hence Duff argues that, faced with this endless dividing, health geographers might be appropriately occupied getting back to ‘basis’. Instead of pondering how health can be labelled and what it means, they might think fundamentally about how it happens (albeit that some posthuman research does align itself with these sub-classifications; see Andrews et al., 2014; Atkinson, 2013; Smith and Reid, 2017).
II The posthuman turn as an ontological turn
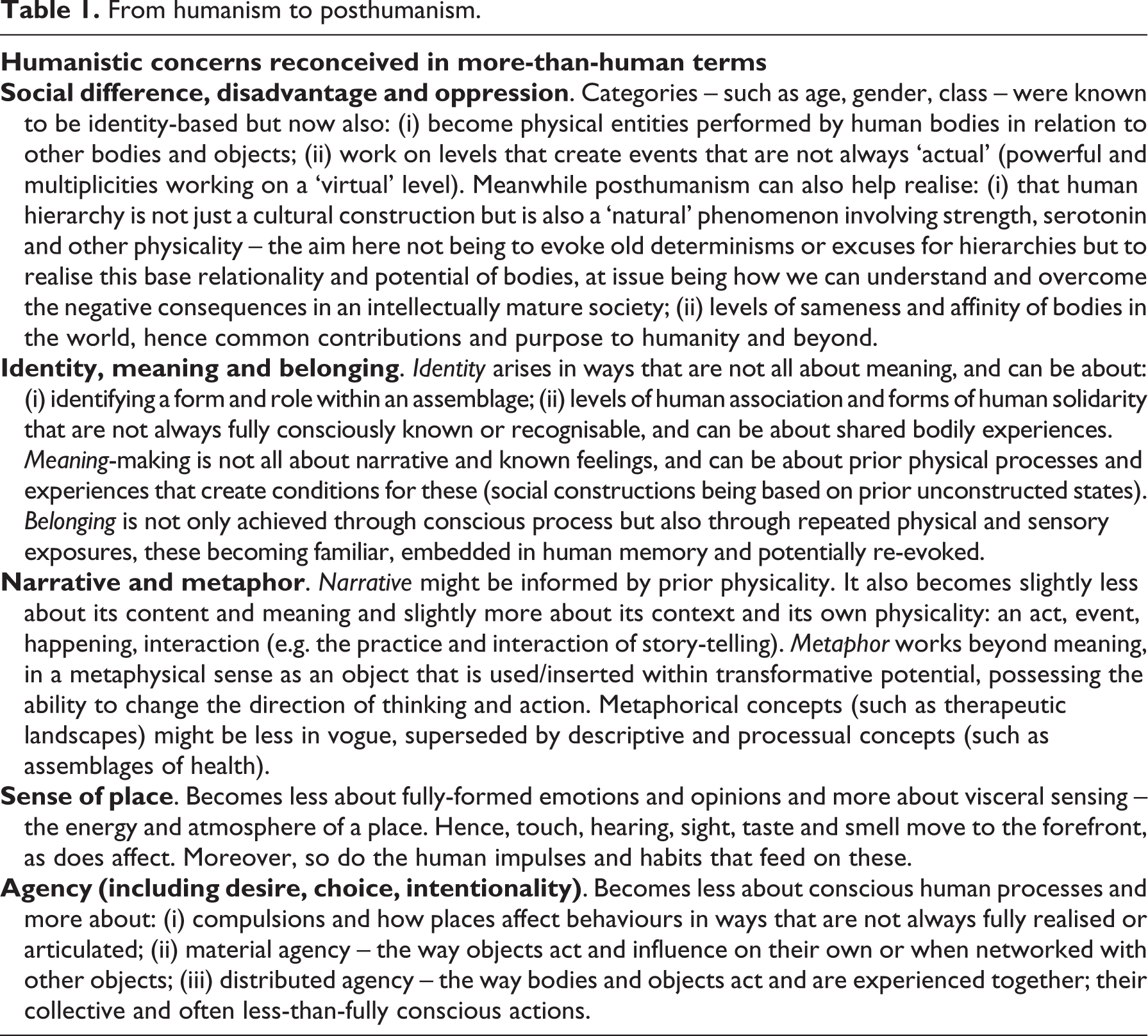
The posthuman turn in health geography still sits reasonably comfortably within Robin Kearns’ well-documented call for a post-medical ‘geography of health’ (Kearns, 1993), in that health is still an interest as a ‘thing’ in a broad sense beyond the non-occurrence of disease. It is unlikely, however, that Kearns and others envisaged that the very humanistic basis of the geography of health would be challenged in the way that it has in recent years, it being unsurprising that they have expressed concerns with certain ideas and departures (Kearns, 2014). This said, the posthuman turn does not signify a complete displacement of humanism in health geography. Humanism has laid a strong foundation for post-structuralist theory, critical approaches and qualitative methods in the sub-discipline, all of which are part of a posthuman approach. Moreover, posthumanism does not reject humanistic concerns and concepts – such as meaning, agency and structures of oppression. Rather, it recognises that these can flow from the processual workings of assemblages comprised of the human and nonhuman, and resulting states of being that are less-than-consciously acted and felt (see Table 1). Indeed, posthumanism does not ignore things that are known to be subjectively important to human subjects. Instead it seeks to rethink and rework them in more-than-human terms (Greenhough, 2014; Philo, 2007).
From humanism to posthumanism.
Interestingly, posthumanism has rarely been explicitly discussed in health geography (see Duff, 2018), yet it very clearly captures a range of interwoven theoretical orientations that have been proposed and used by health geographers for rethinking and reframing human environment relations in health. In particular these include vitalist philosophy (Philo, 2007, 2012), actor-network-theory (Duff, 2011; Greenhough, 2011a), assemblage theory (Atkinson, 2013; Brown et al, 2012; Duff, 2014; Kearns, 2018), non-representational theory (Andrews et al., 2014; Andrews, 2018; Lea, 2018) and new materialisms (Doel and Segrott, 2004; Middleton, 2010; Williams, 2010). They also include, to an extent, certain ideas in critical biosocial studies and environmental epigenetics (Guthman and Mansfield, 2013; Lorimer, 2017; Prior et al., 2018), relational thinking (Conradson, 2005; Cummins et al., 2007), political ecology (Jackson and Neely, 2015; King, 2010), complexity theory (Curtis and Riva, 2010; Gatrell, 2005) and applied pragmatism (Cutchin, 2004, 2016). Certainly, then, posthumanism is not a totally coherent or cohesive theoretical position in health geography, it appearing in many guises and to various extents.
It was Canadian health geographer Josh Evans who first publicly floated the idea, at a session of the 2017 International Medical Geography Symposium, that certain features of the posthuman turn in health geography point to it being not only epistemological but also ontological in character. While this might not be a particularly surprising observation given the nature of posthumanism, his point was that, whereas the humanistic turn in the 1990s was ontological in terms of rethinking place as a social and cultural phenomenon (i.e. rethinking fundamentally what place is), it was merely a more expansive epistemological engagement with health (i.e. about the way we can know health). The posthuman turn, in contrast, is ontological all round. In the new wave of posthuman health geography there exists, on one level, an extensive theoretical project. This is to re-think explicitly and fundamentally basic ontological categories involved in being – such as body, object, subject, space, place, time, cause – in order to challenge current ontological understandings of health and develop new ones. On another level there exists a concurrent reformed empirical project. This is to use these re-thought ontological categories and new ontological understandings of health to underpin more applied research on more-than-human processes in health. These new understandings act as a loose framework for health geography, with scholars accepting them as principles which enable them to ask certain questions. Three themes, I suggest, compose this framework – relational material assemblages; performing and open human bodies; the immediate, pre-personal and more-than-representational. Through this framework health is (re)conceived not as a physiological or psychological condition, but instead as a mode of existence. At issue are the struggles and journeys humans undergo, and the actors they encounter, in becoming and feeling more or less healthy (Duff, 2014).
1 Relational, material assemblages
Posthuman health geography emphasises the relational materialities involved in health. It recognises that not only are human and nonhuman bodies and nonhuman objects (hereafter referred to as human and nonhuman agents) responsible for the emergence of health but that, being on the same level of existence in ontological terms, they are of equal importance, can co-evolve and can lack clear distinction. As Andrews (2014) suggests, posthuman health geography recognises that these relational materialities are ‘trans-scaled’, in that human and nonhuman agents in any one place are complexly networked with human and nonhuman agents in other places. Moreover, that they are ‘performed’ in that human and nonhuman agents possess positions and movements relative to each other, and interact and interrelate with particular timing and spacing. These ideas have underpinned, for example, examinations of equipment, workers, animals and pathogens in the creation of disease knowledge (Greenhough, 2012; Hinchliffe et al., 2016), and examinations of belonging and materiality in mental health (Tucker, 2017).
Providing some additional parameters, and helping to explain further how health emerges, posthuman health geography has lent heavily on assemblage theory. In particular this approach draws attention to the ‘composition' and ‘processes' of health-mediating assemblages. With regard to composition, it emphasises the grouping of human and non-human components (agents) in place which might contribute to health in some way (Andrews, 2018). As Duff (2014) suggests, just as it would be rare for everyday encounters in life to be intrinsically healthy or unhealthy, similarly it would be rare for components of assemblages to be intrinsically healthy or unhealthy; instead, they are contributors to the becoming or retraction of health. Hence, with regard to processes, assemblage theory emphasises the many mechanisms – such as affects, relations and events – involved in the becoming or retraction of health in particular places (Andrews, 2018; Duff, 2014). These mechanisms release the potential of the components and the excessive vitality of the assemblage.
In sum, assemblage theory leads to scholars asking fundamental questions of assemblages such as: What is in-situ? What is arriving or leaving? What is passive or active? What is interacting with what and how? (Andrews, 2018). Although assemblages often bridge communities and institutions, they can originate or be experienced in one or the other. The aforementioned questions are hence being asked in community-based research, for example, in studies of assemblages in movement and fitness activities (Barratt, 2012; Middleton, 2010), baths and bathing (Foley, 2014), caring and disabilities (Stephens et al., 2015), mental healing and recovery (Duff, 2012) and urban drug use (Duff, 2016a). They are also asked in institutional-based research, for example in studies of hospitals and global health imperatives (Sullivan, 2012), schools with surveillant anti-obesity practices (Rich, 2010) and classroom-based therapeutic interventions (Atkinson and Scott, 2015). Clearly evident from this literature is variety, and that different assemblages achieve quite different health forms.
2 Performing and open human bodies
The posthuman idea of health as a modulation of life produced through assemblages decentres the human body, removing it from its former privileged position in terms of health events, agency and experience. Hence the emphasis in posthuman health geography turns towards the wider origins and character of the emergence of bodily health (as opposed to changes in the body itself or opinions on the body). In these terms, certain research is focused on the practices and performances that human agents (bodies) undergo with nonhuman agents (objects) in health contexts. The efforts they exert collectively in particular directions often resulting in expressive arrangements which are read and reacted to either consciously or less-than-fully consciously by other human bodies (Andrews, 2014). Here, following pathbreaking work on the movement and gestures of fat bodies (see Colls, 2007), more recent subjects studied have included lines of movement in dance therapy (McCormack, 2013) and physical expression in running (Lorimer, 2012).
Posthuman health geography also acknowledges that health is not stable or static in human bodies, even within short timeframes; that health states and experiences are only momentary actualisations, and that human bodies are always in the process of becoming more or less healthy (Andrews, 2018). Unlike a biomedical view of the human body as biological machine to be maintained (e.g. at a state of morbidity), an epidemiological view of it as a unit (e.g. infected or not infected), or a humanistic view of it as emotional (e.g. negotiating, opinionated, coping), a posthuman view instead sees the human body as matter and energy, open to change through its encounters. Hence, although the human body might be de-privileged under posthumanism, it is still recognised as an important sense-making vessel that is waiting with its numerous receptors for something to happen and to react in some way. In terms of empirical research, on the one hand a focus has developed on senses and sensations as a different form of knowing achieved through feeling but not necessarily thinking deeply. Empirical subjects of interest include smell in care farming (Gorman, 2017), sight, sound and touch in animal laboratory work (Greenhough and Roe, 2011), the look and feel of simulations in nursing training (Soffer, 2015), the sights and sounds of medical tourism (Solomon, 2011) and ground feel in cycling (Brown, 2017). Notable other research focuses on sensing the body itself, such as in the context of pain (Bissell, 2010) and drug highs (Bøhling, 2014). On the other hand, a research focus has developed on impulses and habits as automatic less-than-fully conscious ways of being that can hinder health (such as classically in drug-taking contexts or cascading negative thoughts in mental health), or alternatively can help humans make sense of and get through life, producing a form of repetition and intelligence that assists them (such as in many forms of care and recovery). Subjects considered have included, for example, the habitual daily routines in managed alcohol and abstinence-based programs (Evans, 2012; Wilton et al., 2014), attempts to get physically fit (Middleton, 2011), anchoring mentally-ill people to their home spaces (Tucker, 2010), and holistic, mindful lifestyles (Lea et al., 2015).
3 The immediate, pre-personal and more-than-representational
Posthuman health geography draws on the philosophy of Deleuze to think about the immediacy of life and health. Rather than attributing health to structural impositions or transcendental phenomenon (such as rules, laws, God, reason or nature), research instead recognises that health arrives within a ‘plane of immanence’. Involving a multiplicity of human bodies, objects and forces, this plane manifests the world (Andrews, 2018). Indeed it is impersonal, subjectless, neutral, indefinite (preceding meaning or individualisation) and exists only through the singularity of events (Duff, 2014). These fundamental ideas have been part of the infusion on non-representational theory into health geography. This tradition focuses on the ‘bare bones’ practices, textures and pushes of life, animating what is happening in the creation of health, often evoking forms of movement, awareness, knowledge and affective inter-body solidarity that do not involve full contemplation or verbalisation (Andrews, 2014, 2018).
Non-representational health geography is such an important part of the posthuman turn that it is not possible to cover it here, particularly when substantive and well-trodden concepts such as affect are considered (reviewed far more thoroughly in my third forthcoming report). Nevertheless, a few areas of interest include: (i) The ‘onflow’ of space and time. Specifically, for example, bodily and material movement in therapeutic community gardening (Pitt, 2014), walking (Gatrell, 2013), running (Barnfield, 2016), and in everyday random moments of wellbeing (Andrews et al, 2014). (ii) ‘Foregrounds and backgrounds’ and their subtle powers. Specifically, for example, therapeutic landscape art in hospital waiting rooms (Evans et al., 2009), ambient background noise in therapeutic retreats (Conradson, 2007), and mental pictures as distraction in needle phobia (Andrews and Shaw, 2010). (iii) ‘Virtuality’ (things not actual, yet still real) and ‘multiplicity’ (complex entities, often in multiple states). Specifically, for example, therapeutic soundscapes in ambient music (Evans, 2014) and memorial benches and therapeutic moments of contemplation (Wylie, 2009). (iv) ‘Ordinary and everyday’ – regular life and space as lived happily, successfully, immediately and sensorially. Specifically, for example, practices and moments of hope in musical consumption (Anderson, 2006), and the ways street music helps produce convivial and healthy public spaces (Simpson, 2014). Finally, (v) ‘Affective mechanisms and experiences’ – collective infectious feeling states and environments which encourage, or even exclude/detract from, health. Specifically, for example, in mental health service use and recovery (Duff, 2016b; McGrath and Reavey, 2016), consuming intoxicants and urban nightlife (Duff and Moore, 2015; Jayne et al., 2010) and fitness/movement activities (Foley, 2015; Simpson, 2017).
III Towards enquiries and ethics of assemblage
Personally, I think that posthumanism holds the potential to unite health geography to a greater degree, our sub-disciplinary divisions having become entrenched under humanism (health) vs positivism (medical). This is because it realises the vital connections, productions and excesses that occur between all levels and scales of geo (earth) and all levels and scales of bio (life) (Philo, 2007; Whatmore, 2006). Only time will tell if this potential is realised, but for now scholars are progressing in promising directions. The ongoing project of posthuman inquiry in health geography has already involved methodological experimentation and innovation aimed at understanding and engaging expertise and resources assembled in relation to health (e.g. Davies, 2006; Roe and Greenhough, 2014). A broader future agenda has however been framed and refined by Duff (2014), who talks about investigating the mechanisms of assemblage. As an approach, this involves deploying projects and methodologies to isolate and describe causal pathways in health’s emergence: following the components of assemblages that reveal themselves as active contributors – or at least leave clues and traces or evidence that they are – in the processual course of humans becoming more or less healthy. As Andrews (2018) outlines, further general questions include: (i) Which particular assemblages (e.g. public, private, voluntary, natural or combinations) provide the best experiences and outcomes (e.g. therapeutic, supportive, curative)? (ii) How can assemblages be organised to create situations whereby human bodies are in the fullest possession of their power of acting? (iii) Which forms of political, economic, institutional and social processes help or hinder the emergence of health producing assemblages (which should be used, which should be resisted and which should be ignored)? (iv) How might we best witness and animate the processes and energetic outcomes of health producing assemblages. This is a complex final question attended to by recent studies (see Boyd, 2017; McCormack, 2013; Whitehead et al., 2016) and given dedicated attention in my next report. As Greenhough (2011b) argues, these questions and such an approach – what she thinks of as part of a wider ‘ontological politics’ – help pull away from binary positions and stereotypes articulated in much health geography (e.g. objective, authoritarian biomedicine vs subjective, vulnerable, passive or resisting patients). This is because it is free and open-minded, based from the very outset in ‘real’ situations rather than on constructs (such as oppression, exclusion). Moreover, it needs no specific presupposed criteria to determine the boundaries of health-related events (such as a specific setting, intervention or even condition) (Duff, 2014).
Duff suggests that such a project is underpinned by an ethical position derived from the work of both Deleuze and Foucault: a focus on the ‘ethics of assemblage’. He argues that whereas bioethics is primarily concerned with encouraging the best attempts to deliver individuals and populations to pre-morbid states (the bio-medical view) and maximising patient experiences of care (the humanistic view), what matters more, ethically, from a posthuman perspective is what resources individuals are able draw upon to maintain their recovery or a certain level of health (Duff, 2014). In theoretical terms, then, deciding what encounters might be unhealthy or healthy requires ethical thinking, not based on transcendental rules or power, but based on a belief in the plane of immanence and life as a self-organising process. ‘Common sense’ practice hence emerges from realising affective, visceral, less-than-fully conscious processes, and in thinking about what might be helpful or unhelpful about them (McCormack, 2003). In these terms creativity, experimentation and innovation and other praxes are valued in order to find the correct assemblages and internal alliances and maximise their health potential (Duff, 2014).
With all this in mind, it has been suggested that a potential educational enterprise might exist hand-in-hand with posthuman health geography that moves beyond traditional judgements of what should or should not happen regarding health according to codes and rules, and instead involves directly addressing the forces and powers of private and public organisations and the state (McCormack, 2003). As Duff argues, through education, greater awareness and reflection can be imparted as to what assemblages and how assemblages create or degrade health. The ultimate goal of this knowledge, once translated, is to unite human bodies with health-producing assemblages (Duff, 2014). The ideal end game here would be to reach a stage where, through increased self-awareness: (i) institutions better realise how they can contribute to health-creating or detracting processes and alter their practices to enhance the former; (ii) individuals and groups are better informed to find and help create health-producing assemblages, and know what they can do better within existing assemblages so that they can inform and pressure institutions in their aforementioned tasks. However, as McCormack alludes to, in undertaking any educational project health geographers need to be careful when advising on what to do and what not to do with respect to health, lest they end up providing yet more codes and orders (and hence mirroring social engineering strategies already employed in new public health practice). Perhaps then, as Duff proposes, health geographers might instead openly ‘play’ with such forces and powers, thinking about which ones can be used, which ones can be re-shaped or redirected, and which ones should be avoided. He suggests that, at the very least, as academics we need be more honest with ourselves and others about all types of assemblages and their outcomes and experiences, such as the benefits and pleasures of some ultimately health-degrading activities. This, he suggests, might lead to more informed debates.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.