
Abstract

Keywords
Migraine is one of the most disabling neurological disorders worldwide, despite the recent therapeutic breakthroughs achieved with receptor antagonists and monoclonal antibodies (mAbs) against calcitonin gene-related peptide (CGRP) signaling. A substantial proportion of patients either fail to respond to or lose the benefit from available treatments over time, underscoring the need to expand therapeutic horizons. Research in 2025 brought renewed momentum to the field, spotlighting several promising targets that might complement or surpass CGRP-directed strategies. Among these, pituitary adenylate cyclase-activating polypeptide (PACAP), substance P, vascular ATP-sensitive potassium (KATP) channels, transient receptor potential melastatin 3 (TRPM3) channels, and protease-activated receptor 2 (PAR2) stand out as particularly exciting avenues (Table 1).
Emerging migraine targets highlighted in 2025.
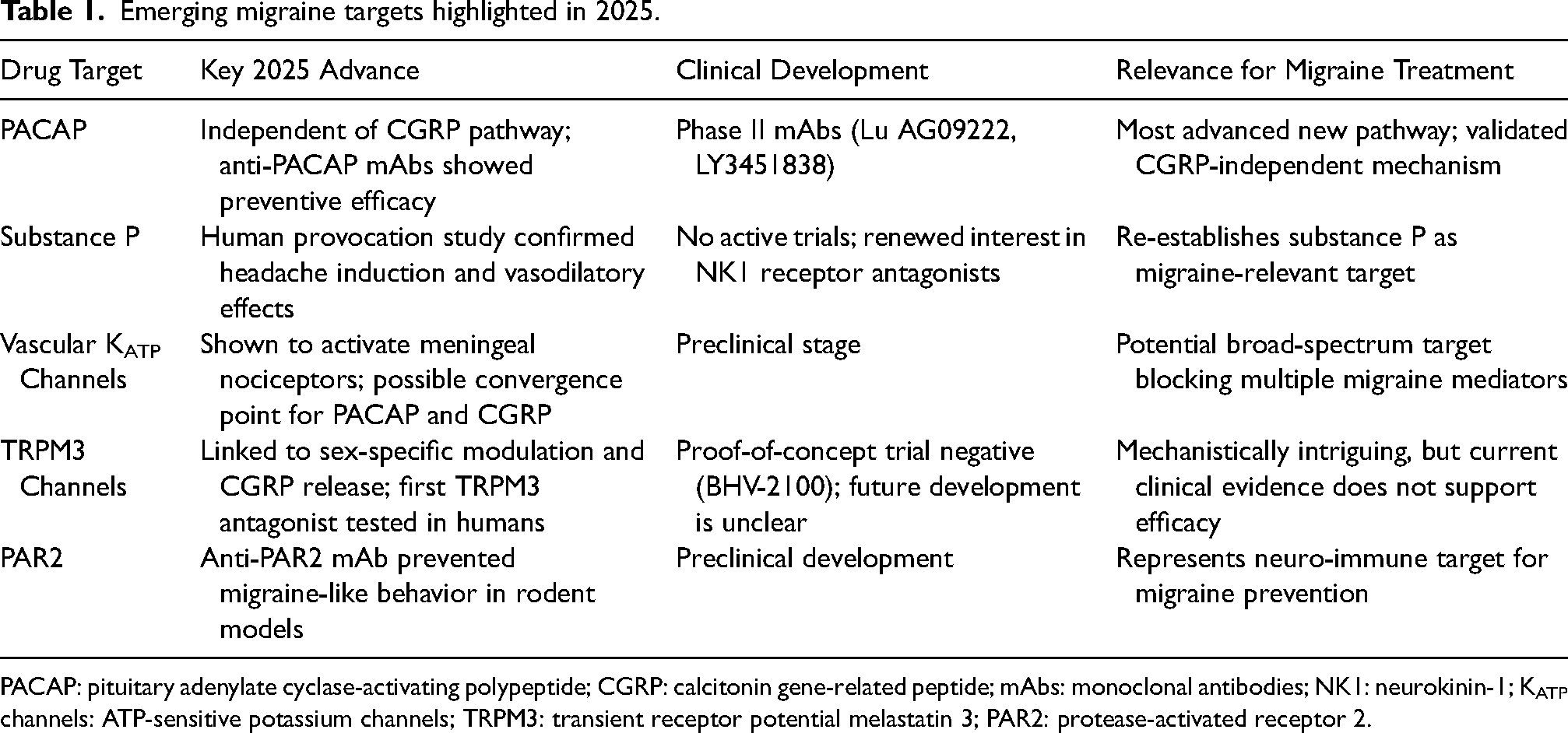
PACAP: pituitary adenylate cyclase-activating polypeptide; CGRP: calcitonin gene-related peptide; mAbs: monoclonal antibodies; NK1: neurokinin-1; KATP channels: ATP-sensitive potassium channels; TRPM3: transient receptor potential melastatin 3; PAR2: protease-activated receptor 2.
Pituitary adenylate cyclase-activating polypeptide: A new drug target is coming of age
Pituitary adenylate cyclase-activating polypeptide (PACAP) has long been recognized as a potent inducer of migraine attacks, but whether its migraine-producing effects are linked to CGRP has remained unclear. An important randomized placebo-controlled study showed that intravenous PACAP induces migraine attacks in people with migraine despite pre-treatment with eptinezumab, a mAb against the CGRP ligand (1). This finding established PACAP signaling as an independent migraine pathway, not merely a downstream branch of CGRP activity. Parallel advances on the therapeutic front confirmed the translational potential of targeting PACAP signaling. The HOPE trial, published in late 2024, showed that Lu AG09222, a mAb against the PACAP ligand, significantly reduced monthly migraine days compared with placebo (2). Using a similar approach, Johnson et al. reported early clinical evaluation of LY3451838, another mAb against the PACAP ligand (3). While efficacy signals in this very small, treatment-resistant migraine population did not reach statistical significance, the observed trends in monthly migraine-day reduction are encouraging and support further evaluation in larger, adequately powered trials.
Mechanistically, these clinical observations are supported by preclinical evidence pointing to a peripheral site of action for PACAP in migraine. Christensen and colleagues showed that PACAP-38 activates and sensitizes meningeal nociceptors, supporting the notion that PACAP can initiate migraine-relevant signaling outside the central nervous system (4). Together, these mechanistic and clinical findings reinforce PACAP as an independent and therapeutically actionable migraine pathway.
Substance P: Perhaps back on the clinical map
Substance P, an early neuropeptide candidate in the trigeminovascular hypothesis of migraine, resurfaced in 2025 as a validated human headache trigger. Al-Khazali et al. demonstrated in a controlled provocation study that intravenous infusion of substance P induces headache and arterial dilation in healthy adults (5). Although clinical development of substance-P–targeted treatments was abandoned in the early 2000s, this work reopens the discussion on therapeutically modulating substance P signaling. As recently reviewed (6), the new provocation data suggest that trial design, patient selection, or the specific receptor targeted could explain past failures and support renewed interest in substance P as a migraine contributor.
Vascular ATP-sensitive potassium channels: A unifying mechanistic pathway
Another major advance came from studies of vascular ATP-sensitive potassium (KATP) channels, which appear to act as downstream effectors for several migraine triggers. Christensen et al. showed that the vascular KATP channel opener levcromakalim directly activates and sensitizes meningeal nociceptors (7). Importantly, both CGRP- and PACAP-induced migraine attacks have been linked to vascular KATP opening, suggesting this ion channel might serve as a convergence point for diverse upstream mediators.
The therapeutic implications are substantial. Selective vascular KATP channel blockers could, in theory, prevent the headache-inducing effects of both CGRP and PACAP, offering a broader mechanism than current therapies. Although clinical development remains in its infancy, vascular KATP channels represent one of the most compelling mechanistic targets to emerge in recent years.
Transient receptor potential melastatin 3: Toward possibly sex-specific therapeutics
Transient receptor potential melastatin 3 (TRPM3) channels attracted growing attention in 2025 for their unique role at the intersection of migraine biology and sex differences. TRPM3 channels are expressed on trigeminal neurons and can be directly modulated by sex hormones and steroids (8). Estrogen and progesterone act as endogenous inhibitors, while pregnenolone sulfate serves as an agonist. This sexually dimorphic regulation could help explain the higher prevalence and severity of migraine in women, particularly around menses.
Reducha et al. provided compelling mechanistic evidence linking TRPM3 activation to migraine-relevant neuropeptide release (8). Using ex vivo and in vivo approaches, the authors demonstrated that stimulation of TRPM3 channels triggered CGRP release from the trigeminal ganglia and dura mater of both male and female rats, with some data suggesting enhanced release in female tissues. Immunohistochemistry confirmed colocalization of TRPM3 and CGRP in trigeminal neurons and dural fibers, as well as TRPM3 expression in vascular smooth muscle cells of the middle meningeal and cerebral arteries. Myograph experiments showed that TRPM3 activation caused arterial vasodilation, even in the presence of CGRP neutralization with fremanezumab, suggesting a CGRP-independent vascular component of TRPM3 signaling.
However, an investor presentation from Biohaven reported that the proof-of-concept trial of BHV-2100 (TRPM3 antagonist) for the acute treatment of migraine did not demonstrate an efficacy signal. Because key parameters—including sample size, treatment arms, randomization, and patient characteristics—were not disclosed, interpretation remains limited. Additional details will be essential before firm conclusions can be drawn.
Protease-activated receptor 2: targeting neuro-immune crosstalk
Neuro-immune interactions also came into sharper focus in 2025 with the identification of protease-activated receptor 2 (PAR2) as a potential therapeutic target. Kopruszinski et al. reported that MEDI0618, a mAb against PAR2, prevented migraine-like behaviors across multiple rodent models (9). Importantly, this efficacy extended beyond CGRP inhibition, suggesting that PAR2 blockade might benefit patients who do not respond to existing therapies. At a mechanistic level, PAR2 is a G-protein–coupled receptor that is activated by cleavage of its extracellular N-terminus by endogenous and exogenous serine proteases, including mast cell–derived tryptase, trypsin, and coagulation-related proteases, thereby engaging multiple inflammatory and nociceptive signaling pathways. Consistent with this mode of activation, PAR2 is expressed on trigeminal neurons, dural fibroblasts, endothelial cells, and mast cells, placing it at a key interface between nociception and inflammation. In line with this anatomical distribution, preclinical studies further demonstrate that PAR2 activation within the meninges can trigger migraine-like behavior in rodents (10). This meningeal localization, together with its protease-driven activation, makes mAb-mediated PAR2 blockade particularly compelling, enabling inhibition of the receptor exactly where migraine-relevant signaling is initiated. Together, these findings not only broaden the therapeutic landscape but also highlight the relevance of immune-mediated mechanisms in migraine pathophysiology.
Conclusions
The year 2025 delivered important progress in diversifying the therapeutic landscape for migraine. PACAP emerged as the most clinically advanced new pathway, now validated as a CGRP-independent driver and supported by early preventive efficacy in the HOPE trial. Substance P returned to the field after confirmation as a human headache trigger, prompting renewed consideration of its therapeutic potential. Evidence for vascular KATP channels was strengthened, positioning them as a possible unifying pathway for multiple migraine mediators. Meanwhile, TRPM3 and PAR2 introduced mechanistically distinct targets with early translational promise. Together, these discoveries point toward a future in which migraine therapy becomes increasingly mechanism-based, offering new hope for patients who remain underserved by current treatments.
Footnotes
Author contributions
Conceptualization: H.A., K.A.H.
Writing – Original Draft: H.A.
Writing – Review & Editing: H.A., K.A.H.
Data availability statement
Upon reasonable request, the corresponding author will provide the necessary data and materials to interested researchers for the purpose of academic scrutiny, reproducibility, and further scientific investigation.
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: K.A.H. has received a research grant from Lundbeck Foundation for projects unrelated to this research paper. K.A.H. is an Editorial Board Member of The Journal of Headache and Pain. H.A. has received personal fees from AbbVie, Lundbeck, Pfizer, and Teva, outside of the submitted work. H.A. has received research grants from Hartmann Foundation, Lundbeck Foundation, and Rigshospitalet Research Council for projects unrelated to this research paper. H.A. is an Editorial Board Member of The Journal of Headache and Pain.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Funding was provided by the Lundbeck Foundation (R403-2022-1352 to H.A. and R345-2020-1977 to K.A.H). The funding sources were not involved in the design or conduct of the study; in the collection, analysis, or interpretation of the data; or in the preparation, review, or approval of the manuscript.
Lundbeck Foundation, (grant number R345-2020-1977, R403-2022-1352 ).