
Abstract
Aim
Calcitonin gene-related peptide (CGRP), vasoactive intestinal peptide (VIP) and pituitary adenylate cyclase-activating peptide (PACAP) play a crucial role in migraine pathophysiology. In recent years, anti-CGRP(R) monoclonal antibodies (mAbs) have emerged as the first targeted and highly effective therapy for migraine. This study aimed to assess any changes in plasma CGRP levels following prophylactic treatment with anti-CGRP(R) mAbs and to compare CGRP dynamics between anti-receptor (erenumab) and anti-ligand (galcanezumab, fremanezumab) therapies. Secondary objectives were: (i) to evaluate changes in VIP and PACAP plasma levels following treatment with anti-CGRP(R) mAbs and (ii) to investigate whether baseline or post-treatment plasma levels of CGRP, VIP and PACAP were associated with clinical response to anti-CGRP(R) monoclonal antibody therapy.
Methods
Between February 2022 and February 2023, we enrolled 56 migraine patients who initiated prophylaxis with either erenumab (26 patients), galcanezumab (16 patients) or fremanezumab (14 patients). Responders were defined as those achieving a ≥50% reduction in monthly migraine days after six months. Blood samples were collected at baseline and at each follow-up visit (baseline, T0; three months, T1; six months, T2; 12 months, T3). Plasma levels of CGRP, VIP and PACAP were measured using a validated radioimmunoassay and commercially available enzyme-linked immunosorbent assay kits.
Results
Overall, 80.3% (45 out of 56) of patients responded to anti-CGRP(R) mAbs. No correlation was found between baseline CGRP, VIP and PACAP plasma levels and clinical response to anti-CGRP(R) mAbs therapy. Regarding CGRP trend, significant differences were found between patients treated with the anti-receptor monoclonal antibody (erenumab) and those receiving anti-ligand therapies. In patients treated with erenumab, CGRP levels did not show a significant change over the treatment period (T1–T3), whereas, in the galcanezumab group, CGRP levels significantly decreased as early as T1 (p < 0.01). CGRP longitudinal assessment of the fremanezumab group were excluded due to assay interference with the drug. VIP and PACAP plasma levels remained stable over time for all treatments, with no significant differences between responders and non-responders.
Conclusions
Galcanezumab reduced CGRP plasmatic levels already after three months, whereas erenumab did not affect significantly CGRP plasmatic levels. VIP and PACAP levels were not influenced by the therapy.
This is a visual representation of the abstract.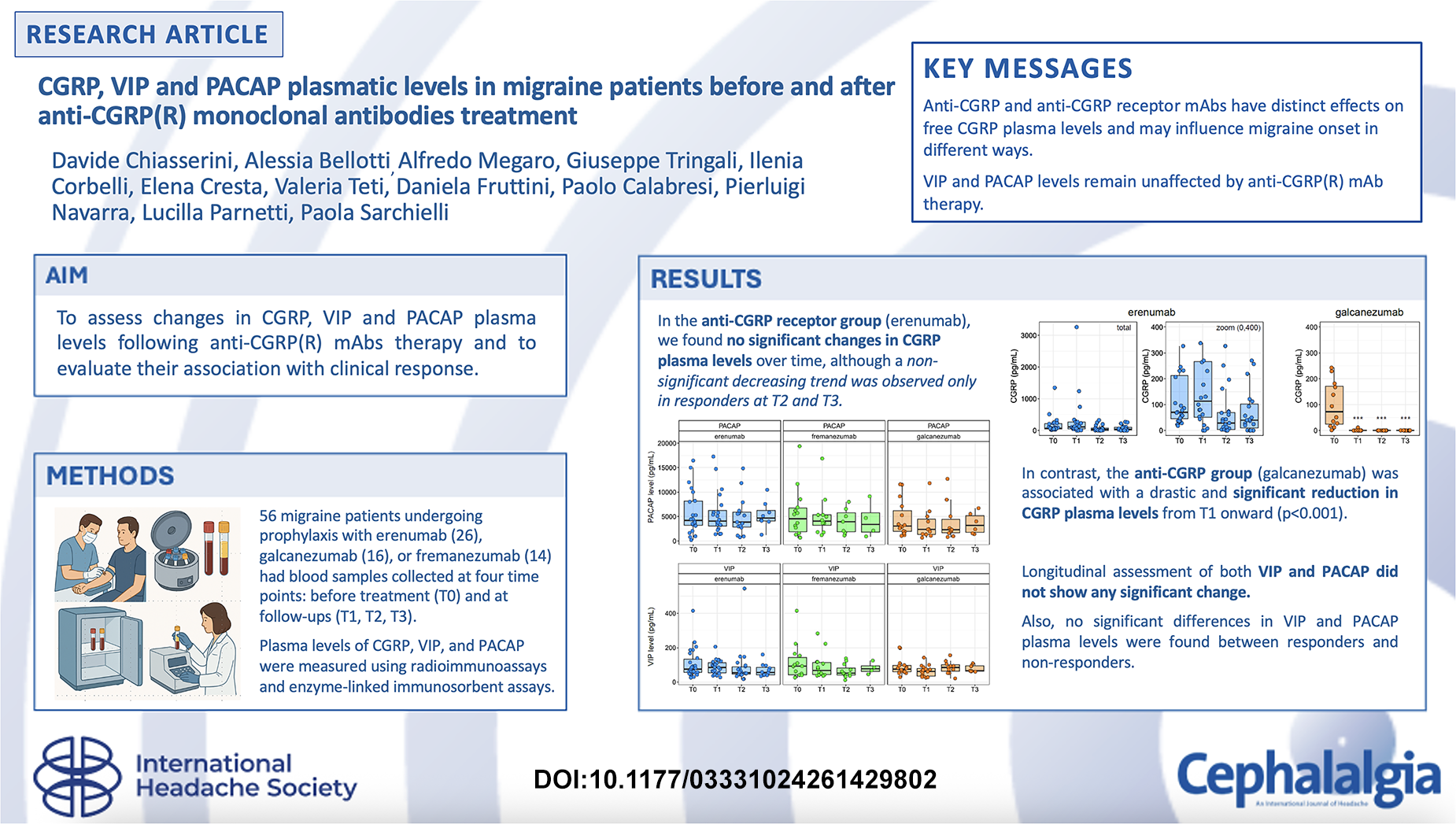
Introduction
Recent evidence highlights the role of calcitonin gene-related peptide (CGRP), vasoactive intestinal peptide (VIP) and pituitary adenylate cyclase-activating peptide (PACAP), in both migraine initiation and maintenance.1–3 VIP and PACAP exhibit potent vasodilatory effects, with PACAP also promoting trigeminal sensitization.4,5 When acting on meningeal afferent fibres, PACAP induces CGRP release in the caudal trigeminal nucleus (TNC). 6 Elevated PACAP levels in peripheral and jugular blood during both ictal and interictal phases further support its role in migraine pathogenesis.7,8 Additionally, PACAP infusion triggers headache attacks with migraine-like characteristics. 9 Similarly, increased VIP levels have been detected in chronic migraine patients, 10 and higher VIP levels correlate with greater efficacy of onabotulinumtoxinA prophylaxis, even in individuals with low CGRP plasma levels. 11 Several studies have demonstrated elevated CGRP levels in jugular venous blood during migraine attacks, both with and without aura.12,13 Furthermore, CGRP concentrations are higher in peripheral blood and saliva of migraine patients compared to healthy controls, in both ictal and interictal phases.14,15 Although multiple neuropeptides contribute to migraine pathophysiology, CGRP plays a pivotal role in headache initiation and persistence, as evidenced by the clinical efficacy of anti-CGRP ligand (galcanezumab, fremanezumab and eptinezumab) and anti-CGRP receptor (erenumab) monoclonal antibodies (hereinafter referred to together as anti-CGP(R)).16,17 These treatments reduce attack frequency, intensity and duration, often reversing chronic headache and medication overuse. 18 Given this, assessing plasma levels of key neuropeptides (CGRP, PACAP and VIP) in patients undergoing these novel prophylactic therapies is essential to fully understand their pharmacological mechanism of action. However, no longitudinal studies have yet investigated changes in CGRP, VIP and PACAP levels following monoclonal antibody treatment. Therefore, the primary aim of this study was to assess changes in plasma CGRP levels following prophylactic treatment with anti-CGRP(R) monoclonal antibodies and to compare CGRP dynamics between anti-receptor (erenumab) and anti-ligand (galcanezumab, fremanezumab) therapies. Secondary objectives were to evaluate changes in VIP and PACAP plasma levels following treatment with anti-CGRP(R) monoclonal antibodies and to investigate whether baseline or post-treatment plasma levels of CGRP, VIP and PACAP were associated with the clinical response.
Methods
Study design and procedures
Our prospective observational study took place at the Headache Centre of S. Maria of Misericordia Hospital in Perugia over a 24-month period. From February 2022 to February 2023, we enrolled 56 patients with migraine who were scheduled to begin prophylactic therapy with one of the three subcutaneous anti-CGRP(R) monoclonal antibodies available in Italy: erenumab, galcanezumab, or fremanezumab. These medications were prescribed in accordance with the Italian Medicines Agency (AIFA) criteria. Given the observational design of the study, patients were not randomized to a specific treatment arm (erenumab, galcanezumab or fremanezumab). Instead, individuals consecutively prescribed one of these monoclonal antibodies in real-life clinical practice were enrolled, allowing blood sampling to be performed before treatment initiation.
We therefore enrolled subjects of both sexes aged between 18 and 65 years suffering from one of the following headache forms:
- Episodic migraine with or without aura (International Classification of Headache Disorders, 3rd edition (ICHD-3) criteria)
19
who had reported at least eight days of migraine per month in the previous three months (high frequency episodic migraine). - Chronic migraine with or without medication-overuse headache (ICHD-3 criteria). - Positive history of other neurological disorders (the presence of a previous or concomitant tension headache was permitted; other types of headaches, such as cluster headache, were also excluded). - Positive history of cardiovascular disease (arterial hypertension, myocardial infarction, ischaemic and haemorrhagic stroke, and atrial fibrillation, which is a contraindication to anti-CGRP monoclonal antibody therapy), respiratory (including asthma), endocrinological, nephrological, autoimmune and psychiatric (except mood disorders) disease. - Ongoing infections or systemic inflammatory states, pregnancy, post-partum and breastfeeding period, tobacco habit. - Previous administration of CGRP antagonist monoclonal antibody therapy.
Exclusion criteria were:
Patients were assessed at enrolment (T0), and then at three (T1), six (T2) and 12 months (T3) after starting anti-CGRP(R) mAbs prophylaxis. During the clinical evaluation at the Headache Centre, clinical data were collected for each patient on age, sex, weight, height, blood pressure, onset of headache (years of illness), symptomatic drugs used as needed and prophylactic drugs (timing of use, dosage, any side effects, effectiveness). At each time point of the study (T0, T1, T2 and T3) headache characteristics (frequency, intensity and migraine features), consumption of symptomatic drugs averaged over the previous three months (number of doses of triptans, non-steroidal anti-inflammatory drugs, paracetamol and combination drugs, etc.) and any treatment-related adverse events were recorded. Ongoing migraine prophylactic treatments were continued throughout the study period without modifications to avoid confounding effects on efficacy and neuropeptide levels as a result of other therapeutic modifications Specific scales were administered to assess the severity of migraine, associated disability and the possible presence of allodynia and insomnia:
To be responders to treatment, patients should have a reduction of at least 50% of migraine days per month (MMDs) after six months of treatment. Throughout the treatment year, patients had four blood samples taken during follow-up visits for the renewal of their treatment plans.
Outcomes
Primary outcome
Variation in plasma CGRP levels before and during prophylactic treatment with anti-CGRP(R) monoclonal antibodies, with comparison of CGRP dynamics between anti-receptor (erenumab) and anti-ligand (galcanezumab, fremanezumab) therapies.
Secondary outcomes
Variation in plasma VIP and PACAP levels following treatment with anti-CGRP(R) monoclonal antibodies.
Association between plasma levels trend of CGRP, VIP, and PACAP and clinical response to therapy.
Sample size/power
Based on previous studies,24,25 we assumed a paired pre–post effect size for CGRP of ∼0.5 (Cohen's dz). With two-sided α = 0.05 and 80% power, the required sample for a paired analysis is approximately 28 patients. We enrolled 56, which provides >80% power to detect within-patient changes as small as dz ≈ 0.37.
For the between-group comparison of change (anti-receptor erenumab n = 26 vs. anti-ligand – galcanezumab/fremanezumab – n = 30), with the same α and power the study is powered to detect a standardized difference in mean change of approximately 0.75.
Sample collection
To evaluate baseline plasma levels and treatment-related trends of the neuropeptides CGRP, VIP and PACAP, plasma samples from 56 patients were analysed at four time points. All patients were tested from T0 to T2, whereas 47 out of 56 were also tested at T3, resulting in a total of 215 plasma samples. All patients were assessed in the interictal period before the start of treatment with mAbs (T0), at three months (T1), six months (T2) and 12 months (T3) after the start of treatment (between days 7 and 14 after drug inoculation). To minimize interference as a result of the use of symptomatic medication, patients (including those with chronic conditions) were asked to attend on the available mornings for blood sampling only if they had not experienced a migraine attack in the previous 24 hours and had not taken any acute treatment during the same period. Migraine patients underwent peripheral venous blood sampling (median cubital vein or forearm cephalic vein) of two 6-ml EDTA blood tubes (BD Vacutainer® EDTA Tubes, code: 367839; BD, Franklin Lakes, NJ, USA) on pre-established days, presenting themselves in the morning, on an empty stomach, from 8.30 to 9.30 a.m. at the Headache Centre outpatient clinic. Immediately after collection, the samples were processed accordingly to previously published procedures 26 at the Neurochemistry Laboratory, University of Perugia. Briefly, blood samples were centrifuged for 10 minutes at 2000 × g (room temperature), and then the supernatant (plasma) was collected and stored in 0.5-mL tubes (72.730.007; Sarstedt AG & Co., Numbrecht, Germany) and immediately frozen at −8° C, pending analyses.
The study was carried out in compliance with the guidelines of good clinical practice (Ministerial Decree of 15/07/97, Legislative Decree 200/2007), the Declaration of Helsinki and all current legislation on pharmacological studies. The study was approved by the Regional Ethics Committee (CER) of Umbria, registered under number 4219/22. All patients provided their informed consent for use of biological samples.
Biomarker measurements
For plasma CGRP measurement, we used a radioimmunoassay (RIA) technique previously validated in our laboratory 27 with modifications. Our assay uses an antiserum raised against the full human form of α-CGRP 1-37 (hα-CGRP) and recognizes an epitope within the central region of the peptide. The assay is not specific for the full CGRP form but may recognize also CGRP fragments. One hundred microlitres of plasma from each patient were taken for the determination of CGRP levels, after thawing and gentle vortexing of the sample. Separation of free from bound α-CGRP was performed by double-antibody technique combined with polyethylene, and the pellet was counted in a γ-counter. All samples and standards were assayed in duplicate. CGRP levels were determined by comparison with a standard curve ranging from 1.95 to 1000 pg/mL hα-CGRP and using a four-parameter logistic curve. Samples showing values above the upper limit of the curve were extrapolated via software. CGRP concentrations were expressed as pg/ml.
To estimate the possible interference of galcanezumab and fremanezumab with the RIA, increasing concentrations of both drugs were tested in the RIA assay. Interference with the assay was expressed as percentage binding (%B/B0), representing the percentage of radiolabeled antigen (CGRP) that is bound to the antibody (B), relative to the initial count in the absence of unlabeled antigen (B0). Values of %B/B0 lower than 100% mean that the antibody interferes with the assay and the interference is “read” by the assay as additional CGRP present in the tube. Commercially available enzyme-linked immunosorbent assays (ELISA) were used for measuring VIP and PACAP-38 (from now on PACAP) plasma values (Biomatik, Kitchener, ON, Canada; PACAP-38 Cat#EKF59217, VIP Cat# EKU08113), in accordance with the manufacturer;s instructions. To assess the dilutions for VIP and PACAP, we performed pilot experiments using pooled plasma samples with the assay diluents included in the kits. The best dilutions to read the samples within the linear part of the standard curves suggested by the manufacturers were 1:20 for PACAP and 1:2 for VIP. The final concentration values were recalculated according to the dilution factor. Lower limit of detection for PACAP was 4.7 pg/ml, whereas that for VIP was 2.63 pg/ml. All of the samples were measured in a blinded fashion.
Statistical analysis
Statistical analysis was performed with SPSS, version 25.0.0 (IBM Corp., Armonk, NY, USA) and R, version 4.2.3 (R Foundation, Vienna, Austria). We summarized all variables of interest using frequencies and percentages for categorical variables, mean and standard deviation or median and interquartile range for numerical variables. The Kolmogorov–Smirnov test was used to determine whether the data were normally distributed. For longitudinal analysis of migraine scales and biomarkers data, a mixed model approach using age and sex as covariates was used (R package lme4). (28) Pairwise comparisons for each time point were performed with the estimated marginal means method (R package emmeans)29, using the Benjamini–Hochberg method for multiple comparison correction. For comparisons between two groups, a t-test or the Mann–Whitney test were used when appropriate. For multiple group comparisons, one-way analysis of variance or the Kruskal–Wallis test was used. Post-hoc comparisons were made with Tukey;s test or Dunn's test. For analysis of CGRP data, imputation to minimum value (0) was used for samples that showed quantifiable values at T1; patients with non-measurable CGRP values at baseline were excluded from the CGRP analysis. For qualitative data, the chi-square test was used. p < 0.05 was considered statistically significant.
Results
Clinical features of the cohort and effect of anti-CGRP(R) monoclonal antibody treatment on migraine scales
The clinical characteristics of the patients are displayed in Table 1. Of the 61 patients who initially met the study inclusion criteria at the time of monoclonal antibody prescription, five subsequently declined to undergo follow-up blood sampling and were therefore excluded from the final analyses of the study. Of the 56 patients included in the final analysis, 50 were females (89.3%), 36 had a diagnosis of chronic migraine, 20 patients had episodic high-frequency migraine and eight patients also had episodes of migraine with aura. Concerning concomitant prophylactic therapies, 33 out of 56 patients (58.9%) were receiving additional migraine prophylactic treatments. Specifically, 11 patients were treated with amitriptyline, 19 with propranolol, 18 with topiramate and 13 with venlafaxine or a selective serotonin reuptake inhibitor. These prophylactic regimens were maintained unchanged throughout the one-year treatment period with the anti-CGRP(R) monoclonal antibody. In relation to mAbs treatment: 26 patients had been prescribed prophylaxis therapy with erenumab (46.4%), 16 with galcanezumab (28.5%) and 14 with fremanezumab (25.0%).
Clinical variables of all patients at T0 and according to the treatment group.

MMDs = monthly migraine days; MIDAS = Migraine Disability Assessment Test; ASC = Allodynia Symptom Score; HIT-6 = Headache Impact Test-6; ISI = Insomnia Severity Index. Values are presented as the mean ± SD. The last column displays the overall p-value across treatment groups, calculated using analysis of variance or the Kruskal–Wallis test where appropriate. *p < 0.05.
At baseline, the three treatment groups were homogeneous in terms of clinical characteristics (age, sex, disease duration, number of previous failed prophylactic treatments and scores on MIDAS, HIT-6, ASC and ISI), except for monthly migraine days (MMDs), which were higher in the erenumab group (17.5 MMDs vs. 14.1 in the fremanezumab group and 14.2 in the galcanezumab group; p < 0.05). Post-hoc analysis for MMDs did not show significant differences across treatment groups (data not shown). Overall, after six months of anti-CGRP(R) mAb therapy (T2), 45 out of 56 patients (80.3%) responded to prophylaxis, showing a statistically significant reduction in MMDs and migraine severity scores (Figure 1; see also Supporting material, Table S1). The decrease in MMDs was already evident at T1 (−9.4 MMDs, SD = 4.0; p < 0.001).

Trend of MMDs, MIDAS, HIT-6 and ASC scores from T0 to T3 across treatments groups. Solid line represents the mean trend across time points while shaded grey areas are 95% confidence intervals (CIs). Numbers on the x-axis represent the four time points. Values at three months (T1), six months (T2) and 12 months (T3) in all the scales were significantly different from T0 (p < 0.001, a complete analysis is reported in the Supplementary material, Table S1). MMDs = monthly migraine days, MIDAS = Migraine Disability Assessment Test; ASC = Allodynia Symptom Score; HIT-6 = Headache Impact Test-6; ISI = Insomnia severity index.
Among the non-responders, nine patients discontinued therapy after six months (T2) due to lack of efficacy (reduction in MMDs <30%), while three patients (5.3%) continued therapy for a subjective benefit, defined as a reduction in MMDs between 30% and 40%.
Regarding the responder rates across the three treatment groups, 18 out of 26 patients (69.2%) responded in the erenumab group, 14 out of 16 patients (87.5%) in the galcanezumab group and 13 out of 14 patients (92.8%) in the fremanezumab group.
In all three treatment groups, we observed a significant reduction in MIDAS (from 110.1 ± 34.8 at T0 to 29.7 ± 23.4 at T2; p < 0.0001), HIT-6 (from 69 ± 5.6 at T0 to 52.5 ± 9.9 at T2; p < 0.0001), ASC (from 7.6 ± 4.2 at T0 to 2.7 ± 3.4 at T2; p < 0.0001) and ISI (from 8.2 ± 5.8 at T0 to 4.1 ± 4.2 at T2;p < 0.0001) (see Supplementary material, Table S1).
Regarding adverse events, five patients (8.9%) reported constipation, two patients (3.5%) experienced an increase in the frequency of visual aura episodes and 10 patients (17.8%) developed respiratory tract infections during treatment, four of whom were infected with SARS-CoV-2. No patients reported serious side effects and no patient experienced an increase in blood pressure during treatment.
Effect of anti-CGRP(R) monoclonal antibody treatment on neuropeptides plasma levels
Baseline (T0) concentrations of the neuropeptides CGRP, VIP and PACAP did not differ among the three treatment groups (see Supplementary material, Table S2).
No significant differences in CGRP, VIP and PACAP plasma levels were observed between responders and non-responders at baseline (data not shown).
We then analysed CGRP, VIP and PACAP plasma levels at different time points across the treatment groups. First, to ensure the reliability of plasma CGRP measurements, interference testing was performed for fremanezumab and galcanezumab, the mAbs directly targeting CGRP. In this experiment, increasing concentrations of the antibody were spiked into the assay matrix and the resulting change in signal was compared with an antibody-free control, calculating the binding percentage (%B/B0), which is representative of the unspecific binding due to the competition between the antibodies (drug and RIA antibody). Our analysis confirmed a substantial interference of fremanezumab starting from concentrations of approximately 10 μg/ml onward (see Supplementary material, Figure S1A and Table S3). This concentration range can be reached in vivo during treatment. 30 We concluded that the amounts of fremanezumab present in plasma samples of the patients can interfere with the RIA assay used in this work. Therefore, CGRP data from fremanezumab patients were excluded from further analyses. On the other hand, the amounts of galcanezumab present in plasma did not interfere with the assay, since they were below the threshold of potential cross-reactivity (i.e. 39 pg/ml) (see Supplementary material, Figure S1B). We therefore limited the analysis to erenumab an galcanezumab treated patients (Figure 2). All plasma samples with VIP and PACAP values above within quantification limits were included in the final analysis.
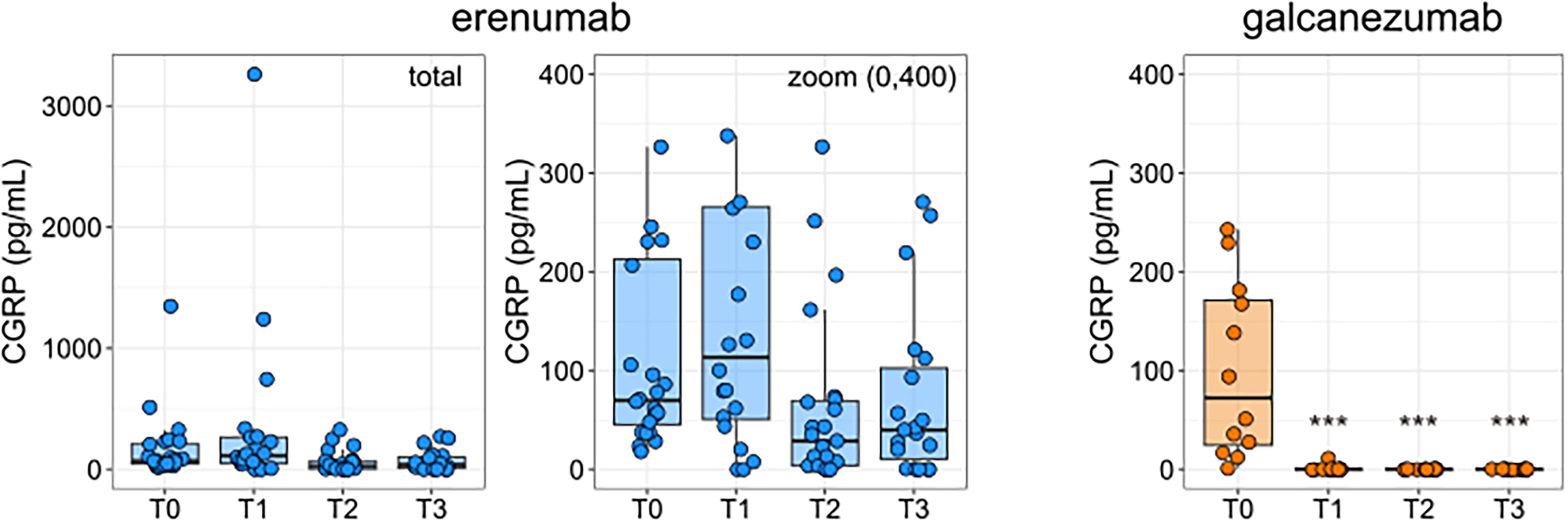
Longitudinal calcitonin gene-related peptide (CGRP) biomarker levels in erenumab and galcanezumab-treated patients. The plasma levels of CGRP across the four time points are represented for the patients who underwent treatment with erenumab (left and middle) and galcanezumab (right). For the erenumab group, the plot on the left represents the total data with outliers, while the plot on the right represents a zoomed version between 0 and 400 pg/ml for comparison with the galcanezumab group. Box plots are described by median (solid black line) and 25–75% percentiles. Dots are representative of single patient data for each analyte. Peptide quantity is expressed as pg/ml (y-axis), while the time points are represented on the x-axis (T0–T3). ***p < 0.001 against T0 (mixed model; see Methods).
In patients treated with erenumab, CGRP plasmatic levels did not change significantly across the four time points (Figure 2; see also Supplementary material, Table S2).
Splitting the patients according to treatment response (18 erenumab responders vs. 8 non-responders) we found a decreasing trend in CGRP levels at T2 and T3 in responders (−60% at T2 and −42% at T3 on average) which, however, was not statistically significant; in non-responders, CGRP levels remained essentially unchanged between T0 and T3 (data not shown).
In the galcanezumab group, we found a significant CGRP reduction starting at T1 (p < 0.001), with plasma values of CGRP becoming undetectable according to the limit of detection of our RIA assay (Figure 2). In this group, only two out of 16 patients (12.5%) were classified as non-responders, precluding a meaningful comparison of CGRP levels between responders and non-responders.
Longitudinal assessment of both VIP and PACAP did not show any significant change in the levels of the two neuropeptides during the whole length of the treatment with any of the antibodies (Figure 3). Also, no significant longitudinal differences in VIP and PACAP plasma levels were found between responders and non-responders (data not shown).
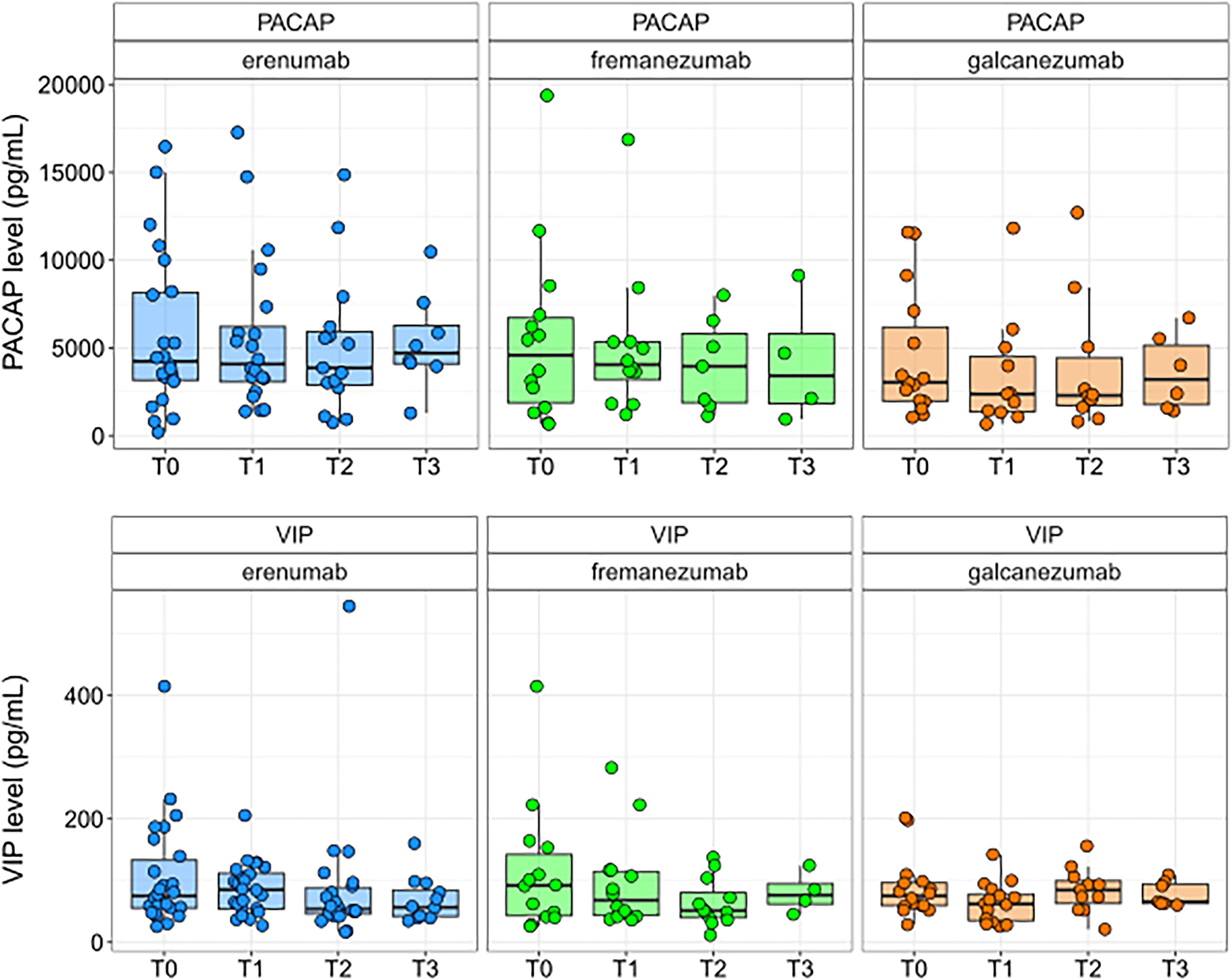
Longitudinal levels of vasoactive intestinal peptide (VIP) and pituitary adenylate cyclase-activating peptide (PACAP) across treatment groups. The plasma levels of VIP and PACAP across the four time points are represented for the patients who underwent treatment with erenumab, fremanezumab and galcanezumab. Box plots are described by median (solid black line) and 25–75% percentiles (boxes). Dots are representative of single patient data for each analyte. Peptide quantity is expressed as pg/ml (y-axis), while the time points are represented on the x-axis (T0–T3).
Discussion
In the present study, we have analysed the plasma level of the three main neuropeptides implicated in the pathophysiology of migraine, CGRP, VIP and PACAP, in patients treated with anti-CGRP(R) monoclonal antibodies. To our knowledge, this is the first longitudinal study to assess the levels of all the three neuropeptides in patients undergoing treatment with both anti-ligand antibodies (galcanezumab and fremanezumab) and anti-receptor antibody (erenumab) over an extended period of time (12 months). This approach addresses the limitations of previous studies,24,25 which relied on one or two follow-up time points, typically restricted to three or six months, despite the considerable variability in neuropeptide levels observed both between individuals and within the same patient over time.
As widely reported in the literature, anti-CGRP monoclonal antibodies represent highly effective therapies for migraine prevention, with a 70–75% response rate after six months of treatment.31,32 The responder rate observed in our cohort (80.3% after six months of treatment) is slightly higher than that generally reported in real-world studies, particularly those including patients with high-frequency episodic and chronic migraine. This difference may be attributable to the relatively small sample size and to selection bias resulting from the strict inclusion criteria. In particular, patients with relevant cardiovascular, autoimmune or psychiatric comorbidities, as well as smokers, were excluded, as these factors could have confounded the analysis of plasma CGRP, VIP and PACAP levels.33,34 Moreover, the analysis was conducted on a per-protocol population: although a larger number of patients were initially screened (n = 61), only 56 participants completed follow-up and were included in the final analysis. It cannot be excluded that non-responders were more likely to discontinue treatment or decline blood sampling, potentially leading to an overestimation of treatment effectiveness. Longitudinal analysis of CGRP plasma concentrations demonstrated stability of CGRP levels over time in the erenumab-treated group, with no statistically significant variations observed across the four evaluated time points. When the population was divided according to response rate, we observed a non-significant downward trend in CGRP levels in erenumab responders compared to non-responders. However, the number of patients in this subgroup analysis was small, precluding a comprehensive analysis of the CGRP levels according to the response rate. In agreement with our results, a previous study did not show significant changes in CGRP levels after six months of erenumab therapy, 24 whereas two more recent studies using ELISA immunnoassays found a reduction in CGRP levels in migraine patients after three months and six months of erenumab prophylaxis.25,35 The CGRP reduction was associated with a decrease in MMDs more evident in chronic patients who have become episodic; in one of these studies, we note that the concomitant use of botulinum toxin was also permitted. The discrepancy between these findings may be partially attributable to the different methods used. Given the absence of standardized guidelines for CGRP measurement and the recent publications discussing some commercially available ELISA immunoassays, 36 there is no universal consensus on which method is best for measuring CGRP, but it is possible that the RIA method, historically used in numerous CGRP quantification studies37–40 may offer greater consistency in the results.
Another recent study using a RIA method also did not found significant changes in CGRP serum levels after one month of erenumab treatment, but showed an association between lower CGRP plasma levels after the first erenumab injection and fewer migraine days per month after three months of treatment, highlighting the possible correlation with treatment response. 41
When considering its mechanism of action as a monoclonal antibody selectively targeting the CGRP receptor within the trigeminovascular system, it is plausible that erenumab exerts only a limited influence on circulating free CGRP levels. Nonetheless, considering the complex mechanisms mediated by CGRP, we cannot rule out the possibility that a reduction in plasma CGRP levels occur in responder patients transitioning from chronic to low-frequency episodic migraine. This reduction may reflect not a direct effect of erenumab, but rather a diminished continuous CGRP release driven by frequent migraine attacks. This observation is supported by research indicating that patients with chronic migraine have considerably higher CGRP levels compared to those with episodic migraine15,42,43 and that CGRP plasma levels may be reduced after treatment with onabotulinumtoxinA, 44 another therapy that we do not expect reduce directly plasma levels of this neuropeptide.
As hypothesized by other authors, although anti-CGRP(R) monoclonal antibodies are large molecules that can cross the blood–brain barrier only to a minimal extent, several neurophysiological and neuroimaging studies in treated patients have demonstrated an “upstream” central effect of these antibodies. In particular, erenumab appears to modulate the activation of specific brain areas in response to trigeminal nociceptive input, including the thalamus, the insular cortex and the secondary somatosensory cortex. 45 Moreover, a reduced activation of the hypothalamus has been observed exclusively in treatment responders. These findings support the hypothesis that anti-CGRP(R) monoclonal antibodies may not only reduce the levels of free circulating CGRP, but also may decrease its release, possibly through modulation of several interconnected central pathways within a complex regulatory system.
In patients treated with the anti-ligand monoclonal antibody galcanezumab, we found a clear and significant reduction in plasma CGRP levels as early as three months into treatment, with levels becoming largely undetectable by six months. This trend is consistent with the mechanism of action of galcanezumab, which directly binds CGRP, thereby markedly decreasing the free circulating fraction. This result is also supported by data from other studies.25,35 Similarly to erenumab, however, we cannot exclude a central upstream effect of galcanezumab, which might also regulate CGRP release. Central effects have been reported for galcanezumab as well, from both neurophysiological and neuroimaging perspectives. Some studies support the role of galcanezumab in acting on cortical targets located beyond the pain network, restoring abnormal occipital reactivity 46 and other data support a reduction in cortical thickness among responders after treatment, reflecting a reduced synaptic density of the nociceptive signalling over time. 47 These findings further support the concept that lowering the “allostatic load” associated with migraine may modulate multiple neural targets, with effects on the trigeminovascular system, thalamo-hypothalamic centers and cortex.
Overall, our findings suggest a differential modulation of free CGRP plasma levels between the anti-receptor antibody erenumab and the anti-ligand antibody galcanezumab, potentially reflecting similar but distinct mechanisms of action in migraine pathophysiology, both at the peripheral and central levels. This observation aligns with existing clinical evidence indicating that patients who do not respond to one class of CGRP-targeted monoclonal antibodies may benefit from switching to the other, supporting the hypothesis of non-overlapping therapeutic effects.48,49
In the present study, we also examined two additional neuropeptides implicated in migraine pathophysiology: VIP and PACAP. It is known that hypothalamic neurons regulate the firing of the parasympathetic superior salivary nucleus, which in turn stimulates the sphenopalatine ganglion to release acetylcholine, VIP and PACAP from its meningeal terminals.1–3 When applied to the meningeal afferent fibers, PACAP induces the release of CGRP in the caudal TNC, 6 supporting the idea that CGRP act downstream with respect to VIP and PACAP. These results are in line with our observations, where blockade of CGRP signalling via monoclonal antibodies did not result in measurable changes in peripheral concentrations of VIP and PACAP.
While preliminary, these findings may indicate that VIP- and PACAP-mediated pathways are not modulated by anti-CGRP therapies, and that targeting these alternative pathways could offer additional therapeutic options for non-responders. In this sense, the relationship between the CGRP and PACAP pathways in migraine genesis warrants further investigation, particularly with the development of new anti-PACAP antibodies for migraine treatment.50–53 Nevertheless, our findings also suggest that measuring VIP and PACAP plasma levels in interictal period may not be relevant for the identification of anti-CGRP(R) mAbs responders. This hypothesis seems to be supported by findings showing that PACAP rises primarily during the ictal phase, 54 while VIP increase is linked to autonomic symptoms and may reflect specific migraine attacks. 55 An interesting study also found that certain migraine attacks are not accompanied by an increase in salivary CGRP levels, supporting the hypothesis that some attacks may not be primarily CGRP-mediated. 56 To further dissect these mechanisms especially in anti-CGRP(R) mAbs non-responders, future studies should include measurements of CGRP, VIP and PACAP during migraine attacks, to identify potential PACAP- or VIP-mediated episodes that may otherwise remain unrecognized.
Despite the relevance of these findings, several limitations of the present study should be acknowledged. Measuring CGRP in biological fluid is still a challenge due to the scarcity of validated assays and lack of pre-analytical procedures. 57 Consistent with these methodological limitations, CGRP measurements obtained using our RIA method may reflect a mixture of full-length peptide and CGRP fragments, and, in some samples, concentration estimates relied on extrapolation, which may reduce precision. Development of new assays and standardized procedures for CGRP measurement in biological fluids is therefore urgently needed. Additionally, we have shown that in fremanezumab-treated patients, the RIA method had a significant interference from the drug, causing a very high increase of the CGRP signal. A similar effect might be present also in other studies, which observed elevated CGRP levels (>4000 pg/ml) following anti-CGRP monoclonal antibody therapy. 58 Another potential limitation is that plasma samples were analysed in series at the end of the collection period (after obtaining four samples per patient). Consequently, baseline (T0) samples had been stored at −80 °C for approximately 12 months before analysis, whereas samples collected at T3 were measured shortly after freezing. This time difference in storage may have affected the results, 57 particularly in the erenumab group. However, given that a clear reduction in CGRP levels across the four time-points was observed in the galcanezumab group, we consider it unlikely that this factor substantially influenced the overall findings.
Analytical limitations were presents also for VIP and PACAP measurements since we did not perform a complete in-house validation of the immunoassays and did not test the analytical specificity for the two analytes. Both peptides are produced after post-translational processing and are present in plasma and tissues under different forms of different length and origin.59,60 Despite the kits manufacturer ensuring no cross-reactivity with other peptides or cleavage products, our results for VIP and PACAP should be taken with caution and confirmed in future studies.
Finally, increasing the sample size could enable a reliable comparison between responders and non-responders, while assessing additional neuropeptides and inflammatory cytokines may provide further insights into migraine pathogenesis and predictors of response to anti-CGRP(R) monoclonal antibodies.
Conclusions
Our study highlights that anti-CGRP and anti-CGRP receptor mAbs may have distinct effects on free CGRP plasma levels and influence migraine onset in different ways. In contrast, VIP and PACAP levels remain unaffected by anti-CGRP(R) mAb therapy, paving the way for possible complementary therapies directed against these two neuropeptides. Future studies involving larger patient cohorts, measuring not only these three neuropeptides, but also other molecules involved in migraine pathophysiology, could provide further insight into the role of these biomarkers in clinical practice and treatment selection.
Clinical implications
Anti-CGRP and anti-CGRP receptor monoclonal antibodies exert distinct effects on free CGRP plasma levels and may modulate migraine pathophysiology through different mechanisms.
Plasma levels of PACAP and VIP did not appear to be influenced by anti-CGRP(R) mAbs therapy, suggesting different pathways.
Supplemental Material
sj-docx-1-cep-10.1177_03331024261429802 - Supplemental material for CGRP, VIP and PACAP plasmatic levels in migraine patients before and after anti-CGRP(R) monoclonal antibodies treatment
Supplemental material, sj-docx-1-cep-10.1177_03331024261429802 for CGRP, VIP and PACAP plasmatic levels in migraine patients before and after anti-CGRP(R) monoclonal antibodies treatment by Davide Chiasserini, Alessia Bellotti, Alfredo Megaro, Giuseppe Tringali, Ilenia Corbelli, Elena Cresta, Valeria Teti, Daniela Fruttini, Paolo Calabresi, Pierluigi Navarra, Lucilla Parnetti and Paola Sarchielli in Cephalalgia
Supplemental Material
sj-docx-2-cep-10.1177_03331024261429802 - Supplemental material for CGRP, VIP and PACAP plasmatic levels in migraine patients before and after anti-CGRP(R) monoclonal antibodies treatment
Supplemental material, sj-docx-2-cep-10.1177_03331024261429802 for CGRP, VIP and PACAP plasmatic levels in migraine patients before and after anti-CGRP(R) monoclonal antibodies treatment by Davide Chiasserini, Alessia Bellotti, Alfredo Megaro, Giuseppe Tringali, Ilenia Corbelli, Elena Cresta, Valeria Teti, Daniela Fruttini, Paolo Calabresi, Pierluigi Navarra, Lucilla Parnetti and Paola Sarchielli in Cephalalgia
Footnotes
Acknowledgments
We thank Ms Marta Ferrettini for supporting sample collection.
ORCID iDs
Ethical considerations
The study was approved by the Regional Ethics Committee (CER) of Umbria, registered under number 4219/22.
Consent to participate
All patients provided their informed consent for use of biological samples.
Author contributions
AB conceived the study, collected data and samples, analysed data, interpreted results and wrote the paper; DC conceived the study, performed biomarker measurements, analysed data, interpreted results and wrote the paper; AM performed biomarker measurements, analysed data and revised the manuscript; GT performed experiments, analysed data and revised the manuscript; DF performed statistical analyses and revised the manuscript, IC enrolled patients, collected data and revised the manuscript; EC enrolled patients, collected data and revised the manuscript; VT performed experiments and revised the manuscript; PC contributed to the study design and revised the manuscript; PN performed experiments, analysed data and revised the manuscript; LP contributed to the study design and revised the manuscript; PS conceived the study, collected data, interpreted results, wrote the paper and provided funding.
Funding
This study was funded through research grants provided by the Headache Center, University of Perugia and by Ricerca Corrente 2025 – Italian Ministry of Health – to PC, Fondazione Policlinico Universitario A. Gemelli IRCCS, Rome.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Data availability statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.