
Abstract
Background
Preventing migraine chronification is a key treatment goal, yet environmental and lifestyle contributors remain understudied in Asian populations. We investigated predictors of the transition from episodic migraine (EM) to chronic migraine (CM) in a prospective Chinese clinical-based cohort.
Methods
This multicenter, prospective study involved 1642 participants with EM meeting ICHD-3 criteria. Baseline characteristics, including environmental factors and psychological scales, were captured via a Clinical Decision Support System (CDSS). Longitudinal follow-up was conducted using a web-based mini-program. Risk factors were identified using multi-variable Cox proportional hazards models, validated by LASSO and stepwise regression.
Results
During a median 6-month follow-up, 47 (2.9%) patients progressed to CM. Multivariable analysis identified anxiety symptoms [Generalized Anxiety Disorder-7 (GAD-7) score: Hazard Ratio (HR) 1.15, 95% Confidence Interval (CI) 1.06–1.25], baseline analgesic use frequency (HR 1.07, 95% CI 1.01–1.14), and age (HR 1.04, 95% CI 1.01–1.06) as independent risk factors. Conversely, weekly physical activity duration emerged as a significant protective factor (HR 0.66, 95% CI 0.45–0.98).
Conclusion
Anxiety and higher frequency of analgesic use are independent risk factors of migraine chronification in this Chinese cohort, while regular physical activity offers protection. These findings support an integrated management strategy combining psychological intervention, medication education, and exercise therapy.
This is a visual representation of the abstract.
Introduction
The progression of migraine varies among individuals, with some patients experiencing increased headache frequency. According to the International Classification of Headache Disorders, 3rd edition (ICHD-3) classification, CM is defined as headache occurring on 15 or more days per month for more than three months, with at least eight days having migraine features. In 1982, Mathew et al. documented a series of patients with a clear history of migraine attacks whose headaches evolved over the years into a daily or nearly daily occurrence. 1 Most migraine sufferers experience EM, while only 2%–8% develop CM.2,3 The disease burden and disability associated with CM are substantially greater than those of EM. In the United States, the annual direct and indirect economic costs for patients with CM reach $7,750, which is 4.4 times higher than the $1757 for patients with EM. 4 In Europe, the projected annual cost attributable to CM is expected to reach EUR 95 billion. 5 Furthermore, CM is associated with higher disability; patients with CM exhibit a mean Migraine Disability Assessment Scale (MIDAS) score of 60.5, compared with 13.7 for EM patients, 6 indicating the severe impact of chronicity on daily living. Therefore, identifying modifiable risk factors to prevent the transition from EM to CM remains a critical challenge in migraine management and public health. 7
Large-scale prospective cohort studies, notably the American Migraine Prevalence and Prevention (AMPP) Study and the Chronic Migraine Epidemiology and Outcomes (CaMEO) Study have established foundational knowledge regarding migraine chronification. The AMPP study revealed a yearly conversion rate of 2%–3% from EM to CM, 8 whereas the CaMEO study observed that 7.6% of EM patients satisfied the diagnostic criteria for CM over a 15-month follow-up. 9 These studies found that high baseline headache frequency, overuse of acute analgesics, and comorbid conditions are major factors promoting disease chronicity.10,11 Methodologically, both AMPP and CaMEO were designed as large-scale, community-based surveys. They have been instrumental in elucidating the natural history and spontaneous trajectory of migraine chronification in the general population, relying primarily on self-reported survey data rather than physician-confirmed diagnoses in clinical settings. A meta-analysis found that “high” evidence for predicting chronic migraine progression with monthly headache days ≥ 10 (risk ratio = 5.95), “moderate” evidence for depression (risk ratio = 1.58), monthly headache days ≥ 5 (risk ratio = 3.18), and annual income ≥ $50,000 (risk ratio = 0.65), and “very low” evidence for allodynia (risk ratio = 1.40) and medication overuse (risk ratio = 8.82). 12 However, these landmark studies were predominantly conducted in Western populations, and patients managed in clinical settings often represent a distinct subpopulation with a higher baseline disease burden. Furthermore, in specialized headache centers, clinical interventions, particularly the initiation of preventive medications, can substantially alter the natural clinical course of the disease. Currently, there is a paucity of clinic-based prospective cohort data, especially in Asian populations, that evaluates the risk factors for migraine chronification within the context of real-world clinical practice.
Beyond clinical characteristics, environmental, and lifestyle factors play pivotal roles in migraine pathophysiology. The most commonly investigated environmental and lifestyle factors include dietary habits, substance intake (e.g., alcohol, coffee, monosodium glutamate), noise exposure, physical activity, body mass index (BMI), psychological status, and educational level11,13–15; their specific contribution to the long-term chronification of the disease remains understudied. For instance, a Dutch cross-sectional survey of 2197 patients observed that 35.6% considered alcohol to be a precipitating factor for their attacks. 16 Various forms of exercise, including aerobic activity, yoga, and resistance training, have been shown to alleviate migraine symptoms. 17 The CaMEO study also indicated that psychological comorbidity contributes to migraine chronicity. 11 There is a paucity of research that systematically analyzes the magnitude of these exogenous factors in driving the transition to chronicity, particularly when adjusted for internal clinical variables.
Migraine represents a significant public health challenge in the Chinese population. According to the 2021 Global Burden of Disease Study, China experienced greater increases in age-standardized incidence rates, age-standardized prevalence rates, and age-standardized disability-adjusted life years (DALYs) rates between 1990 and 2021 compared to the global average. 18 Furthermore, the current state of migraine diagnosis and treatment in China shows that only 31.1% of migraine patients are correctly diagnosed, and 62.2% receive standardized treatment, 19 indicating substantial pressure on migraine prevention and control efforts. Despite these alarming statistics, prospective cohort studies investigating migraine chronification in Chinese populations are lacking.
To address these gaps, we conducted a multicenter prospective cohort study in China. This study relied on neurologist confirmed diagnoses based on ICHD-3 criteria. Employing standardized headache diaries and structured follow-up assessments, we applied multidimensional statistical methods to systematically investigate the internal, environmental, and lifestyle factors associated with migraine chronification in a Chinese population. The findings aim to provide evidence-based insights for developing targeted prevention strategies against migraine chronicity.
Methods
Participant recruitment and clinical assessment
The study utilized data from a cohort platform established by the Chinese PLA General Hospital. The registry design follows the recommendations for Clinic-Based Headache Registries set forth by the International Headache Society. 20 Functioning as a prospective, multicenter, longitudinal cohort, the research aims to evaluate the real-world diagnosis and treatment status of migraine patients.
All patients provided informed consent to participate. The research was conducted in compliance with the principles of the Declaration of Helsinki and has been approved by the ethics committee of the Chinese PLA General Hospital (Approval No. 2022-565 and No. 2024-347-01) as well as the responsible ethics committees of each participating headache center. The study adhered to the Strengthening the Reporting of Observational Studies (STROBE) statement. It is registered with the China Clinical Trials Register (ChiCTR2200064494).
Migraine patients were recruited from multiple headache centers in China. Diagnosis of migraine was conducted by headache specialists at these centers. Inclusion criteria were: (1) a diagnosis of primary migraine according to the ICHD-3; (2) age range of 18 to 65 years; (3) provision of informed written consent; and (4) completion of the environmental factors questionnaire and other baseline information. Exclusion criteria included: (1) having a second primary or secondary headache; (2) meeting CM or medication overuse headache (MOH) diagnostic criteria at baseline; (3) presence of other chronic pain disorders, severe neuropsychiatric diseases, cardiovascular disorders, or substance abuse; and (4) anticipated inability to complete follow-up.
Baseline data were collected using the standardized Clinical Decision Support System (CDSS 2.0) platform. 21 Information included demographic characteristics (sex, age, and education level), clinical features (disease duration, monthly headache days (averaged over the past three months) [MHDs], and headache intensity measured by the Visual Analog Scale [VAS] score). Regarding medication, we recorded the specific type of analgesics used and the monthly frequency of intake (averaged over the past three months). Psychological well-being was evaluated using the GAD-7 and PHQ-9 scales, while sleep quality was assessed via the Pittsburgh Sleep Quality Index (PSQI). Furthermore, we measured headache-related disability using the MIDAS. Additionally, a self-developed questionnaire (Environment Questionnaire) was used to assess nutritional supplementation, dietary habits, lifestyle factors, and environmental exposures (Supplementary Table 1). Specifically, this questionnaire categorized weekly exercise duration into four levels: under 30 min, 30 to 150 min, 150 to 300 min, and over 300 min.
Patient follow-up and outcome definition
Follow-up assessments were conducted at 1, 3, 6, and 12 months. Headache-related data were collected prospectively and continuously through a smart headache diary integrated into a WeChat mini-program (named as Headache Supervisor). Psychological assessments and disability evaluations were completed via questionnaires distributed through the same platform. The primary outcome was migraine chronification, defined strictly as meeting the ICHD-3 criteria for CM with or without medication overuse. This diagnosis was operationalized using the continuous diary data and evaluated at the 3-, 6-, and 12-month clinical checkpoints. Patients who experienced a transient increase in headache frequency (≥15 days) during the first month but failed to sustain this for the required ≥3 months were not considered to have developed CM. This exclusion ensured the temporal stability of the diagnosis. To minimize loss to follow-up, multiple strategies were implemented, including (1) reminder notifications prior to each scheduled visit and (2) the option of telephone-based follow-up when necessary. Patients who completed six months of follow-up were included in the subsequent analyses.
Statistical analysis
All statistical processing was executed using R software (version 4.4.1). Categorical data were expressed as frequencies and percentages. The differences between groups were assessed using either the chi-square test or Fisher's exact test. Continuous data were described as mean (standard deviation) for normally distributed variables, and as median (interquartile range) for non-normally distributed variables. Normally distributed data were compared using Student's t-test, while non-normally distributed data were analyzed using the Mann-Whitney U test.
Independent predictors were identified using multivariable Cox regression, validated by C-index and Schoenfeld test. To address unobserved heterogeneity and unbalanced data across centers, a mixed-effects Cox model (shared frailty) with Gaussian random intercepts was preferred over fixed-effects approaches. For sensitivity analysis, a time-dependent Cox proportional hazards model was employed. Longitudinal data were restructured into a counting process (start-stop) format, enabling specific covariates to be updated dynamically at follow-up intervals while retaining baseline variables as fixed effects. Analyses utilized the ‘coxme’ package in R. Besides, backward stepwise selection was applied to significant univariate factors, with model optimization based on minimizing the Akaike Information Criterion (AIC). To assess robustness, a bootstrap method was employed to evaluate the frequency of variable inclusion upon refitting. LASSO regularization (α = 1) was applied within the Cox framework to perform variable selection. The optimal penalty parameter (λ) was determined via 10-fold cross-validation based on partial likelihood deviance. Final predictors with non-zero coefficients were identified using the one-standard-error (1-SE) rule. All statistical analyses were conducted with two-tailed tests, and a p-value of less than 0.05 was considered as statistically significant.
Results
Participant enrollment
During the research period, 2093 patients enrolled in the follow-up study and provided complete baseline data. Ultimately, 1642 patients from 67 headache centers across China were finally included in this study (Supplementary Table 2). The enrollment and exclusion procedures are depicted in Figure 1. The total follow-up duration was 10,074 person-months. During the follow-up period, 47 (2.9%) patients with EM met the diagnostic criteria for CM.

Patient inclusion and exclusion flowchart.
Baseline and follow-up characteristics comparison between the chronification and non-chronification groups
The baseline and follow-up characteristics of the chronification group (n = 47) and the non-chronification group (n = 1595) were shown in Table 1. No statistically significant differences were observed between the two groups in demographic characteristics, including age, gender distribution, or BMI. At baseline, headache-related characteristics were notably more severe in the chronification group than those in the non-chronification group (all p < 0.001), including MHDs (6.0 vs. 4.0), monthly analgesic use (2.5 vs. 2.5), and MIDAS (19.0 vs. 10.0). The chronification group showed more severe psychological and sleep symptoms, with significantly higher baseline scores (all p < 0.001) for GAD-7 (6.0 vs. 3.0), PHQ-9 (7.0 vs. 5.0), and PSQI (8.0 vs. 6.0). During follow-up, PHQ-9 scores remained higher at 3 months (5.0 vs. 4.0, p = 0.039) and 6 months (6.5 vs. 4.0, p = 0.002), and GAD-7 scores were elevated at 6 months (5.0 vs. 3.0, p = 0.043). Additionally, the chronification group had a higher rate of environmental noise exposure (14/47, 29.8% vs. 269/1,595, 16.9%; p = 0.034) and less exercise time level (1.0 vs. 2.0, p = 0.037).
Baseline characteristics and follow-up measures of patients in the non-chronification and chronification groups.

BMI = Body Mass Index; GAD-7 = Generalized Anxiety Disorder-7; IQR = Interquartile Range; MHDs = Monthly Headache Days; MIDAS = Migraine Disability Assessment; MMDs = Monthly Migraine Days; MSG = Monosodium Glutamate; PHQ-9 = Patient Health Questionnaire-9; PSQI = Pittsburgh Sleep Quality Index;* p < 0.05.
Identification of risk factors for migraine chronification using cox regression
Univariate Cox proportional hazards regression analysis identified environmental noise (HR = 2.06, 95% CI: 1.10–3.85), analgesic use (HR = 1.12, 95% CI: 1.05–1.18), MIDAS (HR = 1.006, 95% CI: 1.004–1.01), GAD-7 (HR = 1.13, 95% CI: 1.07–1.20), PHQ-9 (HR = 1.11, 95% CI: 1.06–1.17), and PSQI (HR = 1.15, 95% CI: 1.06–1.24) as risk factors, while exercise was protective (HR = 0.66, 95% CI: 0.44–0.99) (Table 2). Variables with a P-value of less than 0.05 from the univariate Cox regression analysis were incorporated into the multivariable Cox regression model. The results of the multivariable Cox regression analysis are shown in Table 3.
Univariate cox regression analysis of risk factors for migraine chronification.

BMI = Body Mass Index; CI = Confidence Interval; GAD-7 = Generalized Anxiety Disorder-7; HR = Hazard Ratio; MHDs = Monthly Headache Days; MIDAS = Migraine Disability Assessment; MSG = Monosodium Glutamate; PHQ-9 = Patient Health Questionnaire-9; PSQI = Pittsburgh Sleep Quality Index; * p < 0.05.
Multivariable cox regression analysis of independent risk factors for migraine chronification.

CI = Confidence Interval; GAD-7 = Generalized Anxiety Disorder-7; HR = Hazard Ratio; MHDs = Monthly Headache Days; MIDAS = Migraine Disability Assessment; PHQ-9 = Patient Health Questionnaire-9; PSQI = Pittsburgh Sleep Quality Index; * p < 0.05.
The multivariable analysis revealed that age (HR = 1.04, 95% CI: 1.01–1.06), GAD-7 score (HR = 1.15, 95% CI: 1.06–1.25), and baseline analgesic use frequency (HR = 1.07, 95% CI: 1.01–1.14) were independent risk factors for migraine chronification. In contrast, weekly exercise time level remained a significant protective factor (HR = 0.66, 95% CI: 0.45–0.98). It is noteworthy that the PHQ-9 score (p = 0.71), PSQI score (p = 0.60), MIDAS score (p = 0.80), and environmental noise exposure (p = 0.38), which were significant in the univariate analysis, lost statistical significance in the multivariable model. Similarly, baseline MHDs did not remain significant (p = 0.077). The C-index of the multivariable Cox proportional hazards model was 0.76 (95% CI: 0.71–0.84) (Figure 2).
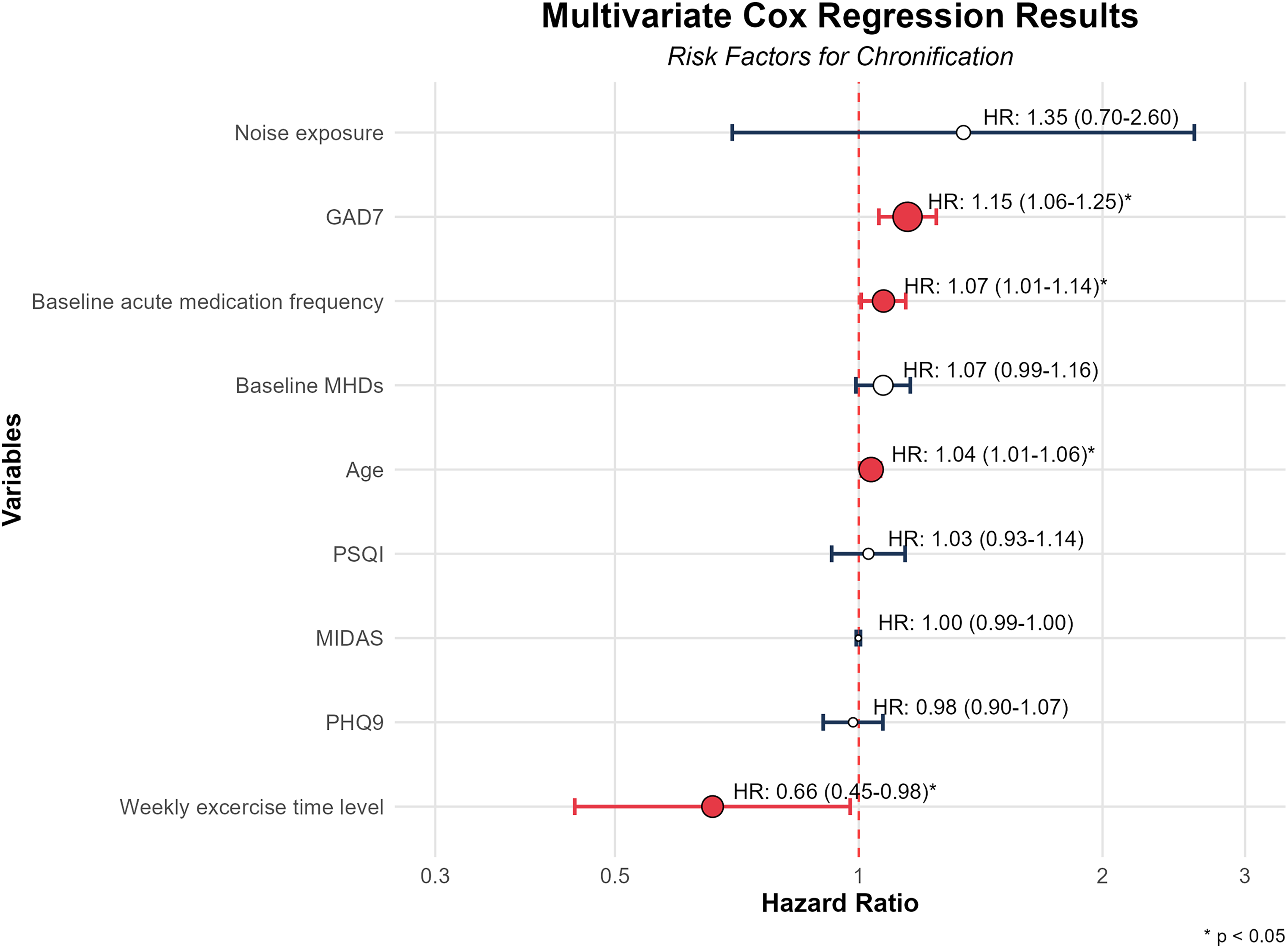
Forest plot of the multivariate Cox regression model.
To assess the potential confounding effect of clinical management, a sensitivity analysis was conducted by adding baseline preventive medication use to the multivariable model. The predictive value of Age, GAD-7, Analgesic use, and Exercise remained stable and statistically significant (Supplementary Table 3). Furthermore, to account for the dynamic nature of psychological and sleep parameters—which may fluctuate secondary to worsening headaches—we conducted a sensitivity analysis using a time-dependent Cox proportional hazards model. In this model, GAD-7, PHQ-9, PSQI, and MIDAS scores were treated as time-varying covariates, dynamically updated at the 3- and 6-month follow-ups. Consistent with the primary analysis, time-updated anxiety symptoms (HR = 1.12, 95% CI: 1.03–1.22, p = 0.007), baseline analgesic use frequency (HR = 1.08, 95% CI: 1.01–1.15, p = 0.022), and weekly exercise time (HR = 0.66, 95% CI: 0.45–0.98, p = 0.039) remained significantly associated with migraine chronification (Supplementary Table 4). Time-updated depression and sleep quality remained non-significant.
To account for the clustering effect inherent in the multicenter design and unobserved heterogeneity across centers, a mixed-effects Cox proportional hazards model was employed. The analysis revealed that age (HR = 1.03, 95% CI: 1.01–1.06), GAD-7 score (HR = 1.11, 95% CI: 1.02–1.22), and baseline frequency of analgesic use (HR = 1.07, 95% CI: 1.00–1.14) remained independent risk factors for migraine chronification. Weekly exercise time was identified as a significant protective factor (HR = 0.67, 95% CI: 0.45–0.99). The PHQ-9 score (p = 0.99), PSQI score (p = 0.50), MIDAS score (p = 0.79), and environmental noise exposure (p = 0.32) did not show statistical significance in the mixed-effects model. Similarly, baseline MHDs showed a borderline trend but did not reach statistical significance (p = 0.084) (Supplementary Table 5).
Subsequent analysis of risk factors for the chronicity of migraine using stepwise and LASSO regression
Stepwise regression
Backward stepwise regression analysis (final AIC = 661.85, full model AIC = 666.56) retained five variables with independent predictive value: age, GAD-7 score, baseline MHDs, baseline frequency of analgesic use, and weekly exercise time (Table 4). The final Cox model is presented in the form of a forest plot below (Supplementary Figure 1).
Stepwise regression analysis of independent risk factors for migraine chronification.

CI = Confidence Interval; GAD-7 = Generalized Anxiety Disorder-7; HR = Hazard Ratio; MHDs = Monthly Headache Days; * p < 0.05.
Bootstrap resampling (R = 500) and stepwise Cox regression on each bootstrap sample identified several predictors with varying degrees of stability. The GAD-7 score (88.0%) emerged as the most stable predictor, followed by age (79.2%) and baseline frequency of analgesic use (75.8%). Moderately stable factors included baseline MHDs (73.0%) and weekly exercise time (72.0%). In contrast, environmental noise exposure (36.0%), PSQI score (27.6%), PHQ-9 score (20.4%) and MIDAS score (13.6%) demonstrated low stability (Figure 3).
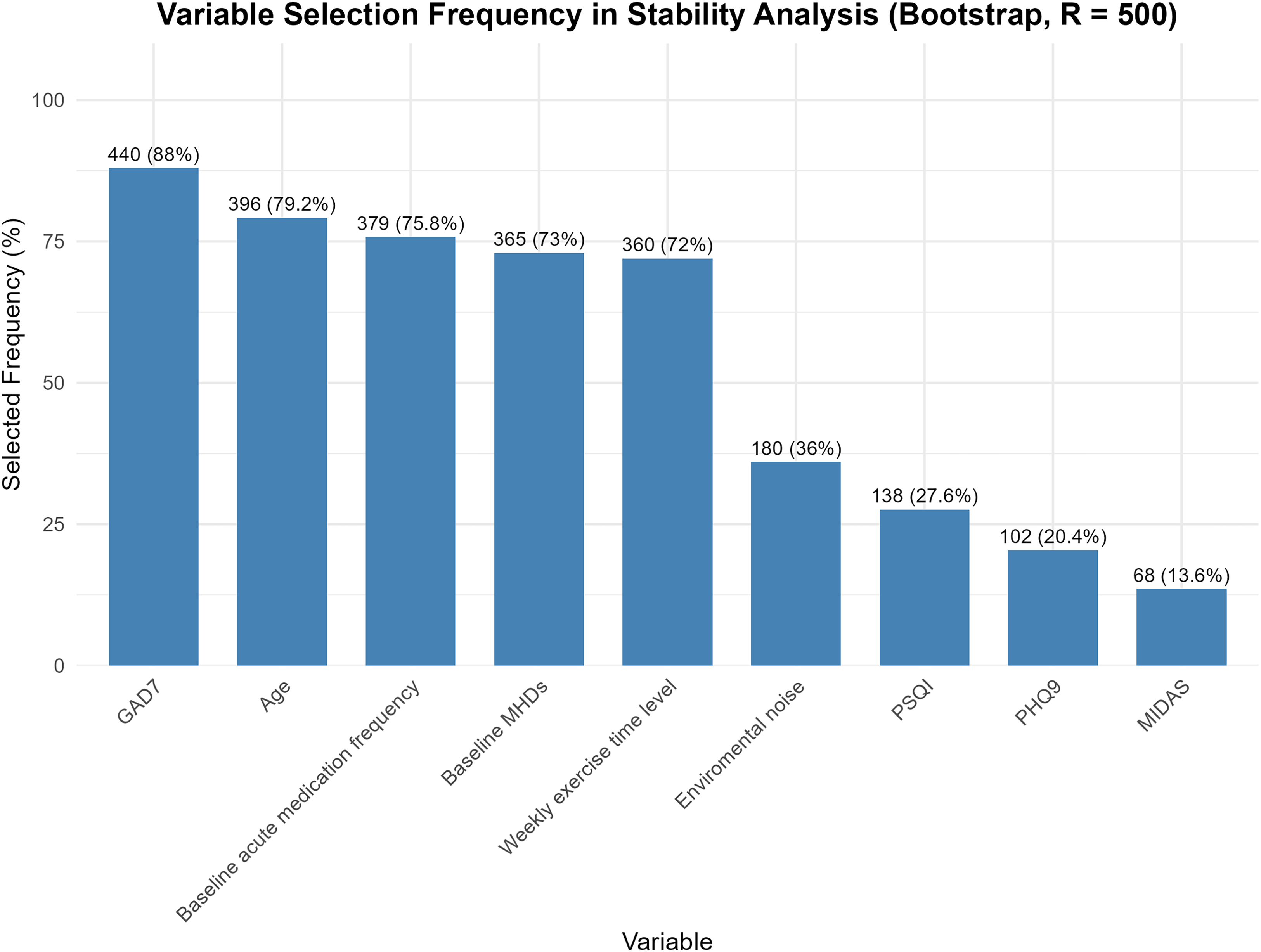
Variable selection frequency in stability analysis based on bootstrap.
Cox-LASSO regression
A Cox-LASSO regression combined with a 10-fold cross-validation variable selection procedure was applied to identify key predictors of migraine chronification. Age, sex, variables with significant group differences, and important clinical factors were included in the analysis. The optimal penalty parameter was determined using the one-standard-error (1-SE) rule, resulting in λ = 0.0129. At this penalty level, three core predictors with non-zero coefficients were retained from the initial set of candidate variables: baseline frequency of analgesic use (coefficient: 0.017), GAD-7 anxiety score (coefficient: 0.056), and baseline monthly headache days (coefficient: 0.023), excluding other variables for optimal parsimony (Supplementary Figure 2).
Discussion
In this prospective, multicenter, clinic-based cohort study, we observed a cumulative chronification rate of 2.9% over a median 6-month follow-up among Chinese patients with EM. By employing a rigorous statistical framework that integrated multivariable Cox regression, mixed-effects models, and machine learning-based variable selection (LASSO and Stepwise), we identified age, higher anxiety levels (GAD-7), and frequent baseline analgesic use as robust independent risk factors. Conversely, increased weekly exercise time emerged as a key modifiable protective factor. Notably, while depressive symptoms, sleep quality, and environmental noise showed univariate associations, their predictive value diminished after adjustment, underscoring the dominant influence of anxiety and medication overuse in the trajectory of migraine chronicity.
Unlike population-based epidemiological studies such as AMPP and CaMEO,8,9 which primarily elucidate the natural history of migraine progression in the general population, our study is a clinic-based cohort comprising treatment-seeking patients. Consequently, direct numerical comparisons of chronification rates between our cohort and population-based data are conceptually inappropriate. Treatment-seeking patients inherently present with a more severe baseline disease burden, characterized by higher headache frequencies and greater disability. More importantly, patients were receiving clinical management, in which acute treatments and preventive medications exerted a substantial impact on the clinical course, potentially modifying the natural chronification trajectory. Therefore, our findings uniquely reflect the chronification risk factors and disease prognosis of treatment-seeking patients within real world clinical settings. This serves as a critical complement to existing community-based evidence.
The observed chronification rate aligns with global epidemiological data, falling between the annual rate of 2%–3% in the AMPP study and the 7.6% in the CaMEO study. 10 This variation may be related to the difference in follow-up intervals, as shorter intervals (e.g., 3 months in CaMEO) capture fluctuations that annual assessments might miss. Similarly, given our median follow-up of 6 months, meeting the ICHD-3 criteria for CM—which strictly requires at least three months of sustained high-frequency headaches—indicates that our 2.9% incidence specifically reflects a trajectory of early or rapid chronification. The consistency of our results with these large-scale epidemiological investigations validates the reliability of our data.
Our study highlights the pivotal role of psychological distress. Multivariable Cox regression demonstrated that each one-point increase in the GAD-7 score was associated with a 14.9% increase in the risk of chronification (HR = 1.15, p = 0.009), and this association exhibited high stability, being selected in 88% of bootstrap resampling models. Psychological factors have long been recognized as key determinants in migraine chronification. Previous studies have shown the prevalence of anxiety among CM patients (30.2%) was 1.8 times higher than that among EM patients (18.8%). 10 In the AMPP study self-reported anxiety remained a significant risk factor for progression to CM (OR = 1.53) even after adjusting for headache intensity (OR = 1.52). 22 Pathophysiologically, this association likely involves shared serotonergic (5-HT) dysregulation, which heightens trigeminovascular excitability. 23 Furthermore, chronic anxiety activates the hypothalamic-pituitary-adrenal (HPA) axis, elevating cortisol and amygdala excitability, which disrupts pain signal processing, amplifies sensory stimuli, and promotes chronification. 24
While depression (PHQ-9) showed significance in univariate analysis, its predictive value was nullified in the multivariable model. This likely reflects the high collinearity between anxiety and depression. For instance, The Medical Expenditure Panel Survey found that among 1556 migraine patients, the comorbidity rate of anxiety and depression was 13.9%, significantly higher than that in the general population. 25 Our findings suggest that anxiety may capture the core variance of psychological distress relevant to chronification, potentially “overshadowing” the specific contribution of depression in the Chinese population.
Frequent analgesic use is a well-established driver of migraine progression. Our study reinforces that frequent medication use is an important risk factor in the transition from EM to CM. Longitudinal data suggest a complex interaction between NSAID use and headache frequency: while protective for low-frequency patients, increased intake in those with high headache burdens accelerates central sensitization. 26 Mechanistically, our prior study utilizing 7 T multimodal MRI techniques identified structural and functional irregularities in the parahippocampal gyrus and middle occipital gyrus among individuals with medication overuse. These neural irregularities correlated with analgesic intake frequency, suggesting that overuse induces maladaptive plasticity and reward system dysregulation. 27 This creates a vicious cycle where frequent headaches prompt overuse, which lowers pain thresholds and further exacerbates frequency.
Our study found that exercise might be a protective factor for migraine chronification, a finding corroborated by the HUNT study which linked physical inactivity to increased headache risk. 28 The protective effects of exercise, particularly aerobic exercise, may be mediated through neurotrophic and anti-inflammatory pathways. A meta-analysis reported that exercise significantly elevated resting peripheral brain-derived neurotrophic factor (BDNF) concentrations, which are typically reduced in migraine patients. 29 Animal studies further found that BDNF improves migraine-like behavior through preservation of the structure and function of the periaqueductal gray and through modulation of microglial signaling within the trigeminal nucleus caudalis.30,31 Additionally, exercise downregulates pro-inflammatory cytokines (e.g., TNF-α, IL-6) and promotes microglial polarization toward the M2 phenotype. 31
It is essential to emphasize that psychological factors, medication overuse, and lifestyle habits do not operate in isolation. These factors interact in a complex, bidirectional manner. Psychological distress can drive maladaptive coping and medication overuse, while the resultant increase in headache frequency and treatment failure further exacerbates anxiety and central sensitization, creating a self-perpetuating loop of chronification.
Based on these findings, we recommend an integrated management approach combining psychological intervention, medication standardization, and exercise therapy. Anxiety emerged as the most consistent predictor, highlighting the need for psychological care. Cognitive behavioral therapy (CBT) represents the cornerstone of such management. A randomized controlled trial by Powers et al. (2013) demonstrated that 20 weeks of CBT combined with amitriptyline resulted in a reduction of 11.5 MHDs from baseline, which was significantly greater than that observed in the amitriptyline-only or headache education control groups, and the therapeutic benefit persisted for 12 months. 32 Moreover, evidence suggests that clear advice on appropriate use can be as effective as formal detoxification programs for certain patients in preventing migraine chronification. 33 When translating the protective effects of exercise into clinical practice, establishing a tangible behavioral target is essential. We recommend aligning with the World Health Organization (WHO) guidelines, which advocate for at least 150 min of moderate-intensity aerobic exercise per week. 34 The clinical efficacy of such regimens is well-supported; for instance, a network meta-analysis by Reina-Varona et al. (2024) that included 28 clinical trials found that moderate-intensity continuous aerobic exercise, high-intensity aerobic exercise, and yoga were all superior to pharmacologic therapy alone in reducing EM attack frequency. Notably, yoga demonstrated additional benefits in alleviating pain intensity and anxiety symptoms. 35 It is essential to note that these three interventions, psychological, pharmacological, and physical, are interrelated rather than independent. Patients with anxiety are more prone to medication overuse due to heightened pain anticipation, whereas regular exercise can simultaneously reduce anxiety and mitigate medication dependence. The integration of these strategies establishes a positive feedback cycle that improves mood, decreases medication use, and enhances pain thresholds, thereby offering a more effective means of preventing the progression from EM to CM.
Strengths and limitations
Strengths: First, to the best of our knowledge, this is the first multicenter, prospective longitudinal study to investigate migraine chronification rates and risk factors specifically within a large Chinese clinical cohort, filling a critical gap in Asian epidemiological data relative to Western-centric studies. Second, our study employed a rigorous methodological framework that integrated multivariable Cox regression with machine learning-based variable selection (LASSO) and bootstrap resampling. This comprehensive statistical approach minimized overfitting and multicollinearity—particularly between anxiety and depression—ensuring the identification of robust, independent predictors. Third, beyond confirming established risk factors like baseline analgesic use frequency, we provided novel longitudinal evidence identifying weekly exercise duration as a key modifiable protective factor. Finally, by synthesizing pharmacological, psychological, and lifestyle variables, our findings offer a holistic “biopsychosocial” evidence base that supports an integrated clinical management strategy for preventing disease progression.
Limitations: First, potential selection bias exists as participants were recruited exclusively from outpatient clinics. This likely led to an over-representation of patients with higher severity or treatment motivation, and higher proportion of novel acute migraine medication use, limiting generalizability to the community-based migraine population. Second, the number of chronification events was relatively modest. While our use of LASSO and bootstrap resampling mitigated model instability, the limited sample size may have reduced statistical power to detect risk factors with smaller effect sizes (e.g., depressive symptoms) or interactions. Third, our data collection methods presented certain limitations. Environmental noise was assessed subjectively without categorizing specific noise types. Additionally, because our CDSS strictly adhered to the mandatory ICHD-3 diagnostic criteria, osmophobia—a highly specific clinical feature of migraine—was not captured in the baseline assessment. Future iterations of the CDSS will incorporate more granular environmental questionnaires and osmophobia evaluations. Reliance on self-reporting introduces potential recall bias, highlighting the need for objective measurements like wearable activity trackers. Finally, the follow-up period (median duration of six months) was relatively short. Although sufficient for our primary analysis of early/rapid chronification trajectories, a longer observation window would be required to capture the long-term dynamics and fluctuations of migraine chronification.
Conclusion
In this multicenter prospective cohort study of 1642 patients with episodic migraine, 47 (2.9%) progressed to chronic migraine (CM) over a median follow-up of 6 months. Age, anxiety symptoms (GAD-7), and baseline analgesic use frequency were identified as robust, independent risk factors driving this progression. Notably, regular physical activity emerged as a key modifiable protective factor. These findings, derived from the first longitudinal evidence in this Chinese clinical cohort, underscore the complex interplay of psychological distress, medication behaviors, and lifestyle in disease trajectories. Consequently, we advocate for an integrated management strategy that combines psychological intervention, standardized medication education, and exercise promotion to effectively prevent the transition from episodic to chronic migraine.
Clinical implications
Anxiety and baseline analgesic use frequency are independent risk factors for migraine chronification in the Chinese population. Weekly physical activity duration is a key modifiable protective factor against disease progression. An integrated management strategy combining psychological intervention, medication education, and exercise should be implemented early in episodic migraine.
Supplemental Material
sj-doc-1-cep-10.1177_03331024261446614 - Supplemental material for Environmental and psychological risk factors for migraine chronification in China: A multicenter prospective cohort study
Supplemental material, sj-doc-1-cep-10.1177_03331024261446614 for Environmental and psychological risk factors for migraine chronification in China: A multicenter prospective cohort study by Longteng Ma, Linfeng Liu, Ye Ran, Xun Han, Hui Su, Mingjie Zhang, Xiaolin Wang, Xingkai An, Liang Zhang, Suiyi Xu, Wenping Gu, Shilun Zuo, Yuncheng Wu, Yan Li, Yuhu Zhang, Ming Dong, Qian Tian, Shengyuan Yu and Zhao Dong in Cephalalgia
Supplemental Material
sj-doc-2-cep-10.1177_03331024261446614 - Supplemental material for Environmental and psychological risk factors for migraine chronification in China: A multicenter prospective cohort study
Supplemental material, sj-doc-2-cep-10.1177_03331024261446614 for Environmental and psychological risk factors for migraine chronification in China: A multicenter prospective cohort study by Longteng Ma, Linfeng Liu, Ye Ran, Xun Han, Hui Su, Mingjie Zhang, Xiaolin Wang, Xingkai An, Liang Zhang, Suiyi Xu, Wenping Gu, Shilun Zuo, Yuncheng Wu, Yan Li, Yuhu Zhang, Ming Dong, Qian Tian, Shengyuan Yu and Zhao Dong in Cephalalgia
Footnotes
Acknowledgements
We gratefully acknowledge all the patients who participated in this study and the staff at the participating headache centers for their cooperation.
ORCID iDs
Ethical considerations
This study was approved by the Ethics Committee of the Chinese PLA General Hospital(Approval No. 2022-565; No. 2024-347-01) as well as the responsible ethics committees of each participating headache center.
Consent to participate
Written informed consent was obtained from all individual participants included in the study
Consent for publication
The authors agree to publish with Cephalalgia if the manuscript is accepted.
Author contributions
L.M. and L.L. contributed to study design, data analysis, and interpretation of results. L.M., L.L., Y.R., and Z.D. participated in manuscript writing. Y.R. and Z.D. conceived the study, and were responsible for manuscript review, study supervision, and funding acquisition. X.H., H.S., M.Z., X.W., X.A., L.Z., S.X., W.G., S.Z., Y.W., Y.L., Y.Z., M.D., Q.T., S.Y., Y.R., and Z.D. participated in data collection. All authors contributed intellectual content to the revised manuscript and read and approved the final version. L.M., L.L. and Y.R. are co-first authors. Z.D. is the corresponding author.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the National Key R&D Program of China (grant numbers 2023YFC2508701, 2023YFC2508705) the National Natural Science Foundation of China (grants 82171208 to Z.D.), the Research Program of the Chinese Research Hospital Association (Y2023FH-TTYGJZA12), the Chongqing Medical Scientific Research Project (Joint project of Chongqing Health Commission and Science and Technology Bureau) (grant number 2024GGXM002), and the Science and Technology Incubation Program of the 983rd Hospital (grant number 983YN23F021).
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Open practices
Not applicable
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.