
Abstract
Public libraries can play a major role in improving health literacy of clients by offering special services. Educating diabetic patients through public libraries can improve the dissemination of health information. The objective of the study was to evaluate the effect of education on the level of health literacy among diabetic patients referring to a public library, and the relationship between health literacy level, age and gender of patients. This research is a quasi-experimental study with pre-test and post-test. The study population included 48 diabetic patients referring to the public library. The research tool is a nationalized adult health literacy questionnaire in Iran. Results showed that 14.5% of samples had the maximum access to the required information in terms of accessibility. In terms of reading skill, 20% of samples had the maximum skill needed to read the information resources. In terms of information comprehension, 27% of samples had a maximum comprehending of the information they needed. In terms of evaluation, 13.5% of samples had completely correct evaluation of the information they needed. In terms of decision making, 24.5% of the people made decisive decisions about their information demands. The mean health literacy of diabetic patients before and after education showed a significant difference. In addition, no significant relationship was found between the level of health literacy and the age of diabetic patients referring to the public library before and after education (r <0.05). The health literacy level of diabetic patients increased before and after education in both males and females. It was concluded that as one of the tasks of public libraries is teaching citizens, the use of educational capacities in public libraries in the health sector can improve community health.
Introduction
One of the centers which have been able to take steps to improve health knowledge of people in many countries, is public libraries. The central public library is a local place for information which provides all kinds of knowledge and information to users. The most vital health issues and demands of the different classes of the society in the health area can be handled by libraries. The public library, as a service institution, plays an important role in collecting, organizing and exploiting, providing and accessing to information resources which is why public libraries have a responsibility in improving the health literacy of communities. In other words, health literacy is the most important issue which can be improved by using the capacity of public libraries (Cobus, 2008; Flaherty, 2013; Malachowski, 2011, 2014).Health literacy is defined as one’s capacity to gain, interpret and comprehend the basic health information needed to make proper decisions (Berkman et al., 2010; Kumar et al., 2010; Rudd, 2010; Speros, 2005).
Based on a WHO report, people lacking the health literacy skills, show
Poor health literacy is associated with a lack of knowledge and understanding health conditions and health services, inability in conducting self-care activities, difficulty in comprehending medicine guidelines, inappropriate medicine consumption, not following physicians’ orders, increase in hospitalization and health care costs, poor health status and increased mortality, less screening for early diagnosis of diseases, the inability to communicate with physicians and medical staff (Sihota et al., 2004). In developed countries such as US, health literacy is an important issue which in this regard, various plans and projects are developed and implemented. For example, National Plan for Improvement of Health Literacy is one of these plans, developed and implemented by the US Department of Human Health and Services seeking to interact with organizations, professionals, policymakers, communities, individuals and families to improve the various aspects of health literacy (Malachowski, 2014). If we consider health literacy as a set of skills, abilities and capacities which involves obtaining health information and comprehending them, processing, interpreting, and using this updated information, these skills and capacities can be the basis for measuring health literacy tools (Speros, 2005). The Test of Functional Health Literacy in Adults (TOFHLA) is one of the most important tools. Parker et al. (1995) designed a reliable and valid tool for assessing functional health literacy in patients. This tool included 50 questions related to comprehending the concepts of words when reading and 17 items related to testing the ability of counting comprehension. To complete this questionnaire, 22 minutes is required (Parker et al., 1995). The shortened form of TOFHLA (S-TOFHLA) is used to measure patients’ ability to read and comprehend health-related concepts. The research conducted by Baker et al. (1999) designing a shortened version of TOFHLA was aimed at reducing to 17 items in the numerical domain, 3 items in the conceptual domain, 4 items in the counting domain. Its completion time also was reduced from 22 minutes to 12 minutes (Baker et al., 1999). Studies have shown that S-TOFHLA is a practical tool for measuring functional health literacy. It can be used by health educators to identify individuals who need special help to achieve learning goals (Baker et al., 2008; Morris et al., 2006).
Rapid Estimate of Adult Literacy in Medicine (REALM) is another screening instrument to assess an adult patient’s ability to read common medical words and lay terms for body parts and illnesses. It is designed to evaluate medical professionals in estimating a patient’s literacy level so that the appropriate level of patient education materials or oral instructions may be used. The test takes two to three minutes to administer and score (Davis et al., 1993).
The Health Literacy for Iranian Adults (HELIA) questionnaire is one of the normalized questionnaires in this area, which has been considered more in comparison with the other questionnaires because of its comprehensiveness of measuring various aspects of health literacy. Its reliability and validity to measure the health literacy in Iran’s context have been confirmed. This research was an attempt to design a tool to measure the public health of adult Iranian people (18 to 65 years) living in Iran’s cities. It has been developed based on the socio-cultural characteristics of Iranian people to be used in other studies. After reviewing various scientific documents on health literacy in the present research, the related definitions were determined in order to develop the tool’s conceptual framework.in addition, according to the health area’s priorities in the country and some important public information about health, the questions were provided.
Then, several items were developed in the mentioned subjects based on the concepts of health literacy dimensions including access, reading skill, comprehension, evaluation and decision making, and applying health information by using existing tools and consulting with experts (66 questions). The content validity of the questionnaire was evaluated by 15 different health professionals and suggested reforms were applied. It included 47 questions. After collecting the information from 336 people selected randomly from 22 districts of Tehran, its construct validity (using exploratory factor analysis) and reliability (by calculating the internal correlation coefficient) were evaluated.
The final results of factor analysis revealed that the questionnaire had 33 questions in 5 specific domains, including 1 – access (6 questions); 2 – reading skill (4 questions); 3 – comprehension (7 questions); 4 – evaluation (4 questions), and 5 – decision making (12 questions). The Cronbach’s alpha of the items in the related constructs was acceptable and varied from 0.72 to 0.89, so the reliability of the questionnaire was confirmed. Results of this research can be used to measure the health literacy of the urban population in Iran (Haghdoost et al., 2015; Montazeri et al., 2014).
Today, the number of diabetic people is growing increasingly in the world. One of the factors affecting diabetes prevention and control is having adequate knowledge about the occurrence and prevention of this disease. In addition, one of the factors affecting the level of knowledge and more effective control and prevention of diabetes is health education through public libraries (Gillaspy, 2005).
Several studies have been carried out on the importance of health literacy education by librarians in foreign countries (Berkman et al., 2004, 2011b; Eichler et al., 2009; Parker and Kreps, 2005; Shipman et al., 2009). However, no independent study was found to evaluate the educational role of public libraries to enhance the level of health literacy. According to the aforementioned, researchers aim to evaluate the health literacy status of diabetic patients referring to the public Andisheh Cultural Library by using the HELIA questionnaire and evaluate their health literacy before and after training. Results of this study not only can explain the effect of education on the health literacy of the patients and the role of public libraries in this process, but also can clarify the value and status of these libraries in promoting health culture.
Methods
The present study is a quasi-experimental study with pre-test and post-test. The research population included diabetic patients referring to Tehran Municipality Cultural and Art Organization (Andisheh Cultural Center) from April to November 2015. The sample population was 48 people using this formula:
Fifty-two participants were selected for the pilot study (6.5 mean difference questionnaire score before and after intervention, with 0.05 significance level and 80% power and 10% dropout). Four persons missed a follow up. We therefore analyzed data for the remaining 48 participants.
The tool applied to collect data was HELIA Normalized Questionnaire, published in 2015. The validity of this tool was confirmed by 15 experts in different fields of medicine. Cronbach’s alpha was used in order to confirm the reliability reported as 0.72 to 0.89. The questionnaire includes 33 questions in 5 domains, including access (6 items), reading skill (4 items), comprehension (7 items), evaluation (4 items), and decision making and application of health information (12 items). the current study evaluates the health literacy of the community before and after the direct and indirect education. The questionnaire was distributed among the research subjects and was collected after completion.
Then, direct and indirect education was provided for the subjects. Direct education was provided for the subjects in four two-hour sessions by the head of the Iranian Association for Diabetes according to the required information for diabetic patients, including self-care, control, treatment, maintaining and promotion of health and so forth. The indirect education included selecting and preparing a brochure, pamphlet, and educational booklets for diabetic patients by a librarian and with the consultation of experts in this area. The questionnaire is scored between 0 and 100, in which a health literacy’s score between 0 and 59, suggests inadequate literacy, score between 60 and 74 suggests borderline health literacy, and score between 75 and 100 suggests adequate health literacy. Data were analyzed by using SPSS21 software. Paired t-test and chi-square tests were applied for pre-test and post-test comparisons. Correlation between variables was also determined by using Pearson correlation coefficient.
Results
Figure 1 indicated that the number of women and men was 22 (45.8%) and 26 (54.2%) respectively. Mean age of individuals was 10.61± 54.62.

Background information of the population under study (gender).
Figure 2 indicated that three individuals had a high school degree (6.25%), two had a primary degree (4.17%), seven had diploma degrees (14.9%), five had associate degrees (10.42%), 18 had BA degrees (37.5%), 10 had MA degrees (2.1%) and two had PhD (4.17%).

Background information of the population under study (education).
Frequency distribution of employment shows (Figure 3) that the highest frequency associates with students (25 persons (52%)) followed by retired individuals (12 (25%)), unemployed individuals (7 persons (15%)), housewives (4 persons (8%)).

Background information of the population under study (employment).
Some participants had experienced more than one source of information (Figure 4). Thus, 24 participants (28.24%) obtained health information from doctors and health personnel, 37 (43.53%) through using Internet, radio, and television, 17 (20%) from educational brochures and pamphlets, journals and magazines, and 7(8.23%) by asking friends.
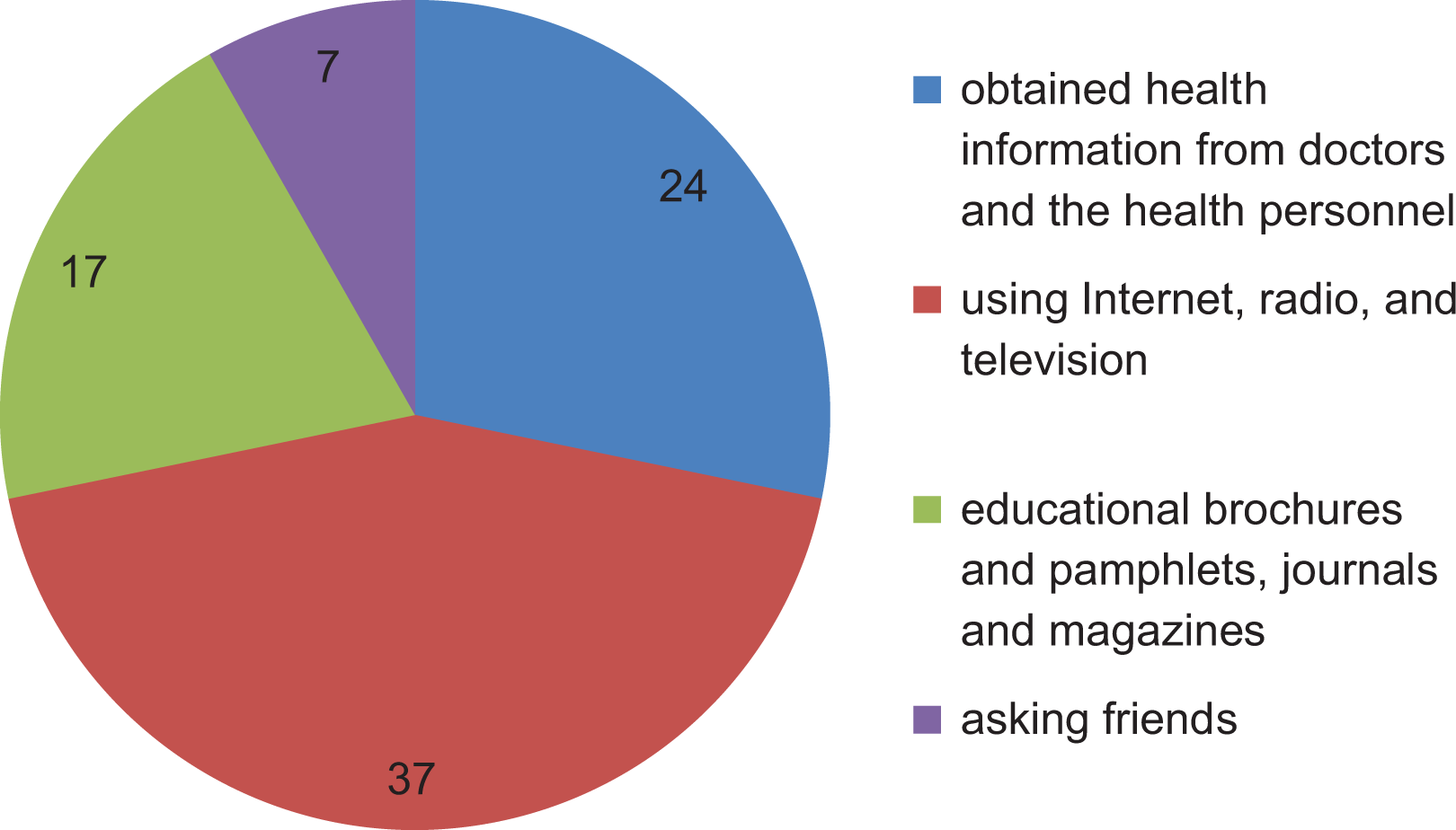
Background information of the population under study (source of information).
Table 1 revealed that: 14.5% of samples had the maximum access to the required information in terms of accessibility while 2.5% of them had the minimum rate of access. In terms of reading skill, 20% of samples had the maximum skill needed to read the information resources while 8.5% of them the minimum rate. In terms of comprehension skills, 27% of samples had a maximum comprehension of the information they needed while 4% of them had the minimum rate of these skills. In terms of assessment skills, 13.5% of samples had completely correct evaluation of the information they needed while 4% of them had the minimum rate of these skills. In terms of decision-making skills, 24.5% of the samples made decisive decisions about their information demands while 6% of them had the minimum rate of these skills.
The frequency of five variables in health literacy.

According to Table 2, the mean score of the health literacy level before intervention was 72.45 ± 9.99 which increased to 79.85 ± 10.22 (p-value < 0.001) after intervention. The mean score difference before and after education was 7.40±10.50.
Mean comparison of health literacy level before and after education.

Table 3 shows that 23% of women under study had borderline health literacy and 77% had adequate health literacy. 19% of men had borderline health literacy and 81% had adequate health literacy. Generally, 79% of participants had adequate health literacy and 21% had borderline health literacy.
Health literacy level of diabetic patients based on their gender.

According to Table 4, mean health literacy of women before education was 119.51 (standard deviation: 17.20) and it was 131.49 after education (standard deviation: 16.89), while mean health literacy of men before education was 119.57 (standard deviation: 16.20) and it was 131.99 after education (standard deviation: 17.18). It can be seen that health literacy of male and female diabetic patients increased before and after education. Therefore, there is no significant relationship between health literacy of patients referred to Andisheh Cultural Center and their genders.
Comparing mean score of health literacy before and after education based on gender.

Discussion
As there are several tools to measure health literacy, different tools have been used in various studies to measure health literacy skills in patients. The results of various studies around the world have reported wide range of inadequate health literacy (Duong et al., 2015; Palumbo et al., 2016; Sørensen et al., 2015).
The current research reported that the maximum rate of the main areas of health literacy, including accessibility, reading skill, comprehending, evaluation, and decision making are at a low level, while the acceptable level of these areas allows people to interpret and understand the issues related to their health and be able to take care of themselves and others against pathogens. The findings of different studies suggest that in communities with a high level of public health literacy, people are more vibrant, healthier, and dynamic and lower costs are imposed on governments to treat the patients. Hence, treatment costs will be spent on the prevention and health of the people, leading to an improvement in quality of people’s lifestyle. People with inadequate health literacy are less likely to comprehend the written and spoken information provided by health professionals and less likely to follow the instructions given to them. They also have weaker health status and incur more medical costs (Berkman et al., 2011a; Howard et al., 2005; Nutbeam, 2008).Although the population in this study had relatively high health literacy at the start of the process; the impact might not have been the same if the group had lower general literacy and health literacy at the outset.
Considering the importance of public health knowledge and its key role in reducing the cost of treatment, new paths can be developed to improve the health knowledge of the community (Hamzehei et al., 2018).Health education is one of these methods that can lead to a change in lifestyle and help individuals, families and communities to make informed decisions about issues that are effective in retrieving, accessing, and maintaining health. This style of education can be implemented through public libraries. Public libraries have always been places to access information and are tied to education and learning in the community. Learning services in these libraries are available for all potential and actual people who are referring to the public libraries. This is a clear case for diabetic patients, because it is a commonly known disease of the century (Sanghera, 2016). Many studies have referred to the public libraries as a platform for education as we mention it this study too. In fact, if we notice the educational role of public libraries as a platform in the community, it can be lead to the better managing and controlling the complications of diseases (Linnan et al., 2004; Luo and Park, 2013). In other words, public libraries can extend healthy lifestyles and promote health literacy through their educational role. The results of the present study, like other similar studies, indicate that patient education is very effective in increasing the health literacy of patients (Kandula et al., 2009; McCleary-Jones, 2016; Nutbeam, 2000; Schillinger et al., 2004; Seligman et al., 2005; Sharp and Lipsky, 1999; Toronto and Weatherford, 2015; Yehle et al., 2016). The results are especially important for diabetes which has been recognized as the most prevalent disease of the century (Graham, 2013; Griffin, 2005; White et al., 2010). In many previous studies, the research setting was hospitals and clinics. However, the library has not been used as the setting in any of the studies conducted in this area although library space, compared to hospital, plays a positive role for education. In the hospital, people are placed in a context related to illness and disease, while in the library they feel more relaxed.
In the present study, the intervention was implemented directly and indirectly, which was different from many previous studies. Those referred to the library obtained information about training methods and self-care (via educational pamphlets) in educational workshops and places other than workshops such as at home, in the workplace, while commuting and so on. It seems that studying pamphlets before attending workshops prepared participants to accept the materials referred to in the workshop. If we believe in the capabilities of public libraries in promoting culture and levels of public literacy, such social institutions can be easily used for public training. It is important to focus on training self-care behaviors, control, and informed prevention, especially with regard to diabetes. It is more efficient to promote patients’ health literacy by leveraging all the advantages of public libraries, although it should be noted that there were some difficulties during the present study, such as identifying and explaining the goals to the participants, holding regular classes based on their time-table, and preparing appropriate and accurate outline for the related intervention session. Therefore, ongoing patient education can reduce the risk of long-term complications (American Diabetes Association, 2011).
Conclusion
Politicians concerned with health and health education can use potential facilities of public libraries, achieve the goals determined in their programs, and set the ground for health promotion in society.
Footnotes
Acknowledgments
The present study is based on the study presented for the partial fulfillment of the requirements for the thesis, entitled “A Study of the Effects of Health literacy Education on Diabetic Members of Art & Cultural Organization of Tehran Municipality – Andisheh Cultural Center ” which was presented to the Department of Medical Library and Information Science, Paramedical School, Shahid Beheshti University of Medical Sciences. Also another version of this article was presented to IFLAWLIC 2018 (Kazerani et al., 2017) with some changes.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.