
Abstract
The COVID-19 pandemic disrupted travel behavior and resulted in the emergence of new mobility trends. In this paper, we study the degree to which vaccines played a role in reversing pandemic-induced travel behaviors and contributed to a “return to normal.” Using five waves of original U.S.-based survey data combined with passive smartphone tracking data collected in 2020 and 2021, we show that in the early phases of the pandemic, the behavioral response of people in the United States was heterogeneous: individuals with low levels of concern about being infected with COVID-19 engaged in riskier behaviors than those with higher levels of concern, such as traveling more, eschewing masks, attending large gatherings, and using public transportation. Vaccine availability in early 2021 played a significant role in reducing those concerns, which in turn was reflected in significantly increased mobility and travel frequency. We also found a strong positive association between getting vaccinated and the frequency of using public transportation. Telecommuting and working from home remained high after vaccine availability, but we found that the fraction of full-time employees that worked from home every day significantly dropped. This reduction in fully remote work was no different among vaccinated and unvaccinated people, which suggests that the decision to return to in-person work was not only driven by employees’ safety concerns and preferences, but was also a function of employers’ expectations and their decision to reopen their offices. We discuss the implications of our findings on understanding travel behavior during pandemic impact- and recovery periods.
The COVID-19 pandemic caused unprecedented disruptions to several aspects of everyday life. Before the development of vaccines, government and public officials relied on nonpharmaceutical interventions (NPIs) and health recommendations to control the disease’s spread, including recommending or mandating mask-wearing, avoiding large gatherings, reducing travel, and sheltering in place. Along with widespread office closures and businesses transitioning to working from home, these measures resulted in significant impacts on the transportation system. Despite extensive literature on the changes in travel behavior during the pandemic, research on whether vaccination changed pandemic-induced mobility behaviors has been limited in scope. Our work fills this gap in scholarship and makes several contributions.
First, we examined the dimensions along which travel behavior and compliance with public health recommendations in the early phases of the pandemic differed. Using five waves of original U.S.-based survey data, we analyzed individuals’ reported degree of compliance with mask-wearing recommendations and avoidance of large gatherings in the early phases of the pandemic preceding vaccine availability. We also used passively collected point of interest (POI) data on our panelists and examined whether compliance with public health measures was correlated with the frequency of travel. We then examined whether concern about contracting COVID-19 determined compliance with public health measures and reduced travel activity. Next, using a series of difference-in-difference designs, we examined the role of vaccines in reducing concern about contracting COVID-19 and reversing pandemic-induced travel behaviors. We focused on three main questions: whether getting vaccinated increased individuals’ travel frequency, increased public transportation use, and encouraged a return to in-person work. Our analysis contributes important insights on understanding human behavior and mobility during pandemic impact- and recovery periods.
The rest of this manuscript is organized as follows: Section 2 contains a review of the literature to which we contribute. Section 3 introduces the data we used in this analysis. We present our findings in Section 4, which contains two subsections: 1) early pandemic compliance behaviors, and 2) the effects of vaccination on personal mobility, transit use, and telecommuting. We finish with a conclusion and discussion of the policy implications of our findings in Section 5.
Review of Mobility and Human Behavior During the COVID-19 Pandemic
Before the development and availability of vaccines, public health officials focused on nonpharmaceutical interventions (NPIs) to manage the spread of COVID-19. Multiple studies have examined the effectiveness of NPIs in reducing the risk of contracting COVID-19 and the severity of symptoms. Early evidence from China showed that NPIs effectively reduced the serial interval of SARS-CoV-2, the virus that causes COVID-19, allowing for quicker identification and isolation of cases ( 1 ). Another study attempted to rank the effectiveness of NPIs and found that banning public gatherings, closing entertainment centers, and shutting down citywide public transport were the most effective at slowing the early spread in China ( 2 ). Other work found that reducing the number of daily contacts from 14 to 20 down to 2 contacts per person effectively reduced the reproduction number below the epidemic threshold ( 3 ), and that adherence to NPIs and behavioral mitigation measures strongly predicted mortality ( 4 ). Despite this evidence, public opinion remained divided on the appropriateness of public health recommendations. In the United States, agreement with and support of public health measures has been highly politicized, with multiple studies showing that political ideology is a strong predictor of policy preferences related to NPIs ( 5 , 6 ). This has led to varying levels of compliance and adherence to public health recommendations ( 7 ). Our work joins the literature on the heterogeneity of compliance with NPIs and examines its implications on the transportation system.
We also contribute to the literature on travel behavior impacts of the pandemic and the role that vaccines played in reversing some of the pandemic-induced mobility trends. Multiple studies have examined the initial impacts of COVID-19 on travel behavior ( 8 – 11 ). Other work proposed and illustrated an approach for policy making in a postpandemic world that accounts for future public health threats ( 12 ). Some research, relying on individuals’ reported expectations about their postpandemic behavior, has argued that the increase in telecommuting, decrease in public transit use, and decrease in travel are likely to persist in a postpandemic world ( 13 ).
On the telecommuting front, researchers found that workers would like to maintain their ability to telecommute after the pandemic is no longer a threat. Research conducted by the Pew Research Center shows that, for individuals whose work responsibilities can be completed from home, the fraction of telecommuters increased from 20% prepandemic to 71% during the pandemic. Perhaps more interestingly, half of those individuals expressed their desire to continue telecommuting postpandemic, suggesting a continuation of the pandemic-induced telecommuting trend ( 14 ). Another study showed that the proportion of workers who expected to telecommute at least a few times a week postpandemic was 26%, double that of prepandemic levels ( 13 , 15 , 16 ). More recent work used quasi-experimental designs to quantify the causal effect of telecommuting on noncommute trip generation, and found that telecommuting leads to the generation of new incremental noncommute trips ( 17 , 18 ). To the best of our knowledge, no study has attempted to investigate whether getting vaccinated had an effect on encouraging employees to return to in-person work. We fill this gap.
Like telecommuting, public transportation has been highly affected by COVID-19 and was the most heavily affected transport mode during the pandemic. For example, public transit ridership plummeted by more than 90% in New York City in March 2020 ( 19 ), and similar declines have been observed throughout the United States and globally. A study in Sweden found that transit ridership decreased by 40% to 60% even when transit service reductions were minor ( 10 ). In Japan, a study found larger decreases in public transit mode use relative to car travel in three out of four studied cities ( 20 ). Some studies found that the higher fear of infection and overcrowding on public transit are key drivers of the reduction in demand, with those who perceive public transit as having a higher infection risk being less likely to use it ( 21 , 22 ). One study suggested that the impact on the public transportation system is likely to persist until confidence in those modes is restored ( 23 ). More recent studies suggest that the postpandemic weakness in the use of public transportation is persisting ( 24 , 25 ).
Despite the extensive literature on pandemic mobility, research on whether vaccination changes pandemic-induced mobility behaviors remains limited in scope. A study in Israel found that for tourism-related travel, vaccines did not necessarily affect individuals’ desire to travel ( 26 ). The study has limitations, however: it relies on stated intentions to travel in the future, and used three waves of independent cross-sectional data, meaning that participants varied significantly between different waves. Another study focusing on the tourism industry found that getting vaccinated increases the probability of taking a holiday trip by 11.3 percentage points for vaccinated individuals ( 27 ). Although the study attempted to provide causal evidence on the effect of vaccination, its use of cross-sectional data raises concerns about confounding, even when controlling for observable differences between the vaccinated and unvaccinated groups using regression adjustment and propensity score weighting. Our work expands this literature by estimating quasi-experimental designs and quantifying the effect of vaccines on weekly mobility, transit use, and telecommuting. Note that although the quasi-experimental design and our analysis ensures the internal validity of our results, we do not attempt to address the broader issue of external validity and consider that beyond the scope of the paper.
Data
Data Collection
We used a combination of data collection methods to develop a database that enables a broad understanding of how COVID-19 has affected people’s travel behavior. First, we included passively collected data by SimilarWeb, a mobile audience analytics company with a recruited panel of 100,000 U.S. smartphone users, which comprises individual-level POI visit information as well as basic user sociodemographic data. The POI data include information critical to inferring daily activities of panelists and understanding their daily travel behavior. These data are not continuously tracked GPS traces, but rather inferred individual check-ins at POIs. SimilarWeb uses proprietary technology from a third-party provider to infer the location category from each of the POIs visited. For each individual check-in at a POI, the dataset includes information about the panelist’s arrival and departure times, the category of the location visited inferred using proprietary methods from SimilarWeb, the distance and time traveled to get to each POI, the distance of the POI from the individual’s inferred home and work locations, as well as its zip code, city, and Metropolitan Statistical Area name. These data can further be processed to compute specific mobility metrics of interest (e.g., distance traveled for specific purposes or locations, variability in commute time).
Second, we designed a longitudinal survey to capture a broad snapshot of people’s behavior, beliefs, and attitudes in response to COVID-19. Our surveys included questions about respondents’ employment status, travel and telecommuting behavior, vaccination status, demographic characteristics, and ideological beliefs. Most relevant to the analysis in this manuscript, we asked detailed questions about 1) the number of days each individual has worked, and 2) the number of days each individual worked from home, in the week before their participation in each survey. We include a summary of the survey content in Appendix A. For more details on the data collection design and response rates, the reader can refer to Bouzaghrane et al. ( 28 ). We recruited from a random sample, stratified by U.S. state, of approximately 15,000 members of this panel to conduct five waves of surveys (August 2020, September 2020, December 2020, April 2021, July 2021).
In total, the analysis leverages a panel dataset consisting of five waves of surveys and a total of 1,962 unique respondents. In the first wave, 1,321 individuals responded to the survey—a response rate of about 9%. We then targeted those same respondents in the subsequent survey waves, and supplemented our sample from the original pool of 15,000 members to account for drop-outs while maintaining a sample size of approximately 1,000 participants in each survey wave.
A key advantage of our dataset is the ability to link the individual survey responses with individual POI tracking data: each participant is indexed with a unique identifier that is the same for both the passive survey database as well as the POI database, allowing us to easily match a participant’s survey response to their POI data. This allowed us to supplement the stated survey responses of the study participants with their observed travel behavior. The other advantage of the data is their longitudinal aspect and the ability to observe the evolution of the participants’ behaviors, beliefs, and attitudes over time. The POI data are available from January 2020. The survey data collection started in early August 2020 and collected data in five total survey waves (August 2020, October 2020, December 2020, March 2021, June 2021, see Figure 1). We should note that the nature of the POI data only allowed us to identify whether an individual had commuted to work and did not help us distinguish telecommute days from other nonwork days. As such, we used survey responses about the number of days worked and the number of days worked from home to supplement the POI data. For a deeper dive into the data used in this research, please refer to the data manuscript that provides more details ( 28 ).
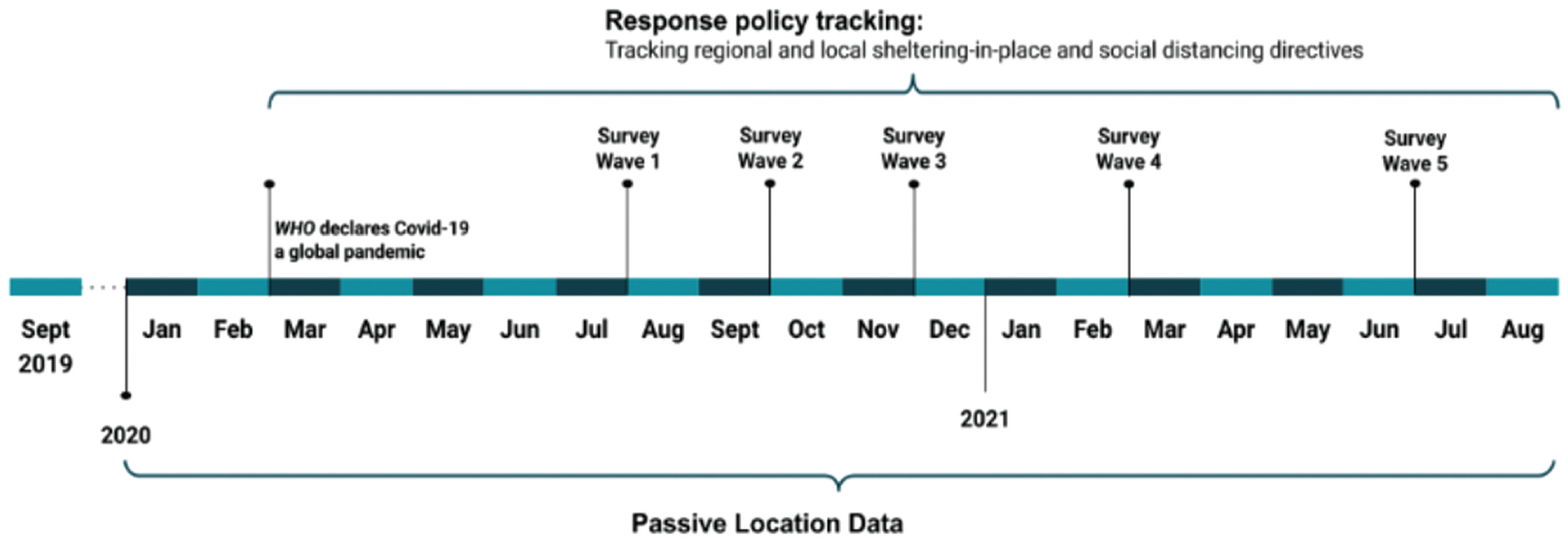
Data collection timeline for passive- and survey data.
Demographic Summary
Table 1 summarizes the demographic characteristics of our survey respondents and compares those characteristics to national statistics from the U.S. census. When compared with the U.S. population, our data undersample men and oversample women. Our data also significantly oversample young adults aged between 25 and 54 years old: this age group represented about 69% to 73% of survey participants (depending on the wave), compared with 39% in the U.S. population. When it comes to household income, our sample overrepresented households with low- and medium-income levels and underrepresented high-income households: about 59% to 65% of the survey respondents earned $50,000 or less a year, compared with only 40% in the U.S. population. Similarly, about 10% to 11% of our respondents belonged to households that earned $100,000 or more a year, compared with 31% of households in the U.S. population. Our sample also underrepresented White Americans and overrepresented other groups. Approximately 72% of the U.S. population are White/Caucasian, compared with approximately 52% to 56% of our respondents across waves. Black respondents represent about 13% of the U.S. population but comprised 18% of our respondents, across all five waves. Our sample underrepresented non-Hispanics/Latinos when compared with the U.S. population, with 75% to 77% of our sample identifying as a non-Hispanic/Latino compared with 82% of individuals in the U.S.
Demographic Characteristics of Study Participants Compared with the U.S. Census
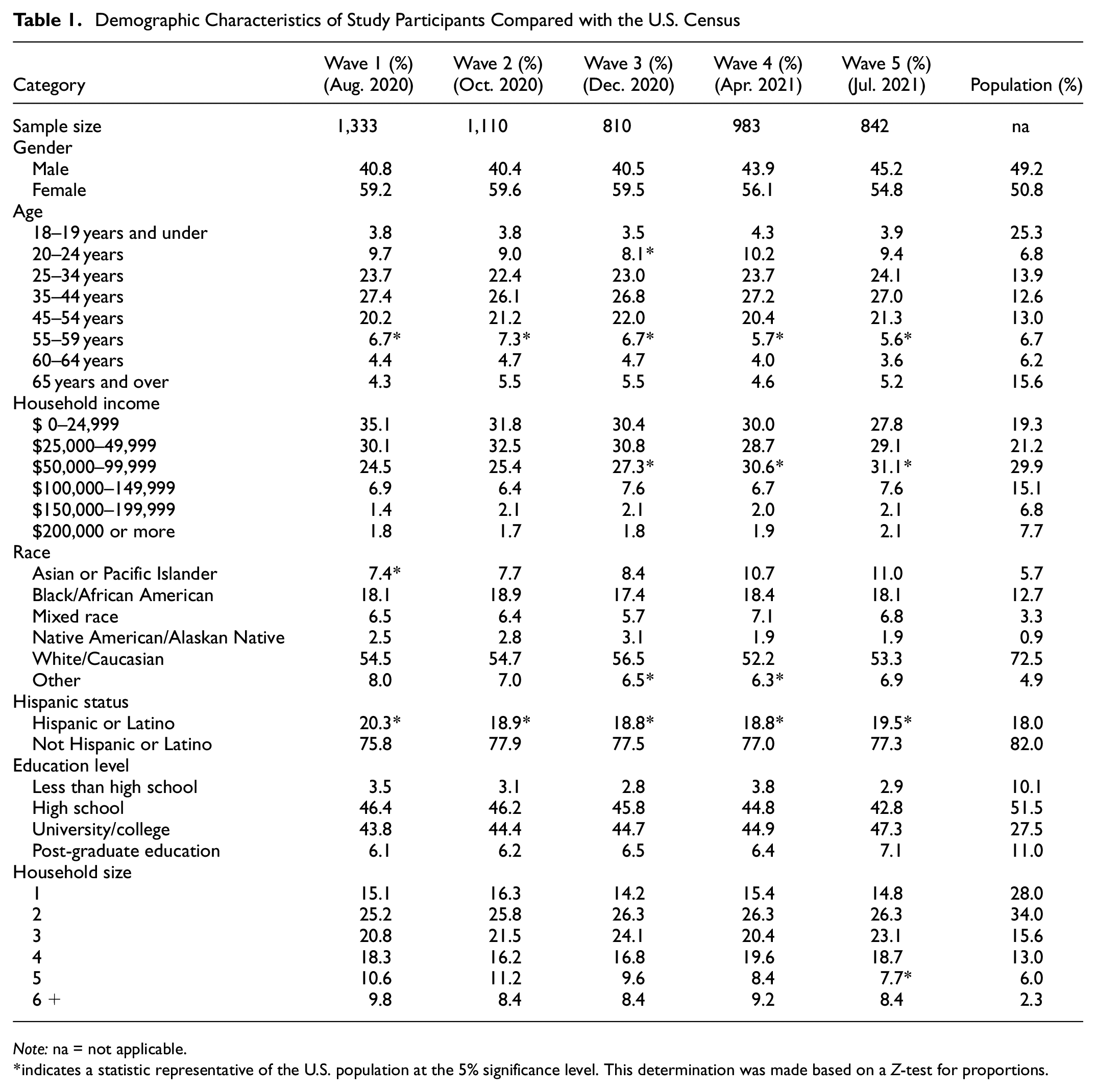
Note: na = not applicable.
indicates a statistic representative of the U.S. population at the 5% significance level. This determination was made based on a Z-test for proportions.
Despite the nonrepresentativeness of some characteristics in our sample, we did not attempt to re-weight observations to match the U.S. population, since our analysis was comparative in nature and controls for demographic differences by design: we investigated the behavior of specific groups relative to other groups and looked at the within-group variation in outcomes, and we did not attempt to present aggregate statistics that are nationally representative. Because of this, our regression results should be seen as internally valid, and more care needs to be taken when attempting to generalize the specific effect sizes to the broader population.
Results
Concern about COVID-19 Explains Compliance with NPIs
Public opinion in the United States has been divided about the severity of the virus and the need for behavioral interventions such as reducing activity and sheltering in place, wearing protective masks, and avoiding large gatherings ever since COVID-19 was declared a global pandemic ( 5 ). Our data strongly confirm this divide: a small fraction of individuals exhibited significantly less compliance with public health recommendations: they traveled more, eschewed mask-wearing, and attended large gatherings at a significantly higher rate than the rest.
An important predictor of people’s compliance with public health measures and mobility levels in our data was the level of concern they had about contracting COVID-19 and the severity of the disease. We found that individuals who were not concerned about contracting the virus (i.e., those who reported being “not worried” or “not too worried” about contracting the virus) were significantly more likely to travel more and exhibited significantly higher mobility relative to those who were very concerned about getting infected (i.e., those who reported being “very worried”). They were also more likely to engage in riskier behaviors such as less frequent mask-wearing where recommended by public health officials and more frequent attendance of large gatherings. Figure 2 illustrates these patterns. These findings confirmed previous literature that found that risk perception and functional fear of COVID-19 were important predictors of behavioral compliance with COVID-19 safety measures ( 29 , 30 ). Our work had significantly more power owing to larger sample sizes relative to the two previous studies in the literature.
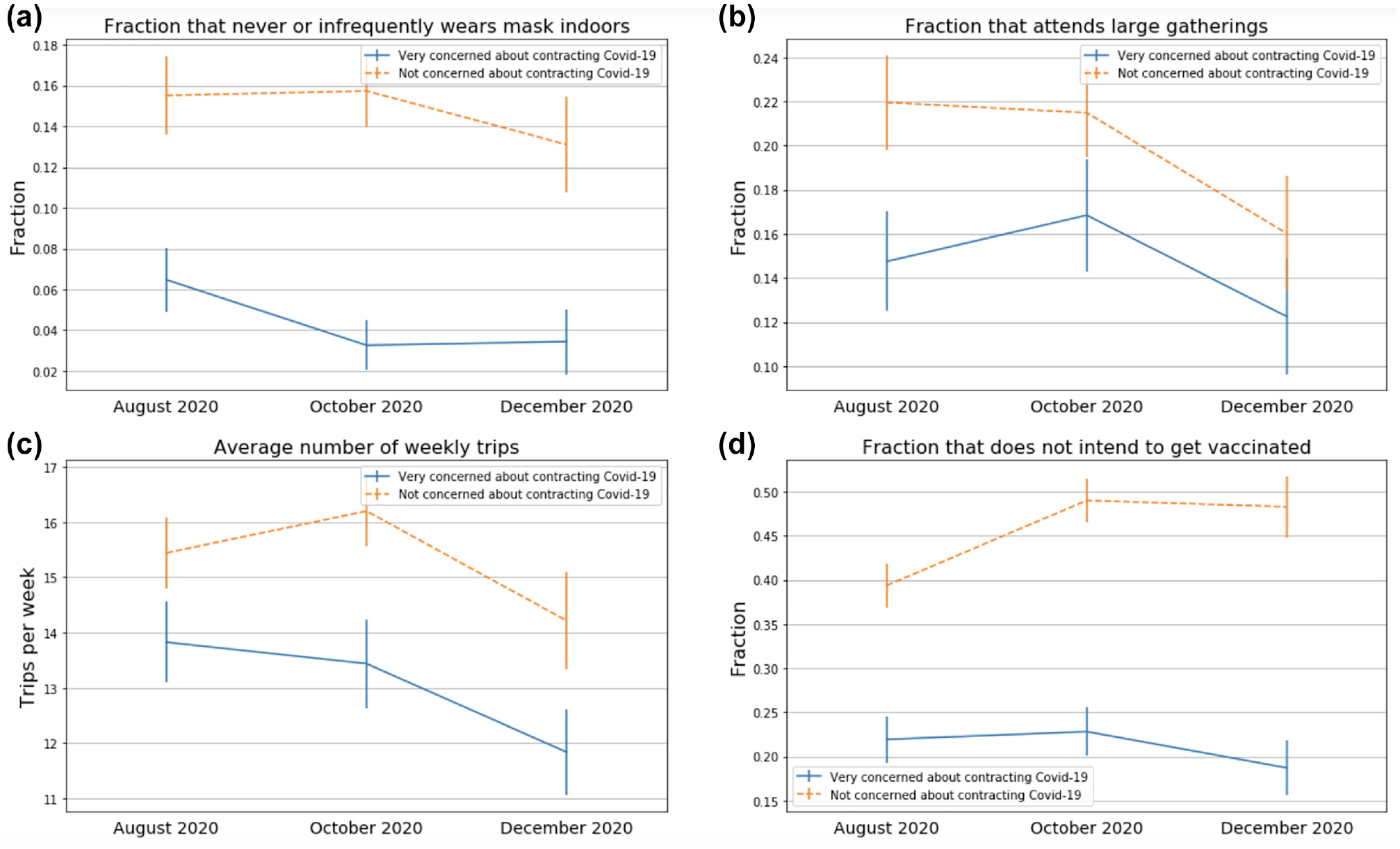
Comparing the behaviors of participants who were concerned (in blue) versus not concerned (in orange) about contracting COVID-19. The behaviors compared are (a) not wearing masks indoors, (b) attending gatherings with more than 10 people, (c) number of weekly trips taken, and (d) unwillingness to get vaccinated (asked before vaccines became available). Lines at the end of each bar are 95% confidence intervals. Sample sizes (very concerned about COVID-19, not concerned about COVID-19): August 2020: (278, 419). October 2020: (184, 356). December 2020: (155, 206).
As expected, we found that those who did not follow one public health recommendation were also less likely to follow others. For example, in our August 2020 survey wave, individuals who attended large gatherings with more than 10 people were five times more likely to never wear masks while socializing with other people, and about four times more likely to never wear masks while traveling in public (p-value < 0.01 for both). These individuals also made more trips, averaging 18.2 weekly trips in August 2020, compared with 14.5 trips for those who did not attend large gatherings. This trend held in the October 2020 and December 2020 survey waves (Figure 3).
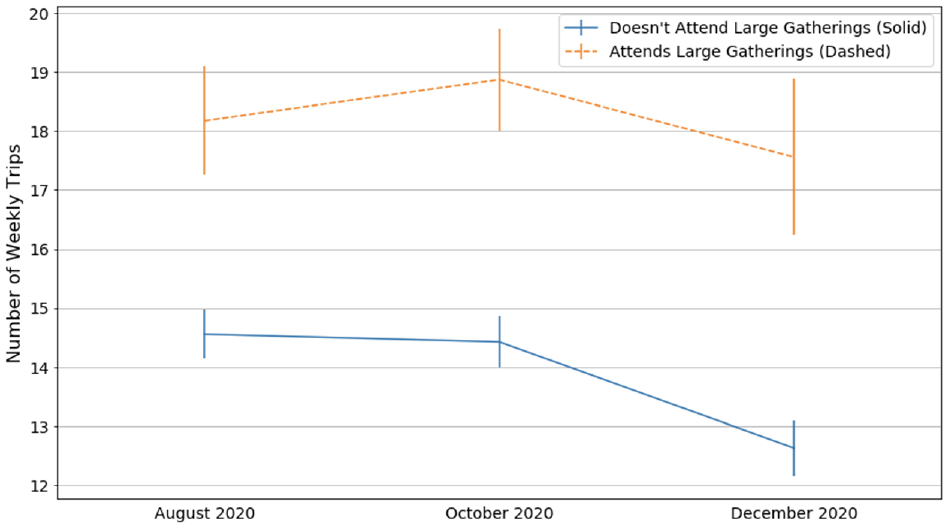
Number of weekly trips (with 95% confidence intervals) exhibited by people who did and did not attend gatherings larger than 10 people.
Similar to NPIs, we found that opinions about the effectiveness, safety, and willingness to get vaccinated varied across segments of the population. We also found a strong association between vaccine hesitancy and compliance with behavioral public health recommendations. Among those who did not follow public health recommendations, a significantly larger proportion reported an unwillingness to get vaccinated: 42% of those who do not wear masks where recommended or attended gatherings larger than 10 people reported being unwilling or unlikely to get vaccinated once vaccines became available. This fraction was 29% in the rest of the population (a 44% difference, p-value < 0.05). At the intersection, that is, for individuals who did not wear masks where recommended and attended gatherings larger than 10 people, the fraction unwilling or unlikely to get vaccinated was 62%, roughly twice as high as the rest of the population. In short, our 2020 data showed that concern about contracting COVID-19 explained some of the behavioral and mobility differences among participants, with more concerned individuals more likely to travel less and comply with public health recommendations. More concerned individuals also showed higher willingness to get vaccinated once vaccines became available. We also found a strong correlation between vaccine hesitancy and compliance with behavioral public health recommendations. In the next sections, we look at how the mobility behavior of the more concerned individuals changed after getting vaccinated, and whether vaccines played a role in alleviating the concerns that kept mobility levels low.
Effects of Vaccination
On Mobility
Our initial survey waves established that following public health recommendations on mobility were, in the early phases of the pandemic, strongly correlated with individuals’ level of concern about contracting COVID-19. As vaccines became the primary tool to combat the pandemic in 2021, a natural question that arises is how getting vaccinated affected the degree to which an individual worried about contracting the disease. And, if levels of concern changed, how did these changes affect travel behavior?
To answer those questions we examined the responses of individuals who got vaccinated by the end of the April 2021 wave of our survey, in which roughly 20% of survey respondents were vaccinated. We limited the analysis to those who got vaccinated by April 2021 to have a more well-defined treatment period (to have included those who were vaccinated in the August 2021 wave would have made the treatment period 8-months long, with no precise information on when the treatment occurred). Our results showed a significant increase in the share of individuals who were not concerned about being infected with COVID-19 among those who received a vaccine (Figure 4), from 25% before getting vaccinated (in the December 2020 survey wave) to 41% after getting fully vaccinated, an increase of about 64% (p-value < 0.01). In fact, Figure 4 shows that getting vaccinated equalized the level of concern about contracting COVID-19 between vaccinated and unvaccinated individuals. Also worth noting is the decrease in concern among those who were not fully vaccinated by the April 2021 wave, although the decrease was much smaller in magnitude compared with vaccinated individuals (Figure 4). This reduction in concern for unvaccinated individuals probably followed the change in public narrative about the pandemic that happened around the time vaccines became available, when government officials adopted a noticeably more optimistic tone ( 31 ).
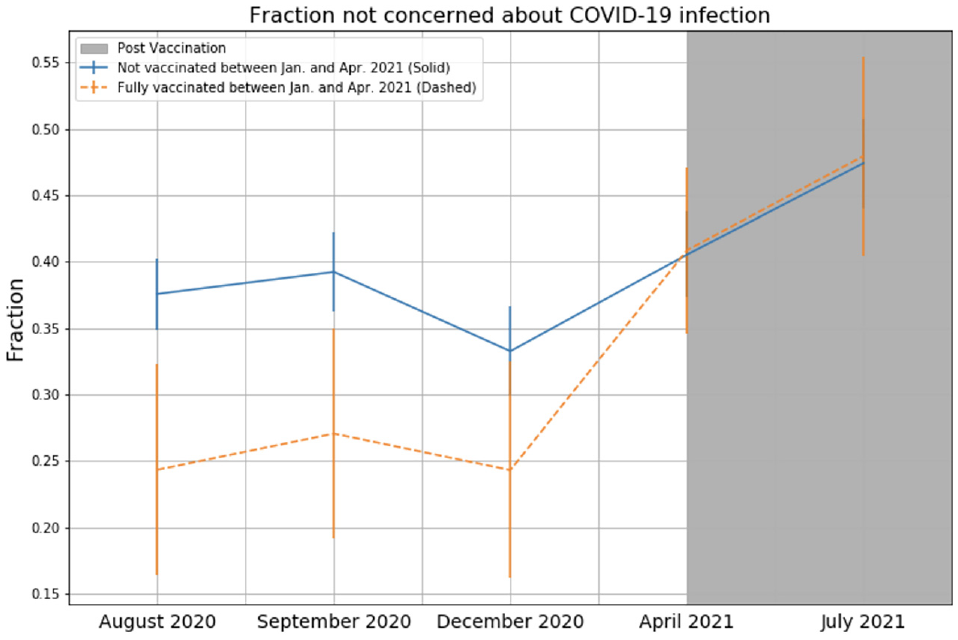
Evolution of the level of concern for those early vaccinated and unvaccinated individuals. Sample sizes: vaccinated = ~190 panelists; not (or partially) vaccinated = ~800 panelists.
In light of this reduced concern about contracting COVID-19 and the previously shown association of this concern with mobility levels, we investigated the effects of vaccines on personal mobility by focusing on survey participants who were fully vaccinated as of the April 2021 survey wave. This corresponded to the first wave of surveys following vaccine availability in the United States. Figure 5 shows the evolution of the number of weekly trips taken by those who got fully vaccinated before May 2021, relative to the rest of the population. Before the onset of the pandemic, in February 2020, the two groups of individuals exhibited similar mobility levels. The figure shows that participants who got vaccinated before May 2021 reduced their mobility more in the early phases of the pandemic. Once vaccinated, however, these participants increased their weekly trips at a significantly faster rate compared with the unvaccinated.
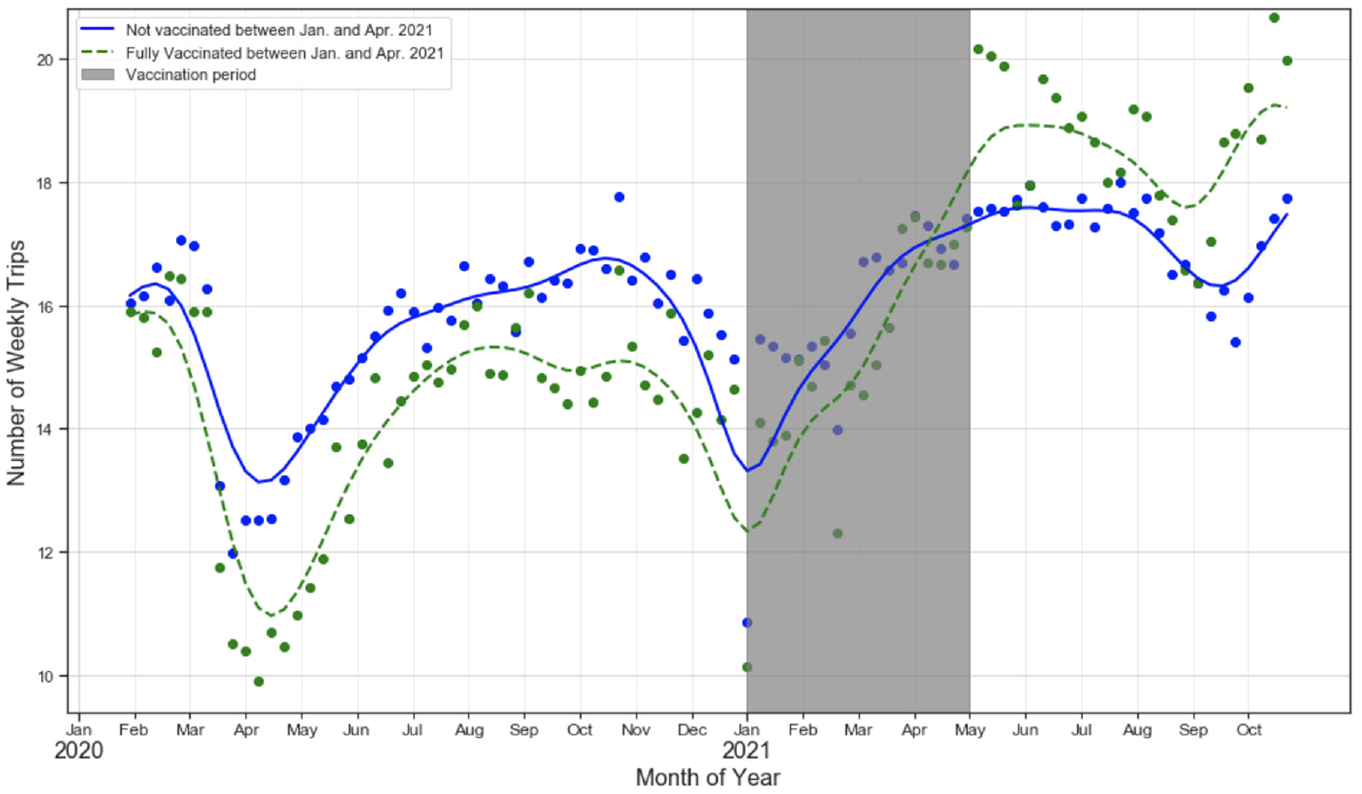
Evolution of the number of weekly trips for vaccinated and unvaccinated individuals. Sample sizes: vaccinated = ~190 panelists; not (or partially) vaccinated = ~800 panelists.
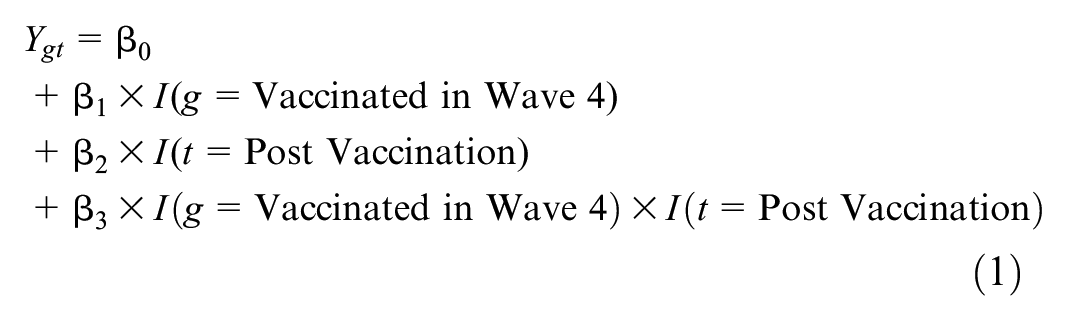
To quantify the net effect of getting vaccinated on weekly mobility, we estimated a difference-in-differences regression where the treatment was the individual’s vaccination status as of the April 2021 wave of our survey and the outcome was the number of weekly trips carried out by an individual, as inferred from the passive mobility data. Our key identification assumption was the parallel trends assumption, that is, that travel activity would have evolved similarly in both groups absent the vaccine rollout. Figure 5 suggests that the parallel trends assumption holds, as the two groups’ average weekly trips tracked closely before January 2021. The grayed-out area is the treatment period between January 1st 2021 and April 30th 2021, corresponding to the early vaccination period in the United States. The posttreatment period is the 4 weeks after the end of the treatment period (May 2021), and the pretreatment period is the 4 weeks before the treatment period (December 2020). Equation 1 shows our structural equation specification: the outcome,
Estimated Coefficients for the Difference-in-Differences Regression in Equation 1. Outcome: Number of Weekly Trips
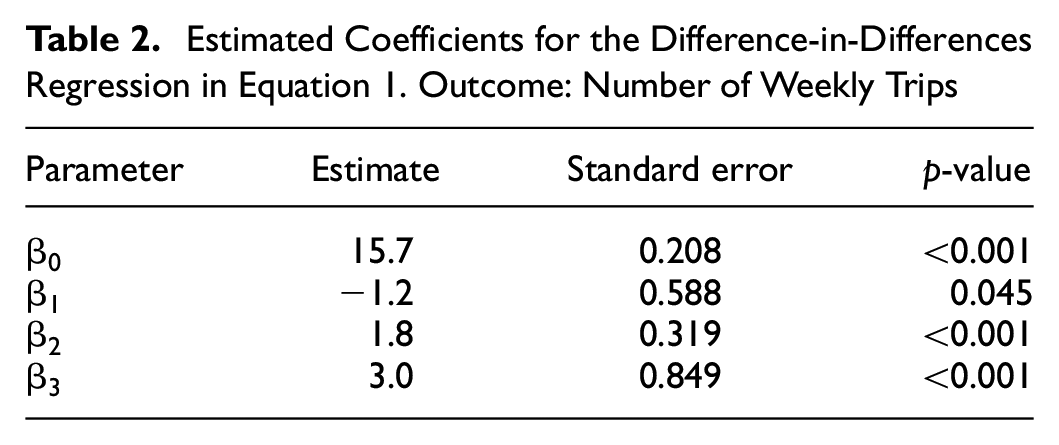
Aside from the vaccine effect, Figure 5 also shows that mobility significantly increased for nonvaccinated individuals, albeit at a slower rate than vaccinated individuals (as shown by the positive and statistically significant
On Transit Use
In our first survey wave (August 2020), when asked about factors that would encourage their increased use of transit, about 39% of prepandemic transit riders indicated that the development of an effective COVID-19 treatment or vaccine would increase their use of public transportation. Data from our postvaccine availability survey waves confirmed that vaccines indeed played an important role in reducing the safety concerns around public transportation and increasing public transportation use, offering a more optimistic perspective on the future of public transportation. As described in earlier sections, worries about getting infected by COVID-19 decreased significantly in 2021 relative to 2020, particularly among vaccinated individuals. This decrease in concern was associated with an increase in public transportation use among vaccinated individuals, where safety has been shown to be one of the main reasons for the reduction in ridership ( 21 , 32 ). In the April 2021 and July 2021 survey waves, about 18% of individuals who got at least one shot of a COVID-19 vaccine before May 2021 reported that they had used public transportation at least once in the preceding 2 weeks. Only 12% of these individuals reported using public transportation in the first three waves of the survey (August 2020, October 2020, December 2020), representing a 50% increase from 2020 to 2021 (p-value < 0.05). There was no significant difference in the frequency of using public transit among those who did not receive any vaccine, with about 15% to 16% of this group reporting using transit in both prevaccine and postvaccine availability survey waves (Figure 6). When it comes to public transportation as a primary mode of commuting to work, we found a similar trend between vaccinated and unvaccinated individuals, albeit among a much smaller sample. Our data showed that between 6% and 7% of all commuters used transit to commute to work, a fraction comparable to the national average of about 5%. This share, and its evolution, differed across the groups of vaccinated and unvaccinated individuals. Of those vaccinated between January and April 2021, only 3% used transit as a primary mode of commute in 2020 (before getting vaccinated), compared with 5.5% after getting vaccinated in 2021, an 80% increase. Among unvaccinated individuals, however, the numbers were roughly the same before and after vaccination (about 7%).
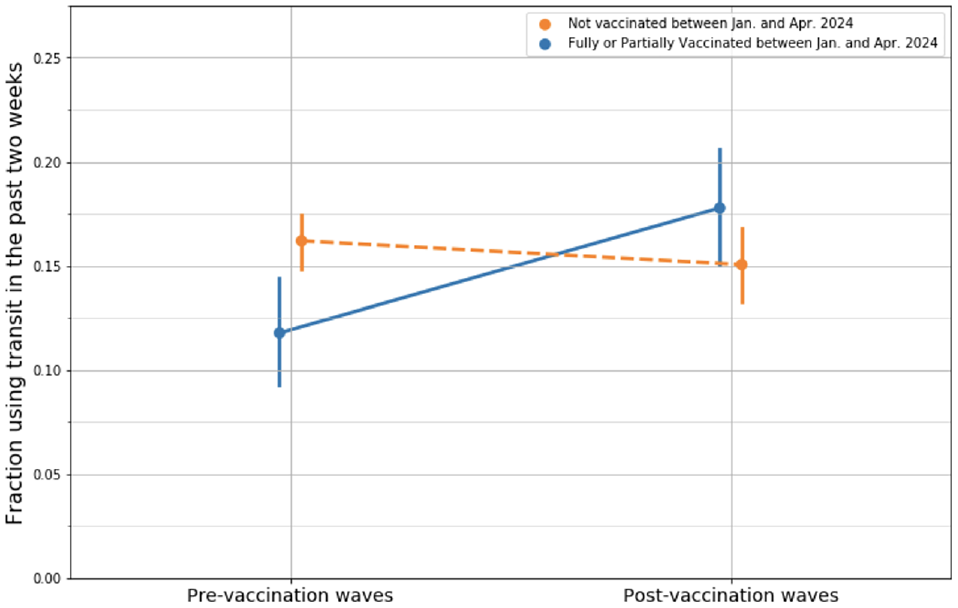
The change in the frequency of using transit for vaccinated and unvaccinated individuals.
This increase in the frequency of using transit among vaccinated individuals was most likely because of the effect of vaccines on reducing concerns about being infected by COVID-19, as shown in earlier sections. Indeed, our data showed that concern about being infected by COVID-19 was strongly correlated with the frequency of using public transit. Across all survey waves, panelists who say they were not concerned about being infected by COVID-19 were 26% more likely to report using public transit in the past 2 weeks (p-value < 0.05)—19% of those who said they were not concerned about being infected by COVID-19 reported using transit at least once in the previous 2 weeks, compared with 15% of those who were concerned.
Our results and data further suggested that addressing safety concerns on public transportation modes could significantly reduce the impact of potential future pandemics on transit ridership, even when transit service changes and reductions are inevitable. In our first wave of surveys, preceding vaccine availability, factors such as the widespread use of face masks and increased sanitation/cleaning on public transit were more frequently reported as measures that would increase transit use (about 45% of transit riders) than factors related to service changes (about 22% of transit riders) ( 32 ). The observed increase in transit use after vaccination provides further evidence that addressing safety concerns will be key to protecting transit ridership in future pandemics and disease outbreaks.
On Telecommuting
Although telecommuting at least once a week remained the norm for the majority of workers in 2021, our data showed a decrease in the share of individuals who fully telecommuted (Figure 7), from a high of 39% in December 2020 to a low of 28% in July 2021 (p-value < 0.001). On the other hand, the number of people commuting to work on every workday increased by approximately 16%, from a low of 50% in December 2020 to just above 58% in July 2021 (p-value < 0.01). These results suggest that whereas partial telecommuting continues to be an option for a significant portion of workers, full remote work will not remain the norm in a postpandemic world. Hybrid work models seem to be the most likely outcome, and this trend will have significant implications on congestion and traffic patterns.
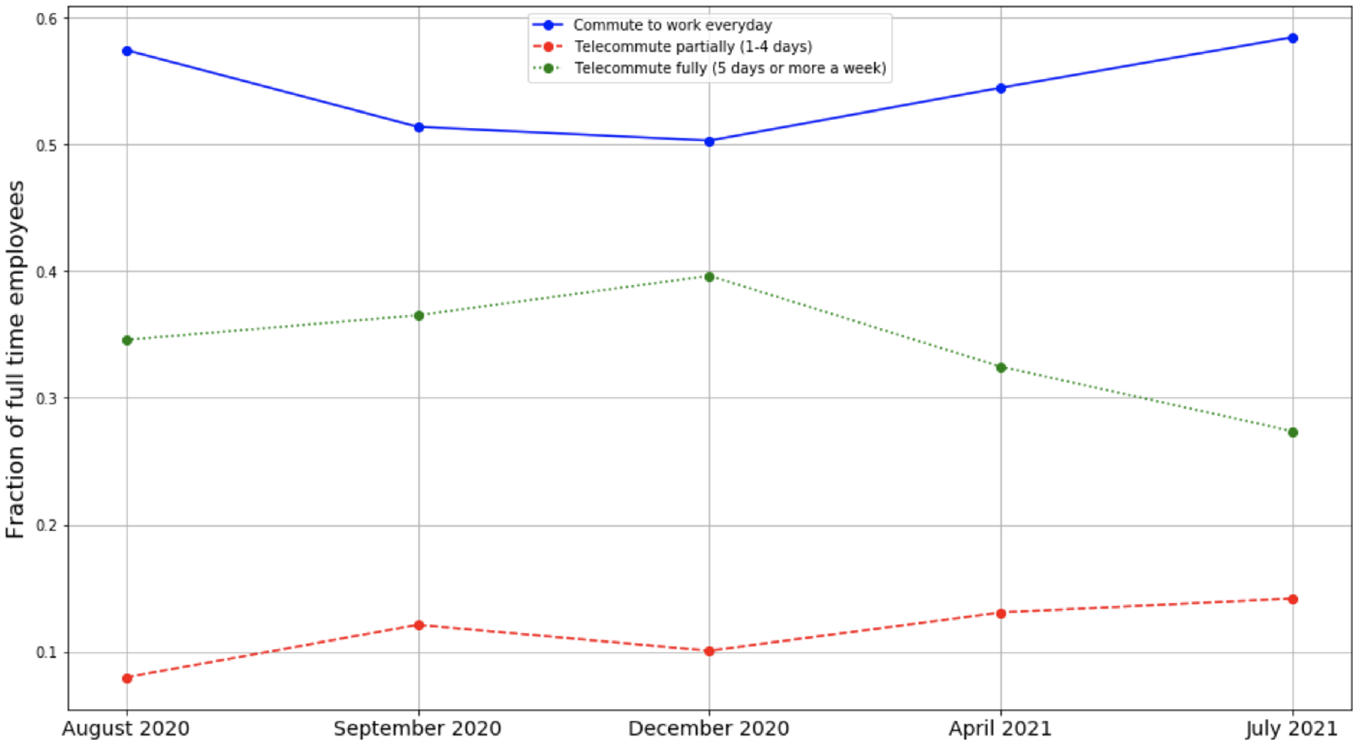
The frequency of commuting and telecommuting to work for fully employed panelists. We define fully employed as those who report working at least 5 days a week in the past week. The number ranges from 402 to 477 depending on the wave, except for the third wave in December 2021 when the number drops to 328 (most likely because of vacation time).
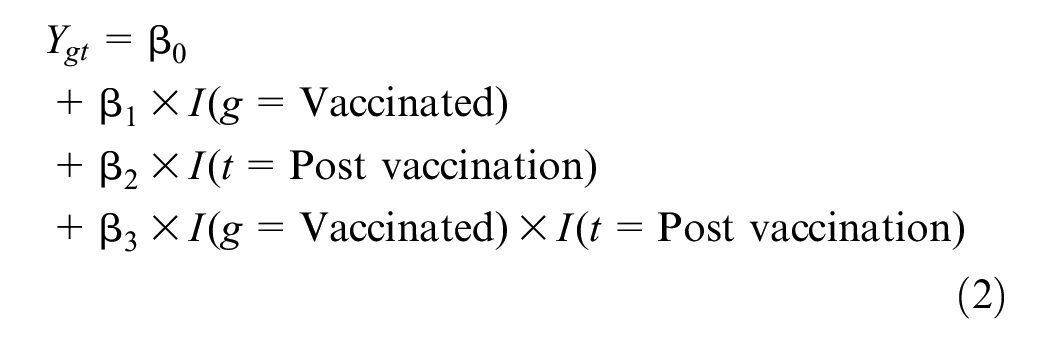
In contrast to our general travel behavior results, the observed decrease in the frequency of telecommuting was not significantly different between vaccinated and unvaccinated individuals. To measure the impact of vaccination status on telecommute frequency, we estimated a similar difference-in-differences design for two cohorts: Fully employed participants who got vaccinated between January and April 2021 compared with those who did not (hereafter referred to as the fourth wave cohort), and fully employed panelists who got vaccinated between April and July 2021 compared with those who did not (hereafter referred to as the fifth wave cohort). The number of vaccinated and unvaccinated individuals (i.e., sample size) in the fourth wave cohort was 143 and 316, respectively. In the fifth wave cohort, the number of vaccinated and unvaccinated individuals was 152 and 156, respectively. The models’ specification is shown in Equation 2: the outcome,
Estimated Coefficients for the Difference-in-Differences Regression in Equation 2. Outcome: Fraction of People Working Fully Remotely
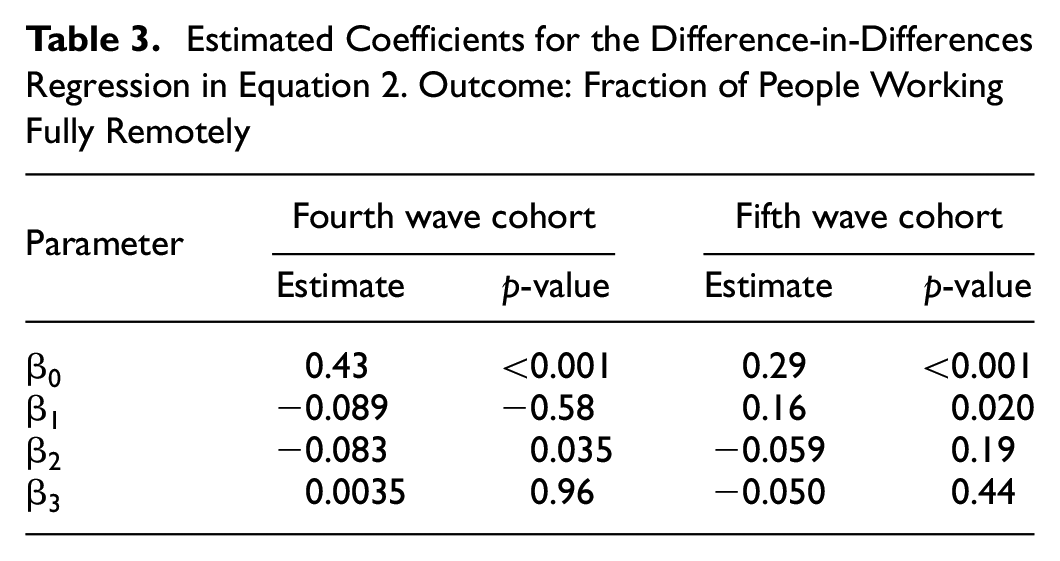
Our estimates for the effect of getting vaccinated were insignificant in both cohorts. The similar drop in telecommuting rates for both the vaccinated and unvaccinated, as shown in the small and statistically insignificant parameter
Conclusion and Policy Implications
This work contributes to the understanding of human- and travel behavior during pandemic impact- and recovery periods. First, we showed that the changes in the frequency of travel, as well as compliance with public health recommendations more broadly, differed for different groups of people. Although the majority of the participants in our study complied with public health recommendations and significantly reduced their travel, a minority did not. These two groups had significantly different levels of concern about contracting and spreading the disease, and we found that higher concern was strongly associated with higher compliance and reduced travel. Next, we showed that vaccination played a significant role in reducing concern among vaccinated individuals, which in turn affected their travel behavior. We estimated difference-in-differences regressions leveraging the longitudinal aspect of our dataset and found that vaccines played a significant role in reversing some of the pandemic-induced mobility trends. We showed that vaccines led to a significantly higher increase in mobility for vaccinated individuals relative to the unvaccinated. We also showed that the frequency of public transportation use significantly increased for vaccinated individuals in 2021 relative to 2020, whereas it remained the same for the unvaccinated. With telecommuting, we saw a significant drop in the fraction of full-time employees that worked from home every day in 2021 relative to 2020, but the fraction of employees telecommuting at least once a week remained high at 42% in August 2021. The drop in fully remote work was not significantly different between vaccinated and unvaccinated individuals, suggesting that decisions to return to in-person work were not only driven by individual safety concerns and preferences, but were also likely to have been a function of employer expectations, and that the high telecommuting rates may well persist in a postpandemic world.
Our results have several implications on policy making during pandemic times:
Insight #1: We showed that in the early phases of the pandemic preceding vaccine availability, although the majority of individuals in our panel complied with public health recommendations, a minority did not. This minority carried significantly more risk of contracting and spreading the disease by engaging in multiple noncompliant behaviors at the same time. For example, whereas only 18% of our panelists reported attending gatherings larger than 10 people in the August 2020 wave of the survey, these individuals were five times more likely to not wear masks while socializing with others, and four times more likely to not wear masks while traveling in public (using public transportation or shared mobility services). We also find that these individuals traveled significantly more than others in the early phases of the pandemic, increasing their risk of spreading the virus and highlighting the role of the transportation system in propagating the disease.
The concentration of “behavioral” risk—risk associated with noncompliant behaviors like eschewing masks, attending large gatherings, traveling more, and so forth—among a small subset of individuals draws parallels to the literature on superspreading: similar to how a small number of individuals were shown to cause the majority of cases in the early outbreak of the disease, a small number of individuals carried a disproportionately higher risk of contracting and spreading the disease based purely on their behavior and noncompliance with multiple recommended safety protocols. From a policy standpoint, additional evidence that superspreading can be, at least partially, explained by human behavior, rather than being a fully biological phenomena, is positive. It suggests that policies aimed at managing human behavior could be effective at controlling the spread of the disease absent any vaccines or pharmaceutical interventions. A key to the success of those policies, however, is ensuring high compliance from the public. Some work suggested that the overdispersed nature of the spread is its Achilles’ heel ( 34 ), since this allows interventions to focus on key behaviors that feature a high number of interactions like indoor events and large gatherings. Our work suggests that this may be an oversimplification of the problem, however, since people who engage in those activities are also the ones who are resistant to behavioral interventions. For example, our August 2020 survey data showed that those who did not wear masks where recommended by public health officials are 181% more likely to believe that COVID-19-related restrictions were too strict (p-value < 0.001). This implies that simply mandating public health recommendations is not likely to be effective on the people whose compliance is needed most. Previous work studied how political ideology and demographic factors can predict the perception of threat of COVID-19 ( 5 , 6 ), which we showed predicts compliance. More work is needed to develop communication strategies that speak to different demographic and ideological groups and are effective at engaging those with low safety concerns to improve their compliance with behavioral prevention measures.
Insight #2: The second important implication of this work relates to the role of vaccines in reversing safety concerns and inducing a return to prepandemic mobility levels. The literature on the effect of vaccination on pandemic mobility is limited, with studies providing conflicting findings. Our data clearly showed the positive effect of vaccination on weekly mobility for the vaccinated early in 2021. Our data also suggests that the mediator through which vaccination affected mobility was likely to be the level of concern about contracting the disease: concern about contracting COVID-19 was highly correlated with mobility levels (Figure 2), and vaccines were very effective at reducing concern among vaccinated individuals (Figure 3). The effect of vaccines on easing concerns and increasing mobility was not limited to vaccinated individuals: our data importantly showed that both vaccinated and unvaccinated individuals significantly increased their mobility right after vaccines became available in early 2021 (Figure 5). The ease in concern among unvaccinated individuals coincided with the significantly more optimistic rhetoric adopted by government and public health officials in early 2021. This reduction in concern and increase in mobility early in 2021, especially among unvaccinated individuals, poses problems for public health and government officials. Multiple studies have found that reduced mobility can have a similar effect on the number of infections and hospitalizations ( 35 , 36 ) as vaccination, with one study suggesting that the effect of mobility reduction is similar to that of a 30% vaccination rate with 70% to 90% vaccine efficacy ( 35 ). This suggests that, at least in the early days of vaccine availability when vaccination rates are still low, the net effect of vaccine availability on transmission and hospitalization numbers can be negative if safety protocols (e.g., mask-wearing) and government restrictions are eased prematurely. Political and public health messaging should be careful to avoid narratives that suggest the pandemic is over, as this can result in a premature sense of safety that could decrease the motivation to comply with behavioral safety measures.
When it comes to public transit, we found a significant increase in the frequency of using public transport among those who got vaccinated early. We also found a high correlation between the concern about contracting COVID-19 and using public transit across all our survey waves, with 19% of nonconcerned individuals using public transit in the past 2 weeks, compared with only 15% of the concerned individuals. Our results collectively showed that safety concerns were an important reason for the public transit ridership declines during the pandemic, and consequently, dealing with safety concerns through improved sanitization, adding capacity constraints, and enforcing NPIs like requiring mask-wearing could soften the magnitude of ridership declines in future pandemics and public health outbreaks.
Insight #3: The third implication of this work relates to our finding that telecommuting will remain high after the pandemic is over. Our data also gives insight into the reasons why people chose to return to work, showing that safety was not an important factor in that decision. We showed this by demonstrating that getting vaccinated did not affect the magnitude of the reduction in telecommuting rates, despite significantly affecting the level of concern about contracting the disease. In addition to the lack of vaccination effect, our data also suggested that working fully remotely was not going to remain the norm for many employees, as evident in the sharp decrease in the fraction of people working fully remotely in 2021. Hybrid telecommuting models seem likely to persist, and travel demand models need to account for this new trend, which has several implications for congestion, peak hour commute, and trip making in general. The literature on the transport impacts of telecommuting remains conflicted: recent evidence suggests that telecommuting results in the generation of additional noncommute trips, but a net reduction in total (commute and noncommute) trip making ( 18 ). With high telecommuting rates likely to persist postpandemic, more comprehensive analyses on the transport impact of telecommuting are needed to appropriately account for its impact in travel demand models, environmental impact reports, and emission analyses.
Supplemental Material
sj-docx-1-trr-10.1177_03611981241249924 – Supplemental material for Early Pandemic Behaviors and the Role of Vaccines in Reversing Pandemic Mobility Trends: Evidence from a U.S. Panel
Supplemental material, sj-docx-1-trr-10.1177_03611981241249924 for Early Pandemic Behaviors and the Role of Vaccines in Reversing Pandemic Mobility Trends: Evidence from a U.S. Panel by Hassan Obeid, Michael Anderson, Mohamed Amine Bouzaghrane, Meiqing Li, Madeleine Parker, Drake Hayes, Karen Frick, Daniel Rodriguez, Daniel Chatman, Raja Sengupta and Joan Walker in Transportation Research Record
Footnotes
Acknowledgements
We would like to thank the University of California Center for Information Technology Research in the Interest of Society and the U.S. Department of Transportation Tier 1 University Transportation Center on Telemobility for their funding support. We also thank Embee Mobile for providing access to the mobility data used in this research, as well as access to their mobile platform to administer surveys to their panelists.
Author Contributions
The authors confirm contribution to the paper as follows: study conception and design: H. Obeid, M. Anderson, M. Amine Bouzaghrane, M. Li, M. Parker, D. Hayes, K. Frick, D. Rodriguez, D. Chatman, R. Sengupta, J. Walker; data collection: H. Obeid, M. Anderson, M. Amine Bouzaghrane, M. Li, M. Parker, D. Hayes, K. Frick, D. Rodriguez, D. Chatman, R. Sengupta, J. Walker; analysis and interpretation of results: H. Obeid, M. Anderson, J. Walker; draft manuscript preparation: H. Obeid. All authors reviewed the results and approved the final version of the manuscript.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by the University of California Center for Information Technology Research in the Interest of Society and the U.S. Department of Transportation Tier 1 University Transportation Center on Telemobility.
ORCID iDs
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.