
Abstract
Empirical data from the past 50 years have illuminated some of the factors that influence pregnancy decision-making. Yet, formal models of pregnancy decision-making are uncommon and rarely incorporate cultural perspectives. In order to address this gap in the literature, we propose the Pregnancy Decision-Making Model (PDMM), a comprehensive model of the factors that are likely to affect pregnancy decisions in the context of unintended pregnancy, with special attention to relational and intersectional components of pregnancy decisions. The PDMM begins with three primary Evaluation factors: Evaluation of Capital, Evaluation of Values, and Evaluation of Narratives. Barriers to Access are proposed to be a key factor in limiting agency and autonomy and determining pregnancy outcomes. Social Influences are also hypothesized to influence Evaluation factors and their relationship with outcome variables, which include the Pregnancy Outcome, Decisional Certainty, and Decisional Satisfaction. As the PDMM is designed to be flexible in its prediction of a variety of outcomes, we consider a number of possible permutations of the model. Finally, we discuss the utility of the PDMM for inspiring future research, as well as the practical implications of the model.
Since the decision of Roe v. Wade in the United States (U.S.), research on abortion and pregnancy decision-making has expanded significantly, with scholars aiming to understand the phenomena of unintended pregnancy outcomes. Specifically, psychological researchers have explored the relationship between mental health and abortion (Major et al., 2009) and the correlates of abortion attitudes thoroughly (Hodson & MacInnis, 2017; Huang et al., 2016). But the process of pregnancy decision-making and the consideration of psychological factors that may influence pregnancy decisions have rarely been explored. Given recent calls for psychologists to contribute to reproductive justice research (Grzanka & Frantell, 2017; Mollen et al., 2018), we aim to improve public understanding of the psychological process of pregnancy decision-making in the context of unintended pregnancy.
The scope of this topic cannot be understated; unintended pregnancy is extremely common and has been found to cause health consequences for pregnant people and their families/ children (Logan et al., 2007; Steinberg & Rubin, 2014). Nearly 215 million pregnancies occur worldwide each year, with global estimates suggesting that 40%–45% (about 85 million) are unintended (Bearak et al., 2018; Sedgh et al., 2014). Rates of unintended pregnancy are similar between developed (46%) and developing nations (43%) but vary by region and culture, with rates as high as 72%–73% in Caribbean and South American regions (Bearak et al., 2018; Logan et al., 2007; Steinberg & Rubin, 2014). Global data indicate that 50%–60% of unintended pregnancies end in abortion, 13% in pregnancy loss/miscarriage, and 38% in live birth; these rates appear to vary based on national and cultural variables (Bearak et al., 2018; Sedgh et al., 2014). While analysis of large-scale datasets of pregnancy outcomes helps us understand more about the demographic factors implicated in abortion and pregnancy (Adamczyk, 2008; Bryant et al., 2010), researchers have yet to produce a comprehensive model that includes psychological and cultural factors to explain pregnancy decision-making. Existing theories and models are quite dated (Shaw et al., 1979; Smetana & Adler, 1979) and do not incorporate modern cultural complexities. Thus, in this paper we introduce the Pregnancy Decision-Making Model (PDMM) to explain the factors that influence people’s pregnancy decisions in the context of unintended pregnancy. We integrate psychological constructs and culturally grounded justice frameworks into the model, providing depth and nuance to pregnancy decision-making.
The Construction and Scope of the PDMM
We developed the PDMM based on our synthesis of knowledge gained from the academic literature and hands-on engagement in the reproductive justice movement. The first author conducted a comprehensive literature review of pregnancy decisions and outcomes, unintended pregnancy, abortion experiences and attitudes, and other pregnancy-related topics, paying particular attention to transnational perspectives and studies of pregnancy in the context of marginalization. We also reviewed literature on health behavior and applied decision-making. In addition to a literature review, the PDMM was informed by the first author’s experience of working with a reproductive justice non-profit organization for four years. During this time, the first author volunteered on a national pregnancy support hotline, speaking with hundreds of people facing unintended pregnancy. This hands-on experience was bolstered by frequent trainings and conversations with fellow volunteers. These experiences, in conjunction with the literature review, led the first author to a broad understanding of the myriad factors that might affect pregnant people in a variety of social locations. The PDMM represents the authors’ integration of both formal academic literature and the lived experiences of people facing unintended pregnancy.
Scope of the PDMM
Due to the fraught political rhetoric and legislation around reproductive decision-making and abortion, it is essential to clarify the proposed limits of the PDMM. Below is a description of the populations and uses for which the PDMM is intended and not intended.
Populations
The group of people who may face making a pregnancy decision is a diverse one; thus, the PDMM is intended to be applicable to a vast and varied group of people. First, we use the term “pregnant person” rather than woman in order to be inclusive of transgender men and people who identify as non-binary who also experience pregnancy (Obedin-Maliver & Makadon, 2016). The PDMM is designed to account for diverse experiences of gender identity during unintended pregnancy. Of note, we do utilize gender-specific language in this paper when referencing studies that only involved women or female-identified participants.
Next, the PDMM applies only to pregnancy decisions that result from unintended pregnancies, in the absence of fetal anomalies or imminently life-threatening situations. Pregnancy decision-making in the context of fetal anomaly is fraught with qualitatively different circumstances, including that these decisions often occur much later in the pregnancy and in pregnancies that are considered wanted (Kerns et al., 2018). Therefore, we do not include circumstances of decision-making in the context of fetal anomaly in the PDMM. Additionally, when the life of the pregnant person is in immediate danger, people often make decisions in such a qualitatively different way that the PDMM would be of little consequence.
Finally, the PDMM is crafted using research with pregnant people around the globe; thus, it is intended to be internationally-applicable, although the relative weight of the constructs in predicting pregnancy decisions will likely vary across culture and geography. For example, we propose that the model is applicable in places where abortion is legal, as well places where abortion is inaccessible, limited, or illegal. Access to abortion is a limiting factor that has disproportionate influence on a person’s pregnancy decision and will therefore affect pregnant people to varying extents across the globe. Despite its broad applicability, many of the examples in this paper are based on the U.S. sociopolitical context; the PDMM may need to be changed or adapted to account for pregnancy decision-making in diverse regions of the world, for example, based on specific economic, policy, or cultural issues (e.g., China’s historical one-child policy).
Utilization
We present the PDMM with two specific purposes in mind. First, we hope that the PDMM, which incorporates cultural frameworks, will prompt culturally grounded intersectional research that identifies the strengths of and barriers for pregnant people in a variety of social locations. Second, it is our aim that psychologists, counselors, social workers, and other clinicians can use the PDMM to gain awareness of the factors that might influence a pregnant person’s pregnancy decision. Through this increased awareness, healthcare providers will be more prepared to have compassionate and non-judgmental conversations with clients/patients about pregnancy and will be open to a nuanced cultural view of pregnancy outcomes.
Given the frequency of sociopolitical strategies to limit reproductive access and autonomy, it seems necessary to identify how the PDMM is not to be used. First, while the PDMM could be useful to reference in discussions with pregnant people in clinical or healthcare settings, it is not designed to be a decision-making tool. Whereas decisional tools/aids often incorporate factual information about pregnancy options and are written specifically to be used by pregnant people, the PDMM does not meet these or other specified criteria (Donnelly et al., 2018). Furthermore, and more importantly, the PDMM is designed from a reproductive justice framework and therefore should never be used in efforts to coerce pregnant people or otherwise limit their autonomy, agency, or access in pregnancy decision-making. Unlike other models of health behavior, which are often used to identify opportunities for behavior change, the PDMM was not designed to change pregnant people’s decisions. Rather, it was crafted to illuminate a decision-making process that is often condescendingly questioned (Landsbaum, 2016), to add cultural nuance to an often-heteronormative and Eurocentric area of study, and to promote justice initiatives that enable access and autonomy in decision-making.
The Integration of Social Justice and Intersectional Cultural Constructs
In the past few decades, two major conceptual developments have arisen which deserve significant consideration in the context of pregnancy decision-making. In the brief overview below we offer a summary of the constructs (intersectionality and reproductive justice) and cover their inclusion in the PDMM and recommendations for incorporating them in future research.
Intersectionality
Movements in cultural psychology and multiculturalism have significantly benefitted from the introduction of intersectionality, a construct developed through decades of activism and scholarship by Black women in the United States (Combahee River Collective, 1995; Collins, 1990; hooks, 1981). The term intersectionality was formally coined by legal scholar and activist Kimberlé Crenshaw to illuminate the ways in which oppressive forces combine to create increasingly complex intersections of marginalization (Crenshaw, 1989, 1991). Feminist psychologists have worked toward integrating intersectionality into psychological research and have called for the translation of research into activism (Moradi & Grzanka, 2017; Rosenthal, 2016); these ideas align with our hopes for the PDMM.
Using an intersectional framework requires two unique approaches to pregnancy decision-making work: first, this work must center the voices of marginalized groups and work collaboratively with communities whose social locations may create additional barriers to autonomy in pregnancy decision-making. This could mean conducting future research with multiply marginalized populations, such as immigrant women or queer people of color, in order to honor and illustrate the unique experiences of pregnant people who have not been represented in previous research. Second, intersectional work on pregnancy decision-making necessitates looking beyond static demographic categories to understand the social forces that create structural inequity. For example, instead of analyses that show racial or class differences in pregnancy attitudes, research ought to incorporate psychological constructs (e.g., identity development) as explanatory variables. Researchers must also consider historical influences, such as the impact of slavery, the forcible sterilization of women of color, or the entanglement of early abortion advocates with eugenicists, to examine how they affect pregnancy outcomes today (Carey, 2012; Khan, 2019; O’Sullivan, 2016; Ross, 1992). In the PDMM and subsequent intersectional research, these two implications are essential.
Reproductive Justice
In contrast with previous movements for reproductive rights or reproductive health which center on legal or medical frameworks, reproductive justice represents the fusion of reproductive rights with social justice (Price, 2010; SisterSong Women of Color Reproductive Justice Collective, 2018). Reproductive justice was developed by the Women of African Descent for Reproductive Justice in 1994 and is defined as “the human right to maintain personal body autonomy, have children, not have children, and parent the children we have in safe and sustainable communities” (SisterSong Women of Color Reproductive Justice Collective, 2018). Reproductive justice is an intersectional movement designed to address the interconnectedness of power structures that create injustice; reproductive justice activists work in solidarity with activists across other justice movements to promote full reproductive autonomy and access (Chrisler, 2012).
The use of a reproductive justice framework also requires us to incorporate three unique viewpoints to research on pregnancy decision-making. The first is that reproductive justice does not focus only on choice (i.e., reproductive justice ≠ pro-choice), but rather centers on access. Thus, research on people’s pregnancy outcomes cannot simply involve attitudes and intent; it must include an analysis of access to resources such as reproductive health care and economic resources. Therefore, when we refer to pregnancy decision-making in this paper, we do so with the recognition that many pregnant people are making decisions in severely constrained situations in which they do not have full access to all options. Second, reproductive justice is not just about abortion access; rather, the movement represents the interests of people who are pursuing access to other reproductive options (e.g., parenting, adoption, surrogacy, being childfree) and their ability to do so autonomously. Thus, the PDMM is framed in the context of pregnancy decision-making (rather than abortion decision-making) because it explores people’s ability to choose and access whatever pregnancy decision is right for them. Finally, using a reproductive justice framework requires recognition of the connections between reproductive and racial, economic, and other forms of justice; thus, pregnancy decision-making research should describe how oppression and inequity in other areas of life (e.g., gender violence or incarceration) influences pregnancy outcomes and decision-making. Given the importance of reproductive justice and intersectionality frameworks and their relevance to an issue that is inherently influenced by inequity, it is imperative that the PDMM and future research on pregnancy decision-making incorporate them.
The Proposed PDMM
With the aforementioned considerations in mind, we now describe the proposed model of pregnancy decision-making. The model is comprised of three primary areas of evaluation that a pregnant person is likely to consider when faced with an unintended pregnancy, as well as a variable to explain the impact of social influences. Barriers to access are hypothesized to be the greatest determinant of pregnancy-related outcomes. We include three outcome variables: the pregnancy outcome (i.e., abortion, parenting, or adoption), decisional certainty, and decisional satisfaction (Figure 1). We begin by exploring the model’s three areas of evaluation.
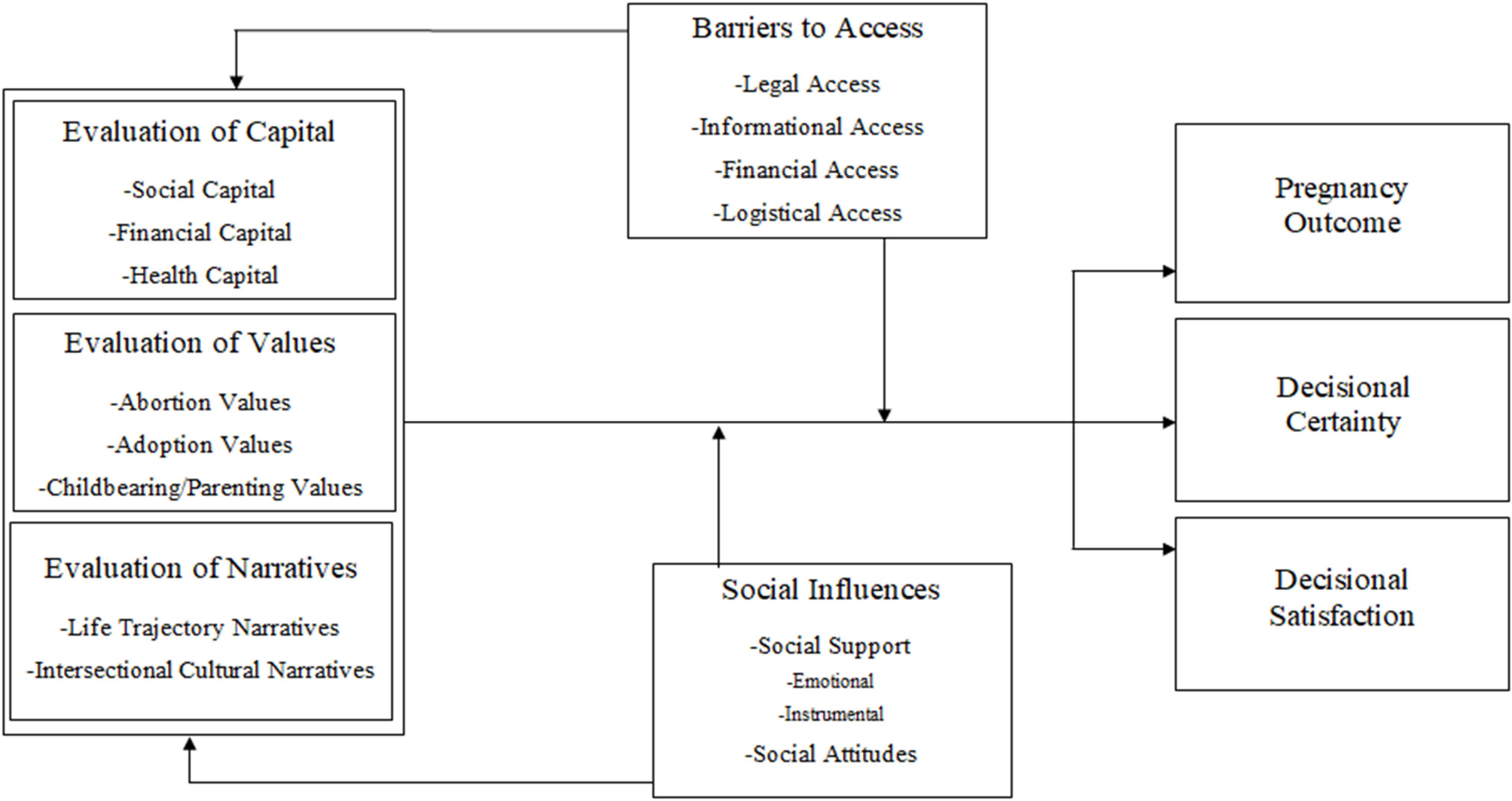
The Pregnancy Decision-Making Model (PDMM). This figure outlines the major components of the PDMM, including predictor and moderating variables (the three evaluation factors, barriers to access, and social influences) as well as the outcome variables: pregnancy outcome, decisional certainty, and decisional satisfaction.
Three Areas of Evaluation
The PDMM addresses three areas of evaluation: (a) evaluation of capital, (b) evaluation of values, and (c) evaluation of narratives. The term evaluation may lend itself to a cognitivefocused interpretation; however, we reject the strict dichotomy of cognitive and affective reactions and use the term evaluation to encompass both, recognizing that pregnant people’s emotions and thoughts about their options are intertwined. People’s consideration of each of these factors may also range on a spectrum from implicit to explicit. Additionally, the order of presentation of each of these three factors does not represent a relative significance; the importance of each factor will vary across pregnant people, and many will face ambivalence due to contrasting thoughts, feelings, or beliefs within and between factors (Allanson, 2007).
Evaluation of Capital
The first area of consideration in the PDMM is the evaluation of capital, which can be broken down into three subareas: social capital, financial capital, and health capital. During the evaluation of capital, a pregnant person explores what resources they may have available to them in the case of a variety of outcomes.
Evaluation of social capital
For the purposes of this model, social capital is defined as the social resources that a pregnant person perceives as being available to them. Thus, a pregnant person evaluates their social support systems and determines the extent to which these systems will meet their needs. One variable included in this factor is partner presence. Studies have shown that the presence of a significant other is a main indicator of pregnancy outcome, such that pregnant people in relationships are less likely to access abortion (Allanson, 2007; Chiweshe et al., 2017; Sihvo et al., 2003). More precisely, many participants in these studies have specified that the presence of a stable partner is a key factor in their decision (Chiweshe et al., 2017; Santelli et al., 2006), suggesting that the presence of a partner should be measured continuously (e.g., relationship quality) rather than dichotomously. The presence of violence in an intimate relationship is likely to be a significant factor during this stage, as some pregnant people may view pregnancy as a stimulus to leave their relationship, while others may find their pregnancy options restricted by an abusive partner (Côté & Lapierre, 2014; Williams & Brackley, 2009). Other considerations might include the social support of parents (viz., for people who become pregnant in adolescence; Pereira et al., 2019), relatives, friends, and communities, especially for families of color, in which extended families are likely to play a stronger role in children’s lives (Wilson, 1989). Evaluating social support networks may be even more complex for people whose pregnancy was a result of rape or incest and especially so for those whose perpetrators were family members or partners. Given the frequency with which sexual trauma is accompanied by secrecy and shame, pregnant survivors may face additional difficulties in identifying social support during pregnancy (Littleton, 2010). We theorize that identifying social support networks helps pregnant people clarify what it would be like to choose various pregnancy options. If it takes a village to raise a child, pregnant people may be prompted to evaluate their village.
Evaluation of financial capital
In addition to considering social resources, a pregnant person is likely to examine the availability of financial resources. A pregnant person may calculate (or estimate) how much financial capital they have to contribute to the possibility of raising a child or accessing abortion. They may consider their income level and stability, cost of living, and the amount of financial assistance they expect to receive. The cost of abortion and costs of raising a child vary widely across nations, with the cost of raising a child (from birth to 17 years) nearing $250,000 in the United States (Lino et al., 2017; UNICEF, 2004). Some pregnant people may see a child as a financial benefit, particularly in agricultural communities where children may contribute labor or in areas where a child may earn them a dowry that could improve their family’s wealth (Chowdhury, 2010). Participants in pregnancy decision-making studies frequently cite financial implications as one of the primary factors they considered (Appiah-Agyekum et al., 2015). Data from the Guttmacher Institute suggest that 75% of pregnant people who terminate a pregnancy in the United States are under 200% of the federal poverty level (Jerman et al., 2016), although this may be partially explained by higher rates of unintended pregnancy in low-income populations. The evaluation of financial capital is a complex issue that often depends on pregnant people’s perceptions and cultural considerations of the costs of accessing reproductive care and raising a child.
Evaluation of health capital
When considering the feasibility of various pregnancy options, pregnant people may also contemplate how their health status may affect their ability to choose a specific pregnancy outcome. In this paper, health capital references the personal health resources that a person stands to gain or lose in the face of an unintended pregnancy (Galama & van Kippersluis, 2014; Grossman, 1972). A pregnant person may evaluate their health capital due to a pre-existing health condition (e.g., epilepsy, addiction), a condition that arises during pregnancy (e.g., gestational diabetes), or in the absence of any such condition. Studies following women with health concerns have reported that many worry about how a pregnancy may be dangerous to their health (Lee et al., 2013) or about their ability to raise a child (Dolman et al., 2013). These concerns may be heightened for people who are living at the intersections of disability and poverty, whose health status may be doubly threatened by a lack of financial capital. Similarly, people with mental health concerns may evaluate whether their mental health could be affected by pregnancy, parenthood, or abortion (McCauley & Casson, 2013). In the case of pregnancy as a result of rape or incest, the effects of trauma may threaten a pregnant person’s existing health capital, making pregnancy decisions significantly more painful. For those who have no known health conditions, an evaluation of health capital might involve a consideration of the person’s energy levels or their ability to stay healthy throughout the pregnancy option they choose. In any of these circumstances, for people with diagnosed conditions and those without, processes such as fear or fatigue may be components of the evaluation, above and beyond any cognitive calculations of health capital. For example, people may be motivated by fear of their health condition worsening, despite their belief about the probability of such an outcome.
Through an evaluation of social capital, financial capital, and health capital, a pregnant person may discover both strengths and doubts about the feasibility of varied pregnancy options. This consideration must then be reconciled with the person’s evaluation of values.
Evaluation of Values
Another primary area in the PDMM is the evaluation of values, which covers a pregnant person’s moral or ethical attitudes toward their pregnancy options. While attitudes about abortion may be most publicly controversial, pregnant people are likely to hold value judgments about adoption, parenting, and childbearing as well (Mollen, 2014). For each of these areas, a pregnant person’s attitudes are likely more multifaceted than for or against; rather, the evaluation concerns their beliefs about the specific circumstances of their pregnancy.
Abortion values
A person facing unintended pregnancy is likely to consider their beliefs about the ethics of abortion. But the complexity of abortion attitudes goes beyond prochoice and pro-life. Research on abortion attitudes indicates that people may have highly complex views on abortion in a variety of circumstances and may be ambivalent about the issue of abortion (Edlund & Edlund, 2014). For example, factors that may affect a person’s belief in the permissibility of abortion include fetal age/development, risk to the pregnant person, whether the pregnant person’s partner or family agrees with the termination, and pregnancy from rape or incest (Hans & Kimberly, 2014; Jozkowski et al., 2018). Conservative and traditional Christian religious beliefs, strong beliefs about gender role traditionality, and benevolent sexism have all been found to be highly related to negative abortion attitudes (Huang et al., 2016; Mosley et al., 2017). The intersections of a person’s identities may also create complex values surrounding abortion; for instance, a person who belongs to a conservative religious group and also identifies as feminist may experience conflict stemming from their ideological backgrounds. Broader pronatalist cultural values may contribute to an ethical stance against abortion (Mollen, 2014).
Values related to abortion may be strongly tied to knowledge about abortion, as studies have shown that individuals with more accurate abortion information feel more favorably about abortion (Mollen et al., 2018). Thus, misinformation about abortion (e.g., the false idea that abortion is dangerous or causes health problems; Rowlands, 2011) may cause a person to feel fear or opposition to abortion (White et al., 2016). Thus, there may be a link between abortion values and Informational Access (as described later in this paper). Furthermore, people’s values may be expressed emotionally; for example, a person may have pro-choice beliefs but feel a sense of shame about terminating a pregnancy. Pregnant people are likely to consider their attitudes toward the possibility of abortion in their specific circumstance and context.
Adoption values
A pregnant person may also evaluate their attitudes toward adoption. In general, data suggest that pregnant people are less likely to consider adoption (compared to abortion or parenting; Sisson et al., 2017; Smith et al., 2016); some may have strong feelings about the permissibility of adoption. For example, a pregnant person may believe that adoption is a noble decision, especially if such attitudes have been modeled by their religious community (Moore, 2010). Others may believe that adoption is unethical or may have a negative emotional reaction to adoption, perhaps because of concerns about transcultural/transracial adoption or due to the perception that placing a child for adoption reflects a lack of maternal care (Moos & Mwaba, 2007). Although literature on adoption attitudes is limited, one recent study recognized value judgments against women who place children for adoption (Rice et al., 2017). More research is needed to understand people’s beliefs about the ethics of adoption.
Childbearing and parenting values
Pronatalist values toward childbearing and parenting may exist in a variety of contexts (Mollen, 2014). For example, if people believe that children are a religious or divine blessing, perceive pregnancy as an opportunity to carry on their family name, feel called to procreate as a part of their religious tradition, or conceptualize additional children as a contribution to their family, childbearing may be viewed as a moral imperative and reactions to parenting may be joyful. Perhaps less commonly, some pregnant people view a decision to parent as unethical. This may relate to sociopolitical problems, referencing the lack of “safe and sustainable communities” in which to parent (as defined by SisterSong Women of Color Reproductive Justice Collective, 2018). For example, pregnant people may question: What does it mean to have a child while my country is at war? Is it okay to bring a child into the world in the face of climate change? Can I raise a child in my neighborhood when children of color are being killed by police? If there is no safe drinking water in my city, can I raise a child here?
A more thoroughly researched aspect of the ethics of childbearing involves people’s moral concerns about the risk of passing along a genetically-transmitted disorder to their children (Chan et al., 2017). Others may see single parenting as unethical or have misperceptions about negative consequences for children raised by single parents (Kleist, 1999; Zartler, 2014). Diverse cultural orientations toward the acceptability of single-parenting based on intersections of race and class may influence these values. Thus, pregnant people may have value judgments about childbearing and parenting based on the circumstances of their life and cultural context.
Evaluation of Narratives
The next component of the PDMM is the evaluation of narratives, a bipartite evaluation involving pregnant people’s consideration of how their pregnancy fits into their life vision and cultural ideas of pregnancy. This factor includes an evaluation of life trajectory narratives and an evaluation of intersectional cultural narratives. Narratives are meaning-making tools through which people interpret their lives through the lens of a cohesive story and may be used to construct an identity (McAdams, 2011). Specifically, narratives have been studied to explain people’s cultural understandings of parenthood, pregnancy, and abortion (McIntyre et al., 2001; Oduro & Otsin, 2014). Narratives allow a more in-depth psychological and cultural view of unintended pregnancy.
Evaluation of life trajectory narratives
The first part of the bipartite evaluation of narratives factor is the evaluation of life trajectory narratives, in which the pregnant person must reconcile the unintended pregnancy with their life vision. At this point, a pregnant person considers how each of their pregnancy options might correspond or conflict with their self-concept, life plan, and ideal family (Cabeza de Baca & Ellis, 2017). One aspect in which pregnant people might need to reconcile their life trajectory and their unintended pregnancy is in the area of educational or career ambitions. Research has consistently demonstrated that, especially for young pregnant people, educational aspirations and goals have a significant influence on pregnancy decision-making, with less goal-orientation related to higher likelihood of parenting (Appiah-Agyekum et al., 2015; Sihvo et al., 2003). Similarly, people who are employed and especially those whose current or ideal careers are seemingly incompatible with parenting may be more likely to choose abortion (Pereira et al., 2019; Reuter, 2018; Sihvo et al., 2003). Thus, pregnant people who perceive continuing their pregnancy as being in conflict with their career or educational goals and lifestyles may be more likely to consider abortion.
Another factor involves the desire to become a parent or to remain childfree. Pregnant people may consider whether they want to become parents at all. Many may imagine their ideal family, which might include family size, partnership status, parental age at first/last birth, spacing between pregnancies, or sex/gender of children. Indeed, one of the primary factors noted in abortion literature is the idea of family size: people often choose to parent when they have not yet reached their desired number of children and choose abortion if they feel their family has reached capacity (Oduro & Otsin, 2014; Sihvo et al., 2003). Data indicate that women who feel “resigned” to becoming mothers early in life, perhaps due to living in areas where early parenthood is common, may be more likely to choose to parent (Bryant et al., 2010). A pregnant person may also assess if the other person who biologically contributed to the pregnancy is someone with whom they can envision raising a child. This may be particularly painful in the case of a pregnant person whose pregnancy is the result of rape or incest. Some pregnant people, particularly those who are older and those whose medical diagnoses (e.g., Polycystic Ovary Syndrome) or medications (e.g., testosterone) may limit their fertility, may be concerned with their future fertility and may perceive the current pregnancy as their only chance at parenthood. Misinformation about decreased fertility after abortion may cause even young pregnant people to worry about their ability to have children in the future. These concerns could lead a pregnant person to consider parenting even if the current pregnancy does not align with their ideal life trajectory. The possibility of abortion may also create an incompatibility with a pregnant person’s life trajectory. Those who never considered the possibility of having an unintended pregnancy or never imagined having to access abortion care themselves may view having an abortion as incompatible with their life narrative (Mann et al., 2015). Alternatively, pregnant people who have terminated prior pregnancies may have envisioned themselves avoiding subsequent unintended pregnancies and may be reticent to choose abortion.
Pregnant people’s reconciliation between their life trajectories and their unintended pregnancy may incorporate myriad life factors. It is important to remember that life trajectories are themselves culturally influenced, and intersections of gender, race, religion, and class affect what is seen as the ideal life narrative or ideal family (Van Hollen, 2007; Woollett et al., 1991). In the next step of the evaluation of narratives component, pregnant people explore cultural representations of pregnancy, parenting, abortion, and adoption more directly.
Evaluation of intersectional cultural narratives
The second part of the bipartite evaluation of narratives factor is the evaluation of intersectional cultural narratives, in which the pregnant person contrasts their pregnancy situation with dominant cultural narratives and scripts. Whereas some of the aforementioned evaluation factors likely involved explicit considerations, the evaluation of intersectional cultural narratives may be more likely to take place implicitly. This factor is one of the more definitive examples of how forces of oppression are theorized to influence a person’s pregnancy decision. During this stage, any aspects of the pregnant person’s identities that contribute to their marginalization or do not fit the dominant narrative become opportunities for insidious removal of agency. A person’s age, race, ethnicity, nationality, ability/disability, gender identity, sexual orientation, religion, education, marital status, or other identity factors may differentiate them from the “ideal” pregnant person (Stevens, 2015). For example, in the United States, the cultural narrative of an ideal pregnancy may be a planned pregnancy embodied by a White, heterosexual, cisgender woman in her late 20s who is married, well-educated, able-bodied, and upper/upper-middle class. Pregnant people whose experiences do not align with this cultural script may face difficulties in choosing or accessing various pregnancy options (Maternowska et al., 2010). We recommend that researchers analyze identity factors as complex phenomena (as described below) rather than simply reporting differential rates of pregnancy outcomes based on demographic categories. Below are a few examples of ways in which inequity might create harm and/or limit agency during pregnancy decision-making.
Discrimination
Pregnant people, especially those who are multiply marginalized, may be affected by discrimination. According to stigma mechanisms theory, discrimination may have a multifaceted effect on (pregnant) people: experiences of discrimination can be harmful, as can anticipated discrimination, or the fear that one person will be subjected to discrimination in the future (Chaudoir et al., 2013). For example, an undocumented person might want to parent but could be threatened by the potential of losing a job through pregnancy-related discrimination in the workplace and have little in the way of legal recourse (Jones, 2017). A pregnant transgender man or non-binary person could be seriously endangered by discrimination in healthcare settings like abortion clinics or hospitals/birth centers (Rodriguez et al., 2018; Shires & Jaffee, 2015). Given the vast physical, financial, and emotional consequences of discrimination, including those which demonstrate potential harm to the fetus and the parent (Bennett et al., 2010; Earnshaw et al., 2013; Stepanikova & Kukla, 2017), fears of discrimination and experiences of discrimination present a severe threat to pregnant people.
Internalized stigma
Pregnant people whose identities are marginalized in their societies may have internalized judgments about themselves and others who share their identities. For example, people who have physical disabilities (e.g., a mobility impairment), health conditions (e.g., HIV), or mental health disorders (e.g., bipolar disorder) may internalize negative messages about their disability or disorder, which could negatively influence decision-making (LaPierre et al., 2017; Orner et al., 2011). Other identities may be connected to stigma about pregnancy or parenting; for example, some pregnant people may hold internalized stigma about being unpartnered or living in poverty during their pregnancy (Rice et al., 2017). This sense of stigma could decrease parenting self-efficacy and increase the likelihood that a pregnant person chooses adoption or abortion. Internalized stigma might cause misperceptions or devaluations of one’s ability to cope with pregnancy or parenting.
Stereotype threat
Pregnant people whose identities are connected to stereotypes about parenting, abortion, or adoption may face stereotype threat or a sense of self-consciousness about the risk of confirming stereotypes about one’s group (Steele & Aronson, 1995). Given the variety of stereotypes about pregnancy, parenting, and abortion, it seems extremely likely that this phenomenon might affect pregnant people. For example, Black/African American and Latinx pregnant people in the United States could encounter stereotype threat if they perceive a risk in fulfilling the stereotype of becoming a person of color with “too many” children. This stereotype may be especially relevant for low-income or unpartnered Black/African American or Latinx people, who face additional stereotypes about being single parents of color or accessing public assistance programs (Rojecki, 2007). Pregnancy-related stereotype threat may also be present for both young and older pregnant people. Young people (especially those from low-income areas) who become pregnant may fear becoming “another statistic” if they become teenage parents (Greene, 2006). Older adults may be concerned about fulfilling stereotypes about advanced maternal age; in fact, the only published paper connecting stereotype threat to pregnancy decisions covers stereotype threat in the context of advanced maternal age (Abdou, 2017). In the United States, bias related to who accesses abortion may also enact stereotype threat for pregnant people who are Black/African American, young, unpartnered, uneducated, and/or living in poverty.
It is obvious that the politics of pregnancy, parenting, adoption, and abortion highlight social complexities and inequities. Thus, pregnant people’s social locations and experiences of their intersecting identities are essential to understanding pregnancy decision-making. The three areas of evaluation highlight areas that pregnant people may consider when facing unintended pregnancy. Next, we present two moderating factors: Barriers to Access and Social Influences.
Barriers to Access
The most important component of the PDMM is Barriers to Access, the limitations to a pregnant person’s ability to freely and autonomously access pregnancy options. Access not only varies based on geographic location and social identity, but also based on structural inequities. People at the margins, and notably those who are multiply marginalized, may face additional restrictions in access. Access is the principal component of the PDMM, one that we theorize to have a disproportionate influence on a person’s pregnancy outcome, decisional certainty, and decisional satisfaction. Barriers to accessing reproductive options are a crucial factor in pregnancy decision-making, as they stand to constrain people’s pregnancy decisions regardless of what they might choose in an ideal world. Access means access not only to abortion care but also to other resources (e.g., financial, informational) that might limit one’s ability to parent (SisterSong Women of Color Reproductive Justice Collective, 2018) or constrain their agency or freedom in decision-making. A lack of access may foreclose a person’s consideration of any of the other evaluation factors in the model; for example, if a person cannot access prenatal care, they may not consider parenthood at all. Thus, we propose that barriers to access are the most powerful variable in the PDMM.
Four facets of access ought to be considered here. First is legal access—does the person have the legal right to access their intended pregnancy decision? In many countries, abortion is illegal or severely restricted based on the circumstances of the pregnancy (de Costa et al., 2015; Finer & Fine, 2013). Even in places where abortion is generally legal, pregnant people may face legal challenges in accessing abortion due to being underage (Ralph et al., 2017) or at an advanced gestational period (Harries et al., 2015). Legal circumstances surrounding abortion are frequently changing, which may obscure a pregnant person’s understanding of their ability to access legal abortion (Keefe-Oates et al., 2019). For example, frequent attacks on reproductive rights such as targeted regulation of abortion provider laws (Mercier et al., 2016) and personhood laws in the United States threaten to undermine legal access to abortion and create confusion about how to access abortion (Brumback, 2019). Individuals whose pregnancy is the result of rape or incest may have increased legal access to abortion, but this legal access may come with additional hurdles, such as the requirement to report their perpetrator, which decrease the pregnant person’s autonomy (Perry et al., 2015). Although pregnant people may still access abortion when it is illegal, legal access is a determining factor for many.
Another essential factor is informational access—access to accurate and culturally-relevant information related to reproductive issues and pregnancy options. Across the world, many people are denied access to comprehensive and accurate sex education and thus may be misinformed about their bodies, pregnancy, or reproductive options (Santelli et al., 2006). Misinformation about abortion may be particularly common, as researchers have found pervasive and pernicious myths about supposed dangers of accessing abortion (Bloomer et al., 2017; Rowlands, 2011). Falsehoods about abortion may be perpetuated by systemic policy (Berglas et al., 2017) or by individuals (e.g., at Crisis Pregnancy Centers; Kimport, 2019) and are prominent on the internet (Bryant et al., 2014). Myths about abortion have also been found to be related to anti-abortion attitudes (Kavanaugh et al., 2013). Similarly, myths or misinformation about childbirth, parenting, and adoption (Perry & Henry, 2010; Pugh, 2014) may also create barriers to freely making autonomous decisions. When pregnant people have been denied access to accurate information (either before or during pregnancy) they do not have the ability to make truly fully informed decisions.
Next is financial access—does the person have the financial means to access their preferred pregnancy decision? And specifically, does the person have the financial means to access a safe and healthy environment for the decision of their choice? When it comes to abortion, this question primarily revolves around the cost of the abortion procedure, which is often not covered by medical insurance (Jones & Jerman, 2017). It could also relate to the financial cost of accessing abortion in a safe environment by an educated or licensed healthcare provider, which may not be financially accessible in various geographic locations. Other related costs, such as lost wages (from time off from work) and transportation and lodging costs (for the many people who do not live in close proximity to an abortion provider), may raise the price of abortion considerably. In some countries, private abortion funds or government-funded abortion care may be more readily available (Adamczyk, 2008). The costs of prenatal care, childbirth, and childcare represent some of the financial burden of childbearing, which may be wholly out of reach for many. Childbirth costs vary widely: in countries such as Argentina or South Africa, the average cost of delivery is around $1000; in other places, such as the United States, costs have risen to over $10,000 for a typical delivery (The Economist, 2018). Other costs associated with delivery, such as hospital stays, may nearly triple the cost of childbirth (The Economist, 2018). Childcare can also be quite expensive, with 2018 data indicating that couples making typical wages in their country pay an average of 13% of their net household income on childcare (Organization for Economic Cooperation and Development, 2019). In some countries, such as Switzerland and Australia, costs approach 35%–42% of household income (Organization for Economic Cooperation and Development, 2019). These costs can make childbearing and childrearing inaccessible for those in poverty, those without adequate health insurance, and those whose geographic locations or mobility restrictions make affordably accessing healthcare extremely difficult.
Last is logistical access—can the pregnant person physically access the pregnancy decision they chose? This may relate to one’s geographic location and physical proximity to hospitals or abortion providers (Moseson et al., 2019). It may also concern one’s ability to travel to access said services, which could be impeded by terrain, lack of transportation, border-crossing restrictions, or inability to secure childcare for existing children or to take leave from work. For example, some U.S. states such as Mississippi and Missouri only have one abortion clinic, while in other states, such as West Virginia, 90%–95% of people do not live in a county with an abortion provider (Jones & Jerman, 2017). For people who use public transportation (e.g., due to income and/or disability), this may present an even more significant barrier. Those in federal, provincial, or state facilities, such as psychiatric hospitals, prisons, or detainment centers, may have little or no access to care (Holter, 2017; Sufrin et al., 2015).
In keeping with the frame of reproductive justice, access is the most important variable in determining pregnancy outcomes. Reduced access may have an effect on the way a person evaluates or considers capital, values, and narratives. Even if a pregnant person is completely certain about their pregnancy decision, they may be unable to access it or the difficulty in accessing it may pose a barrier so great that choice is co-opted for them. Thus, Barriers to Access are an essential component of the PDMM.
Social Influences
Social influences are another key component of the PDMM. We define social influences as the social interactions that influence a person’s pregnancy decision-making process. We argue that pregnancy decision-making is a relational process, often taking place in the context of relationships with family, friends, or cultural communities (Osur et al., 2015). We propose that the power of social influence is so strong that it affects every other component of the PDMM and moderates the effects of predictors on proposed outcomes. We conceptualize social influences as taking two primary forms in the model. First is social support, which can be further broken down into emotional and instrumental support (Sherbourne & Stewart, 1991). Emotional support refers to empathy and understanding, while instrumental support may be understood as informational and tangible aid. The second form of social influence is social attitudes, which refers to the norms, values, and appraisals that are communicated from groups and individuals to the pregnant person. Both forms of social influence (social support and attitudes) can be positive or negative; that is, social support may be offered or withdrawn, and attitudes may reflect approval or disapproval of pregnancy options.
Research demonstrates that a majority of people making pregnancy decisions consult or are influenced by someone close to them, including partners, parents, or friends, and that many pregnant people view these perspectives as very important to their decision-making process (Agbemenu et al., 2018; Osur et al., 2015). Social influences are not limited to close family and friends; they also include religious leaders, healthcare providers, public figures, and strangers on the internet (Lagan et al., 2010). And social and relational processes themselves are affected by power dynamics and cultural forces (Guerra-Reyes & Iguiñiz-Romero, 2019; Omeje et al., 2011). For example, pregnant people living with a disability or those who are living in poverty may be more likely to receive condescending and forceful pressure from social influences. A particularly nefarious form of social influence includes reproductive coercion, in which a person (often a partner) attempts to coerce the pregnant person into a specific pregnancy outcome. Reproductive coercion is particularly common in the context of interpersonal violence and pregnancy resulting from rape or incest (Basile et al., 2018). Below, we offer examples of how social influences might augment each component of the PDMM.
During the evaluation of capital, offers or withdrawals of financial and social capital from friends, family, or community members might cause a person to reconsider their decision. For example, one might imagine a pregnant person entering a crisis pregnancy center (an organization that purports to provide pregnancy support and counsels against abortion) and receiving promises of diapers and low-cost childcare. In terms of health capital, a pregnant person could be influenced by a physician who strongly advises termination of their pregnancy based on their medical condition (McCauley & Casson, 2013). Information received from relevant others during the evaluation of capital may be a key facet in pregnant people assessing their resources. When pregnancy decisions are made based on misleading social influences on capital, pregnant people may feel less satisfied with their decision. For example, a person who chooses abortion after being promised emotional support by a partner may feel less satisfied with their decision if that support does not come to fruition.
During the evaluation of values, pregnant people are likely to be impressed upon by many social influences. Pregnant people may hear from family or friends about the ethics of abortion or read online forums where people argue it is immoral to raise a child in a single-parent or same-sex household (Zartler, 2014). They may visit a crisis pregnancy center and be persuaded that abortion is dangerous (Kimport, 2019) or receive accurate information about abortion from a health clinic. Social norms theory (Berkowitz, 2004) posits that people’s attitudes are, in part, based on what they believe to be the attitudes of the majority of relevant others. Thus, through a process of social persuasion or social norms, pregnant people’s ethical attitudes towards their pregnancy options may be mitigated or intensified by input from others (Adamczyk, 2008). If this sense of pressure is particularly vitriolic or coercive, it may cause pregnant people to have lower decisional satisfaction due to a lack of autonomous choice.
During the evaluation of narratives, a number of social influences may affect the ways in which people formulate their trajectory narratives, integrate the unintended pregnancy with those narratives, and evaluate cultural narratives. People’s life trajectory narratives, including their career ambitions, ideal family situations, and partnership expectations, are all influenced by cultural and peer norms. For each of the mechanisms of oppression (discrimination, internalized stigma, and stereotype threat), exposure to harmful messages about one’s marginalized identity may amplify these effects. Social influences may provide a protective eff if pregnant people are surrounded by similar others (MacQuarrie & Edmeades, 2015), and receive counter-messages about the perceived stereotypes connected with their identities. Thus, pregnant people might experience greater decisional certainty and satisfaction when they are influenced by affirming messages from friends or media. Through these and numerous other examples, social influences and relationships in multiple spheres of life may affect pregnant people’s pregnancy outcomes and decision-making.
Outcomes of the PDMM
We hypothesize that the preceding factors of the PDMM can be used to predict three categories of outcomes: pregnancy outcome, decisional certainty, and decisional satisfaction.
Pregnancy Outcome
First, we posit that the PDMM can be used to predict a person’s pregnancy outcome, that is, whether their unintended pregnancy ends in abortion, adoption, or parenting. Each person’s unique combination of evaluation factors, barriers to access, and social influences may be causally linked to their likelihood of accessing different reproductive healthcare services. For example, a person whose anti-abortion (pro-life) values are central to their beliefs may be unlikely to choose abortion, even in the context of other social factors that may indicate a lower likelihood of choosing to parent. Another pregnant person who faces parenting stigma due to race and class as well as barriers to accessing prenatal care due to their disability may be more likely to choose to terminate their pregnancy. The aforementioned factors may affect not only outcome, but also the pregnant person’s experience of their decision.
Decisional Certainty
We hypothesize that pregnant people’s experience of their pregnancy decision-making process, including decisional certainty and decisional satisfaction, will be affected by PDMM factors. While studies suggest that people’s feelings toward their choice of pregnancy outcome may be quite stable (Brown, 2013), there may also be a subset of people who do not experience such certainty. Decisional certainty may be related to the balance of evaluation components in the PDMM (Ralph et al., 2017), such that conflict between evaluation factors may be related to ambivalence and negative emotional experiences (Allanson, 2007). For example, if evaluation of capital leads someone strongly toward abortion but evaluation of values and narratives lead them strongly toward parenting, they may experience enhanced inner conflict and lower decisional certainty.
Decisional Satisfaction
Decisional satisfaction may also be influenced by the components of the PDMM. Research indicates that pregnant people who feel pressured by significant others to choose abortion may be less satisfied with their decision (Pereira et al., 2017; Ralph et al., 2014). Similarly, we propose that people whose decisions are more heavily influenced by factors related to injustice, such as a lack of access to their pregnancy option of choice, or experiencing discrimination or internalized stigma may be less likely to be satisfied with their pregnancy outcome and decision-making process. Furthermore, we anticipate that people’s psychological post-pregnancy experiences will be shaped by the PDMM factors. For example, we propose that negative social influences (e.g., judgment from family) or evaluations of capital that do not match a person’s reality after making their decision may lead to negative emotional experiences, such as regret or guilt after abortion or difficult adjustment to parenthood in the post-partum period (Koletzko et al., 2015). The PDMM may also be useful in predicting positive psychological experiences in the post-pregnancy period, such as satisfaction, psychological well-being, and positive self-concept. Such positive outcomes may be related to people’s lack of barriers in access, positive social influences, and lack of conflict between values and decision. In a decision-making instance where a sense of autonomy and agency is especially important (Ekstrand et al., 2009), the balance of PDMM factors may be integral in understanding how to bolster and support pregnant people’s sense of decisional certainty and satisfaction.
Summary
We present the PDMM as a potential genesis for a new era of research into the psychological factors in reproductive decision-making in the context of unintended pregnancy. Building upon decades of research on reproductive outcomes and integrating frameworks of reproductive justice and intersectionality (Crenshaw, 1989; SisterSong Women of Color Reproductive Justice Collective, 2018), we propose the PDMM to contribute a contemporary conceptualization of the realities that pregnant people across the world experience when facing a pregnancy decision. These realities are necessarily shaped by culture and forces of inequity that create disparate circumstances based on pregnant people’s identities and social locations. Combining theoretical frameworks with recent research on pregnancy decisions and outcomes (Guerra-Reyes & Iguiñiz-Romero, 2019; Jozkowski et al., 2018) gives this model evidentiary support, with the hopes that future research will further bolster the scientifi rigor of the PDMM.
The foundation of the PDMM are the three evaluation components: evaluation of capital, which includes an evaluation of social, financial, and health resources that are available to pregnant people in their potential pregnancy outcomes; evaluation of values, which involves an assessment of a pregnant person’s moral views and attitudes about their pregnancy options; and evaluation of narratives, a bipartite element comprised of evaluation of life trajectory narratives and intersectional cultural narratives. Each of these components is affected by social influences, as pregnant people make their pregnancy decisions in the contexts of their relationships. Finally, we theorize that barriers to legal, informational, financial, and logistical access have the largest effect on outcomes. We suggest that these factors predict pregnancy outcome, decisional certainty, and decisional satisfaction. In the PDMM, we integrate relational, psychological, and cultural factors more comprehensively than any other pregnancy decision-making model.
Limitations
Although the PDMM represents a significant improvement in the integration of theory into research on pregnancy decision-making, we acknowledge multiple limitations of the model in its current state. First, and most obviously, is the lack of empirical evidence for the model; despite being crafted based on extant evidence, the model has not yet been tested for its predictive power or fit with pregnant people’s conceptualizations of their experiences. Future research is certainly needed. Next, we acknowledge the lack of parsimony in the PDMM, as this model integrates a variety of predictors and outcomes. Whereas many other models of health behavior prioritize parsimony, this model aimed to be more comprehensive to provide nuance and to be generalizable while still incorporating various cultural perspectives. The broad nature of the PDMM means that a clear calculation of the likelihood of a person’s pregnancy decision is not easily ascertained from the model. Because every person’s personal, relational, and cultural context is different, the predictors in the PDMM may be weighted differently for different individuals. For example, while we suggest that barriers to access might be the single most important factor in any person’s pregnancy decision-making process, pregnant people may conceptualize their decisions as being made predominantly based on other factors. Thus, there is no inherent weight structure in the model, as we intend the PDMM to be flexibly interpreted based on variable circumstances. Additionally, we recognize that there are many important intersections of unintended pregnancy that deserve more attention than we have given here. For example, although we referenced pregnancy as a result of rape and incest, the intersection of trauma and pregnancy deserves more thorough examination in future work. In the future we also hope to see intersectional work examining unintended pregnancy for those who are incarcerated, undocumented, experiencing homelessness, and seeking asylum/refugee status. Lastly, we acknowledge that despite attempts to integrate international data and perspectives, this manuscript represents a U.S.-based point of view, which may not encapsulate cultural differences from other areas of the world. We hope that international scholars will utilize and adapt the PDMM to better fit the sociocultural realities of many different regions.
Future Directions
The PDMM lends itself to myriad empirical studies based on its components. Below, we list a variety of future research directions arising from the PDMM. What are people’s perceptions of the costs of childrearing, and what cultural beliefs influence these perceptions? How do pregnant people with a variety of health concerns conceptualize their health being affected across the context of pregnancy, birth, or parenting? How do pregnant people cope with the disequilibrium that occurs in the context of unintended pregnancy when it does not match their life trajectory narrative? What cultural factors influence people’s life trajectory narratives in relation to their integration of work and family (e.g., family size, timing of pregnancy)? How does the experience of discrimination during pregnancy affect a pregnant person’s mental and physical health, and how does it predict pregnancy outcome? What are the common stereotypes surrounding abortion, parenting, and adoption for different cultural groups (e.g., Black women, people with disabilities, adolescents), and how do people experience stereotype threat during unintended pregnancy? How might mental health or disability stigma influence people’s pregnancy decision-making? What factors influence people’s perceptions of access to resources and reproductive options, and how can we improve access to reproductive care? Which of the evaluation factors are most strongly related to a person’s pregnancy outcome, and how does the strength of these relationships vary across cultural groups? How do narrative factors relate to experiences of grief or relief after abortion? These and a host of other questions might be addressed in future research using the PDMM.
Practical Implications
One of our primary reasons for crafting the PDMM, in addition to the hopes of spurring new research on the psychology of pregnancy decision-making in cultural context, was that the PDMM might be used to improve social services available to people facing unintended pregnancy. Because of the vitriolic public conversations surrounding reproductive issues, pregnant people often fear judgment from healthcare providers regarding their pregnancy options (Abdou, 2017). In order to combat their own assumptions, healthcare providers in fields such as medicine, nursing, psychology, social work, and counseling can use the PDMM to improve their awareness of the decisional complexities that clients might face when experiencing an unintended pregnancy. In fact, health service training programs might utilize the PDMM as a teaching tool to expand students’ worldviews regarding unintended pregnancy.
While the PDMM is not a decisional aid, it may still be helpful to providers who are working with pregnant people in the process of pregnancy decision-making. Clinicians can utilize the PDMM as a guide for a non-judgmental and open discussion of factors that are relevant for the client. Having the PDMM as a framework for the discussion might help clinicians empower their clients to gain clarity in a potentially stressful situation (Ely et al., 2018). Additionally, clinicians who are working with clients in the post-partum period or with clients who have accessed abortion might use the PDMM to explore and validate the complexity of their clients’ pregnancy decision-making experiences and to help clients build self-compassion around their decision and the factors that led them to it.
On a macro-level, we hope that the PDMM can be utilized to identify specific cultural and sociopolitical barriers and limitations to reproductive access, so that we may be better equipped to pursue global equity initiatives toward reproductive justice (Association of Women’s Health, Obstetric, and Neonatal Nursing, 2009; Moseson et al., 2019). Specifically, we hope that this intersectional approach spurs greater understanding of the factors affecting pregnant people who are marginalized so that we may break away from a cisheteronormative and colonialist viewpoint of unintended pregnancy and be better prepared to dismantle the structures that restrict the autonomy and agency of all pregnant people. This could involve efforts such as public campaigns to improve abortion knowledge, innovative community support structures for single parents, or increased training for medical providers regarding transgender and gender non-conforming pregnant people. Our aim is that the PDMM illuminates unintended pregnancy and pregnancy decision-making such that it is no longer fraught with secrecy or shame. We hope that this work will be a step toward a world in which every person has the ability to freely choose and access the pregnancy option that is right for them.