
Abstract
A population problem represented by the declining birth rate came to the focus of experts’ and politicians’ attention in interwar Czechoslovakia. Significant activities concerning the decrease in quantity and alleged population quality were pursued within the broad spectrum of experts who questioned the nation's future. Drawing from the concept of biopolitics, this article demonstrates through the analysis of medical discourse how medical professionals and social workers together with counseling bureaux, foregrounded the idea of a healthy family, primarily inspired by a (pseudo)science of eugenics, in order to maintain appropriate quantitative and qualitative population development. This article aims to expand the body of knowledge on experts’ attitudes toward demographic trends in interwar Czechoslovakia and to draw attention to two types of counseling bureaux and their role in reproductive policy. While the idea of eugenic premarital bureaux was explicitly linked to the eugenic movement that aimed at discouraging the reproduction of people identified as inferior, the role of counseling bureaux for mothers and children regarding family planning and reproduction remains overshadowed by their mission of medico-social care for children.
Keywords
“It is impossible not to mention the basic fact that child healthcare begins before the child is conceived. ‘You are young and want to have children and get married. But I ask you: Are you a person who can allow yourself to want to have a child?’ says Nietzsche to a young man. A eugenic bureau should say the same to every young man and woman. These counseling bureaux experience a very unfavorable time in our country, so their number is hardly enough to carry the banner of the whole movement, and so for many conscientious men the question of marriage and offspring remains unanswered. It is the task of other counseling bureaux and other doctors to give an answer to the interviewers, at least in outline, as long as eugenic bureaux, which require great expertise and thoroughness, are up to the task themselves.” 1
These words were written in 1934 by the Czech doctor and expert advisor to the Ministry of Healthcare and Physical Education, Dr. Josef Veselý, in his article on counseling bureaux for mothers and children issued in the publication of the Social Institute of the Czechoslovak Republic. As the quote informs, under the guise of protecting the health of future generations, the process of family planning and reproduction, an intensely intimate matter, was not treated as a private concern. On the contrary, it was subjected to surveillance and scrutiny by various experts, who wanted to determine to a substantial extent the patterns of reproductive behavior. Indeed, from the nineteenth century onwards, the practices of human reproduction became an object of state interventions that sought to define how people could and should reproduce.
This article attempts to address the emergence of two different types of counseling bureaux. Both emerged in interwar Czechoslovakia and served as a tool for implementing knowledge, standards, and practices concerning reproductive behavior, which became a serious public concern. While the idea of eugenic premarital bureaux was explicitly linked to the Czechoslovak eugenic movement aimed at preparing young adults for proper marriage in a biological sense, the role of counseling bureaux for mothers and children regarding family planning and reproduction remains hidden in the background of their social and health mission. However, this article suggests that we may view counseling facilities as a means of population policy that intervened in reproductive-related issues to combat the nation's threat, a declining birth rate.
Drawing from Michel Foucault's concept of power, especially the relationship between power and knowledge, I examine practice of counseling bureaux as a way of governing human beings. My theoretical and methodological approach draws on the concept of biopolitics, a product of modern society, the focus of which was directed at the masses, literally the “body” of the population, and its demographic processes of mortality, natality, migration, etc. 2 Similarly, a newly established Czechoslovak Republic started policing “not only the boundaries of its polity but also the bodies of its citizens and families” 3 and health and eugenic concerns became part of a biopolitical agenda and intertwined with modern processes of nation-building.
Inspired by the concept of medicalization and biopolitics, I will demonstrate through the analysis of medical discourse how medical professionals foregrounded the idea of a healthy family, largely inspired by a (pseudo)science of eugenics, in order to maintain appropriate quantitative and qualitative population development. An important aspect of biopolitics was its normalizing nature, which was intended to protect society against “abnormal” and potentially dangerous individuals. This article primarily looks at the formation and activities of counseling bureaux during the interwar era, which witnessed the institutionalization of public health care and social protection, both on the national and international levels. During the period under investigation, newly created institutions provided the basis for reinforcing the position of professionals and reproduced the variety of procedures and practices aimed at protecting the health of the nation. 4
This article aims to address preventive health care and health promotion concerning reproductive issues as modes of governing human beings, directed in the case of eugenic bureaux toward the general public in contrast to counseling bureaux for mothers and children, which primarily targeted women. Public health thus represents a form of governing that addressed not only human transformation, but also human conduct; transformation of the body and mind, which occurred with the emergence of problematizations, i.e., the decreasing birth rate, declining marital fertility, differential fertility, or high infant mortality. Moreover, the fight against depopulation seems a relevant case for exploring more how people were governed and governed themselves along the lines of prescribed norms of health, which singled out categories of desirable and non-desirable (abnormal) modes of reproduction and set up a paradigm of the healthy family and “normal” trajectories of healthy offspring development.
The Demographic Context
During the interwar period, the newly established democratic republic of Czechoslovakia, which had emerged after World War I, was hit with a slowdown in demographic growth. This regression came to an alarming point during the 1930s when politicians and experts addressed the issue of declining fertility. 5
Generally, the numbers showed a long-term phenomenon of a birth rate decrease. During the decade from 1926 until 1935, the number of births decreased from 199,022 (9.01) to 65,731 (4.09) and continued to diminish in the following years. 6 The surplus of live births per 1,000 people in Czechoslovakia decreased from 9.3 in the years 1919–1923 to 3.9 in the year 1937 (Table 1). 7
Surplus of Live Births per 1,000 People in Czechoslovakia.
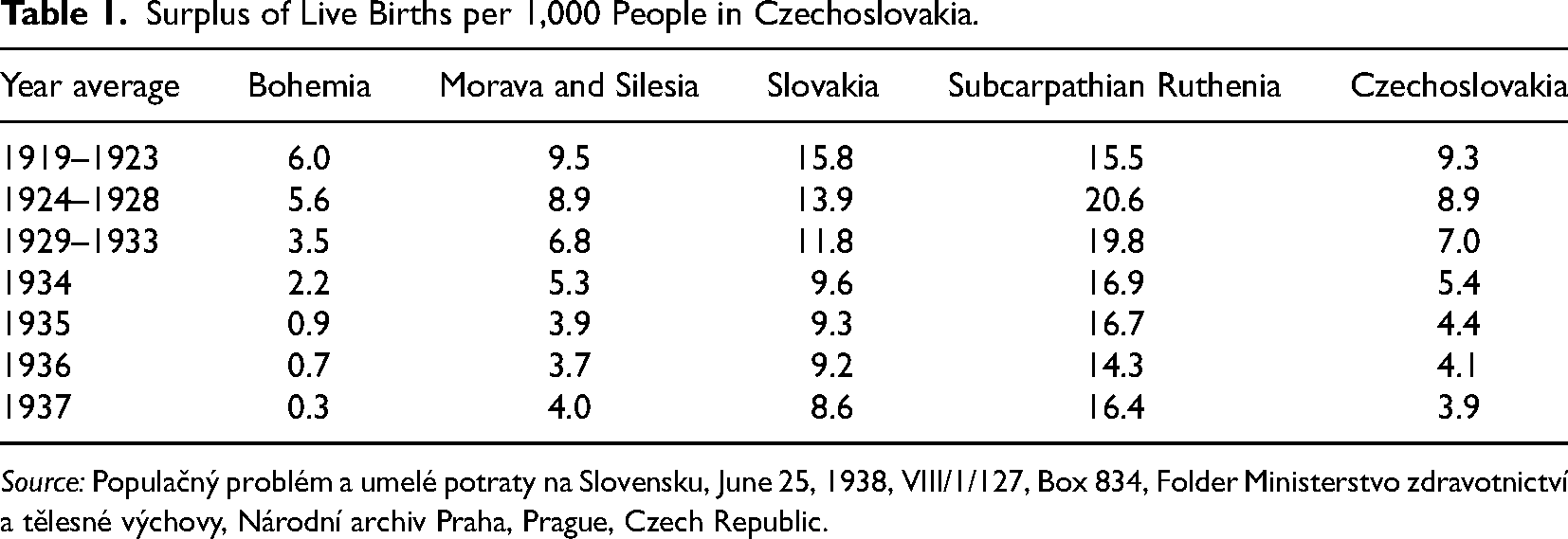
Source: Populačný problém a umelé potraty na Slovensku, June 25, 1938, VIII/1/127, Box 834, Folder Ministerstvo zdravotnictví a tělesné výchovy, Národní archiv Praha, Prague, Czech Republic.
However, there were significant contrasts in the population dynamics of two different types of fertility across the Republic, which required various approaches in population policy. On the one hand, the population in the Czech lands (Bohemia, Moravia, and Silesia) had started to follow a downward trend before the World War I and copied the development in the countries of the West-European cultural sphere. This development left Czechs with the second lowest birth rate in the Habsburg Monarchy, thirty-two children per 1,000 people, directly behind the Germans with thirty children per 1,000 people, and this decline continued in the following decades. 8 On the other hand, the population in the eastern parts (Slovakia and Subcarpathian Ruthenia), referred to as the “population reservoir”, kept increasing. Nevertheless, overall, natality decreased in the country from the east to the west, accompanied by a high coefficient of infant mortality, which proved a severe and ongoing problem. 9
While historian Radka Šustrová has pointed out that there was practically no population policy in interwar Czechoslovakia, and no particular success of a visible improvement in the population curve, 10 historian Pavol Tišliar has spoken of a somewhat contradictory and unsystematic policy, which manifested itself in a significant effort to support the most endangered part of the population, i.e., mothers, children, and youth, while the state simultaneously regulated population by means of passive and active migration policy, namely from Slovakia and Subcarpathian Ruthenia. 11
Both aspects, quantity and quality, were present in the debate on depopulation. As a professor of genetics Bohumil Sekla wrote in 1936, there was a qualitative eugenic problem hidden behind the falling birth rate and “…there is differential fertility, whence it follows that this period of transition from the naive to the rational type of population development brings with it, as studies from different countries suggest, increased dysgenic risks for future generations. In this period, the process is continuing on such a large scale that an impoverishment in the hereditary endowment of the population must result.” 12
The term differential fertility, a concept conceived by various experts researching demographic changes, represented an observed difference in the fertility value of individual strata of the society and became a pretext for positive and negative interventions (in a eugenic sense) in reproduction policy. The divergence in fertility was viewed—in particular, but not only by eugenicists—as problematic and endangering the nation. Especially striking differences between the “healthier and more cultivated” strata that limited its natality versus the “less able” that “barely” controlled its fertility was, according to them, a severe cause for alarm. 13 However, the question of belonging to one of the groups (genetically valuable or inferior) was multifaceted and not purely a matter of the genetic makeup of an individual but was also determined by their social status, ethnicity, education, etc. Historian Victoria Shmidt recognized the role of race science in Czechoslovak politics concerning ethnic minorities, i.e., Jews, Roma, and Rusyns, as the opposite of a healthy majority 14 and pointed out the intersectionality of ethnicity and inferiority, which resulted in an institutional form of violence such as forced sterilizations in the second half of the twentieth century against minorities, in particular Roma. 15
However, negative eugenic ambitions concerning reproductive behavior such as medical certificates for spouses 16 or eugenic sterilization 17 proposed by the Czechoslovak eugenic movement to prevent a deterioration of the population's quality proved not to have sufficient political or expert support in the interwar era. Nevertheless, both measures remained the core requirements of the movement to combat the spread of venereal diseases, the crisis in institutional care, and the growth of the population in the eastern Czechoslovak periphery. 18
The depopulation discussion also shifted the focus to the family as a natural reproducer of the nation and a means for ensuring its status and protection. The disintegration of family life, marriage crisis, an increasing proportion of single and two-child families, the advance of modern lifestyles, and women's emancipation were all issues that attracted the attention of experts as they searched for the causes of the fertility decline. 19 As historians Jakub Rákosník and Radka Šustrová argued, the population crisis produced a discourse of national extinction that allowed a gradual creation and formulation of family policy. Yet, it was only after the World War II that a conceptual and complex family policy was introduced in Czechoslovakia. 20
However, growing public concern about the future generation directed experts’ focus toward public health, namely improving social and health care for mothers and children due to the high infant mortality rate. This effort manifested itself in tackling premature mortality, following the motto of the first Czechoslovak president T. G. Masaryk “that people may not only be born, but also alive.” 21 The new working concept of the Ministry of Healthcare and Physical Education published and introduced by the minister Ludwig Czech in 1937 intended to create an appropriate framework in three directions: youth health care, medical school inspections, and social and health care for women and mothers in close cooperation with the Ministry of Social Care. 22
In this respect, the attention of medical experts and public figures refocused on the fight against child mortality, saving and supervising children, both after conception and birth, and protecting mothers based on a new type of preventive health care. District offices were supposed to take part in a campaign to keep the number of live births as high as possible (statistics from 1937 showed that of 80,000 live births in Slovakia, 12,000 children died under the age of one) and help to keep “numerically strong and healthy offspring.” 23 In this regard, counseling bureaux for mothers and children were promoted as institutions in charge. Slovak pediatrician, university professor, and pro-natalist Alojz Chura referred to them as “active eugenic components,” which could contribute to the future generation's higher birthrate and healthy physical and mental development. These bureaux provided medico-social care and education on health-related issues to mothers and children and its basic aim was to ensure that healthy couples reproduce healthy offspring. 24
Attempts to Influence Reproduction from a Eugenic Perspective
Soon after the World War I, the first attempts were made to introduce eugenic principles concerning family and reproduction policy into the Czechoslovak legislature. In 1919, the government wrote a draft proposal introducing compulsory medical examinations before marriage. 25 In § 1 of the marriage law, the government proposed an amendment according to which the couple could be married “only if they can prove with a medical certificate issued by a publicly appointed doctor that they are not burdened with a disease that transcends the purpose of a marriage or which would be detrimental to the health of the other spouse or offspring.” 26 According to the explanatory memorandum, draft authors considered it essential to ensure, at least temporarily, that only healthy couples marry “right now when soldiers from different countries are returning,” and because of the kinship marriage practice in Slovakia. 27 Although the draft proposal was presented as a campaign against venereal diseases and kinship marriage practice, the very idea of marriage certificates was linked to the Czech eugenic discourse and presented already prior to the World War I. Though not accepted then, eugenic rules applied to the act of marriage, or the so-called marital revision, was among the core requirements of the Czech and later Czechoslovak Eugenic Society (Československá eugenická spoločnosť) and considered a condition sine qua non to improve the state of humanity. 28 According to eugenicists, the purpose of medical certificates was to achieve a healthy marriage, in which it would be possible to take care of the offspring as well as possible and thus also to take care of the existence of the nation, state, and society. 29
According to the eugenicists, marriage, as an institution of fundamental importance, required in addition to legal and social, also health protection from the state and support to prevent the spread of venereal diseases, tuberculosis, and hereditary physical and mental defects. 30
Nonetheless, the State Health Council in Czechoslovakia expressed fundamental objections concerning the proposal, resulting in the draft's withdrawal. The main contra arguments were the impracticability of the law, insufficient scientific knowledge, interference in the private sphere of couples and families in favor of public health concerns, and the impossibility of monitoring extramarital sexual relations and fertility. 31 However, as historian Victoria Shmidt concludes, there was another argument against obligatory premarital medical examinations, represented by general resistance to the secularization plans, including resistance to civil marriage. “According to Catholic experts, medical assessment could not replace the moral obligations established by religion, nor could civil marriage substitute for a marriage made in heaven. The power of physicians’ authority could not be a viable alternative to the moral obligations set out for women and men as prescribed by the Christianity.” 32
Likewise, medical circles also expressed their doubts about marriage restrictions. As a Czech physician, Josef Pelnář concluded in his article on eugenic restraint: “The future of the human race will, I think, continue to depend on the subconscious and unconscious components of the sexual search in men and the sexual lure in women, on instinctual choices that can be somehow regulated by intellectual and emotional culture but not replaced.” 33 Although not on a mandatory basis, the eugenic movement started to emphasize conscious consideration of eugenic aspects in partner choice and family planning via the platform of premarital eugenic bureaux. These premarital bureaux, in addition to medical examinations, spread eugenic propaganda and tried to pave the way for an acceptance of the need for the legislative introduction of eugenic measures. 34 The first bureau was established in Prague in 1916 35 , and during the 1920s and 1930s, there were similar institutions opened in other towns such as Hradec Králové, Brno, Topoľčany, Košice, and Užhorod. 36 The bureaux provided a medical examination of couples due to be married, collected statistical material, provided expert opinions, and served as a counselor for engaged and married people in all matters of married life, including health, sexuality, and legal advice. 37
The bureaux, led by medical experts, focused their work on issues of practical eugenics regarding heredity and genealogy. Among the practical requirements of the eugenic movement were comprehensive care for pregnant women and mothers, comprehensive health and social care for children, fertility maintenance, laws on fetal protection, standard birth rates, etc. 38 The main focus was on the protection of spouses from infectious diseases, assurance of the marriage purpose, i.e., fertility, fetal delivery, and childbirth, and on the protection of offspring from sexually transmitted diseases, tuberculosis, nervous diseases, fetal alcohol syndrome, etc. 39 The medical appraisal either encouraging or discouraging the marriage intention was of a recommendary nature, and the final decision was left to the couple. According to eugenic proponents, marriage and family were essential life steps that the couple should have approached wittingly, with a sense of moral responsibility and, most importantly, conscious of their state of health. 40 Eugenicists, aligning themselves with national ideas and a belief in progress, brought into action a motive of responsibility toward future generations and informed the public about the negative consequences that could occur if genetically burdened offspring were further procreated. From Foucault's point of view, the imperative of health was a duty for everyone and a goal for all. 41
The Ministry of Public Health and Physical Education considered eugenic bureaux beneficial and promoted the establishment of other eugenic facilities under the administrative and supervisory center of the Czechoslovak Eugenic Society and the Czechoslovak Institute for National Eugenics (Československý ústav pre národnú eugeniku). 42 However, there were very few eugenic bureaux in interwar Czechoslovakia. They were an exception rather than the rule, and the eugenic efforts remained illusory in the context of free marriage. Eugenic activities partly overlapped with other counseling centers, i.e., clinics and counseling centers for venereal diseases, prenatal counseling, or counseling for mothers and children. Despite the negligible number, eugenic bureaux were an interesting element in the campaign to promote healthy marriage and families, which was often seen as an issue with national ramifications. As a preventive, prophylactic, voluntarily organized healthcare component, eugenic marriage bureaux were generally perceived positively. Both progressive and conservative medical and political circles emphasized the importance of health screening prior to marriage. However, there was no such consensus on the issue of providing contraceptive means and information via eugenic bureaux. 43 Historical sources suggest that contraceptives were not distributed in eugenic bureaux at all, 44 although eugenicists, like Czech doctor and biologist Vladislav Růžička, recommended contraception in extramarital affairs as protection against venereal diseases and extramarital conception. 45
The public's interest in eugenic or marital advice was, according to the publication “A Question of Progeny – A Question of National Existence” (Otázka potomstva-otázkou národného bytí), 46 reflected in the number of visitors to private doctors’ clinics. This suggests that people turned to regular medical practices in the search for information on marital life. Similarly, appropriate marital and eugenic counseling was mediated via an extensive network of counseling bureaux for mothers and children, and some of these worked as sexual or contraceptive clinics. 47
Counseling Bureaux for Mothers and Children
Counseling bureaux for mothers and children represented a new form of voluntary health and social care institutions in interwar Czechoslovakia that practically did not exist before the war. Its origin can be traced back to nineteenth-century France, when Professor Alphonse Hergott and Dr. Piere Budin introduced in 1892, the concept of “well babies clinics” as a reaction to downward demographic trends and infant mortality. This happened in the context of France after the Franco-Prussian War, where there was depopulation in contrast to expansionist Germany. “Well babies clinics” promoted breastfeeding as a primary method for reducing infant mortality and improving infants’ health. Since they proved successful, they expanded throughout Europe. 48
In Czechoslovakia, counseling bureaux for mothers and children increased in number after the World War I. However, clinics in the form of milk stations set up by the association Protection of Mothers and Infants (Ochrana matek a kojenců) had already existed as charitable organizations during the war when they were set up in response to the conditions of general material and food deprivation to support mothers and infants. 49
After the World War I, American Red Cross personnel who operated in Czechoslovakia from 1919 within the American Relief Administration, a mission aimed at combating children's malnutrition and infant mortality through a nationwide canteen system, built a network of approximately twenty-one clinics “For Our Children” (Naším deťom), mainly in heavily populated industrial regions. 50 British Red Cross personnel, based at that time in Slovakia, then established sixteen social health stations for children and mothers in rural areas. 51 The latter were forerunners of later counseling bureaux for mothers and children (Poradne pre matky s deťmi), which were run by the Czechoslovak Red Cross (in Slovakia and Subcarpathian Ruthenia) and later in the 1930s by the District Youth Associations (Okresná starostlivosť o mládež). 52 The For Our Children counseling facilities maintained a separate position when the Ministry of Public Health and Physical Education overtook these centers of child hygiene in 1922. 53
The bureaux, led by medical doctors, were supposed to be fundamental pillars of the new systematic child, putative healthcare policy priority of the new Republic, which was supposed to flourish under the motto “healthy mothers and healthy children” (Figures 1 and 2). 54

Bratislava city counseling bureau for mothers and children.

Bratislava city counseling bureau for mothers and children. The equipment of the counseling bureau was a gift from the American Red Cross.
The number of For Our Children clinics and mother–child counseling facilities within District Youth Associations kept increasing. As of 1936, there were around 2,314 mother–child and maternity counseling centers operating at the national level, forming a dense network of social and health facilities across the Republic. 55 As of December 31, 1937, 143 counseling facilities for mothers and children were operating only in Slovakia. 56 The goal was to establish a consultation service in each health district so that every mother would be in the care of a counseling center before and after giving birth. However, the reality was discrepant, the pace of setting up new facilities ran slow, and the goal remained unfulfilled.
The nature of counseling bureaux underwent a visible change, from their supportive postwar function focused on children suffering from malnutrition gradually into a research role of a sanitary and pedagogical nature. The focus also shifted from the transformation of children's bodies toward the transformation of conduct, particularly relating to women and children. Czech Professor of Social Medicine, Hynek Pelc, defined these counseling centers as “institutions, specially equipped to provide counseling based on professional examination and to mediate the implementation of advice by making contact with families through the visiting service.” 57
However, their objective included more areas: (1) Systematic examination of the health and social conditions of children up to fourteen years of age by inspecting or visiting their homes and investigating the causes of health and social weakening; (2) Educating the general public to use legal facilities that provided the poor with medical care, counseling, medicine, and legal and social assistance; (3) Provision of medical and social assistance to the poor who were not insured and were insufficiently secured by relief for the poor; and (4) Educating mothers and children about the knowledge of basic health rules, prophylaxis, especially about maternity and childhood, increasing revenue by promoting private donations, and recruiting communities and corporations to support these goals. 58
Under the Scrutiny of Doctor and Social Worker
Systematic health examination of children, which was one of the counseling activities, included an examination of the child, search for ill family members or roommates, sensory diseases, spinal deformity, hidden incipient tuberculosis, and blood testing to detect hidden syphilis. Furthermore, medical practitioners and social workers identified general deficiencies that could lead to a child's disorder like insufficient or excessive warm clothing, lack of personal and oral hygiene, dioptric problems, insufficient nutrition, poor posture, constrictions in the waist, or issues related to the household deficiencies like a lack of a separate bed for a child, unventilated rooms, or the presence of ill or infectious household members. The aim was to maintain the health of healthy children and intervene in the case of a deviation from the norm. Although examinations centered around the child, the family and family environment were also scrutinized. If anything pathological and undesirable was found within the family environment, which was considered a contagion center, affected family members had to similarly undergo rectification, i.e., through referral to an anti-tuberculosis bureau, anti-venereal bureaux, alcoholism treatment, etc.
The social workers who provided the visiting service monitored children's home environments and mediated and supervised the implementation of advice. 59 The core idea of the counseling was that the intervention itself must take place within a family, and the visiting service enabled this intervention. However, reaching out to the mothers and fathers involved a long process of transformation and confidence-building toward medical professionals and social workers, especially in rural areas, where superstitions, distrust, and a lack of general health knowledge persisted, and parents resisted subjecting children to preventive examinations. Similarly difficult was the task of attracting and engaging the wider public, including middle-class strata, in issues of public health and preventive care. As director of the Slovak division of the Czechoslovak Red Cross, wrote:
“People and intelligence still underestimate the importance of hygienic advice relating to life adjustments. They forget that changing damp, dark, and crowded flats, adjusting the ventilation and use of the sun and nature, improving nutrition and clothing, and raising awareness of the extent of infection and the importance of breastfeeding is often many times more important than medical treatment and material support and that moral support is much more important than material support.” 60
As archival sources suggest, especially people among the lower strata of the society responded to the material assistance and medical treatment provided in counseling bureaux (except in large cities, where bureaux in principle did not treat patients), which made them visit counseling facilities. However, women who were primarily interested in material support in the form of milk vouchers, baby equipment, medicine, clothes, baby powder, etc., were often criticized by social workers as being “greedy.” Nevertheless, as Hynek Pelc wrote, “advice is not attractive enough,” and acknowledged these material benefits as a means of attaching people to counseling. He understood the development of counseling activities in three stages, depending on the population's education level. In the first stage, it was necessary to provide people with material help to encourage them to pay a visit to the counseling bureau. In the second stage, a physician was required to perform a medical procedure, and in the third, final stage, counseling would be able to focus on education, which had to be masked in earlier stages by more immediately desirable services. 61
The activities of counseling bureaux for mothers and children addressed improving and adjusting the social, health, and living conditions of families, based on general hygiene principles, thus setting standards of health, child welfare, and family behavior. Organizing public health care that would minimize the mortality rate, together with the betterment of social conditions for families without causing a fear of social decline was seen as the best way to prevent a real population decline. 62
The discourse on depopulation and the refocus on the high infant mortality rate brought about a change and a shift away from the perception of the high infant mortality rate as a “natural necessity” or a component of natural selection. 63 The children who were previously referred to as a “human material incapable of life” were about to be “preserved for humanity as a productive element”. 64 Counseling bureaux for mothers and children played an important role in combating the opinion that the high infant mortality rate was inevitable and unchanging and promoting an understanding of children's needs. As stated by the Czech doctor, politician, and medical organizer operating in Slovakia, Dr. Ivan Hálek, children's mortality was generally accepted very easily by the society, and people used to say that it was good to have as many children as mugs, so that when one broke, there would still be some left. 65 The aim was now to change such attitudes and populations regarded by experts as exhibiting primitive population development—typically with a high birth rate on the one hand and a high mortality rate on the other—presented a unique opportunity for practical population policy. Systematic health care was perceived as a reliable means for its implementation. 66 According to Professor of Social Hygiene, Hynek Pelc, the desired result was a transition from “random” parenthood (nahodilé rodičovství) to “desired” parenthood (uvědomělé rodičovství), which would affect all strata of the society and involved regulating fertility by various means including contraception or abortion (considered a crime in interwar Czechoslovakia under §285 and §286 of the Criminal Code). 67 Counseling bureaux for mothers and children were a suitable intermediary of this goal. However, progress was hampered by their inconsistent character and the inconsistency of submitted information concerning family planning and reproduction. While some counseling bureaux for mothers and children operated as sexual health or contraceptive centers, others preached pronatalism. This stemmed from the leading personality of the medical professional involved in counseling service. Slovak pediatrician and university professor Alojz Chura expected all areas of prenatal care to be penetrated and guided by the spirit of anti-abortion, and the fight against contraceptives or any other “demoralization” of marital cohabitation. According to him, the whole organization of mother and childcare should promote and support a genuine population policy, building on ideals of an inseparable marriage, a morally strong family, and material support. He considered any form of contraceptive advice immoral and a sin against the nation and state. 68 He promoted instead quantitative eugenics, whereby the population's quantity naturally generates the desired quality. 69 But Czechoslovakia had no plan for a radical pro-natal policy. Professor of Social Medicine, Hynek Pelc, summed up Czechoslovak interests as a sufficient population in a balanced number, with the most orderly social conditions possible, so that the quality of the people who compose society would be as high as possible. 70 Thus, the focus was diverted to minimizing the mortality rate and uplifting social conditions for families.
However, counseling bureaux for mothers and children were a crucial intermediary of current health-related knowledge that influenced the country's reproductive behavior from the health point of view. After all, the primary mission of counseling bureaux was motherhood education, which was expected to reduce the high infant mortality and get women to cultivate their health. Similarly, like eugenic bureaux, counseling facilities for mothers and children brought up the motive of responsibility for the offspring. On the one hand, it was essential to arouse the mother's interest in nurturing her health. On the other hand, women were instructed that sinning against their child's health would be “an unforgivable sin,” also when committed out of ignorance.
Moreover, some doctors proposed that “women need to be taught about the natural law of inheritance: that children inherit not only their parents’ physical characteristics but also their personality traits, and that both mother and father must combat, overcome, and limit their bad qualities that they can pass on to their children.” 71
The need to cultivate one's own health, the importance of a medical examination before entering marriage, instruction on married life, maternity, and fostering the so-called “will to the child” (vůle k dítěti) were other vital points made by counseling. In addition to ensuring children's welfare, the second main objective of mother–child counseling was education relating to motherhood, which was celebrated yearly in May as a Mother's Day, and maternity care. The reduction of women's ignorance and lack of health information was one of the priorities, along with the regular prenatal and postnatal medical care (Figure 3). 72

Mother's Day in Námestovo, “everything for mothers” and “like mother, like family”.
Nevertheless, attracting pregnant women and mothers to counseling bureaux was a difficult task because many of them were not aware of the need for care, or rather the need for preventive examination. Alerting the expectant mother to this vital need was one of the prime and the most challenging tasks due to the scant public understanding of these objectives, a general lack of finance, lack of counseling’s’ conceptual workload, the low level of public altruism, and a lack of experts in this sphere. As there was no unified system for the registration of expectant mothers and newborns in counseling facilities for mothers and children, the centers had to cooperate independently with registry offices, insurance corporations, schools, and local midwives. Registering newborns sometimes required an individual approach, for example, when social workers visiting remote villages were notified about the birth of a child by means of the local custom of hanging a red ribbon from the window. 73
A more elaborate procedure was in the case of health-insured women. The insurance company would notify the counseling center about the expectant mother and invite the policyholder or dependent to visit the counseling center and recommended that she submit a voucher for pregnancy support according to Act No. 221/1924 on the insurance of employees in the case of illness, disability, and old age (Zákon o pojištění zaměstnanců pro případ nemoci, invalidity a stáří) through the counseling bureau. 74 The insurance act entitled policyholders to receive support during the postpartum period. A two-thirds wage allowance was paid to insured mothers for six weeks to take care of their children. Additional assistance came in the form of the so-called “breastfeeding premium”, whereby one-third of the wage was paid for twelve weeks after the birth only to mothers who breastfed their children. Insurance companies were to pay support only if the mother submitted a certificate from the counseling center as proof that she followed the advice and regularly cooperated with the bureau. However, this was not rigorously practiced, and premiums were paid even without a control. 75
Like French “well babies clinics”, a great emphasis was placed on breastfeeding because a significant percentage of infant mortality was due to disease of the digestive system caused by artificial nutrition in a form of cow's milk. More support on this topic was introduced in the form of a law partially banning wet nursing, forbidding the mother of a child under the age of four months to be admitted as a wet nurse unless she would be allowed to breastfeed her own child regularly. The authors of the law expressed that the service of wet nursing represented a “brutal exploitation of the poor” and was “despicable from a eugenic point of view, when a child whose mother could breastfeed was, in this case, sacrificed for the benefit of a “biologically inferior child”, whose mother was not able to perform that task.” 76 A decree of the Ministry of Public Health and Physical Education from December 1933 allowed for an even more systematic supervision of infants by introducing regular compulsory medical supervision of children in foster care and children born out of wedlock until the age of two by counseling bureaux. 77
Conclusion
Soon after the World War I, attempts began to be made in the newly created democratic Republic, to regulate the Czechoslovak legislature concerning reproduction in favor of public interest to secure healthy future population development. These attempts stemmed in particular from the eugenic movement, which wanted to infiltrate policy and family planning with eugenic principles. The ongoing demographic crisis, a declining birth rate, and observed differential fertility served as a pretext for various experts to justify state intervention in matters of marriage and reproduction. Two negative (selective) eugenic initiatives, namely compulsory premarital medical certificates and eugenic sterilizations, proposed by the Czechoslovak eugenic movement to prevent a deterioration of the population's quality, remained unfulfilled due to insufficient political and expert support and significant doubts surrounding the selective eugenics movement. However, eugenic promotion continued to be carried out via a relatively small number of private, free-of-charge, voluntary, eugenic premarital bureaux, which disseminated propaganda on healthy marriage in a biological sense and healthy families, which were often seen as issues with national ramifications. Eugenicists brought into action a motive of responsibility toward future generations and an imperative of health, which spouses were supposed to follow on the question of starting a family. The same motive of responsibility was adopted by counseling bureaux for mothers and children, voluntary associations set up to improve the social and health levels of children and their families. The supportive postwar nature of counseling bureaux for mothers and children focused on children suffering from malnutrition underwent a change into research, sanitary and pedagogical nature. Counseling bureaux for mothers and children, led largely by general practitioners, were a crucial intermediary in disseminating to the lay population current health-related knowledge, including information on reproduction, which emphasized women's biological role and the exercise of responsible motherhood. The activities of the counseling bureaux were clearly framed in terms of protecting the health of children as a future generation rather than supporting women's right to decide in matters of motherhood. Although some counseling centers for mothers and children may have operated also as contraceptive counseling centers, the emphasis on proper maternity performance under the medical scrutiny prevailed to maintain favorable population development, thus reducing infant mortality and morbidity, and ensuring healthy physical and mental development of children. An important aspect of counseling bureau for mothers and children was their normalizing nature to correct deviance on children's bodies and supervise mothers’ actions. In this case, mothers were expected to lean on modern scientific and medical knowledge and leave their skills, taught by their mothers, friends, family, or midwives behind.
Footnotes
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author discloses a receipt for the following financial support for the research, authorship, and/or publication of this article: This study was written with the support of the Slovak Research and Development Agency, Contract No. APVV-17-0399, project: “From the Monarchy to the Republic. The Transition Process of the Society in Slovakia in the European Context. From the End of the 19th Century till 1945” research at the Institute of History of the Slovak Academy of Sciences.