
Abstract

Keywords
Preamble
In a review titled “Forensic Evaluation of Sexsomnia” published in the Journal of the American Academy of Psychiatry and the Law, approximately half of the 27 cited articles explicitly included the term “sexsomnia” in their titles. 1 This suggests that since we first described the phenomenon in the Canadian Journal of Psychiatry, 2 sexsomnia has become increasingly recognized as a legitimate clinical entity.
A recent self-reported survey suggests that the condition may be more common than previously believed, with reported lifetime prevalence of approximately 7.1% to 10.1% and a current (past 3 months) prevalence of 6.1%. 3 Public awareness has also expanded beyond medical literature and sexsomnia was also featured in an episode of the popular medical drama, House, M.D.
Awareness of the condition is increasing, but sexsomnia may still be overlooked by clinicians. It is generally conceptualized as a subtype of non-rapid eye movement (NREM) parasomnia, a form of arousal such as sleepwalking. In the Diagnostic and Statistical Manual of Mental Disorders-Fifth Edition-Text Revision, 4 these disorders are characterized by incomplete arousal from deep sleep accompanied by complex behaviours occurring without full awareness.
The forensic literature describes a wide range of behaviours, including non-consensual sexual contact, masturbation and penetrative sexual activity while asleep. Sexsomnia is generally considered to arise from a primary sleep disorder rather than from paraphilic interests or other primary sexual disorders.2,4
Parasomnias encompass a spectrum of behaviours occurring during sleep or partial arousal, including somnambulism, sleep talking, sleep eating, sleep laughing (hypnogely) and even driving a motor vehicle while asleep. Sexsomnia can be conceptualized within this broader family of parasomnia disorders.
This brief clinician's guide aims to increase awareness of sexsomnia. It outlines initial screening questions and diagnostic indicators for suspected sexsomnia, identifies key precipitating triggers and provides an actionable framework for clinical assessment, collateral interviewing and referrals.
Relationship, Social and Legal Context
Sexsomnia can have significant interpersonal and psychosocial consequences. Amnestic episodes typically involve sexual behaviours directed toward a bed partner. The disorder is often chronic and may result in significant relationship strain and (in some circumstances) legal issues. Individuals may face accusations of sexual assault or non-consensual sexual behaviour during sleep, which may lead to legal charges and forensic evaluations.
A web-based survey conducted in 2004 explored psychosocial experiences associated with sleep-related sexual behaviour. 5 Among 121 respondents (mean age 37; 65% female), 6 primary problem areas emerged: fear and reduced emotional intimacy; guilt and confusion; feelings of repulsion or sexual abandonment; shame, disappointment and frustration; annoyance and suspicion; and embarrassment or a sense of self-incrimination. 5
In a 2019 review of 351 forensic referrals to a sleep centre, 41% were related to allegations of sexual assault. 6 Of these, 110 cases were accepted for forensic sleep evaluation after excluding cases better explained by other medical or psychiatric conditions, alcohol intoxication or illicit drug use. Sexsomnia was the most frequent diagnosis in this population. None of the evaluated cases was thought to be malingering.
Potential Precipitating Factors
In a survey of 219 respondents (mean age 30; 69% male), 92% experienced multiple episodes and 48% reported sexual intercourse during sleep. Sexual behaviours during sleep are often triggered by factors such as physical contact with another person in bed (64%), stress (52%), fatigue (41%), alcohol (14.6%) and drugs (4.3%), with nearly half (47%) of affected individuals reporting another sleep disorder. 7 In a recent study, 30.4% of individuals with sexsomnia reported that alcohol exacerbated their sleep-related sexual behaviours. 8 This may be the result of a combination of increased “deep” (N3) sleep and arousals.
Indicia of Sexsomnia
Several factors may be considered when determining whether an individual exhibits features of sexsomnia (Table 1). When such behaviours occur within established relationships, they may be unusual but do not typically lead to legal consequences. However, incidents with relative strangers carry serious legal allegations.
Indicia of Sexsomnia Highlighting Possible Triggers.
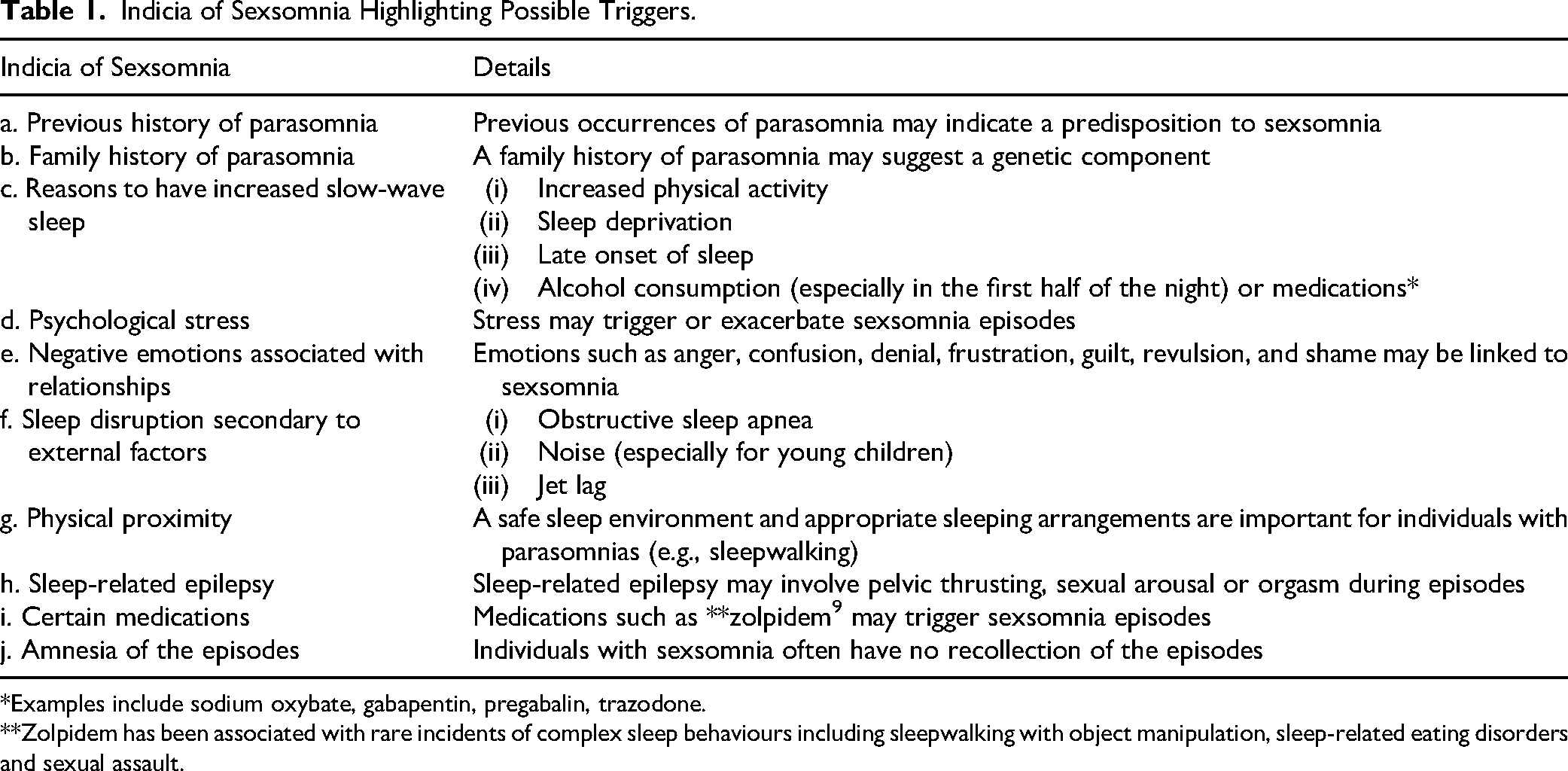
*Examples include sodium oxybate, gabapentin, pregabalin, trazodone.
**Zolpidem has been associated with rare incidents of complex sleep behaviours including sleepwalking with object manipulation, sleep-related eating disorders and sexual assault.
If a sexual interaction is non-consensual and the individual is awake, it constitutes sexual assault. When the active partner is genuinely asleep, the behaviour may be considered non-volitional. In many jurisdictions, this can mean the individual is not held criminally responsible. A central challenge in such cases is determining whether the individual was truly asleep or whether sleep is being claimed to avoid culpability. Because such events typically occur in private settings, there is often no independent witness and assessments must rely on the circumstances surrounding the episode, collateral history and evaluation for other parasomnias or precipitating factors (see Figure 1, Infographic).

Infographic.
A case encountered by the author (CS) highlights the challenges in assessing sleep-related sexual behaviour. At a gathering, a guest (“Z”) fell asleep near another sleeping individual. The next day, Z learned that sexual contact had occurred and reportedly expressed surprise, saying, “I think that may have been me.” Legal interpretations may vary, with some classifying such acts as “non-volitional,” others as “psychiatric conditions.” Regardless of jurisdiction, the possibility of feigning sleep must always be considered.
Clinicians are advised to differentiate sexsomnia from other nocturnal or behavioural conditions. Sleep-related epilepsy features highly stereotyped, often sudden, brief and repetitive motor seizures, while REM behaviour disorder occurs during late-night REM sleep, presents with vivid dream-enactment and primarily affects older adults. 4 In contrast, substance-induced disinhibition, dissociative states, active psychosis/mania, paraphilic disorders and malingering are distinguished by preserved conscious awareness, distinct daytime psychiatric symptoms or clear volitional motives.
For clinicians, the key point is that sexual behaviours during sleep can occur without conscious awareness and should be considered within the broader spectrum of parasomnias during clinical assessment.
Clinical Pearls
Footnotes
Author Contributions
CS is the first author and was responsible for developing the concept, conducting the majority of the literature search, drafting the principal content and structuring the manuscript to address the broad scope of the article. JG (forensic psychiatry) and CK contributed critical feedback, key references, substantive edits, essential content additions and guidance on the overall direction of the article. CK formatted and prepared the final manuscript and accompanying infographic and served as the corresponding author. Colin Shapiro coined the term “sexsomnia,” by which the condition has become widely known.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.