
Abstract
Past research on organizational change has explored how workers embrace change in some scenarios, resist it in others, and in some cases, subtly circumvent change efforts by feigning conformity. What remains unclear is the role of occupations in explaining workers’ responses to change. Using survey data (N = 226) and in-depth interviews with workers (N = 33) in a neonatal intensive care unit as it transitioned from a multiple-occupancy ward design to single-patient rooms, this study examines occupational discrepancies in reactions to the change. Findings reveal that misgivings about the move vary considerably across groups and illustrate the enduring significance of occupational identity.
The healthcare system is rapidly evolving as new technologies, evidenced-based practices, and institutional logics develop that purport to improve patient outcomes. These changes mean that healthcare organizations are consistently restructuring and implementing new policies (Cunningham et al., 2002). As previous studies have shown, healthcare providers play a vital role in shaping whether change efforts are successful (Jones et al., 2008; Kellogg, 2009). Studies suggest that the meanings workers attach to organizational change are particularly salient for understanding why some reform efforts are implemented while others fail (Brooks & Bosk, 2012; Kellogg, 2009; Piderit, 2000). In the context of healthcare, workers’ perceptions of change are often filtered through the lens of their profession (Dopson et al., 2002). Indeed, workers’ professional identities influence whether they view organizational changes as posing a threat to their occupational status or negatively affecting their work conditions (Dopson et al., 2002; Piderit, 2000). Studies of workers’ attitudes toward change originally simplified reactions into frames of embrace or resistance (Piderit, 2000). Within this dichotomy, resistance has often been depicted as stemming exclusively from workers’ self-interest, undermining the validity of their concerns (Dopson et al., 2002; Piderit, 2000).
Recent research includes a more comprehensive analysis of the factors that influence resistance to change, including rational concerns about the feasibility of implementing proposed changes and fears concerning the negative effects of change on one’s workplace conditions (Bartunek et al., 2006; Choi, 2011). These studies suggest that work roles and professional affiliation provide critical explanations for workers’ reactions to change. Yet studies of organizational change have largely overlooked occupational affiliation when accounting for variation in workers’ reactions to change efforts. A more explicit focus on occupations allows for the examination of how different groups interpret the impact of change on their workplace responsibilities, as well as how the change aligns with their occupation-specific training and corresponding beliefs about best practices.
To understand the motivations underlying different healthcare workers’ reactions to organizational change, we use the case of a neonatal intensive care unit (NICU) as it transitions to the single-patient room model. Employing a sequential mixed-methods design (Small, 2011), we document striking occupational variation in response to the move to single-patient rooms. Quantitative analyses of survey data collected prior to the move indicate that occupational differences in worries about move to single-occupancy rooms are rooted in differential assessments of the injurious consequences of the single-patient room model for patient care and work conditions. Analyses of in-depth interview data demonstrate that while some providers’ initial concerns eased following the move, new challenges also surfaced. Openness to the change was largely informed by workers’ professional identities, specifically, whether the changes to work conditions accompanying the move aligned with respondents’ schematic models of the goals and responsibilities of their occupational group. The present study contributes to research on organizational change by examining the meanings that different occupational groups ascribe to such changes and explicating the mechanisms that cause these meanings to evolve over time.
Theory and Background
Responding to Change
Organizational change has been widely studied across a range of disciplines. A key finding from these studies is the crucial role of employees in the overall success or failure of change efforts (Choi, 2011; Eilam & Shamir, 2005; Jones et al., 2008; Kellogg, 2009). Studies in this vein frequently examine employees’ negative reactions to change as a means of providing managers and organizations with strategies to avoid or mitigate worker resistance (Bhattacherjee & Hikmet, 2007). Other scholars have critiqued this approach, and the concept of worker resistance more generally, arguing that it privileges the perspective of managers and delegitimizes the concerns of workers (Eilam & Shamir, 2005; Piderit, 2000). In light of these criticisms, several scholars have pushed for an understanding of organizational change that more fully incorporates workers’ perspectives. These studies propose revised models and frameworks for understanding workers’ reactions that account for the multifaceted and dynamic reactions workers often have to organizational change (Choi, 2011; Hodson, 1997; Hoff & McCaffrey, 1996; Jones et al., 2008; Oreg et al., 2011; Piderit, 2000). For instance, in an extensive overview of worker resistance studies, Piderit (2000) proposes a tripartite conceptualization of employees’ reactions to organizational change that accounts for “emotional, cognitive and intentional” components (p. 783). Piderit (2000) similarly underscores the necessity of studying workers’ perceptions of change efforts and how these sentiments evolve over time.
Just a decade later, Choi (2011) assessed studies of employee attitudes—not just resistance—toward change. Relevant to the current study, in discussing the concept of “readiness” for organizational change, Choi (2011) notes that it is essential to consider organizational context, as employees actively seek out information when making assessments about change. Components of readiness are often studied as distinctive beliefs or attitudes that can be aggregated to assess a worker’s overall readiness for change. For example, in considering factors that might affect employee support for a particular change, scholars have assessed worker perceptions of the “appropriateness” of a proposed change (Armenakis et al., 2007, p. 484). Applying this concept to the case of the NICU, workers might view the move to private rooms as appropriate if they believe it will achieve its intended goals of reducing infections and improving patient outcomes. However, as a significant organizational change, the move to single-patient rooms carries multiple goals, making it essential to understand which aspects of the change are perceived as appropriate, since workers may hold conflicting beliefs depending on the specified outcome. Workers’ opinions of a particular change are also predicated on their beliefs regarding how the change will benefit themselves. This belief, termed “valence” by Armenakis et al. (2007, p. 488), is a significant factor underlying workers’ reactions toward change.
Within medical sociology, workers’ responses to healthcare system change have largely been understood as self-interested efforts to carve out jurisdiction over particular domains of patient care. Similar to studies coming from the organizational literature, more recent research has shown that organizational change is interpreted, experienced, and implemented by healthcare providers as more complex ways than previously imagined (Hoff, 2003). For instance, Kellogg (2009) examined the response of healthcare providers to work hour reforms across different surgical units. By examining workers’ experience of the change and the different meanings they assigned to it, Kellogg (2009) was able to document why hospitals that were otherwise similar had strikingly different outcomes in the implementation of work hour reforms.
These studies point to the significance of understanding both organizational context and individual worker attitudes. But despite expanded frames for understanding worker reactions to organizational change, there is a paucity of empirical research on the reactions of different occupational groups to institutional transformation. Given the importance of professional affiliation for workers’ respective roles (Dopson et al., 2002), and the increasing amount of cross-occupational collaboration (Hodson, 1997; Subramanian & Suquet, 2018), this study contributes to the body of knowledge on workers’ attitudes toward change by examining multiple occupational groups as they navigate the same organizational transformation.
Cutting Across Occupational Boundaries: Identity, Status, and Resistance to Change
A robust literature examines how the relative strength of workers’ organizational identification predicts reactions to change efforts (see Drzensky & van Dick, 2013, for a review). This research finds that in the midst of organizational turmoil, those who are highly identified with the organization not only report greater job satisfaction but are also less likely to resign (van Dick et al., 2006). While scholars have examined individual responses toward organizational change, we build upon this literature by emphasizing the importance of occupational affiliation for understanding reactions to change.
Professional identities deeply inform the disposition healthcare workers hold toward organizational change, and whether they view the evidence supporting it as credible (Dopson et al., 2002; Ferlie et al., 2005). When workers’ professional schemata 1 are challenged and forced to adapt to organizational changes that are incongruent with their cognitive representations of their profession and its mandates, it can inspire resistance (Scott, 1989). For instance, research on physicians’ attitudes regarding the use of computerized order entry forms indicates that doctors who perceive this technology as a threat to their clinical autonomy are more likely to resist its implementation (Bhattacherjee & Hikmet, 2007). Yet this resistance may not only represent an attempt to thwart reform efforts that pose a threat to autonomy but also “potentially valid employee concerns about proposed changes” (Piderit, 2000, p. 784). In the present case, occupational variation in worries about the single-patient room model may reflect not only anxieties about how the move will negatively affect one’s work conditions but also concerns about how the single-patient room model might adversely impact the quality of care providers are able to provide (Bartunek et al., 2006).
In terms of understanding occupational patterns of resistance to change in healthcare settings, the literature on workers’ reactions to mergers and acquisitions is instructive. This research finds that members of the dominant organization in these transactions view the merger as a continuation of their existing work obligations, whereas members of the subordinate group are more likely to view the transition as an existential threat (Gleibs et al., 2008). In the context of the rigid status hierarchy in the NICU, these findings suggest that status differentials across workers—denoted by occupational affiliation—might be instrumental for understanding employees’ reactions to change efforts. In settings such as the NICU, practitioners work closely in medical teams comprising providers belonging to different occupations of varying levels of status and prestige. For example, in their study of medical staff in a NICU, Heimer and Stevens (1997) found that lower status social workers helped physicians focus their energies on patient treatment by managing the “disruptions of social variability” presented by each case (p. 133). This research provides evidence for the importance of considering not only the individual but also the experiences and practices of groups (Dopson et al., 2002; Fine & Hallett, 2014).
Despite high levels of cross-disciplinary collaboration in contemporary healthcare, few studies have explored how organizational change is experienced by workers belonging to different occupational groups. This research finds that occupational status plays a significant role in shaping workers’ attitudes toward, and interpretations of, change in hospital settings (Leicht et al., 1995). For example, workers in jobs distinguished by greater levels of autonomy and proactivity—hallmarks of high-status occupations—are more likely to respond positively to organizational change (Cunningham et al., 2002; Hornung & Rousseau, 2007). However, this research tends to focus more on occupational characteristics, such as status, rather than the distinctions that exist across occupational groups. To this end, our study makes two primary contributions. First, studies have demonstrated the significance of professional affiliations and group membership for shaping beliefs, practices, and identities (Dopson et al., 2002; Tajfel & Turner, 1979), yet an examination of occupations remains largely absent from research on workers’ reactions to change. The current study explicitly examines this relationship and provides evidence regarding the importance of occupational distinctions for implementing organizational reforms. Second, by examining occupations as distinctive groups, we contribute to recent calls for the inclusion of “meso level” analysis in organizational studies (Fine & Hallett, 2014, p. 1786). By moving beyond individual attitudinal measures and considering occupational status, we aim to shed light on how professional identities actively shape workers’ perceptions of change efforts.
The Move to Single-Patient Rooms and the Status Hierarchy of the NICU
The transition to single-patient rooms is unfolding in healthcare organizations throughout the United States (Cunningham et al., 2002; Hornung & Rousseau, 2007). The single-patient room broadly refers to a physical arrangement in which each patient has their own, private room. In the NICU, this shift represents a major organizational change as units have historically been designed as large multipatient rooms (Floyd, 2005). Research suggests a multitude of benefits associated with transitioning to the single-patient room model, including improved patient outcomes, reduced length of stay, increased patient privacy, and reduced infection spread (Domanico et al., 2010; Floyd, 2005; Shepley et al., 2008; Walsh et al., 2006). But despite its many benefits, several studies suggest that this model also entails important trade-offs for hospital staff. This research indicates that the single-patient room reduces key aspects of teamwork, including communication and interaction among providers, with these unfavorable outcomes most commonly reported by nursing staff (Donetto et al., 2017; Walsh et al., 2006). Findings from this research also suggest it is important to adjudicate between the attitudes healthcare workers hold toward different aspects of the single-patient room model and the anxieties that such a major organizational shift might induce among workers. Indeed, while most nurses surveyed believed that the single-patient room was better for patient care than the open-bay setting, they nevertheless reported that this arrangement made their day-to-day work more difficult (Walsh et al., 2006). Such nuance may exist among other occupational groups.
To further interrogate these potential differences, we focus on four occupational groups whose day-to-day work was most directly affected by the move to single-patient rooms: doctors, neonatal nurse practitioners, registered nurses, and respiratory therapists. Doctors in the NICU typically work service periods lasting several weeks at a time. While on call, physicians are tasked with leading rounds, reviewing patient histories, and making treatment decisions. As a part of their practice, the majority of physicians were also assigned service periods at other NICUs in the area. Neonatal nurse practitioners are nurses with advanced educational training, which allows them to exercise greater diagnostic autonomy than registered nurses. Although the clinical abilities of nurse practitioners more closely resemble those of neonatologists than registered nurses, state laws circumscribe the autonomy of nurse practitioners. Specifically, nurse practitioners in this study work in a state that is classified by the American Association of Nurse Practitioners (2018) as allowing “reduced practice”; meaning nurse practitioners’ ability to prescribe medication is based on a “collaborative practice agreement with a supervising medical professional.” In addition, nurse practitioners were responsible for gathering patient history information and, at times, presenting patient cases during medical rounds.
Registered nurses in the NICU typically work in 12-hour shifts, during which they are at, or near, the patient’s bedside. Registered nurses are typically assigned two patients during their shift. In the open-bay setting, nurses are assigned infants located in the same room as those belonging to two to three of their nurse colleagues. Nurses’ chief responsibilities include administering medication and feeding neonates. They also spend time talking with parents and assisting them with the care of their infant, and “charting”—or recording notes—on their patients throughout their shift. Respiratory therapists are healthcare professionals who specialize in the treatment of patients with cardiopulmonary issues. During emergency care situations, respiratory therapists initiate and monitor mechanical ventilation. In addition, respiratory therapists are responsible for checking-in on patients who are on, or potentially in need of, ventilation and responding to any emergent situations.
Past research suggests that provider reactions to the single-patient room are not uniform across occupations. While many studies of the single-patient room have focused exclusively on nurses, those that have broadened their analytic focus to include multiple professional groups find significant occupational variation in reactions to this model, with more favorable attitudes among higher status workers. For instance, Domanico et al. (2010) found that while nurse practitioners and neonatologists held similar, positive attitudes toward single-patient rooms, nurses possessed a far more pessimistic outlook. While providing evidence that healthcare workers’ professional affiliation informs their beliefs about the single-patient room model, Domanico et al.’s (2010) study looks at workers’ attitudes concerning individual components of the single-patient room model rather than overall worries or anxieties about the change. Furthermore, while this study includes survey data regarding postmove attitudes, it is not clear why occupations experienced shifts in their initial premove attitudes once the change occurred. As a consequence, this study does not fully resolve which mechanisms contribute to occupational differences in misgivings about single-patient rooms.
In the NICU we studied, doctors and nurse practitioners in the open-bay environment assessed patients across the unit, moving from one bedside to another during rounds, when performing procedures, or offering further assessment. By contrast, registered nurses and respiratory therapists spent the vast majority of their workday at patients’ bedsides or in the same room as their patients. Thus, members of these occupations were accustomed to being able to see their patients as they worked. In a similar vein, these workers were used to having multiple colleagues who were able to “keep an eye” on their patients at all times. The move to single-patient rooms thus represented a potentially more radical shift in the work conditions of, and patient care provided by, respiratory therapists and registered nurses compared with nurse practitioners and physicians. Cumulatively, these insights lead us to examine the following hypotheses: H1: Registered nurses and respiratory therapists will report greater worry about the move to the single-patient room than doctors and nurse practitioners. H2: Providers who view the single-patient room model as more negatively affecting work conditions will report higher levels of worry about the move to single-patient rooms. H3: Providers who view the single-patient room model as more negatively affecting patient care will report higher levels of worry about the move. H4: Occupational differences in worries about the move will be explained by occupational variation in negative evaluations of single-patient room model for work conditions and patient care. H5: Postmove, workers’ experiences in the single-patient room will be more important in influencing their overall opinions of the move compared with their professional identities.
Methods
Site and Sample
We employ a mixed-methods design to understand how healthcare workers respond to organizational change. We focus on the NICU of Midwest Hospital (pseudonym), a premiere children’s hospital in the Midwestern United States. Traditionally housed in their own hospital wing, NICUs are hospital divisions that specialize in the treatment of premature and critically ill newborns. As a Level-4 NICU, Midwest NICU treats the most severe cases in the region, with patients varying in length of stay from a few days to several months. We followed a sequential design for our data collection (Small, 2011). We began by collecting survey data from NICU staff prior to the transition to single-patient rooms to gauge whether there were occupational differences in reservations about the upcoming move. The first author then conducted an ethnographic study that spanned from the period before the move took place to after the change occurred to gain further understanding of how different healthcare providers made sense of, and negotiated, the move to single-patient rooms. Although our focus on a single healthcare organization precludes the generalizability of findings to other settings or implementation efforts, this study is one of the few to examine perceptions of organizational change across a wide range of healthcare workers. The study was approved by the institutional review board at Indiana University Bloomington: Protocol #1108006542 and Protocol #1209009495.
Quantitative Data
Quantitative data come from the Teamwork, Clinical Culture, and Change (T3C) in the NICU Study. From late 2011 to early 2012, we surveyed 257 of 296 members of Midwest NICU (87% response rate). For the present analyses, the sample is filtered in two ways. First, to focus on workers with direct involvement in medical care, we exclude support personnel—a varied group that includes social workers, chaplains, and custodial staff (N = 28). We also chose to exclude this group due to our specific interest in occupational distinctions. Including support personnel based on their unique job titles or even broader occupational categories would have potentially violated their anonymity, given that many of these positions were held by one or two individuals. Second, respondents with missing data on focal independent and dependent variables were also removed (N = 3), leaving us with a sample of 226 respondents. Table 1 presents descriptive statistics for the quantitative sample. Sixteen percent of the sample is comprised of doctors, 10% are nurse practitioners, 59% are registered nurses, and roughly 15% are respiratory therapists. The sample’s demographic profile is predominantly female (88%) and White (92%), which is a function of both the large number of nurses who comprise the NICU staff—nursing is a predominantly White, female occupation (McMenamin, 2015)—as well as the geographic region where our data were collected (a state where non-Hispanic Whites compose 63% of the population). Respondents report having worked in Midwest NICU for an average of just over 10 years (SD=8.9). A correlation matrix of key study variables can be found in online Appendix A.
Means and Standard Deviations of Study Variables (N = 226).
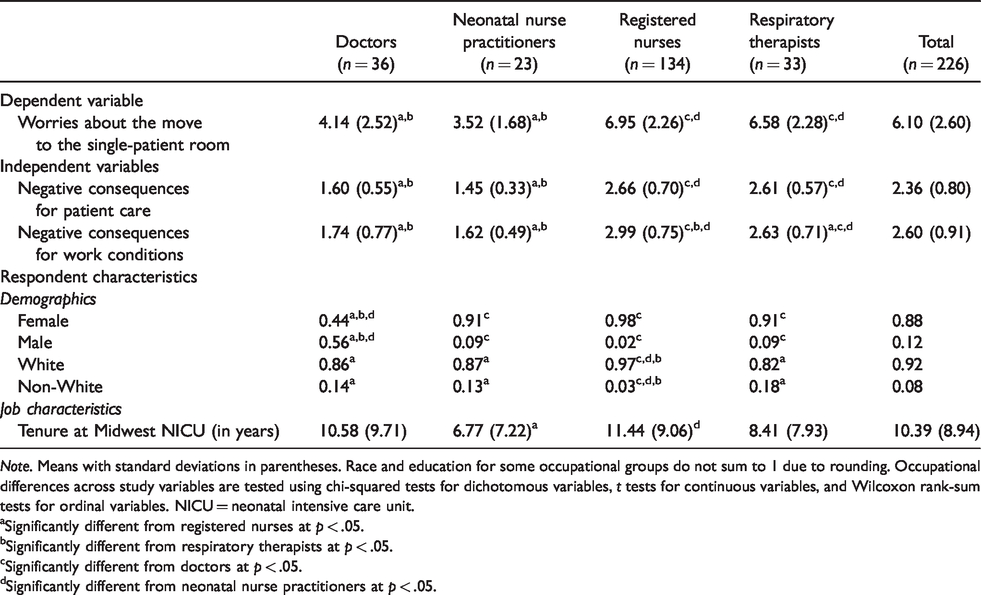
Note. Means with standard deviations in parentheses. Race and education for some occupational groups do not sum to 1 due to rounding. Occupational differences across study variables are tested using chi-squared tests for dichotomous variables, t tests for continuous variables, and Wilcoxon rank-sum tests for ordinal variables. NICU = neonatal intensive care unit.
aSignificantly different from registered nurses at p < .05.
bSignificantly different from respiratory therapists at p < .05.
cSignificantly different from doctors at p < .05.
dSignificantly different from neonatal nurse practitioners at p < .05.
Quantitative Measures
Worries About the Move to the Single-Patient Room
The study’s focal dependent variable, worries about the move to single-patient rooms, was measured by an item that asked, “On a scale of 1 to 10, where 1 is the least concerned and 10 is the most concerned, how concerned are you with the upcoming move to the single-patient room?” Response choices were anchored at (1) least concerned and (10) most concerned.
Negative Consequences for Patient Care
Respondents’ perceptions of the single-patient room model as having adverse consequences for patient care were assessed using several items adapted from the work of Walsh et al. (2006). These items asked respondents the extent to which they agreed with the following five statements: “Regardless of acuity and staffing, the single-patient room model is better for patient care” (reverse coded); “the single-patient room configuration is better for the growing preemie who is not on the ventilator and can tolerate 3:1” (reverse coded); “the large room configuration with a maximum of 5 babies is better for the care of the critically ill ventilator-dependent baby”; “the single-patient room configuration is dangerous for a ventilated infant”; and “the single-patient room configuration is dangerous for a ventilated infant even if staffing is 1:1.” Response categories range from (1) strongly disagree to (4) strongly agree. A mean scale measuring respondents’ negative assessment of patient care in the single-patient room model was created using these items (
Negative Consequences for Work Conditions
Three items written by the research team were used to gauge respondents’ perceptions of whether the move to single-patient rooms would negatively affect their work conditions. These items asked respondents the extent to which they agreed with the following statements: “The move to single-patient rooms will make me feel isolated”; “the move to single-patient rooms will hinder communication with my colleagues”; and “the move to the single-patient room will have a negative effect on my working relationship with colleagues.” Potential responses span from (1) strongly disagree to (4) strongly agree. A mean scale capturing respondents’ concerns about negative changes to their work as a result of the move to the single-patient room model was created using these items (
Occupational Group
Occupation is captured by a series of dichotomous measures where (1) Neonatal Nurse Practitioner, (1) Registered Nurse, (1) Respiratory Therapist, and (0) Doctor serves as the omitted reference group.
Controls
To explore occupational variation in worries about the move to the single-patient room, and to verify that differences are not merely a reflection of sociodemographic features that markedly vary across occupational groups, we incorporate a series of control variables into all regression models. Because nursing remains a female-dominated occupation, we control for respondent’s sex (male = 1). Similarly, because there are significant occupational differences in length of employment at Midwest NICU, a control is also added for NICU Tenure, which captures the number of years respondents report working in Midwest NICU. Race is a dichotomous measure coded as (1) non-White and (0) White. Due to high levels of collinearity between occupational categories and education (e.g.,
Analytic Plan: Quantitative Analyses
Analysis of quantitative data proceeds in several stages. First, a series of ordinary least squares models are estimated where variables measuring worries about the move to the single-patient room, and perceptions of the negative consequences of the single-patient room for patient care and work conditions, are regressed on occupational groups and study controls to discern occupational differences across these measures. Postestimate Wald tests are used to identify occupational variation in responses to these items. Next, reservations about the move to the single-patient room are regressed on scales capturing respondents’ perceptions of the negative consequences posed by the single-patient room for both patient care and work conditions to explore the associations among these measures. Next, to gauge the extent to which occupational differences in worries about the move can be attributed to perceptions of adverse patient outcomes or negative consequences for one’s work conditions, a series of mediation tests are performed. Specifically, we use a multiple mediator method developed by Breen et al. (2013) to decompose the contributions of each mediating variable to occupational differences in concerns about the move to the single-patient room.
Qualitative Data
Qualitative data are used to examine how medical staff navigate and make sense of the move to single-patient rooms. These qualitative data include field notes gathered by the first author at Midwest Hospital over a 13-month period pre- and postmove, as well as 40 in-depth interviews conducted with healthcare providers after the move to single-patient rooms took place. In the current study, we use data from 33 interviews conducted with members of the four occupational groups that comprise our analytic focus. This includes interviews with 17 registered nurses, 10 physicians, 3 respiratory therapists, and 3 nurse practitioners. Interviews lasted an average of 30 minutes.
Analytic Plan: Qualitative Analyses
Qualitative analyses occurred through the thematic coding of interview transcripts. The interviews were all conducted by the first author and were semistructured in format. All providers were asked a similar set of questions, including a series of questions focused specifically on their experience moving to single-patient rooms. The qualitative data were transcribed and coded by the first author, following the methods recommended by Emerson et al. (1995). Specifically, an initial round of open coding was first pursued to identify emergent themes in the data. Additional rounds of more focused coding followed, with an emphasis on refining codes related to providers’ experiences of the change, as well as their perceptions of how the change influenced patient care and workplace conditions (Emerson et al., 1995). Quotes have been slightly modified for readability and to preserve anonymity. Because this study is focused on providers’ attitudes toward change, qualitative analyses draw heavily from in-depth interview data due to the analytic leverage these data provide for understanding how NICU staff made sense of the change and justified their attitudes toward it. The findings presented here are broadly consistent with observation and field note data.
Quantitative Results
Occupational Variation in Worries About the Move to the Single-Patient Room
Models presented in Table 2 explore occupational variation in worries regarding the move to the single-patient room. In Model 1, which excludes study controls, nurses and respiratory therapists report significantly greater worry about the move to the single-patient room than both doctors—respectively, β = 2.81, p < . 001 and β = 2.44, p < . 001—and nurse practitioners—respectively, F(1)=45.32, p < .001 and F(1) = 24.86, p < .001. Doctors and nurse practitioners do not significantly vary in their concerns about the upcoming move. Likewise, nurses and respiratory therapists also did not significantly differ from each other on this measure. When control variables are introduced into the regression equation in Model 2, the relative magnitude and significance levels of these occupational differences are unchanged. Among control variables, only NICU tenure has a significant association with worries about the move, with respondents who have worked more years in the NICU reporting greater trepidation about the upcoming move than their less seasoned counterparts (β = 0.05, p < . 01).
Ordinary Least Squares (OLS) Regression Models Predicting Worries About the Move to the Single-Patient Room (N = 226).

Note. Unstandardized beta coefficients presented with standard errors in parentheses. NICU = neonatal intensive care unit; BIC = Bayesian information criterion.
aDoctors are reference group for all occupation variables.
bFemale is reference group.
cWhite is reference group.
**p < .01, ***p < .001; for occupational comparisons indicates significantly different from doctors (two-tailed test).
†††p < .001; significantly different from nurse practitioner (two-tailed test).
Occupational Variation in Negative Evaluations of the Single-Patient Room Model for Patient Care and Work Conditions
Table 3 examines occupational differences in perceptions of the single-patient room model as having negative effects on patient care and work conditions. In Model 1, which predicts perceptions of negative consequences for patient care, nurses and respiratory therapists report more negative evaluations of patient care in the single-patient room model compared with doctors—respectively, β = 1.06, p < .001 and β = 1.01, p < . 001—and nurse practitioners—respectively, F(1) = 72.81, p < .001 and F(1) = 46.29, p < .001. There are no significant differences between doctors and nurse practitioners, or between nurses and respiratory therapists, in viewing the single-patient room as having adverse consequences for patient care. When control variables are added in Model 2, these occupational patterns remain consistent.
Ordinary Least Squares (OLS) Regression Models Predicting Negative Perceptions of the Single-Patient Room Model for Patient Care and Work Conditions (N = 226).
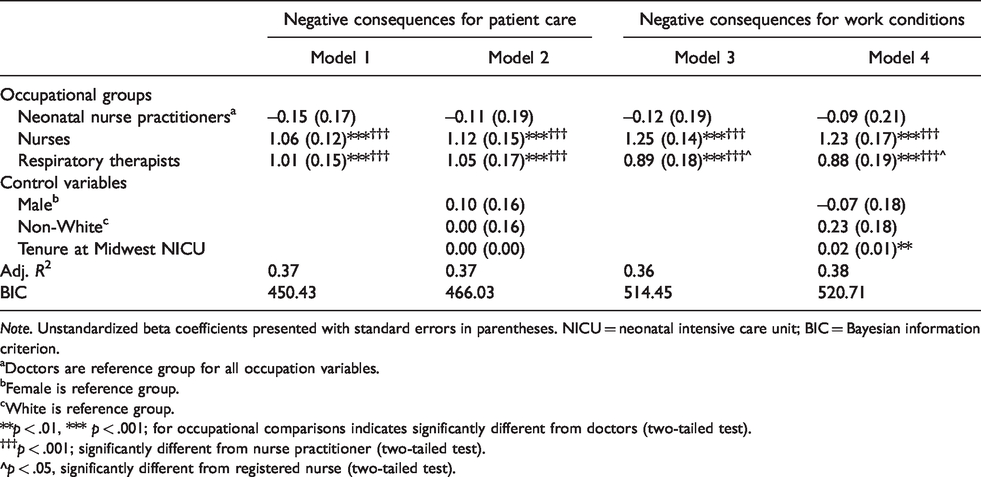
Note. Unstandardized beta coefficients presented with standard errors in parentheses. NICU = neonatal intensive care unit; BIC = Bayesian information criterion.
aDoctors are reference group for all occupation variables.
bFemale is reference group.
cWhite is reference group.
**p < .01, *** p < .001; for occupational comparisons indicates significantly different from doctors (two-tailed test).
†††p < .001; significantly different from nurse practitioner (two-tailed test).
^p < .05, significantly different from registered nurse (two-tailed test).
Models 3 and 4 in Table 3 present results from regressions predicting perceptions of the single-patient room as having injurious consequences for one’s work conditions. Results from Model 3 show occupational differences in negative evaluations of work conditions in the single-patient room that largely mirror those found for patient care. Both registered nurses and respiratory therapists are significantly more likely to view the single-patient room as having a negative impact on their work conditions than doctors—respectively, β = 1.25, p < . 001 and β = 0.89, p < . 001—and nurse practitioners—respectively, F(1) =69.91, p < . 001 and F(1) = 26.11, p < .001. Of note, registered nurses were also significantly more likely than respiratory therapists, F(1) =6.60, p < .05, to view the single-patient room as adversely affecting their day-to-day work. Doctors and nurse practitioners did not significantly differ on this outcome. When controls are added in Model 4, these occupational differences are largely unchanged. Only one control variable, NICU tenure, has a significant association with negative evaluations of the single-patient room for work conditions. Specifically, respondents who have worked in the NICU longer are significantly more likely to view the single-patient room arrangement (β = 0.02, p < . 001) as having negative effects on their work conditions.
Associations Between Worries About the Move to the Single-Patient Room and Negative Evaluations of the Single-Patient Room Model for Patient Care and Work Conditions
Table 4 presents results from models that regress worries about the move to single-patient rooms on negative perceptions of the single-patient room model for patient care and work conditions. Aligning with expectations, net of controls, more negative evaluations of the single-patient room model for patient care (β = 2.01, p < . 001) and work conditions (β = 2.00, p < . 001) are associated with greater reservations about the move to single-patient rooms.
Ordinary Least Squares (OLS) Regressions Predicting Worries About the Move to the Single-Patient Room (N = 226).
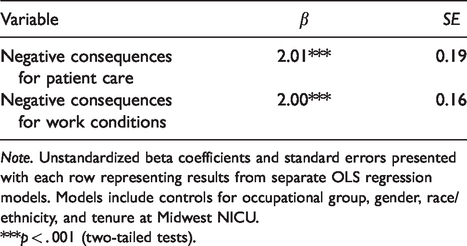
Note. Unstandardized beta coefficients and standard errors presented with each row representing results from separate OLS regression models. Models include controls for occupational group, gender, race/ethnicity, and tenure at Midwest NICU.
***p < . 001 (two-tailed tests).
Do Negative Perceptions of Patient Care and Workplace Conditions in the Single-Patient Room Model Help Explain Occupational Variation in Worries About the Upcoming Move?
In light of considerable occupational variation in negative perceptions of the single-patient room model for patient care and work conditions, we use mediation tests to discern the extent to which these divergent views contribute to occupational differences in trepidation about the move. Table 5 presents results from multiple mediator models for occupational differences in worries about the move that include all study controls.
Tests of Mediation for Occupational Differences in Worries About the Move to the Single-Patient Room (Teamwork, Clinical Culture, and Change [T3C] Study).
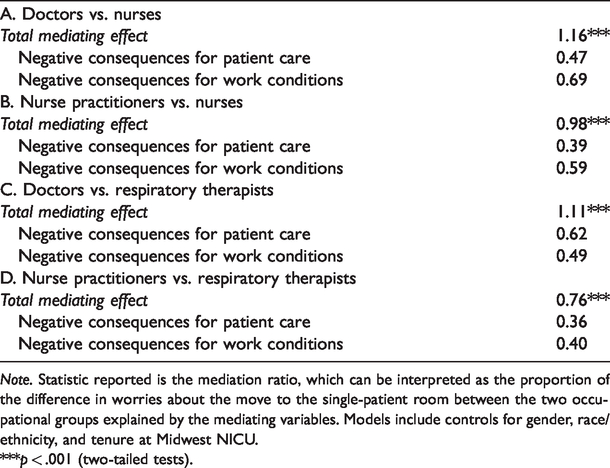
Note. Statistic reported is the mediation ratio, which can be interpreted as the proportion of the difference in worries about the move to the single-patient room between the two occupational groups explained by the mediating variables. Models include controls for gender, race/ethnicity, and tenure at Midwest NICU.
***p < .001 (two-tailed tests).
Results from Panel A indicate that controlling for negative evaluations of the single-patient room model for patient care and work conditions fully explains (p < .001) nurses’ greater worries about the move relative to doctors. While nurses’ heightened concerns about patient care explain 47% (p < . 001) of the difference between these groups, a greater proportion of the difference (69%) in reservations about the move can be attributed to nurses’ more negative appraisals of the single-patient room model for their work conditions. A similar set of findings can be observed in Panel B, where jointly controlling for negative evaluations of the single-patient room model for patient care and work conditions almost fully mediates (98%, p < .001) the difference between nurses and nurse practitioners in their worries about the move to the single-patient room. While nurses’ more negative evaluations of patient care in the single-patient room model explains 39% of the difference between these groups, an even larger proportion of this gap—59%—is explained by nurses’ stronger beliefs that the single-patient room model will negatively affect their work conditions. These patterns suggest that registered nurses’ greater anxiety about the shift to single-patient rooms relative to doctors and nurse practitioners is driven more so by their perceptions of the negative consequences of this model for work conditions than for the delivery of patient care.
Panel C presents results from a multiple mediator model that examines differences in reservations about the move between respiratory therapists and doctors. Simultaneously controlling for negative evaluations of the single-patient room model for patient care and work conditions fully explains (p < . 001) the difference between these groups. Roughly 62% of this difference can be attributed to respiratory therapists’ more negative perceptions of patient care in the single-patient room model, whereas a more modest proportion of this gap (49%) is explained by respiratory therapists’ stronger belief that this model will have negative ramifications for their work conditions. A slightly different pattern unfolds when examining differences in reservations about the upcoming move between respiratory therapists and nurse practitioners (Panel D). Controlling for perceptions of the negative consequences of the single-patient room model for both patient care and work conditions explains 76% (p < .001) of the difference in concern about the move between these groups. Respiratory therapists’ more negative evaluations of patient care and work conditions under this model contribute almost equally (36% and 40%, respectively) to this gap. Thus, while respiratory therapists’ greater worry about the move to single-patient rooms relative to doctors is motivated more so by concerns about the effects of this model on patient care than its consequences for work conditions, these factors contribute almost identically to their greater reservations about the move relative to nurse practitioners.
Qualitative Results
To explore whether and how NICU staff members’ attitudes toward single-patient rooms changed over time, we analyze qualitative data from in-depth interviews conducted with providers following the move to single-patient rooms. Qualitative results expand on the central findings of the quantitative analyses while also adding important insights into providers’ attitudes toward the change that were not anticipated during survey design. We begin with themes that were prevalent across interviews with respondents belonging to different professional groups before turning to occupation-specific themes.
In discussing their premove attitudes, many providers—most notably nurses and respiratory therapists—mentioned concerns that the move to single-patient rooms would negatively affect patient safety. For many providers, two initial fears were the potentially detrimental effects of the move for provider response times and the visibility of patients. After the move occurred, however, providers were more mixed in terms of whether they viewed the new space as a boon for patient outcomes. Among providers who felt that the move positively affected patient care, these workers mentioned the ability to safely monitor patients despite initial doubts about whether this would be possible in single-patient rooms, the quieter and cleaner environment fostered by the single-patient room model, and the increased privacy single-patient rooms afforded to families.
For example, Keera,
2
a registered nurse, describes how her worries about the move dissipated the more confident she grew in her ability to observe patients though the use of electronic monitors and other assistive technology: I was actually a little worried about how we would answer alarms. Like what if a baby had something happening? Would someone come out of a room and answer an alarm if you couldn’t do it quickly enough? How many people would be around at a time? I mean mostly just patient safety was a concern. After being over here, I feel like it’s not that big of a deal … . Having the extra monitors around where you can see what [patients are] doing helps a lot … . I feel like because of that I don’t have quite the concern I did before. (Keera, Registered Nurse) I love it [the single-patient room]. I think it’s wonderful. I think the babies alarm less, I feel like they get better rest, I feel like it’s great for the families that they’re here more [and] they interact more … . I can’t believe the conditions we worked in before, I could never go back. (Melanie, Registered Nurse)
While these justifications for embracing or opposing the change emerged across participants regardless of professional affiliation, analysis of the qualitative data reveals several clear-cut, occupation-specific concerns about the single-patient room. Of course, not all providers within an occupation experienced the single-patient room in the same way. Nevertheless, several themes were more strongly connected to certain occupational groups than others. These distinctions shed light on how professional group membership guides patterns of resistance and adaptation.
Nurses
In the original open-bay setting, 8 to 10 babies were cared for in a large, open room. At Midwest NICU, nurses are typically assigned two patients at a time. This staffing level meant that there were usually four nurses inside the open-bay room at all times. Other providers would also trickle in and out of the room as they conducted rounds, performed checks, and provided different treatments. Quantitative data highlight that nurses were particularly concerned that the single-patient room design would make them feel isolated and reduce their interactions with colleagues. After the move, several nurses, along with other providers, mentioned a decreased level of interaction with their colleagues. Jessica, a nurse, provided a typical description of what the change meant for coworker relationships: “I mean there’s less personal interaction with the nurses. You don’t know as much about each other as you used to. Just simply because you don’t spend a lot of time being close enough to interact” (Jessica, Registered Nurse).
Aside from these social aspects of the job, several nurses voiced concerns about staffing arrangements in the single-patient room. As Sheila, a registered nurse, puts it: I never thought that they would give us 3 babies at times, our acuity or our census has been very high right now and we’re in a staffing shortage, with no new hires in sight just with all the changes going on with (Midwest Hospital) and so now they have actually tripled, so [that means] taking three patients … it was funny because in the modules they never let us triple and you would think that in private rooms they wouldn’t do that. (Sheila, Registered Nurse) I think our biggest challenge [is getting] the right level of nurses that can take care of the child. Cause I mean [in the open-bay] if there were just two nurses and our room had ten patients in it even, but one of them [was a] level 1 [and] one [was a] level 3 … that would have been fine, right. But here [in the single-patient room] my one level 3 can be all the way down the hall around the corner and my level 1 [is] next right next to me. (Naomi, Registered Nurse) We can’t rely on other people to kind of know if something looks funny … . Now to do that, my person may be down the hall and around the corner … . I think our charge nurses and our management have done, or are working on and are doing a good job of putting people in the right places … (laughs) I had a moment a couple weeks ago, I mean I’ve only been here just over two years and I walked out and was like ‘oh I’m the most senior person in this hallway and I was like, that’s a big responsibility I feel that they’re putting on me. (Rachel, Registered Nurse)
Doctors
Mirroring quantitative results, doctors were not initially as concerned about the move to single-patient rooms as their colleagues. At Midwest NICU, these lower levels of concern among physicians were explained, in part, by the fact that several of the doctors had prior experience working in single-patient rooms at other hospitals. At Midwest NICU, doctors work as a part of a larger team of neonatologists who routinely rotate their service time among a select group of NICUs in the area. Some of the other NICUs in the area had already transitioned to units with single-patient rooms. For example, Dr. Miller discusses his experience moving to single-patient rooms: I’d already worked in a single room environment. I guess I’d already been through the concern about not being able to see all the babies at once and realizing that didn’t really affect my ability to care for patients in any way at all … . Here [at Midwest NICU] I’d already been in that environment so I don’t think there was anything that surprised me too much. (Dr. Miller)
Yet in reflecting on their experience of the move at Midwest NICU, some doctors felt that the move created less awareness about what was happening on the unit as a whole among the medical staff. Namely, doctors felt that providers across occupations were less cognizant of what was going on with patients outside of their assigned cases. For doctors, the move presented a new challenge, as they could no longer rely on nurses to be as readily aware of different patients’ statuses. This included nurses knowing whether parents had visited or whether a patient’s vital signs during their observation were within the normal range for that patient. In her interview, Dr. Moore, a neonatologist, described this shift and how it changed the type of information she could elicit from the nurses: It used to be, in the old module based system … . There would be a primary nurse assigned to a certain baby who knew that baby really, really well. But since they all [the nurses] kind of sat in the middle and they all kind of saw what was happening with all the babies they all had a sense of what was going on with all the babies … . And so if the baby got sick for some reason or if we were worried about the baby you had multiple people who could say “well this is not how the baby normally acts.” … . Whereas now I feel like with the babies in separate rooms, and the nurses really kind of spread out distance wise I feel like you don’t really get that quite as much. (Dr. Moore)
Respiratory Therapists and Nurse Practitioners
While the quantitative data showed dramatically different premove attitudes toward the single-patient room between respiratory therapists and nurse practitioners, qualitative results suggest they had similar experiences once the move took place. Specifically, while their patient loads did not notably increase, both occupational groups reported feeling busier as a result of their work taking longer to complete. In large part, this was a result of staff members having to traverse greater distances to check-in on patients and respond to calls from other providers. As Steve, a respiratory therapist explained: If you have a baby on a high frequency ventilator on one end of your assignment and a baby on a high frequency ventilator on the other end of your assignment, which I had last weekend, you’re going to be real busy. You’re gonna be way busier than if you have a baby in position 1 and a baby in position 10 [and] they’re 8 feet away from each other. If you have a baby in room 1 and a baby in room 10 now, they’re a hundred feet away from each other. And you can’t see anything that’s going on with your stuff from the other baby’s bedside like you could before. (Steve, Respiratory Therapist)
Nurse practitioners, who as a whole had little concern about the move prior to the transition, similarly discussed feeling busier in the single-patient room. As this segment of an interview with Shelby highlights, nurse practitioners felt they had to hasten their work in the single-patient room to account for the increased amount of time it now took them to cover patients in private rooms—a challenge that led some nurse practitioners to start doubting the benefits of the move. Shelby: I do think it [the single-patient room] takes more time to do what we used to be able to do and in theory I didn’t think that it would. But I do think it takes more time. Interviewer: So when you say adjusted, what do you think some of the biggest adjustments for either yourself or the NNPs in general have been? Shelby: Actually [the] physical part of it. Just getting to where you need to be all the time. Then playing into that the safety of your patients and [planning] can you take care of a sick [patient] over here and a sick kid over here.
Discussion
In this study, we drew upon survey and in-depth interview data to examine how healthcare workers with different professional identities respond to organizational change. We documented striking occupational differences in providers’ initial worries about the move to single-patient rooms, with these discrepancies rooted in differential assessments of how this model of care might negatively affect patient care and workers’ job conditions. Qualitative data draw attention to the subtle ways that professional schemata inform workers experiences of the move and shape their perceptions of whether the change is ultimately beneficial for care.
In our quantitative analyses, we found support for our first hypothesis: Prior to the move, nurses and respiratory therapists expressed significantly greater worry about the transition to single-patient rooms than doctors and nurse practitioners. Next, confirming our second and third hypotheses, we found evidence that providers who viewed the single-patient room model as having negative consequences for work conditions and patient care were more likely to express anxiety about the looming move to the single-patient room. Largely aligning with our fourth hypothesis, we found consistent evidence that much of the occupational variation in worries about the move could be attributed to occupational differences in negative evaluations of the single-patient room model for work conditions and patient care. Specifically, nurses’ higher levels of worry about the move relative to doctors and nurse practitioners were driven more so by how the change would negatively affect their work conditions than by how it might harm patient care. The same was not true of respiratory therapists, whose greater anxiety about the move vis-à-vis nurse practitioners was driven in equal parts by worries about the detrimental effects for patient care and work conditions, while their greater worry about the move relative to physicians was driven considerably more so by concerns about how the move would adversely affect patient outcomes. These results indicate that while workers’ concerns about how a change might impact their work conditions plays a prominent role in shaping healthcare workers’ misgivings about organizational change, so too do concerns about how changes might negatively impact patients. It is important to recognize that while there were clear distinctions across occupational groups in concerns about how the single-patient room model would negatively affect working conditions and patient care, these two measures may be related, as changes to one’s work conditions may have implications for the administration of care.
Given the stark occupational differences in premove attitudes about the single-patient room model, qualitative analyses sought to examine the durability of these sentiments and to understand which factors, if any, led workers belonging to different occupational groups to alter their views of the single-patient room. Qualitative results provide mixed support for our fifth hypothesis. We found that while some providers’ concerns persisted after the move, other workers’ attitudes shifted in unexpected ways. The relative resilience of workers’ attitudes toward the move was influenced in large part by perceptions of whether the changes to their work conditions and patient care following the move fit with staff members’ conceptions of their occupation’s responsibilities and functions.
Conclusion
The findings from this study further broaden the analytic frame with which workers’ reactions to organizational change are examined. Specifically, by focusing on multiple occupational groups consisting of collaborative frontline workers, this study contributes to the literature on workers’ reactions toward change by moving beyond individual-level attitudes to offer insights into why particular occupational groups may voice concerns about change compared with others. Further, this study highlights the dynamic sense-making process of healthcare workers as they navigate organizational transitions and the salience of professional identities—including educational training, work routines, and organizational expectations—for shaping worker reactions to change efforts.
Much recent research argues that individual emotive and cognitive states are central to predicting employee reactions to organizational change (Choi, 2011; Hodson, 1997; Hoff & McCaffrey, 1996; Jones et al., 2008; Oreg et al., 2011; Piderit, 2000). While accounting for these attributes is undoubtedly vital to painting a more complete portrait of worker responses to organizational change, our findings signal the enduring significance of professional affiliation for shaping how employees attempt to demonstrate their competence and reaffirm their clinical jurisdiction amid seismic organizational shifts (Abbott, 1988; Hafferty & Castellani, 2011). Given the interconnected nature of work in most workplace settings, it is essential to understand how institutional change is perceived and experienced by all members of an organization. This is especially true in hospital settings where numerous occupations work together side by side to ensure patient safety. By unpacking the meanings providers assigned to the move to the single-patient room, we show how medical staff differentially make sense of organizational change on the basis of their professional affiliation and occupational duties. This finding provides insight into why healthcare providers motivated by shared goals of patient safety and improved outcomes may nevertheless respond to organizational change in dramatically different ways. Understanding these varied responses may help to further disaggregate why certain healthcare reform efforts are successful in one setting but not in another.
This study is not without limitations. To begin, we examined a single organization undergoing a specific institutional change. By studying one organization, we were able to control for external variation in organizational culture and management styles. Our focus on a single organization also helped to ensure a high survey response rate, an increasing rarity in studies of medical professionals. Yet it must be recognized that by focusing on a single organization, this study captures only the experiences and attitudes of providers in one hospital unit. An obvious limitation of the quantitative data we utilize in this study is that several occupational groups are comprised of relatively few respondents, limiting statistical power in analyses that examine group differences in attitudes toward the move to the single-patient room. Caution must also be exercised in interpreting results in view of the measurement of our key dependent variable. We use a single item to assess worries about the move to the single-patient room. While multiple items that tap into these fears would provide a more holistic measure of healthcare workers’ concerns about the move that is less sensitive to respondents’ subjective interpretations of question wording (e.g., how workers may have construed the word “concerned”), this item was the only question included in the survey that directly asked respondents about their opinion regarding the impending move.
Another issue is that quantitative data capture only premove attitudes. To more fully describe healthcare providers’ experiences of organizational change, it would be helpful to gather longitudinal data that captures shifts in attitudes and perceptions before and after the implementation process. Our logic in gathering qualitative data after the move took place was to understand how healthcare providers subjectively experienced and made sense of the transition to single-patient rooms. To this end, the qualitative data we collected provide insight into the fraught, messy transition process healthcare workers navigate as part of organizational change, an aspect that can be easily obscured by solely relying on survey data. It is important to note that in analyzing qualitative data, we are reliant on providers’ memories of how they felt about the move prior to its implementation. Thus, it is important to keep in mind that some aspects of the qualitative data may be subject to recall bias.
Organizational change in healthcare is unlikely to slow in the future. As a consequence, understanding how providers make sense of and negotiate organizational change is critically important for discerning how reform efforts are actually implemented on the ground. We demonstrate the continued salience of profession-specific training, socialization, and cultures for influencing how different healthcare workers adapt to organizational change. Specific to the case presented here, our study finds that one way of smoothing the change process is to fully consider how levels of staffing are impacted by reforms that physically restructure healthcare settings. For example, both respiratory therapists and nurse practitioners had to respond to emergent situations for patients throughout the unit. Covering multiple patients in rooms that were distant from one another increased the amount of time it took to complete their respective tasks. It is imperative that organizations consult with those workers expected to be most affected by institutional change to gauge what they view as the core aspects of their work-related tasks. This collaboration would allow organizations to make modifications to reform efforts that allow workers to continue their duties seamlessly following the transition and ensure that workers are still able to deliver optimal care to patients. Our study also makes evident the importance of appreciating how work is accomplished by different occupational groups to more fully understand how workers will respond to change. As organizational change continues to take hold throughout the healthcare system, administrators and scholars would benefit from a continued emphasis on the individual and group experiences and of the healthcare workers who are responsible for enacting these changes.
Supplemental Material
sj-pdf-1-wox-10.1177_0730888420919144 - Supplemental material for Occupational Heterogeneity in Health-Care Workers’ Misgivings About Organizational Change
Supplemental material, sj-pdf-1-wox-10.1177_0730888420919144 for Occupational Heterogeneity in Health-Care Workers’ Misgivings About Organizational Change by Jane S. VanHeuvelen and Matthew K. Grace in Work and Occupations
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project was supported by a Project Development Team within the Indiana Clinical and Translational Sciences Institute, Indiana University School of Medicine (NIH/NCRR Grant #TR000006).
Notes
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.