
Abstract
In recent years, many studies have focused on examining the relationship between democracy and health outcomes in developing nations. However, the overwhelming majority of this research utilizes direct-effect modeling approaches, assuming that increases in democracy are going to directly translate into improvements in well-being. Drawing on a sample of 136 less-developed nations, I first conduct a basic regression, where I find no significant impact of democracy on infant mortality. I then utilize structural equation modeling (SEM) to show significant indirect effects of democracy on infant deaths through public health spending. The results help place in context previous studies that have found inconsistent effects of democracy on health outcomes. The regression and SEM analyses demonstrate how erroneous findings can result from solely utilizing direct-effect approaches, which incorrectly treat key mediating mechanisms as competing predictors.
Introduction
While there have been great improvements in population health in the last 50 years, these improvements have not been experienced by people in all countries in the world in an equal manner (e.g., Austin and McKinney 2012). To help explain these health inequalities, researchers have turned their attention to the upstream social conditions or the structural factors of a society. In the last three decades, democracy has been identified as one of these structural factors that may explain health disparities in developing countries. A variety of health indicators have been used to assess the relationship between democracy and health, such as life expectancy or healthy life expectancy (Besley and Kudamatsu 2006; Franco, Álvarez-Dardet, and Ruiz 2004; Ghobarah, Huth, and Russett 2004a, 2004b; Lena and London 1993; Navarro et al. 2003; Reidpath and Allotey 2006), the mortality rate (Franco et al. 2004; Lake and Baum 2001; Li and Wen 2005; McGuire 2006; Navarro et al. 2003; Navia and Zweifel 2003; Safaei 2006; Zweifel and Navia 2000), and infant and child mortality (K.-Y. Chuang, Sung, Chang, and Chuang 2013; Y.-C. Chuang, Sung, Chao, et al. 2013; Houweling et al. 2005; London and Williams 1990; Moon and Dixon 1985; J. M. Shandra et al. 2004, 2005; Wickrama and Mulford 1996). While many of these studies yield results indicating that democracy positively impacts health, others question this link (R. Burroway 2016; R. A. Burroway 2011; Ross 2006; Weede 1993).
Despite increased attention to the role of democracy on health, the exact mechanisms by which democracy impacts health outcomes in developing nations are underspecified and underexplored in the current literature. For example, democratic societies are more likely to respond to citizens’ needs and concerns, including providing more social goods, such as health care, in comparison with autocratic societies (e.g., Besley and Kudamatsu 2006; Ruger 2005). Rather than considering the key indirect processes by which gains in democracy might improve health, empirical studies examining the relationship between democracy and health utilize direct-effect modeling approaches, such as ordinary least squares (OLS) regression (e.g., Besley and Kudamatsu 2006; Brady, Kaya, and Beckfield 2007; R. Burroway 2012; R. A. Burroway 2016; Franco et al. 2004; Gerring, Thacker, and Alfaro 2012; Gizelis 2009; Houweling et al. 2005; Iqbal 2006; Moon and Dixon 1985; Navia and Zweifel 2003; Safaei 2006; J. M. Shandra et al. 2004, 2005; Shandra et al. 2010; Wigley and Akkoyunlu-Wigley 2011; Wullert et al. 2016). This body of research demonstrates a mismatch between theory and empirical methods, and, thus, misses the opportunity to advance knowledge on the mechanisms involved in the upstream determinants of health, such as democracy.
In this study, I carefully scrutinize the relationship between democracy and health in developing nations by employing two analytic strategies: OLS regression, to examine the impacts of democracy using traditional approaches, and structural equation modeling (SEM), which allows for the explicit consideration of direct versus indirect effects through mediating social mechanisms. While other methods for uncovering indirect effects exist (e.g., Baron and Kenny 1986), SEMs are advantageous for a number of reasons, including the ability to estimate an entire system of linear equations at one time, to assess model fit at the overall and parameter level, and to construct latent variables from multiple observed variables. While a handful of recent studies has examined if democracy is a predictor of health outcomes in an SEM framework (Factor and Kang 2015; Klomp and De Haan 2009; Pillai and Gupta 2006, 2011; G.-Z. Wang 2004, 2007, 2014), more work needs to be done. What is lacking is a clear assessment of the indirect, direct, and total effects of democracy on health and a direct comparison of these results with those from an OLS regression. SEMs represent a more suitable analytic approach to utilize when the empirical model will include predictors and indicators of the social mechanisms through which they operate.
This study begins by explaining why infant mortality is a good indicator of population health and explores some of the key causes of infant deaths in developing nations. Next, I examine theories that explain how democracy should impact health, including a discussion of prior research that has empirically assessed this relationship cross-nationally. Following this, I identify limitations in prior studies and demonstrate how SEM can be leveraged to address weaknesses of existing modeling techniques. Then, I will discuss the analytic strategies and empirical models used, as well as the sample and variables. I conclude by presenting my findings and conclusion.
Infant Mortality: Cross-national Trends and Determinants
Despite considerable international effort, the problem of infant mortality remains vast, as each year approximately 4.5 million infants die before their first birthday (World Health Organization [WHO] 2017). The clinical leading causes of infant deaths globally are neonatal encephalopathy, infections, preterm birth complications, lower respiratory infections, and diarrheal diseases (National Institutes of Health [NIH] 2017). Rates of infant mortality vary dramatically between rich and poor countries, with the developing world accounting for 98 percent of infant deaths in 2015 (United Nations Inter-agency Group for Child Mortality Estimation 2017). Even within this group of developing countries, substantial variation exists, including regional variation, in rates of infant mortality. For instance, Belarus and Croatia had rates of 3.4 and 3.6, respectively, while the Central African Republic and Angola had rates of 91.5 and 96. Furthermore, two world regions, Sub-Saharan Africa and Southern Asia, account for more than three quarters of infant deaths annually (United Nations Inter-agency Group for Child Mortality Estimation 2017).
The infant mortality rate is often used in cross-national studies of democracy and health for a variety of reasons. First, as will be discussed below, democratic governments are generally thought to be responsive to the needs of the poor. Infants, children, and mothers often represent the poorest and most vulnerable segment of a society, with inequalities in their access to medicine and health supplies being an important dimension of vulnerability (United Nations Secretary-General 2012). Thus, the infant mortality rate gives us a good window into the health conditions of the poor (Welander, Lyttkens, and Nilsson 2015). In addition, studies have identified clean water, improved sanitation, increased education, and increased number of health workers as all being important ways to prevent infant mortality (R. A. Burroway 2016; C. L. Shandra, Shandra, and London 2011; Welander et al. 2015). I argue that these are indicators of the social mechanisms by which democracy is theorized to improve population health. Furthermore, data on infant deaths tend to be well-recorded and are comparable across countries, while many other health indicators are not (Ross 2006). Their wide availability allows for large samples of less-developed countries to be used, thus, answering a critique of many existing studies (Farag et al. 2013). Thus, this study will follow previous studies and utilize a country’s infant mortality rate to approximate the health of its population (e.g., K.-Y. Chuang, Sung, Chang, and Chuang 2013; Y.-C. Chuang, Sung, Chao, et al. 2013; Houweling et al. 2005; London and Williams 1990; Moon and Dixon 1985; J. M. Shandra et al. 2004, 2005; Wickrama and Mulford 1996).
Theorizing on Democracy and Health in Developing Countries
Researchers increasingly draw attention to political institutions as important macro-structural, upstream factors that impact cross-national inequalities in infant mortality and other health outcomes (e.g., R. A. Burroway 2016; London and Williams 1990; Moon and Dixon 1985; Ruger 2005; J. M. Shandra et al. 2004, 2005; Shen and Williamson 2001; Wigley and Akkoyunlu-Wigley 2011). While there may be several ways in which political institutions impact health, this paper will focus on the type of political system, or the extent of democracy in a country. Democracy is a system of government in which the people hold the real power, and its principles, such as free and fair elections, universal suffrage, regular elections, and respect for rights and civil liberties, are theorized to be amenable to better health outcomes. Governments in democratic societies are more likely to respond to citizens’ needs and concerns than autocratic or repressive governments (Besley and Kudamatsu 2006; Ruger 2005). Autocracies may not have incentives to invest in the human development of their people because this may mobilize citizens to push for greater rights and freedoms, in turn, jeopardizing the government’s hold on power (Ruger 2005). However, there are notable cases such as Cuba and Sri Lanka where real health gains have been made, as evidenced by some of the lowest levels of infant mortality in less-developed countries under low levels of democracy.
Theoretical arguments as to why democracy should lead to improvements in health include competitive elections, the motives of political leaders, and the presence of oppositional parties (Frey and Al-Roumi 1999). Competitive elections promote the accountability of political leaders to their population. Elections provide leaders with incentives to listen to and respond to marginalized groups whose needs are identified and then incorporated into plans of action. Often, some of the most important demands by the masses are increased provisions for public services, including health care (Ruger 2005). Elections also allow for restrictions on elite powers that if left unchecked could be negative for quality of life. Thus, to get elected, a candidate must be seen as responsive to the demands of the citizens who have as a priority improved health care (Besley and Kudamatsu 2006). The goals of the politicians themselves in democracies should also promote the distribution of goods and services, including health spending and basic resources for the population (Lake and Baum 2001).
Political participation, through individual and collection action, allows for people to organize and make their needs known to others and to their government leaders. These needs often surround those for a better quality of life including provisions for public services. More autocratic governments tend to be less responsive to the demands of the masses and more likely to neglect calls for greater gender equality and cut spending on social programs whereas democratic governments will respond to these needs. Increased institutional space in a democracy will allow people the opportunities to help themselves and others in terms of pushing for greater health provisions (Álvarez-Dardet and Franco-Giraldo 2006). Also, democracies invest more in the human capital of their citizens compared with non-democracies (Lake and Baum 2001). Democracies are likely to be responsive to public opinion, movements, and interest groups that are concerned with health-related issues than are non-democracies. In contrast, non-democratic governments are likely to be more responsive to other interests such as transnational corporate interests that may not be amenable to better health (J. M. Shandra et al. 2004). Oppositional parties can help define problems and propose how they can be solved and pressure the government to tend to the needs of the poor and vulnerable (Frey and Al-Roumi 1999). As such, oppositional parties represent another check on the political power of the elites. In other words, the opposition is merely another tool the majority can invoke to help keep those in power in check if they fail to adequately address their main concerns (Frey and Al-Roumi 1999).
Theoretical arguments as to how democracy should lead to improvements in health are important to consider, and it is clear that democracy in no way directly yields better health outcomes. Rather, democracy operates through indirect processes that are mediated by intervening social mechanisms, such as a government’s increased attention to health issues, better socio-health resources, and greater gender equality. These social mechanisms represent some of the proximate determinants of health outcomes, while political conditions such as democracy can be seen as foundational to these dynamics (Arah et al. 2005). Thus, empirical testing of a link between democracy and health would certainly benefit by including the mediating mechanisms by which the relationship operates. Ignoring important indirect relationships represents a mismatch between theory and empirical modeling. In addition, neglecting the indirect mechanisms could lead to misleading results and incorrect conclusions as to democracy’s impact on health.
Democracy and Health in Cross-national Research
Cross-national research on the effect of democracy on population health has proliferated since the late 1980s. Earlier works focused on country-level characteristics (London and Williams 1990; Moon and Dixon 1985; Navia and Zweifel 2003; Zweifel and Navia 2000), with later studies adding larger, structural factors such as indicators of dependency related to the world political economic system (London and Williams 1990; Wickrama and Mulford 1996). While the majority of studies find a positive relationship between democracy and population health, some studies challenge this finding (Burroway 2011; R. A. Burroway 2016; Ross 2006; Weede 1993). Others argue that the relationship between democracy and well-being is spurious, and both are consequences of economic development (Iqbal 2006) or dependency status (Wickrama and Mulford 1996). The link between democracy and health is further questioned in former Soviet states after their transition to democracy (Adeyi et al. 1997; Wejnert, Parrot, and Djumabaeva 2008). While democratization brought many positive changes to people’s lives, the transition to democracy in Poland and Kyrgyzstan had negative effects on gender politics and health policies for women and signaled a return to traditional roles of women, leading to more negative health outcomes (Wejnert et al. 2008:281).
So, while not all studies find that democracy leads to improved health and well-being, the bulk of empirical work focusing on this relationship in developing nations does demonstrate a positive link. However, testing the mechanisms by which a positive association occurs remains underexamined. While the mechanisms by which democracy is assumed to impact health are theorized to be indirect in nature, few studies have measured these mechanisms empirically. John M. Shandra et al. (2004, 2005); Kun-Yang Chuang, Sung, Chang, and Chuang (2013); and Ying-Chih Chuang, Sung, Chao, et al. (2013) begin to consider some of these processes by utilizing interaction effects on health involving democracy and other variables, such as public health resource indicators.
In addition to these works, a small handful of studies has employed SEM as the method of analysis to examine links between democracy and health (Factor and Kang 2015; Klomp and De Haan 2009; Pillai and Gupta 2006, 2011; G.-Z. Wang 2004, 2007, 2014). A major goal of these studies involves using latent variables to measure complex constructs, such as political stability or reproductive health. However, these studies are lacking an assessment of the direct, indirect, and total effects of democracy and other key exogenous variables (such as economic development) on the key health outcomes of interest. Thus, while a limited number of studies on democracy and health do utilize SEMs, they have not focused on carefully considering the role of indirect and direct effects and explicit comparison to direct-effect approaches.
Key Research Question
Theoretical insights point to the relevance of social mechanisms, such as a government spending on health, better socio-health resources, and greater gender equality as mediating the relationship between democracy and population health. Accordingly, the goal of this analysis is to empirically model these indirect pathways to assess if democracy does, indeed, have a significant indirect effect operating through these mechanisms. Furthermore, this study will compare results from this analysis with an analysis that utilizes OLS regression approaches to see if the results differ as to the importance of democracy to population health.
Analytic Strategy
In this analysis, I employ two quantitative methodologies: regression analysis and SEM using the same sample of data. To carry out the analyses, I rely on two statistical software packages: IBM SPSS Amos and Mplus. My research design utilizes a time-ordered outcome variable, where the outcome, infant mortality, is measured in time after the explanatory variables. This research design is useful in cross-sectional macro-comparative research to help adhere to conditions of causality, where causes must precede effects in time (e.g., Austin and McKinney 2012; R. Burroway 2010, 2012; J. M. Shandra et al. 2004, 2005; Shircliff and Shandra 2011). In this study, the infant mortality rate for 2015 is predicted by variables measured in 2010–2014, depending on their sequence in the path diagram, as I expect the influence of the explanatory variables on a country’s infant mortality rate to be fairly immediate.
OLS regression procedures only openly yield the direct effect of one variable on another, holding all other variables constant (Allison 1999). Studies using these procedures have several limitations such as not revealing the mechanisms by which one variable impacts another variable, failing to fully integrate existing theory to posit interconnections between variables in the model, and not always dealing with missing data in a way that yields consistent samples and comparable results with other studies.
SEMs can be viewed as a more general and flexible framework for modeling relationships between variables than multiple regression (e.g., Bollen 1989), and there are several benefits in using SEMs in this study compared with OLS regression methods. First, SEM analysis utilizes multiple outcome variables in a simultaneous equation, allowing for the specification of mediating effects. Thus, insights from theory as to how democracy impacts health can be included in an SEM instead of the more basic assessment from a regression model if democracy impacts health, holding other variables constant.
Second, in SEM framework total effects, comprised of direct and indirect effects, of a predictor on an outcome can be estimated, not just the direct effects as in OLS regression (Bollen 1989). This is vitally important in this study as our theory specifies that democracy impacts health indirectly, through the mediating social constructs. The use of SEM allows the empirical model to match the theory and avoid the problems of model underspecification or model misspecfication that occurs when OLS regression is used in this research. The consequence of these problems can range from a limited picture as to how democracy impacts health to drawing biased conclusions.
Third, SEM can include latent variables, such as socio-health resources, consisting of multiple indicators, including access to clean water, access to improved sanitation, the number of physicians per capita, and secondary schooling. These variables all contain measurement error, and using multiple indicators for a latent variable in an SEM permits measurement error to be controlled. This is a clear advantage of SEM over OLS regression in that results are easily biased if the errors are correlated with the outcome (J. Wang and Wang 2012).
Furthermore, SEMs deal with missing data in a superior manner in comparison with options available for OLS regression, such as pairwise deletion, listwise deletion, or multiple imputation. SEMs rely on direct maximum likelihood (ML) estimation, which allows all the models in this study to be estimated with exactly the same sample data, and, thus, the sample size is consistent throughout all analyses (Asparouhov and Muthén 2010). In addition, the assumptions about missing data are less stringent when robust ML estimators are utilized compared with the assumptions of missing data for OLS regression. With the robust ML estimator used in SEMs, the assumption is that data are missing at random (MAR), whereas in OLS regression, the assumption is that data are completely at random (MCAR), a harder condition to satisfy (J. Wang and Wang 2012). In addition to common measures of parameter fit used in traditional regression (e.g., estimated coefficients and R2), SEMs also permit models to be judged on overall model fit, which is estimated by how closely the variances/covariances implied by the model come to recreating the variances/covariances found in these data.
As is emphasized above, SEM is a superior empirical tool for teasing out the interconnections between variables and the direct and indirect effects of one variable on another. In other words, it is a proper technique for this study in that theory hypothesizes an indirect effect of democracy on health via mediating social mechanisms. These mediating relationships are omitted from OLS regression techniques because all variables are entered into the model as competing predictors, disregarding important information about the interrelationships between variables.
As with any method of analysis, there are important underlying assumptions about the use of SEM. Four main statistical assumptions underlie the SEM, including multivariate normality, MCAR data, a sufficiently large sample, and the correct model specification (Kaplan 2008). First, it is important that the observations come from a continuous and multivariate, normal population for the ML estimator to have estimates that are normally distributed, unbiased, and efficient. Second, the data should be MCAR although this assumption is relaxed when the robust ML estimator is utilized (J. Wang and Wang 2012). It is important to point out that the estimator utilized in SEM estimation procedures, the direct or full information ML estimator is seen as a superior way of dealing with missing data and one of the strengths of the SEM technique. Third, the positive asymptotic properties of the ML estimation procedure including consistency and efficiency are known when the sample size is relatively large. A fourth assumption of SEMs is that there are no model specification errors. This type of error occurs when relevant variables are omitted from the model. In this case, the errors and the exogenous variables in the model would be correlated, and this would lead to biased estimates (Kaplan 2008). In addition to the above assumptions, it is also necessary that an SEM be able to be theoretically and empirically identified. In the appendix, a summary of a series of robustness checks is given that explains the steps taken to meet these assumptions, and the procedures used to theoretically and empirically identify the SEM.
Sample
All less-developed nations for which data on infant deaths in 2015 and democracy in 2010 are available are included in the sample for analysis in this study. Due to the fact that 98 percent of infant deaths in 2015 occurred in developing countries, high-income nations are excluded from the analyses. Less-developed nations are defined as nations falling within the lower three quartiles of the World Bank income classification of nations, which is based on per capita gross domestic product (GDP; World Bank 2017). In sum, the sample consists of 136 less-developed nations, listed in Table 1 below, for which there are data for infant deaths and democracy.1,2
Countries Included in the Analysis (N = 136).

Variables Used in the Analysis
Dependent Variable
Infant mortality rate
In this study, I utilize as my indicator of population health a country’s infant mortality rate in 2015. The infant mortality rate is the number of children who die before their first birthday per 1,000 live births (World Bank 2017).
Independent Variables
Democracy
I measure the concept of democracy with Bollen’s Liberal Democracy Series I Indicator, a continuous variable with a range from 0 to 100 (Bollen 2009). 3 This is formed by taking a weighted combination of nine indicators representing the two dimensions of liberal democracy (political liberties and democratic rule) derived from expert ratings of the political landscape within each country and originating from four sources: Sussman at Freedom House, Gastil at Freedom House, the Arthur Banks Cross National Time Series (CNTS) databank, and a suffrage database (Paxton et al. 2003). In this study, I hypothesize that democracy measured in 2010 will impact population health measured as infant mortality indirectly, through social mechanisms such as public health spending and socio-health resources. It is also possible that democracy could operate through gender equality.
Gross Domestic Product per capita (GDPpc; logged)
To measure the concept of economic development, GDPpc is utilized. This is the total annual output of a country’s economy, per person, measured in current international dollars for 2010. This study utilizes the purchasing power parity measure of GDP per capita, which allows countries to be compared, not on a strict comparison of income, but rather by how much it costs to buy the same basket of goods, accounting for differences in cost of living. I utilized the measure of skewness and a histogram to determine that this variable was originally skewed. Thus, I performed a natural log transformation to correct for this skew, to better approximate linearity in the parameters, and reduce the influence of extreme outliers.
Public health expenditures (logged)
To measure a government’s commitment toward improving health, Public Health Expenditures are used. This measure represents the percent of GDP that is spent on health from government budgets, borrowed funds, grants from external sources, and social health insurance funds in 2012. Based on previous research and theory (e.g., Ross 2006; Tsai 2006), I predict that a country’s level of democracy is related to the amount of public health expenditures. In addition, I hypothesize that countries with higher public health spending will have increased socio-health resources (e.g., access to clean water, sanitation, doctors, and education). I also found that this variable was initially skewed. I, therefore, performed a natural log transformation to correct for this.
Secondary school enrollments
The secondary school enrollment variable represents a gross enrollment ratio that calculates the ratio of total enrollment, regardless of age, to the population age group that officially corresponds to secondary-level education. This variable is used as the latent variable’s scaling indicator meaning that the latent variable will be fixed to the units of this variable.
Number of physicians
Number of physicians captures the number of formally trained physicians, nurses, and midwives in a nation per 100,000 people (World Bank 2017). Properly trained medical personnel are necessary to properly treat and prevent illnesses and diseases, and, therefore, represent an important health resource measure included in the analysis.
Clean water
Clean water refers to the percentage of the population using an improved drinking water source. Improved drinking water sources include piped water located inside the user’s dwelling, plot, or yard, and other improved drinking water sources, such as public taps or standpipes, tube wells or boreholes, protected dug wells, protected springs, and rainwater collection.
Improved sanitation
Improved sanitation is the percent of a country’s population with access to improved sanitation facilities. I determined that none of these four variables was skewed, by use of the measure of skewness and a histogram.
The fertility rate
In this study, I utilize the fertility rate as an indicator of gender inequality. 4 Prior research demonstrates that fertility rates represent an important indicator of women’s status or female empowerment, where low fertility rates indicate higher levels of empowerment and gender equality (e.g., Wickrama and Lorenz 2002). The fertility rate is an estimate of the number of children an average woman would have if current age-specific fertility rates remained constant during her reproductive years. I hypothesize that countries characterized by gender inequalities, measured through high fertility rates, will have elevated rates of infant mortality. This variable is measured in 2014. 5
Results
The Results section is organized as follows. First, the descriptive statistics are introduced. Then the analysis is presented in three steps. The first step reports the results from the OLS regression analysis, and the second step reports the results from the traditional regression model with the latent variable of socio-health resources in the analysis. This step also allows for a direct comparison between models. The third step reports findings from an SEM that utilizes knowledge from existing literature, such as how democracy is theorized to impact health indirectly through mediating social mechanisms.
Descriptive Statistics
Descriptive statistics for the variables used in the analyses are presented in Table 2 including means, standard deviations, and a measure of skewness. In 2015, the average infant mortality rate was 31.4 per 1,000 live births for my sample of less-developed countries. The lowest and highest values of infant mortality in less-developed countries in 2015 range from 3.4 in Belarus, 3.6 in Croatia, and 4 in Cuba to 87.1 in Sierra Leone, 91.5 in the Central African Republic, and 96 in Angola.
Correlation Matrix and Univariate Statistics.
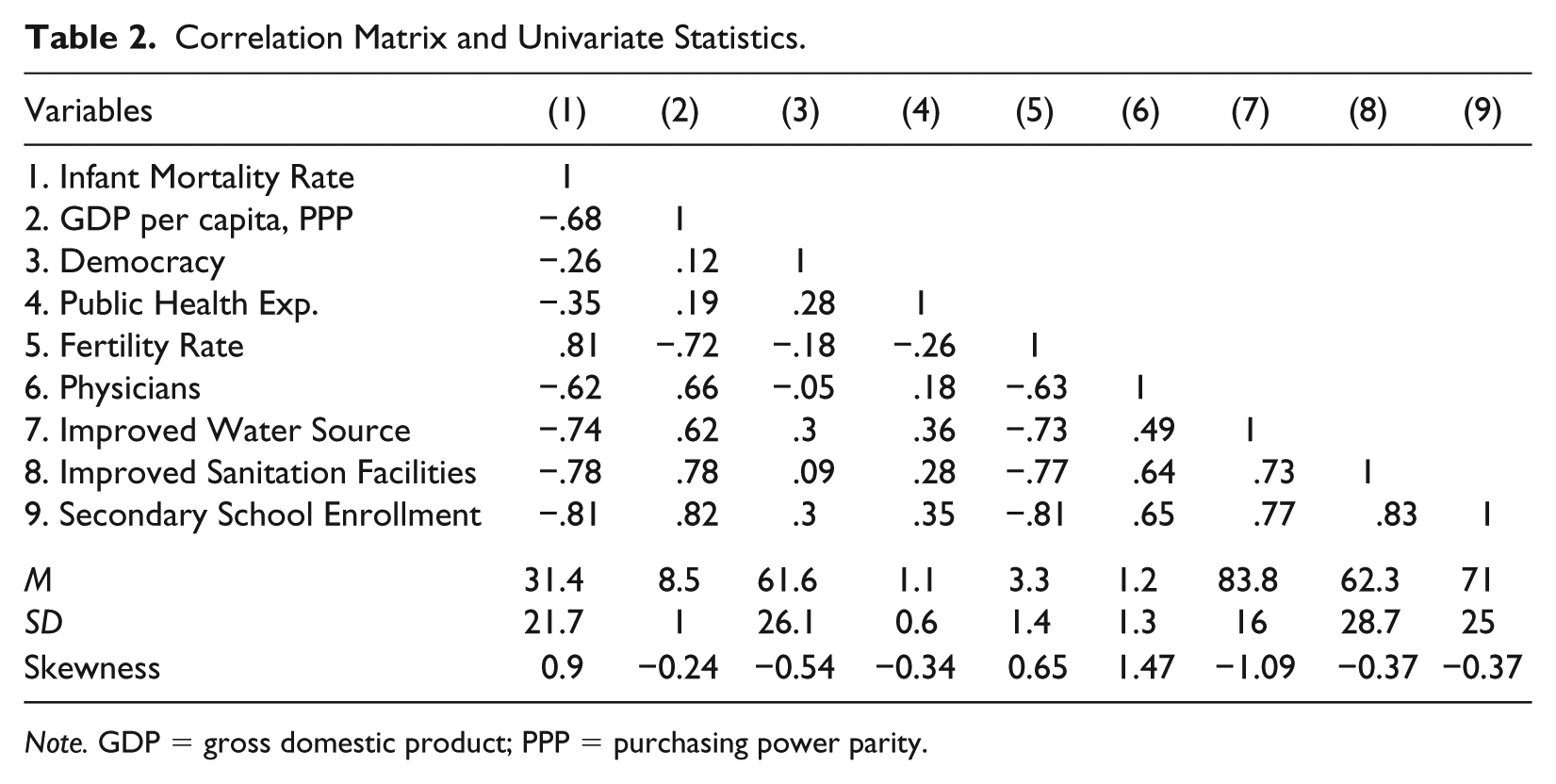
Note. GDP = gross domestic product; PPP = purchasing power parity.
OLS Regression
The first step of the analysis is the traditional regression model illustrated in Figure 1 and summarized in Model 1 of Table 3. The traditional regression results presented in Figure 1 are identical to those in Model 1 of Table 3; they are displayed in a path diagram framework in Figure 1 akin to how SEM results are presented to allow for clear comparisons across the models displayed in Figures 1 to 3.
Regression of LDCs for infant mortality in 2015 with standardized coefficients.
Regression Results for Infant Mortality Rate.

Note. Standard errors in parentheses; unstandardized coefficients in brackets. SEM = structural equation modeling; GDP = gross domestic product; PPP = purchasing power parity.
Standardized coefficients flagged †p < .10. *p < .05. **p < .01. ***p < .001, two-tailed tests.

Regression of LDCs with latent factor for health resources for infant mortality in 2015 with standardized coefficients.

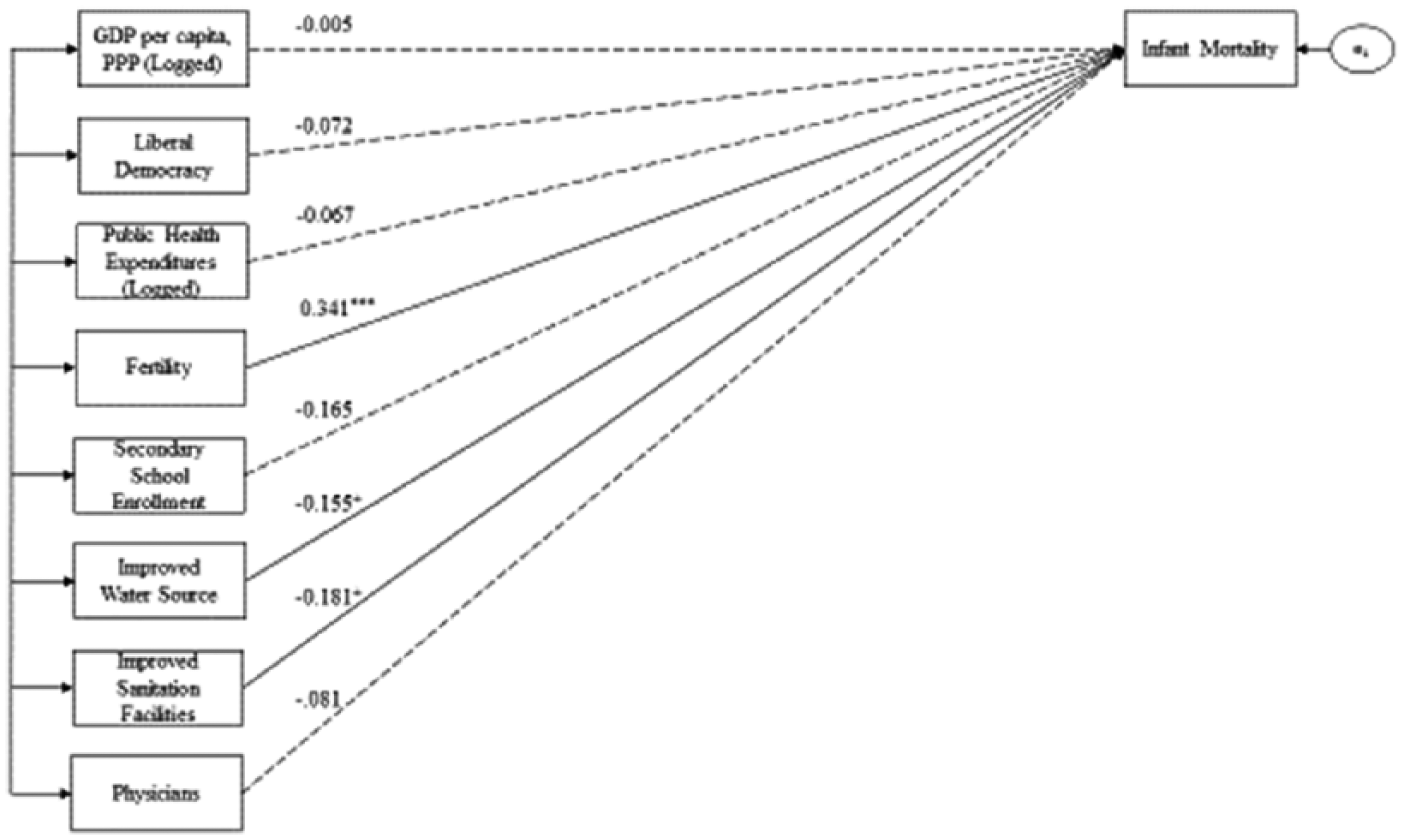
SEM of LDCs for infant mortality in 2015 with standardized coefficients.
A brief description of how to interpret path diagrams is needed before examining the results. Path diagrams are constituted by rectangles, ovals, single and double-headed arrows, and coefficients flagged for statistical significance. The rectangles represent variables that are measured in the dataset. As seen further in Figures 2 and 3, a variable represented by an oval is a latent variable, meaning that it is not directly measured in the dataset. The latent variable “socio-health resources” is not directly measured but is reflected in the four variables that are contained in rectangles (secondary school enrollment, improved water source, improved sanitation facilities, and physicians). In Figure 3, other smaller ovals in the path diagram (i.e., e1–e8) are errors in estimation and are also conceptualized as latent variables. Across Figures 1 to 3, single-headed arrows signify direct effects originating from the variable to the variable where the arrow terminates. The numerical values on these pathways represent standardized regression coefficients and can be interpreted just as in OLS regression. Solid lines represent paths that are statistically significant, and the dashed lines represent paths that are not statistically significant.
The traditional regression results presented in Figure 1 and Model 1 of Table 2 illustrate that only three of the variables in this analysis are statistically significant predictors of infant mortality: fertility rates at the .001 level and access to improved water and access to improved sanitation facilities at the .10 level. The signs for these variables are in the hypothesized direction, where higher levels of fertility are associated with higher levels of infant mortality, and higher levels of improved water and sanitation are associated with lower levels of infant mortality in developing nations. Several important nonsignificant effects should be noted; economic development, democracy, public health spending, and the other health resource indicators in the model are not significant predictors of infant mortality, despite the fact that all these variables are theorized to lead to improvements in infant mortality in prior research. The lack of significant effects is puzzling, and it is likely that nonsignificant results are due to not properly specifying the mediating mechanisms. 6
OLS Regression with Latent Variable
In Figure 2 and Model 2 of Table 2, I add a latent variable of socio-health resources using number of physicians, the percentage of the population with access to clean water, the percent of the population with access to improved sanitation, and secondary school enrollments. As described previously, an advantage of SEM involves the creation of latent concepts. A preliminary step in the empirical assessment of the SEM was to validate empirically whether socio-health resources represent a latent factor that can be appropriately estimated with secondary school enrollments, number of physicians, access to clean water, and access to improved sanitation. To test this, I initially construct a confirmatory factor analysis (CFA) and analyzed the overall and component measures of fit. The results indicate that schooling, physicians, clean water, and improved sanitation are all related and can be seen as indicators of an underlying latent variable, socio-health resources. 7
The results presented in Figure 2 and Model 2 of Table 3 demonstrate that the latent variable, socio-health resources, has a very large standardized coefficient and is highly significant in predicting infant mortality. This is completely consistent with previous health and development literature that posits that a lack of public health resources underlies infant deaths in developing nations. Similar to the prior model, GDP per capita, democracy, and public health expenditures are not significant predictors of infant mortality. The results also illustrate that there is one key inconsistency with the prior model: fertility rates now have no significant relationship to infant deaths.
Both of the regression models displayed in Figures 1 and 2 only model the direct effects of key variables on infant mortality. I now move to the next step of this analysis, modeling the SEM, to appropriately test for indirect or mediating relationships involving democracy as well as the other predictors. In the SEM, the theoretical linkages between democracy, economic development, government spending on health, socio-health resources, and population health are explicitly modeled.
SEM
The results of the SEM are organized as follows. First, the overall model fit of the SEM is discussed followed by a discussion of the parameter-level fit or interpretation of the path diagram coefficients. This is followed by a more careful assessment of the total, direct, and indirect effects in the SEM and the specific indirect effects. Finally, the results of the OLS regression models and the SEM are compared.
Overall model fit—SEM
Before examining the path coefficients of the SEM model, the overall model fit statistics are presented. SEMs are overidentified models, meaning that because the researchers explicitly specify information about the relationships between variables in the model, there is more information than is necessary to estimate the variance/covariance matrix allowing the calculation of overall model fit statistics. The better the model specified represents the variance/covariance matrix found in the data, the better the model fit. This allows them to be judged on overall model fit in a way that OLS regression models cannot as they are exactly identified models. The SEM displayed in Figure 3 has a χ2 of 29.153 with 19 degrees of freedom and a nonsignificant p value of .64. Thus, a nonsignificant χ2 test means that the null hypothesis, which is that the observed data fit this empirical model, cannot be rejected.
As is standard practice, additional indicators of fit are also reported (Schreiber et al. 2006). Some popular overall fit statistics that I report here are the Comparative Fit Index (CFI), the Tucker-Lewis Index (TLI), the Incremental Fit Index (IFI), Standardized Root Mean Square Residual (SRMR), and the Root Mean Square Error of Approximation (RMSEA). The fit statistics on these indicators range from 0 to 1. For the CFI, TLI, and IFI, a value closer to 1 is better, and for SRMR and RMSEA, a value closer to 0 is superior. Additional details of these indices can be found in SEM texts (e.g., Bollen 1989; Bollen and Curran 2006; J. Wang and Wang 2012). The values for the CFI, TLI, and IFI are .985, .972, .985—all well above the traditional recommended cutoffs of .90 (J. Wang and Wang 2012) and more stringent recommendations of .95 for acceptance as a good-fitting model (Schreiber et al. 2006). The SRMR is .04, which is well less than the cutoff of .08 for good fit (Hu and Bentler 1999). The RMSEA (.063) is just above the cutoff recommended for a good model fit (Hu and Bentler 1999) and within the fair range of other authors (J. Wang and Wang 2012). Thus, a consistent message that this is an overall good-fitting SEM is presented when examining all of the fit indicators.
SEM findings
Turning attention to the SEM results presented in Figure 3 (and Model 3 of Table 3 and Table 4), we find, most importantly, that democracy once again has no direct impact on infant mortality. Similarly, and also consistent with the models above, GDP per capita and public health spending have no direct impact on infant mortality rates. However, fertility rates and socio-health resources directly and significantly impact infant mortality rates, and socio-health resources are also significantly associated with fertility rates, therefore, having direct and indirect influences on infant mortality in less-developed nations. The results depicted in Figure 3 and Table 4 also suggest the importance of other indirect pathways; for example, public health spending is significantly and positively associated with socio-health resources, and public health spending itself is influenced by democracy and GDP per capita. Thus, the effect of democracy is mediated by public health expenditures.
Parameter-level Fit—Regression Estimates of Direct Pathways in for SEM displayed in Figure 3 and R2 for Endogenous Variables.
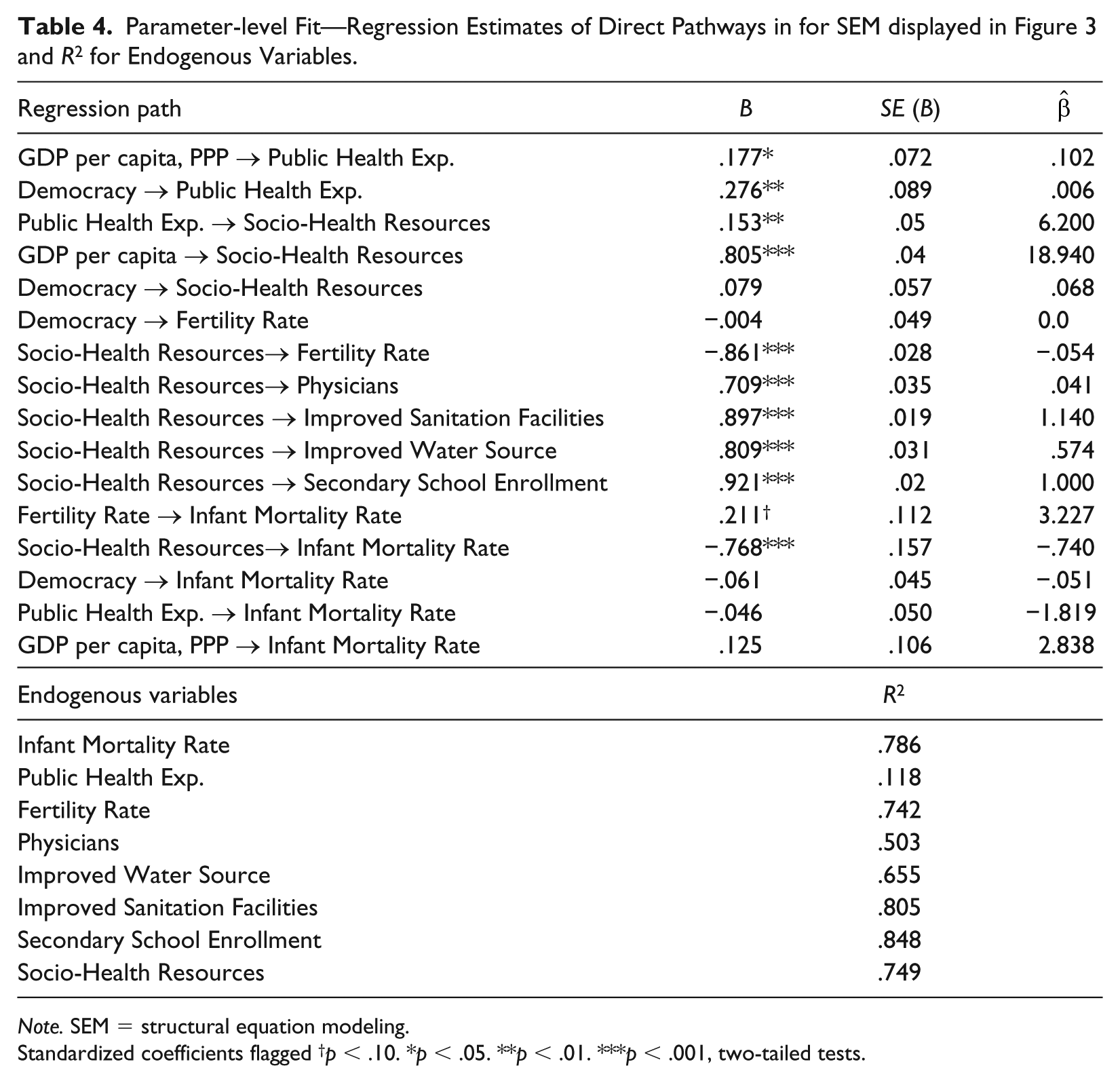
Note. SEM = structural equation modeling.
Standardized coefficients flagged †p < .10. *p < .05. **p < .01. ***p < .001, two-tailed tests.
To assess how well the model explains the variance in the endogenous variables, we can examine their individual R2 values (also in Table 4). For the main outcome of interest, the infant mortality rate, 78.6 percent of the variance is explained by the structural model indicating that the SEM is predicting this variable well. The latent variable of socio-health resources is also predicted well, with an R2 of .749. In addition, the fertility rate has an R2 of .742 and is only predicted directly by socio-health resources. The remaining R2s are those for the indicators of the latent variable, socio-health resources, and demonstrate that the latent variable explains a substantial amount of the variance in its indicators (between 50–85 percent).
Certainly, the SEM results suggest the indirect importance of democracy, as well as GDP per capita and public health spending, in influencing infant mortality rates in developing nations. Other mediating relationships are likely also to be important, as GDP per capita similarly significantly influences socio-health resources. To fully understand the relative importance of the indirect pathways, I next carefully decompose the indirect and direct effects.
Decomposing direct, indirect, and total effects
While informative, the above discussion of results from the path diagram is incomplete, as we are unable to directly compare the importance of indirect pathways. Table 5 displays the estimates for the direct, indirect, and total effects. Reporting the standardized coefficients allows for comparison. In addition, the specific indirect pathways are estimated individually. The specific indirect pathways are important to consider as some indirect pathways may be more important than others. To use an example from this analysis, public health expenditures can indirectly impact infant mortality in two ways; first, by impacting socio-health resources, then infant mortality; or second, by impacting socio-health resources, then the fertility rate, and then infant mortality. Thus, instead of lumping together all possible indirect pathways, we can isolate the effects from each potential indirect path to identify which ones are significant or most important. The statistically significant, specific indirect pathways have bold coefficients in Table 5.
Direct, Specific Indirect, Indirect, and Total Effects Predicting Infant Mortality.

Note. Standard errors in parentheses; unstandardized coefficients in brackets. Significant specific indirect effects in bold. SHR = socio-health resources.
Standardized coefficients flagged †p < .10. *p < .05. **p < .01. ***p < .001, two-tailed tests.
Focusing on the relationships involving democracy and infant mortality, the results presented in Table 5 demonstrate that there is only one significant specific indirect effect from democracy to infant mortality, and it is mediated by public health expenditures and socio-health resources. These results establish that democracy has an indirect effect on infant mortality, and also identify the specific mechanism of how this occurs. In other words, democracy significantly impacts infant mortality rates in developing nations by improving government public health spending, which then enhances provisions for socio-health resources, and then leads to reductions in infant mortality rates. The other potential paths involving democracy, public health spending, and fertility rates are not statistically significant.
The results presented in Table 5 also indicate a number of other important indirect pathways. For example, there are three specific indirect pathways from GDP to infant mortality that are statistically significant, including as GDP per capita is linked to improved socio-health resources, which then impact mortality rates or fertility rates, then infant mortality; and as higher GDP per capita is associated with increased public health spending, which in turn significantly impacts socio-health resources and infant mortality rates. Public health expenditures also have a significant indirect influence on infant mortality, which is mediated by socio-health resources, and the relationship between socio-health resources and infant mortality is also significantly mediated by fertility rates.
In carefully reviewing Table 5, it is important to emphasize that when comparing the overall size of the standardized regression coefficients for total effects on infant mortality, socio-health resources (physicians, water, sanitation, and schooling) have the largest overall influence on infant mortality rates (–.950). GDP per capita, or level of economic development, has the next largest impact on infant mortality rates in less-developed nations (–.673), which is accounted for entirely through specific indirect mechanisms. In contrast, the fertility rate (.211), public health expenditures (–.191), and democracy (–.189) overall have more modest impacts in infant mortality in developing countries.
Comparison of Traditional Regression Results and SEM Results
Concerning the central research question of this study, the results presented across Tables 4 and 5 demonstrate that democracy does have a statistically significant negative total effect on infant mortality. Democracy impacts infant mortality indirectly by increasing public health expenditures, which then promotes provisions for socio-health resources (secondary schooling, improved water, improved sanitation, and doctors), and, thus, improves health (infant mortality). These indirect paths are guided by theory and prior research, as described above, but are often incorrectly modeled in numerous studies using OLS regression methods. Thus, this study finds that it is easy to achieve flawed results when variables indicating mediating mechanisms are included as competing predictors.
In this study, I demonstrate these ideas by comparing results from a traditional OLS regression and an SEM analysis utilizing data on the same sample. The results drawn from the two traditional regression models suggest that democracy does not significantly impact infant mortality. Indeed, as seen in Table 3, one would arrive at the same conclusion about the nonsignificant impact of democracy on infant mortality if only the direct effects were examined in the SEM. However, when the indirect pathways, as described in the literature, are modeled properly, the importance of democracy is made evident. The important indirect effect of democracy is obscured if the focus is only on modeling the direct effects.
The initial use of direct-effect approaches also leads to erroneous conclusions surrounding the relevance of GDP per capita and public health expenditures in predicting infant mortality. With these two indicators as well, traditional regression approaches suggested a lack of importance, while the techniques of SEM reveal important indirect effects for these measures. In the SEM results presented in Table 5, the particularly large total indirect impact of GDP per capita on infant mortality is especially notable. Thus, this analysis demonstrates that the statistically significant total effects of all three of these variables (democracy, GDP per capita, and public health spending) would be missed if conclusions were made from only the direct-effects models.
Conclusion
Infant mortality remains a persistent problem in developing nations. Sadly, the majority of infant deaths are due to conditions that are preventable and treatable, such as pneumonia and diarrhea (WHO 2017). Many studies in recent years have examined cross-national variation in infant mortality, with a key focus on the role of democracy in mitigating unnecessary infant deaths in developing nations (e.g., K.-Y. Chuang, Sung, Chang, and Chuang 2013; Y.-C. Chuang, Sung, Chao, et al. 2013; J. M. Shandra et al. 2004, 2005). My findings demonstrate that democracy plays a role in reducing infant deaths, however, these effects are indirect in nature. Consistent with the theorization, important mechanisms, such as a government’s increased attention to health issues and better socio-health resources, mediate the relationship between democracy and infant mortality. By utilizing both traditional direct-effects approaches and SEM models that allow for the specification of indirect and direct effects, I am able to demonstrate the weaknesses in relying solely on traditional regression models. I illustrate that including mediating variables as competing predictors in OLS regression models obscures the true impact of larger, underlying predictors, such as democracy and level of economic development.
Indeed, the indirect effects of democracy on health demonstrated in the SEM analysis are not unique to democracy, but also characterize the relationships involving GDP per capita and public health expenditures. Neither democracy, GDP per capita, nor public health expenditures had a significant impact on infant mortality in the direct-effect models. Thus, these factors do not automatically equate to better health. Instead, increased political freedoms, economic development, and health spending only lead to better health outcomes when they are channeled in an appropriate manner to provisions for health resources, including access to physicians, clean water, improved sanitation, and schooling. These more macro-structural features matter because they lay the groundwork for basic resources to be provided to populations.
This analysis speaks to previous studies that have found inconsistent effects of democracy on health outcomes. When mediating variables are placed in regression models and the interlinkages or indirect relationships between these mechanisms are not specified, then the variables are incorrectly considered as competing predictors. As demonstrated here, this can result in misleading or erroneous findings. It is important to note that failing to specify important mediating relationships is not a problem unique to this particular vein of research or comparative studies of health outcomes. Instead, this is a potential problem whenever regression-based methods include in the same direct-effects model variables that mediate the effect of others.
One aspect that was not examined in this analysis is the debate over whether democracy has a significant long-term effect on health, or rather if the relationship is relatively contemporaneous (see Gerring et al. 2012). The present study utilizes a five-year lag between democracy and infant mortality. Certainly, the effects of time are an avenue for future research. However, regardless of whether or not the effect of democracy is relatively quick or long term in nature, the way in which it would impact health is arguably the same. Governments with democratic regimes are likely to impact health through the social mechanisms identified in this study, namely, a government’s increased attention to health issues and providing expenditures to enhance basic health resources.
Future research should also explore the potential mechanisms through which democracy improves other types of health outcomes, such as life expectancy, HIV prevalence, and other disease rates. It is possible that democracy impacts different types of health outcomes through different mechanisms, and it should not be assumed that the intervening mechanisms for all health outcomes are the same. For instance, for some diseases, such as HIV, the presence of international nongovernmental organizations (INGO) or other external health resources (such as provisions for antiretroviral drugs) may act as mediating factors to consider. Previous studies such as Austin et al. (2016) have shown that public health spending ameliorated tuberculosis but private health spending had no effect, thus, demonstrating that each health outcome is potentially driven by different mechanisms and that all types of health expenditures are not equal.
Thus, in summary, this study has two main contributions. First, the findings reveal an indirect effect of democracy on health, by government spending on health, and successively provisions for socio-health resources. This is consistent with the bulk of theories on democracy and health, despite that appropriately accounting for these indirect mechanisms has largely been untested in the current empirical research. Despite having significant indirect effects, the actual impact on infant mortality is quite small in comparison with other indicators, such as health resources. Second, this study illustrates that relying solely on direct effects regression-based methods and leaving out the interrelations between democracy and its mediators could lead to incorrect conclusions on the relationship between democracy and health. Studies that do not model these interrelationships are underspecified models at best and likely misspecified. This finding was also demonstrated with other indicators, including GDP per capita and public health expenditures.
Based on the evidence presented here, the pursuit of democracy and economic development cannot by themselves lead to improved health outcomes for infants in developing nations. These improvements must be accompanied by targeted policies and practices that seek to improve the public health spending and resources of a country. Sri Lanka represents a relevant example as it has rather low levels of democracy (58.5 out of 100) and economic development (US$8,389 GDP per capita). However, the level of infant mortality is a modest 8.4 per 1,000 births. Thus, impressive gains in infant health were made because of effort placed on improving access to basic resources, such as clean water and education (Medcalf et al. 2015). Health benefits are most directly and intensely realized through provisions for basic health services. It is not enough that countries rank high on traditional development indicators such as democracy or economic growth to have good health outcomes. The United States ranked 44th in the world in infant mortality in 2015 (at 5.6), and other declines and severe inequalities in population health are overwhelmingly evident. This study serves as a reminder that it takes concerted efforts on the part of governments not just to make sure that money is being spent on health services, but that it is being channeled to those that need it most and to the most essential elements of care.
Footnotes
Appendix
Authors’ Note
Mark D. Noble is now affiliated with Susquehanna University.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.