
Abstract
Synthesizing the theory of fundamental causes in the health literature with the stratification research on transitional economies, this paper investigates how the multidimensional socioeconomic status (SES), especially education and communist party membership, is associated with three self-rated health outcomes in urban China. Using data from the 2013 Chinese General Social Survey, we find that party membership is associated with better self-rated health, higher health-related quality of life and work, and lower levels of self-rated depression, whereas the effect of education is somewhat more elusive than it usually is in Western societies. Our findings suggest that the effects of socioeconomic indicators are better understood by being contextualized in a sociopolitical environment. It is also fruitful to include both global (education, income, employment status, and subjective SES) and local measures of SES (party membership and housing ownership) in exploring their associations with health in the world’s largest transitional society.
Introduction
No pattern in health research has elicited more enduring attention among medical sociologists and social epidemiologists than the association between socioeconomic status (SES) and health (Adler et al. 1994, Braveman et al. 2010; Link and Phelan 1995; M. G. Marmot, Shipley, and Rose 1984; Michael Marmot and Allen 2014; Phelan, Link, and Tehranifar 2010). Spanning more than the past three decades, scholarly works have corroborated not only the prevalence of such an association across different ethnoracial groups and distinct contextual environments, but also its temporal reproducibility for a wide array of health outcomes. Concurrently, health scholars have highlighted the relevance of institutional variables, such as sociopolitical characteristics and organizational structures that vary across societies, to health disparities in international contexts (Beckfield and Krieger 2009; Beckfield, Olafsdottir, and Sosnaud 2013; Krieger 1994, 2008). Yet, few studies have systematically examined how the multidimensional SES, contextualized in a dynamic and complex institutional environment, is associated with health outcomes in a non-Western transitional society such as China.
As the most populous country in the world, China has undergone momentous changes in multiple domains since 1978, making itself the fastest growing economy with a size only second to the United States. Such profound social and economic transformations have received extensive attention and given rise to an invigorating scholarly debate on the changing patterns of social inequalities during the market transition (Nee 1989, 1996; Nee and Cao 1999; Xie and Hannum 1996; Zhao and Zhou 2017; Zhou 2000, 2004). Most studies engaged in this debate, however, have typically focused on tangible socioeconomic rewards, including income and housing (Bian 2002), while devoting much less attention to other important life outcomes, such as health and quality of life (for exceptions, see Shu and Zhu 2009, for an example). As China has undergone a substantial increase in living standards, physical and mental health issues (e.g., severe acute respiratory syndrome [SARS] in 2003) have also emerged as major public and scholarly concerns. While socialist China provided basic and relatively equitable health care to its citizens in the past, recent socioeconomic reforms and marketization have purportedly increased health disparities in significant ways (Hsiao 1995; Yip and Hsiao 2008, 2014). With this backdrop of probably the largest-scale social experiment ever conducted in the human history, many health scholars have speculated, and yet few have empirically investigated how SES indicators, especially those pertaining to China’s market transition, are associated with health (for exceptions, see Soyoung and Mustillo 2017; Yu 2008; Yu and Chiu 2016).
To address this research gap, our paper aims to advance the emerging literature and make important theoretical as well as empirical contributions. Theoretically, we integrate the theory of fundamental causes in health literature with the stratification research about transitional economies to analyze how the multidimensional SES is associated with health (Link and Phelan 1995; Nee 1989; Phelan et al. 2010; Zhou 2000). We move beyond the widely used global measures of SES, such as education, family income, and subjective SES, to further include local measures (Soyoung and Mustillo 2017), such as party membership and housing ownership. Although both sets of SES indicators are interconnected, they can also play independent roles in China’s multilayered stratification system and affect health accordingly. Of all, we particularly highlight communist party membership and education because their roles in configuring social inequalities are often viewed as the touchstone of the market transition swinging between a state-dominant and a market-oriented system (Nee 1996; Zhou 2004).
Empirically, our article furnishes new evidence on health disparities in urban China. While most published works used data collected in the 1990s or at the beginning of the twenty-first century, we use data from the 2013 Chinese General Social Survey (CGSS), the most recent CGSS data that collect rich health information, to appraise health inequality in urban China. As China has undergone major state policy changes under the Hu-Wen reign from 2002 to 2012, this study can update our knowledge on the patterns of health disparities after the so-called “golden decade” of economic growth in China. Instead of focusing on a single health outcome, we investigate self-rated health (SRH), health-related quality (HRQ) of life and work, and self-rated depression (SRD) to provide a broad view of health profiles of urban residents in China. We also note that while it is valuable to examine both urban and rural China at the same time, we are wary of the great divide between the two, which in and of itself warrants careful examination; an indiscrete attempt to incorporate both could easily lead to serious confounding as well as endogeneity issues (cf. Whyte and Sun 2010). Therefore, in this paper, we devote our attention to urban China, the center stage of socioeconomic reform in the twenty-first century, to provide more focused discussions about health disparities.
Contextual and Theoretical Background
SES and Health in Western Societies
A spate of studies have documented a positive association between SES and health in the Western industrialized countries; that is, for a tangible amount of increase in major indicators of SES, such as education or income, we would expect a corresponding improvement in health outcomes (Adler et al. 1994; Braveman et al. 2010; Link and Phelan 1995; M. G. Marmot et al. 1984; Michael Marmot and Allen 2014; Phelan et al. 2010). Ostensibly straightforward, the mechanisms linking SES to health are multifaceted and can vary with specific measures. As the conventional wisdom has it, education, income, and occupation are primary indicators of SES (Elo 2009) and are therefore among the fundamental causes of disease, because these three variables usually involve the possession of, access to, and mobilization as well as utilization of resources (Link and Phelan 1995).
Notwithstanding considerable empirical evidence, the classical theory of fundamental causes has not gone unchallenged or un-reconstrued, even by those who initially submitted the theory (Colgrove 2002; Lutfey and Freese 2005; Phelan et al. 2010). For example, Jo C. Phelan et al. (2010) argue that risk factors or fundamental causes have to be contextualized for a sophisticated understanding of their effects on health, especially when investigating countries outside of the Western hemisphere where the associative mechanisms might operate differently under distinct sociopolitical environments. There may also exist some countervailing mechanisms with which people may utilize resources to pursue life goals compromising health (Lutfey and Freese 2005). For example, some risk factors, such as overweight, tobacco usage, and binge-drinking, are often idolized and indicative of affluence and high social status in some non-Western cultures, such as China (Hao et al. 1998; Shuangshuang Li, Ma, and Xi 2016; Tang et al. 2013; World Health Organization 2017).
In addition, the set of SES indicators that are commonly used in the Western world might not cover the full spectrum or even important types of resources in developing countries. Income, education, and occupation, for example, have shown to be associated with health across a wide array of distinct cultural contexts, ethnoracial groups, and sociopolitical environments (Beckfield and Krieger 2009; Beckfield, Olafsdottir, and Sosnaud 2013). Thus, they could be viewed as global measures of SES in health research. But some research also notes that even a global measure of SES may play a different role in affecting health outcomes across various local contexts (cf. L. Song 2015). As some health scholars have further argued, there may exist important SES factors, such as communist party membership and housing ownership in China, that also involve the utilization of resources for disease prevention and health enhancement, but bear distinct characteristics of local contextual environments. These can be conceptualized as local measures of SES (Soyoung and Mustillo 2017).
Moreover, the intermittent but enduring debate about the social causation and health selection hypotheses as two competing arguments about the relationship between SES and health may cast further doubt about the validity of the theory of fundamental causes. The health selection hypothesis emphasizes that genetic predisposition to early health disadvantages may lead to low SES, which in turn can exacerbate the adverse health conditions. Although some recent research further suggests the few contingencies under which the health selection hypothesis dictates the association between SES and health (Hoffmann, Kröger, and Pakpahan 2018; Kröger, Pakpahan, and Hoffmann 2015), the overwhelming majority of literature, especially those in sociology, has submitted to the social causation explanation subsumed in the general theory of fundamental causes (Dohrenwend et al. 1992; Warren 2009).
Overall, while the main indicators of one’s position in Western society have usually been reduced to education, income, and occupation, such a simplified operationalization to measure SES may have to be adapted in China’s distinct institutional context. Following the Weberian approach to social stratification, this paper aims to examine the effects of the multidimensional SES, broadly defined, by incorporating not only economic and social resources, but also political capital (Bollen, Glanville, and Stecklov 2001). In particular, as the Chinese Communist Party (CCP) continues to wield its political power over all realms of social life, it has become almost imperative to include party membership in most social stratification research, including studies on health disparities, in the Chinese context.
Market Transition, SES, and Health in Urban China
Since China launched its “reform and open door” policy in 1978, dramatic changes have transpired in economic, political, and other social realms, including health and health care (Bian 2002; P. Liu, Wang, and Zhang 2008; Nee 1996; Xie and Hannum 1996; Yip and Hsiao 2008; Zhou 2000, 2004). As the size of the economy and individual wealth accumulation in China has grown at a staggeringly high rate, so has its level of social inequality. Since the reform, China’s gross domestic product (GDP) per capita has grown by almost 50 folds, from $156 in 1978 to $8,123 in 2016 (The World Bank 2018), and the size of its economy now is only second to that of the United States. Meanwhile, social inequality has increased tremendously over the same period of time, despite some different estimates of the recent level of income disparity (e.g., Shi Li 2016; Shi Li and Sicular 2014; Molero-Simarro 2017; Xie and Zhou 2014).
Unlike Russia or other former socialist countries in East Europe that implemented the “shock therapy” or “big bang” package of policies, China has adopted an incremental approach, allowing the private sector to grow rapidly and pushing state-owned enterprises (SOEs) and the whole economy to gradually “grow out of plan” in the early stage of market transition (Naughton 1995). Following a series of organizational and labor reforms since the mid-1990s (Zhao and Zhou 2017), marketization has accelerated, especially during the Hu-Wen’s 10-year reign from 2002 to 2012 (National Bureau of Statistics of China 2012). Over this decade, employees of private firms and individual business increased to 200 million by 2012, two and a half times the level of 2002 (Lardy 2014:70).
Under the state socialist regime, education and party membership have been the two primary credentials to achieve high occupational statuses and join the sociopolitical elites, albeit along different paths (Li and Walder 2001; Walder, Li, and Treiman 2000). Inspired by Nee’s market transition theory, scholarship in sociology has engaged in an invigorating debate about the general trend of this transition and paid particular attention to the returns to human and political capital, the key measures of which include education and party membership, respectively (Bian and Logan 1996; Nee 1996; Szelenyi and Kostello 1996; Walder 1996; Wu and Treiman 2004; Zhou 2000). According to Victor Nee (1989, 1996), along with the market advancement, the effects of human capital will rise and the influence of political capital should wane over time. Nee’s market transition theory, however, has received both compliments and criticisms. For example, Yanjie Bian and John R. Logan (1996) and Xueguang Zhou (2000) argue that political capital still plays an important role in reproducing social inequality during the market transition. Because human capital (e.g., education) and political capital (e.g., party membership) are the lynchpins of this scholarly debate and crystallize the socioeconomic dynamics and changes along with the market transition, we anchor most of our discussions on education and party membership in this study.
Moreover, due in large part to the fragmented market, the effects of other SES indicators in China could be more nuanced than what we would usually observe in a Western market economy (Zhao 2012). For example, in a developed and more integrated Western market economy, income is the foremost indicator of one’s economic resources, and thus it is the most widely used summary indicator of economic well-being to examine health inequality (Mirowsky and Ross 2003). In contrast, after dismantling the socialist redistributive system in urban China in the mid-1990s, the Chinese state has adopted different strategies to develop markets in various arenas in accordance with its sociopolitical agenda. As a result, what have emerged are “fragmented markets,” characterized by heterogeneous market conditions and distinct allocation mechanisms across domains (Walder, Luo, and Wang 2013; Zhao and Zhou 2017). For example, the labor market emerged after the state privatized SOEs and implemented the radical labor reform, which drastically redefined the employment relationship and led to prevalent unemployment. The housing market was created after the state transformed public housing into private property, and the social welfare domain was characterized by the dominance of an underdeveloped market after a modest state reform and a strong socialist legacy (Zhao and Zhou 2017). Accordingly, to better gauge an individual’s economic conditions embedded in China’s fragmented market environments, we need to consider multiple indicators, such as income, employment status, health insurance, and housing, which are often subject to different allocation mechanisms and exert independent effects on individuals’ socioeconomic well-being (Zhao 2012).
Party Membership and Health
In this study, we focus on the CCP membership as a key indicator of political capital under the umbrella of multidimensional SES. Usually granted on the basis of merit and political loyalty, party membership had been a social status strenuously sought after by many under the socialist regime (Dickson and Rost 2000; Guo 2005; Walder 1995). Studies have shown that under the reign of the party-state, communist party members have benefited considerably in social and spatial mobility, career advancement, economic compensation, and housing (Walder 1995; Wu and Treiman 2004; Zhao and Zhou 2017; Zhou 2004). Despite an overall slackened grip on the market and the redistributive system in recent years, the party-state continues to play a pivotal role in dispensing benefits and resources as well as shaping an emerging free market (Bian and Logan 1996; Bian, Shu, and Logan 2001; Dickson 2007). As the market looms huge and becomes increasingly important in the socioeconomic life, it is important to revisit how political capital would operate to affect various life outcomes, in this case, health.
To broaden its political base in the market economy, in 2001, the CCP allowed entrepreneurs from the private sectors to join the party for the first time since it took over power in 1949 (Dickson 2007). Coupled with several other moves toward the retrenchment of an overly liberal market, this would have clear ramifications for how party membership has been associated with a variety of life outcomes, including health. When the political and economic elites coalesce to game the system, party membership can be valuable not only to join the political elite, but also to receive recognition and gain better market opportunities in the nonstate arena. In addition to these perceivable returns, party membership proffers intangible but important health-related resources, such as a sense of belonging and security, high sociopolitical prestige, and expansive and powerful social network (Li and Walder 2001; Walder 1995; Walder et al. 2000; Yu and Chiu 2016). Following the premises of the theory of fundamental causes of disease and further considering China’s distinct institutional context, we conceptualize party membership as an important indicator of SES. Thus, we would expect party membership to be positively associated with good health outcomes. 1
Education and Health
Education is often considered the most important SES indicator for predicting health outcomes. Education embodies a wide array of resources to be utilized for disease prevention and health enhancement (Beckfield et al. 2013; Link and Phelan 1995; Phelan et al. 2010). First and foremost, it is a classical measure of human capital that helps obtain other forms of capital, including economic and social resources, to shield individuals from health-damaging environment and factors; education also harvests “learned effectiveness” in accumulating information, knowledge, and skills enabling individuals to “coalesce health producing behaviors into a coherent lifestyle”; moreover, education avails oneself of cognitive ability in identifying health-relevant information and statistics and critically analyzing them, and it also represents or shapes noncognitive characters, such as discipline, motivation, and perseverance (Elo 2009:558–59; Mirowsky and Ross 2003). As the effects of education on health have been long recognized for a large variety of health outcomes across a wide range of social contexts, one would expect education to play a significant role in predicting health in China.
Moreover, as contended by Nee (1989), when the market makes further inroads, returns to human capital, usually measured by education, should increase. Through this process, various forms of capital and resources may gravitate toward those with high levels of education, thus making education an important predictor of health disparities. Therefore, we should expect to see a clear education-health gradient as observed in a typical Western market economy.
Under China’s distinct institutional context characterized by strong state power, however, state policy changes can drastically reconfigure how education is associated with many important life outcomes (Zhou 2004; Zhou and Hou 1999), thus introducing some countervailing mechanisms. For example, intellectuals and those with higher education had endured several major waves of political campaigns and repression under the state socialist China during 1955–1976. Such targeted persecutions are expected to have particularly adverse effects on the health of the well-educated, reducing or even reversing the positive effects of education on health (Chung 2011; Walder 2015; Zhou and Hou 1999). Toward the end of the 1990s, the powerful party-state made another dramatic policy change to drastically expand its higher education. Within a few years, the total enrolled undergraduate student body had quadrupled, rising from 3.41 million in 1998 to 13.33 million in 2004 (Wan 2006); this number multiplied again by 2.6 times by 2013, reaching a record high of 34.6 million (National Educational Development Statistical Bulletin 2013). Such a “great leap” in college enrollment, coupled with partial marketization in higher education, has led to soaring tuition, deterioration in student quality, and oversupply of college graduates in the labor market, all of which could possibly dampen the positive effects of higher education on individual health in various ways (Li et al. 2011; Zhong 2011).
Other Measures of SES
In China’s fragmented markets, income, employment status, housing, and subjective SES are also important indicators of SES (Zhao 2012; Zhao and Zhou 2017). These SES indicators, both global and local, objective and subjective, may have special implications for health disparities in China’s distinct sociopolitical environment. They capture multiple dimensions of socioeconomic conditions and can be associated with various health outcomes in and of themselves.
As a direct measure of financial resources, income is viewed as more important for the prognosis of a disease, especially later in life, as the treatment of disease, especially chronic ones in the developed world, requires a stable stream of financial support (Adler et al. 1994; Evans, Wolfe, and Adler 2012). In China, the rising income inequality over the past few decades may have increased health disparities. Nonetheless, the overall rising living standard, the improvement of the quality of care, and the involvement of other local sources of SES, such as housing ownership, may suppress the effects of income to some extent (Zhao and Ge 2014). After dismantling the work-unit system as the institutional and organizational foundation of the socialist health care system in the mid-1990s, the burden of health care expenditure had increasingly shifted to individuals since 1978 and peaked around 2000, and this trend was somewhat stalled and even reversed after that as the state made a greater investment in improving the health care system and health insurance coverage (Liu, Vortherms, and Hong 2017). But overall, income could become increasingly important to purchase health services and thus have important effects on personal health.
Employment status is another important indicator of SES in contemporary China. Under the socialist regime, the urban labor relationship was characterized by the “iron rice bowl,” referring to permanent employment in the state sector. Since the radical labor reform and massive scale of privatization of SOEs in the mid-1990s, however, there have been waves of layoffs and a sharp increase in the unemployment rate during 1995–2002 in urban China. While the unemployment rate declined slightly after 2002, it remained relatively high with an average of 9.5 percent from 2002 to 2009 (Feng, Hu, and Moffitt 2017). Moreover, as a part of the socialist legacy, housing (e.g., via Housing Purchase Fund), social benefits, and health insurance are still closely attached to employment organizations (Zhao and Zhou 2017). As unemployment may have severe economic, financial, and psychological consequences under the precarious market environment, we would expect that employment status can have a considerable impact on health.
Unlike in the developed market economies where income generally determines living conditions, housing in urban China can be subject to different allocation mechanism and it is also indicative of one’s SES (Song and Xie 2014; Walder and He 2014; Zhao and Ge 2014). As China terminated the welfare housing distribution system and opted for privatization in the late 1990s, a booming housing market has emerged and the housing price skyrocketed. Housing has become the most valuable asset for many urbanites, and housing inequality is estimated to be even higher than income inequality in China (Zhao and Ge 2014). While urban residents often obtained ownership of their primary home through the housing privatization process via the help of their state employers in the late 1990s, some acquired second or even more housing properties from the market or other venues. Over time, housing ownership has become a prominent marker of one’s economic well-being and socioeconomic security, and it is closely related to dating patterns, family formation, and quality of life in urban China. In a sense, housing is not only a shelter for comfort, but also an important marker of SES in urban China.
In addition to these objective measures of SES, recent scholarship has indicated that subjective SES plays a key role in predicting various health outcomes (Demakakos et al. 2008; Singh-Manoux, Adler, and Marmot 2003). Such an association can be disentangled through multiple pathways. First, subjective SES might be associated with health through relative deprivation, the perception that one’s resources and possession are less than what is expected, which in turn affects emotional and physical well-being. Subject SES is also believed to operate as a global measure of the cognitive average of major SES indicators. In tandem with relative deprivation, subjective SES can affect health via the stress-response system, within which a sense of inferiority, insecurity, and lack of control can trigger a series of well-orchestrated physiological changes, leading to an overworked body (Nobles, Weintraub, and Adler 2013; Operario, Adler, and Williams 2004). Mental and physical deviations emerge as a result.
Due to fast economic changes, multifaceted stratification processes, and the still-emerging social hierarchy, SES and its objective measures can be elusive to the extent that even multiple indicators might not suffice to cover the full spectrum and all varieties. Therefore, subjective SES can play a critical role in predicting health outcomes in China. While a caveat is in order that the association between subjective SES and health might be recursive or confounded by some temperamental trait (Nobles et al. 2013), research using experimental design and other methodological approaches has shown otherwise (Kraus, Adler, and Chen 2013; Wolff et al. 2010). Because of the unsettled nature of this issue, it is advisable that our findings about subjective SES be read with caution.
Data and Methods
Data
We drew data from the 2013 CGSS, the only recent release of the CGSS data with rich individual health information, to appraise our theoretical predictions. The 2013 CGSS used a stratified sampling design to collect data from individuals residing in both urban and rural areas of 100 city districts and counties; three municipalities directly administered by the central government, including Beijing, Shanghai, and Tianjin; and other two large metropolitan areas, Guangzhou and Shenzhen. To avoid confounding issues arising from the great urban-rural divide affecting multiple areas of life simultaneously, we focused only on the urban subsample of the survey data. We further restricted our sample to those who were above 25-year old because that is about the age when people start to have a roughly stable level of education and income.
Dependent Variables
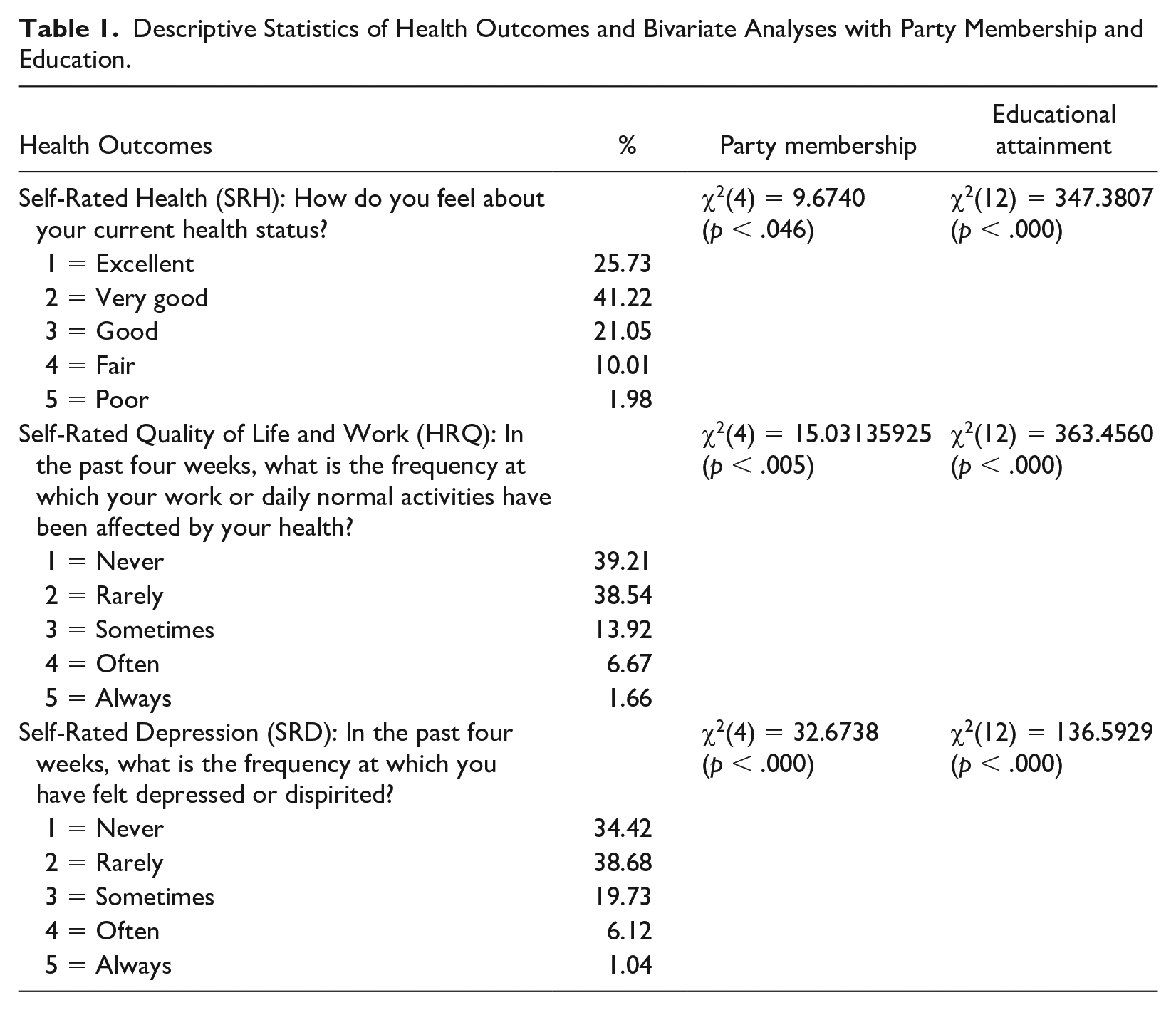
In our analysis, we used three ordinal measures of health outcomes, including SRH, HRQ of life and work, and SRD. SRH is a widely used general assessment of one’s health status, and it has been validated as a powerful predictor of mortality and morbidity in a wide array of countries and across various cultural and sociopolitical environments (Idler and Benyamini 1997). HRQ is an important measure of the impact of chronic disease (Guyatt, Feeny, and Patrick 1993). It has also been recognized as a useful measure for identifying health disparities and tracking trends, and is compatible with the definition of health by the World Health Organization (Moriarty, Zack, and Kobau 2003). SRD, our third health outcome, taps into an important dimension of psychological well-being; it is a common psychological disorder and the leading cause of disability worldwide (Friedrich 2017). Despite some caveats about the use of self-rated measures (Xu and Xie 2016; Zimmer and Amornsirisomboon 2001), numerous studies have documented the predictive power of these measures for a variety of health outcomes in different contexts (Abdulrahim and El Asmar 2012; Burström and Fredlund 2001; Idler and Benyamini 1997). All three variables were measured on a five-point scale, with SRH ranging from very poor to excellent, HRQ from always to never for whether health has affected life or work during the past four weeks, and SRD from always to never for feeling depressed during the past four weeks. We reverse coded these three variables so that a higher value corresponds to poorer health status (see Table 1 for the detailed coding schema).
Descriptive Statistics of Health Outcomes and Bivariate Analyses with Party Membership and Education.
SES Measures
We included both global and local measures (Soyoung and Mustillo 2017) of SES as our main predictors of the three health outcomes. Global indicators of SES are variables commonly used to measure SES across a variety of contexts, usually including education, income, employment, and subjective SES. We used four binary indicators to measure education, including junior high school, senior high school, and college and beyond, with elementary education used as the reference category. We also included log of family income in our analyses. Because there was a nonignorable percentage of missing data for income (13 percent), we used Stata 14 to impute the missing data and then used the imputed data in later analyses. 2 To account for psychosocial effects that operate through SES, we also included subjective SES, measured on a 10-point scale with one denoting at the bottom of society and 10 at the top. Employment status was measured using binary indicators for unemployed and other employment status (e.g., study, on leave, seasonal employment), with being employed as the reference category. 3
Local measures of SES, on the contrary, are more context specific. Because political capital in urban China is often viewed as an important driving force for upward mobility and housing is a particularly important indicator of SES, we included party membership (no = 0; yes = 1) and a set of indicator variables on housing ownership (no housing ownership [reference], owning one property, owning two properties, and owning three and more properties) as local measures of SES.
Control Variables
Control variables used in our study include age groups (based on a 10-year span and with 25–29 as the reference category), gender (male = 0; female = 1), ethnicity (non-Han Chinese = 0; Han Chinese = 1), marital status (first marriage [reference], unmarried, other status), and hukou (registered household residence) status (urban = 0; rural = 1). As China is characterized by a huge variation across regions in terms of economic development, health care resources, and natural and social environment, we created a set of dummy variables on geographic regions of residence (east [reference], central, west, and three traditional municipal cities). 4 To measure individuals’ access to health care resources, we included a binary indicator variable with one denoting having any kind of social health insurance in urban China, such as urban resident basic medical insurance, urban employee basic medical insurance, or public medical insurance (yes = 1; no = 0).
Lifestyle Measures
Scholarship in health research has long documented that lifestyle mediates the effects of SES indicators on health (Cockerham 2005; Colberg et al. 2010; Kawachi and Berkman 2001). Individuals with a high SES can more easily access and mobilize resources to improve their health status, including adopting a healthy lifestyle, which in turn leads to better health outcomes (Adler and Newman 2002; Lantz et al. 1998). Mainly to test the robustness of findings on SES indicators, this study also included the frequency of physical exercise and social activities with friends, both measured on an ordinal scale. Physical exercise ranges from one (never) to five (everyday), and social activities with friends range from one (never) to seven (everyday).
Statistical Models
Because the three outcomes are all measured on an ordinal scale, a natural candidate for modeling such ordinal responses is the proportional odds model. The proportional odds assumption behind this model, however, is often violated as is the case with all three ordinal outcomes used in this study. Thus, a less restrictive modeling technique that relaxes this assumption is needed (Fullerton and Xu 2016; Long and Freese 2006; Williams 2006, 2016). Of several viable possibilities, we chose the stereotype logit (SL) regression, which has a few advantages over its alternatives. For example, it allows the slopes to vary across different odds comparisons by proportionality constraints, thus making it possible to model response variables measured at both ordinal and nominal levels. Andersen (1984), J. Scott Long and Jeremy Freese (2006), Andrew S. Fullerton and Jun Xu (2016) all have cogent discussions about the SL model for ordinal responses, which is usually specified as follows:

where

By exponentiating
In our multivariate analyses, we ran a series of nested stereotypy logit regression of the three health outcomes. The first model includes party membership as a key and unique SES indicator along with commonly used controls, including age categories, gender, ethnicity, marital status, hukou status, and geographic regions. The second model adds other major indicators of SES, including education, income, employment status, housing ownership, and subjective SES, along with social health insurance status. The third model further includes lifestyle factors, including frequency of physical exercise and socializing with friends, mainly to test the robustness of findings on SES indicators. To account for possible correlations among observations within the same administrative/geographic regions, we controlled for the clustering effects of city districts in all our models.
Results
Table 1 presents descriptive statistics of the three ordinal response variables and results from our bivariate analyses between the three variables and party membership as well as educational attainment. It can be shown that roughly 12 percent of the respondents felt their health (SRH) was poor or fair, roughly 8 percent felt that their work or life (HRQ) was always or often affected by their health status, and 7 percent felt depressed (SRD) always or often. Our bivariate analyses using both contingency tables and stereotypy logit models (not shown in Table 1) indicate that both party membership and educational attainment are significantly associated with all three health outcomes in the expected direction.
Table 2 contains descriptive statistics of all independent variables. In our sample, about 15 percent of the respondents were party members, slightly less than half of the respondents were female, about 64 percent were aged between 30 and 60, and more than 94 percent were Han Chinese. Other interesting descriptive statistics include, for example, about a quarter of the respondents had a college degree or above, and close to 80 percent of the respondents stayed married in their first matrimony.
Descriptive Statistics of Independent Variables (N = 5,663).

Note. SES = socioeconomic status.
Results from the stereotype logistic regression of SRH are presented in Table 3. Model 1 shows that most of the control variables performed in the expected direction. For example, aging, being female, being out of first marriage, and living in inland regions all contributed to relatively poor SRH. As for our key independent variable, party membership, on the contrary, was associated with better SRH; that is, being a party member as opposed to a nonparty member increased the odds of having excellent, very good, good, and fair versus poor health by a factor
Stereotype Logistic Regression of Self-rated Health.

Note. Standard errors in parentheses. SES = socioeconomic status.
p < .10. *p < .05. Two-tailed test.
Almost all SES indicators, to varying degrees, were positively associated with better SRH in Models 2 and 3. Among the three binary indicators of education, ceteris paribus, only individuals with senior high school education, but not college-educated, turned out to have better SRH than those with elementary level education at the conventional significance level. We then took it further to examine the bivariate relationship between education and SRH, and our supplementary results showed that at the bivariate level, individuals with all three levels of education had better SRH than did the elementary-educated, with the strength of the association being in the expected order; that is, compared with the reference group with elementary education, the health benefits for college education were greater than those of junior and senior high school. Such a reduction in the strength of the association is indicative of some confounding or mediating effects via other demographic and socioeconomic variables added later on. The effects of family income, employment status, and subjective SES were all significantly associated with SRH in the expected direction, although such an association did not exist for housing ownership.
5
In addition, social health insurance did not have a statistically significant effect on SRH either. Also note that all estimated
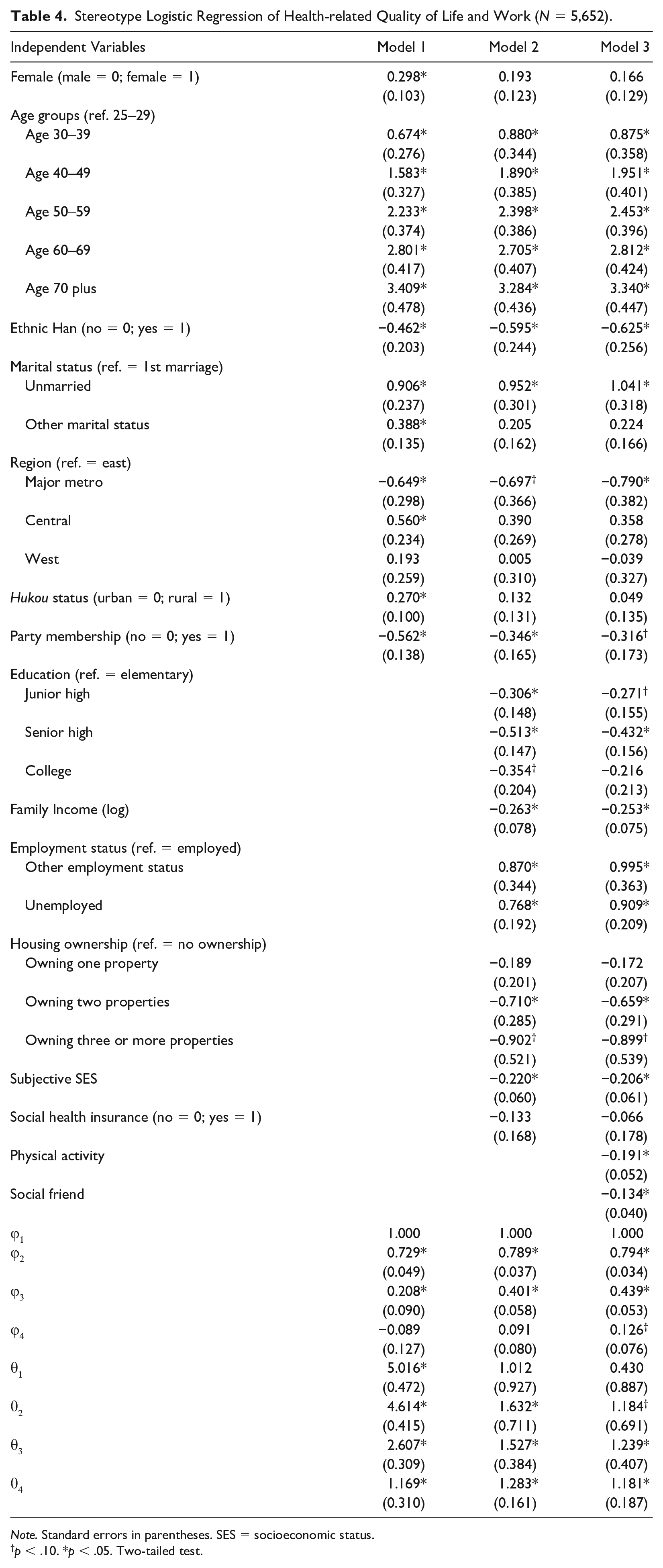
Results about our regression of HRQ are shown in Table 4. The general patterns are very similar to those of SRH in Table 3. Almost all corresponding parameter estimates in these two tables are in the same direction, with a few falling into different significance ranges. For HRQ, for example, being an ethnic Han, living in a major metropolitan area, and owning two or more residential properties were all associated with better HRQ, compared with their corresponding reference categories. The coefficients for these variables in our SL regression of SRH, however, did not reach the conventional level of significance (see Table 3).
Stereotype Logistic Regression of Health-related Quality of Life and Work (N = 5,652).
Note. Standard errors in parentheses. SES = socioeconomic status.
p < .10. *p < .05. Two-tailed test.
Results about our regression of SRD are shown in Table 5. The effect of party membership on depression remained negative and significant across all three models, even after we controlled for all other SES indicators and lifestyle factors. Of all traditional SES indicators, only subjective SES and, to a lesser degree, education (senior high vs. elementary school) were significant predictors of depression. For housing ownership, only when one possessed three or more housing properties, symptoms of depression subdued in a statistically significant way. In addition, staying in first marriage clearly provided emotional benefits, compared with other marital statuses. It is of note that people reached their peak of depression around the middle age, and then it tapered off. People living in major metropolitan areas had among the lowest level of depression, especially compared with individuals residing in inland regions.
Stereotype Logistic Regression of Self-rated Depression (N = 5,651).

Note. Standard errors in parentheses. SES = socioeconomic status.
p < .10. *p < .05. Two-tailed test.
We also used alternative modeling strategies, including proportional odds, generalized ordered logit, and multinomial logit models, to predict the three health outcomes, and the SL model was preferred in all cases using the Bayesian information criteria (BIC) statistic. Results from alternative models, in general, were consistent with what we presented here and even led to more liberal findings, in favor of our substantive conclusions. 6
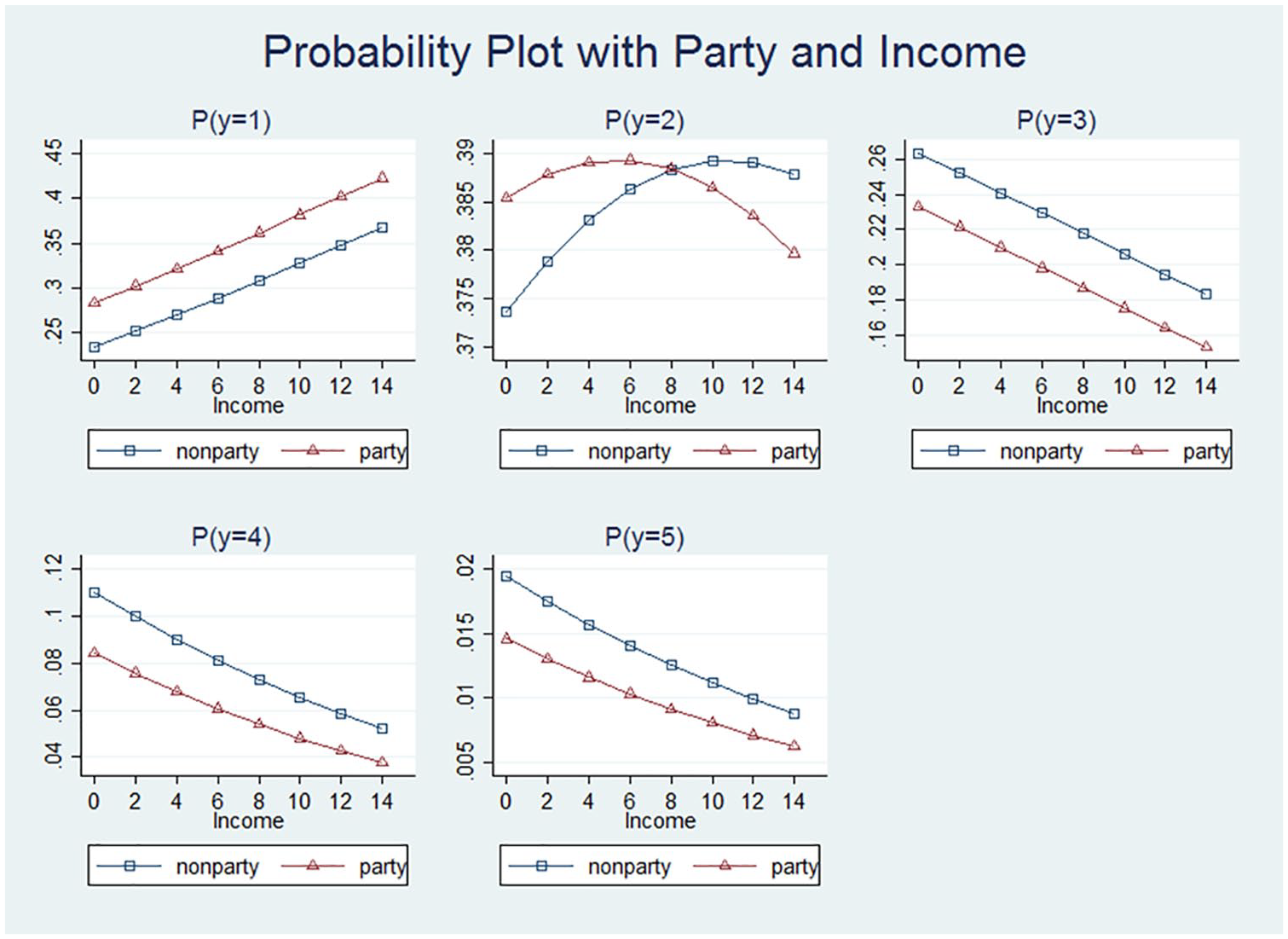
In many cases, raw and even odds ratio coefficients from typical ordered regression models are not that intuitively comprehensible except that they roughly inform the direction of the association. To further elucidate our findings, we took a step further to graph predicted probabilities against party membership along with logged income, with the former as a distinct local SES indicator and the latter as one of the most widely used global measures. Figures 1 to 3 illustrate such graphical patterns for SRH, HRQ, and SRD, while varying the values of party membership and logged income with other variables set to their respective means. Parameter estimates were obtained from Model 3. Note that each subfigure corresponds to a probability graph for a different response level labeled in subtitles. In agreement with findings from Table 3, Figure 1 on SRH shows that income increases the likelihood of having excellent (y = 1) and very good health (y = 2), but decreases with other response levels. In subfigures 1 to 2, the curve for the predicted probability of party membership is consistently, albeit slightly, above that of the nonparty members across the whole range of income, and the pattern is reversed in subfigures of the predicted probabilities for higher response levels (y = 3, 4, and 5) and correspondingly poorer SRH, suggesting that party members had a slight advantage over nonparty members in SRH even after we controlled for major indicators of SES and lifestyle factors. Figure 2 on HRQ presents almost identical patterns to those in Figure 1.
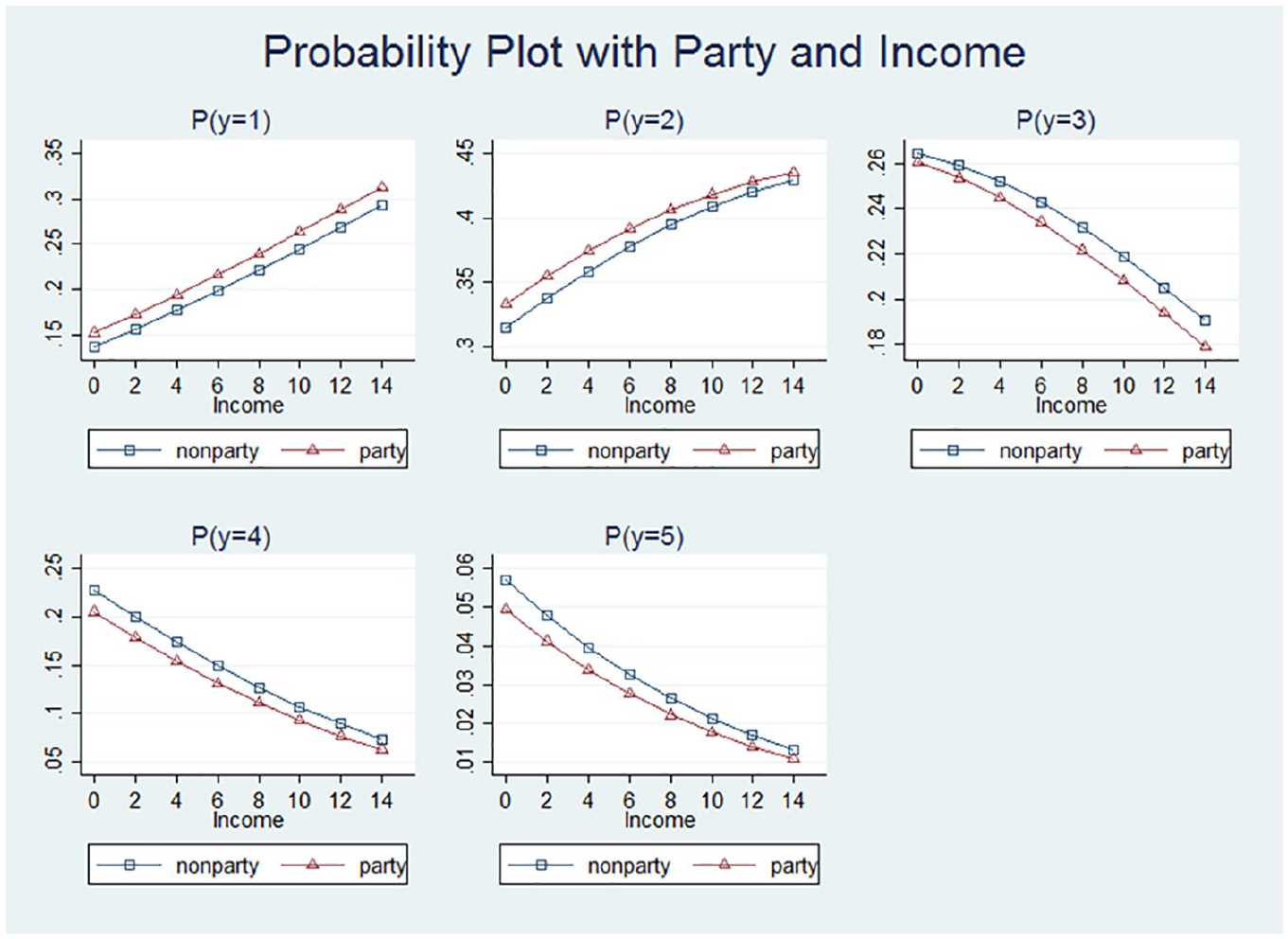
Predicted probabilities of self-rated health by response levels against party and income.

Predicted probabilities of health-related quality by response levels against party and income.
Predicted probabilities of self-rated depression by response levels against party and income.
In Figure 3, patterns similar to those for SRD emerge from the five subfigures. In general, income increases with the likelihood of an absence of depression (y = 1), whereas it is negatively associated with high levels of depression (y = 3, 4, 5). There is a curvilinear association between income and rarely having depression (y = 2). While income is around its middle range, depending on party membership, the probability of this particular depression level reaches its peak. But because the whole range of probabilities of rarely having depression is small (as shown in the subfigure), this finding may not have strong inferential basis. The same story can be told about party membership. As the level of depression increases, there is a clear advantage of being a party member as opposed to a nonparty member as all the probability curves for party membership are lower for feeling depressed sometimes, often, or always.
Conclusion
Both human capital and political capital are critically important in mobilizing and transferring resources as well as producing and reproducing social inequalities, especially in transitional societies. Prior scholarly works, however, have almost exclusively focused on economic inequality (e.g., income and housing), while largely ignoring other important measures of human development, such as health. Through integrating the theory of fundamental causes in health research and the stratification research about transitional economies, this study examines local forms of health-related resources in addition to global measures of SES, and yields novel and interesting findings. Using the stereotype logistic regression, a relatively new modeling technique that usually outperforms its traditional alternatives for ordered responses, our results show that all major SES indicators are associated with SRH, HRQ, and SRD, albeit to varying degrees. As far as we know, this study is among the first few to highlight that political capital, measured by communist party membership, is beneficial for self-rated health outcomes. In addition, our results also illustrate both the uniformity and peculiarity of the association between education and health in China.
It is not surprising to find that in China party membership is associated with better health outcomes as it represents a wide array of resources. In our analyses of SRH, the effect of party membership changes from strong to moderate to weak after we add a set of SES indicators and lifestyle factors, suggesting that much of the influence of party membership is mediated through these variables. Nevertheless, even after we control for these variables, the effect of party membership is marginally significant (SRH and HRQ) or very strong (SRD). The scarcity of literature on this topic and the lack of data for examining more nuanced mechanisms only allow us to entertain several possibilities. First, party membership possibly captures environmental adaptability or some underlying traits that are both preferred by the party member selection process and conducive to better health outcomes. Although party membership is primarily based on political allegiance and loyalty, the selection process increasingly emphasizes merit, which is often preconditioned on good physical and mental health (Bian et al. 2001; Braveman et al. 2005; Guo 2005; Walder 1995). Second, party membership may represent resources that are not commonly captured by traditional measures of SES. For example, expansive and powerful networks that could help party members gain easy access to health care and most up-to-date medical technology and treatment. A third possibility is that the status of party membership may provide a strong sense of belonging, security, and elevated self-esteem, given that the CCP is the only ruling party in China.
With regard to education, another important predictor of social inequalities in the market transition, the findings are not that straightforward for interpretation, particularly for college education. First of all, evidence from our study does show that having more education is associated with better health outcomes, but not necessarily in a linear or gradational manner. It appears that different levels of education may be associated with health in somewhat different ways. The most surprising finding is that after we control for other major indicators of SES and lifestyle factors, the effect of having college education reduces and disappears eventually, but it is much less so for secondary education, all compared with elementary education.
There can be several possible mechanisms in operation that lead to the indiscernible benefits at the college level. As discussed earlier, the two major exogenous factors that may contribute to this nuanced association include the long-term belaboring of the well-educated between 1955 and 1976 and the dramatic expansion of tertiary education since 1999, which may reduce or even reverse the positive association between education and health. Other factors, including the drastically changing institutional environment, the informalization and vast expansion of higher education through open universities (e.g., night and TV universities), the lack of emphasis on health and physical education across all educational levels, the promotion of unhealthy lifestyles in the upper-middle class (e.g., tobacco usage and binge-drinking/eating), and the pressure and stress induced by the soaring college tuition and increasing challenges for finding white-collar jobs, all may contribute to the intricate association between college education and health. Nevertheless, our findings regarding communist party membership and education in general align well with some new directions that the fundamental causes theory is taking; that is, it is equally important to investigate the effects of multidimensional SES, broadly defined, while taking into account contextualization and potentially countervailing mechanisms underlaying these SES indicators.
Among all SES indicators, it turns out that only subjective SES is consistently associated with all three health outcomes, indicative of its unequivocal predictive power for health. The effects of other SES indicators are less unequivocal, however, echoing some prior scholarship on similar associations in fragmented markets (e.g., Zhao 2012). For example, family income is associated with SRH and HRQ, but not SRD. Housing ownership has significant effects on HRQ and SRD, but not SRH. These may well be due to chance variation or some unobserved structural processes that are not considered in this study. Note that family income and housing ownership have significant bivariate associations with all three variables, and it appears that such associations are probably confounded with or mediated through other SES indicators for a particular health outcome. The underlying mechanisms through which such associations are accentuated or attenuated are intriguing in and of themselves, but they are beyond the scope of this project and warrant careful examination in future research.
While scholars have engaged in a lively debate on social inequalities during the market transition in China, most studies have typically focused on economic inequality, such as income or housing inequality. Instead, our study directs scholarly attention to health disparity, another important dimension of social inequalities. We have established that political capital (i.e., communist party membership), the lynchpin of social stratification in China’s market transition, is associated with SRH, HRQ, and SRD. While some scholarship on social stratification in transitional China predicts that the influence of political capital should have reduced to weak or nil, our results fail to show any sign of major decline. Instead, political capital seems to sustain the inroads of the market or even becomes formidable again, given the recent development in China’s politics. The net effect of human capital (i.e., education) on the three health outcomes is significant in our study, albeit devoid of a clear SES-health gradient similar to the one in the developed world. Such findings, as we argued, may be attributable to institutional characteristics and/or reforms in higher education in China. All these suggest that health scholars contextualize SES indicators in specific institutional and market environments to better appreciate their relevance to health disparities.
Like most empirical studies, this project was not executed without limitations. The cross-sectional nature of the sample data limits our ability to make causal claims. More detailed information that can help unfurl nuanced processes is not available in this project, thus making our findings on the relations between health outcomes and SES indicators less conclusive. There may also exist, to some extent, the issue of endogeneity, for example, the confounding effects between subjective SES and SRH. In spite of such caveats, our project is among the first few efforts to cross-fertilize important theoretical insights and empirical analyses in comparative sociology, health literature, and stratification research.
Footnotes
Authors’ Note
The three authors contributed equally to this paper. An early version of the paper was presented at the 2019 International Chinese Sociological Association Annual Meeting held at New York University.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.