
Abstract
The present study explores whether adolescent religiosity, health-related behaviors, and marital stability mediate the association between parental religiosity and health. Using data from the National Longitudinal Study of Adolescent to Adult (Add) Health, I model potential direct and indirect effects between three measures of parental religiosity (i.e., parental institutional religiosity, parental personal religiosity, and parental religious affiliation); three sets of mediators indicating adolescent religiosity, health-related behaviors, and marital stability; and self-rated health during late adolescence/early adulthood. Overall, I found that parental institutional religiosity has a direct effect on the self-rated health of children during late adolescence/early adulthood, and that it influences self-rated health by reducing adolescent and parental smoking. I also found evidence for deleterious effects of parental institutional religiosity on health as well. Future research should explore variation in the influence of parental religiosity on self-rated health between various sociodemographic groups and between different stages of the life course.
Introduction
Despite a large body of research exploring the association between religiosity and health, only a few studies have explored whether parental religiosity can influence health of one’s children. This is a perplexing omission because there are several reasons that it is likely that a parent’s religiosity indirectly influences the health of their adolescent children. First, studies consistently show strong positive associations between adolescent religiosity and both parental religiosity and adolescent health. Therefore, it is likely that parental religiosity improves the health of adolescent children by increasing an adolescent’s level of religiosity. Second, parental religiosity likely influences the health of adolescent children by encouraging behaviors that are positively associated with adolescent health (e.g., healthy eating, physical activity, getting adequate amounts of sleep) and discouraging behaviors that are negatively associated with adolescent health (e.g., substance use). Finally, parental religiosity likely influences the health of adolescent children indirectly by increasing marital stability, which is associated with improved adolescent health.
The present study explores whether adolescent religiosity, health-related behaviors, and marital stability mediate the association between parental religiosity and the self-rated health of children during late adolescence/early adulthood. Using data from the National Longitudinal Study of Adolescent to Adult (Add) Health, I model potential direct and indirect effects between three measures of parental religiosity (i.e., parental institutional religiosity, parental personal religiosity, and parental religious affiliation); three sets of mediators indicating adolescent religiosity, health-related behaviors, and marital stability, respectively; and self-rated health during late adolescence/early adulthood. I chose self-rated health as the outcome because it has been utilized as a measure of health across a variety of studies due to its easiness to interpret and administer, as well as the fact that it is associated with a wide variety of measures of objective health (Wu et al. 2013). I specifically utilize a measure of self-rated health measured during late adolescence/early adulthood to ensure that my measures of parental religiosity and mediators precede my measure of health in time, which is a requirement for testing mediation.
I posit that all three measures of parental religiosity will indirectly influence self-rated health through each of my mediators. I also posit that parental religiosity will not have a direct effect on self-rated health. In the next section, I will first provide a historical overview of the literature on the association between religiosity and health. Then I will explore the association between religiosity and health among adolescents, including potential mechanisms linking those phenomena, followed by a theoretical overview explaining the various mechanisms potentially linking parental religiosity and self-rated health of adolescent children. Finally, I describe each hypothesis in detail.
Literature Review
Historical overview
Research dating back to the nineteenth century reveals significant positive associations between various dimensions of religiosity (e.g., religious attendance, religious salience) and numerous measures of health and health-related behaviors. These measures of health and health-related behaviors include substance use disorders (Bartkowski and Xu 2007; Kelly et al. 2015; Koenig, King, and Carson 2012; Yonker, Schnabelrauch, and DeHaan 2012), depression (Bonelli et al. 2012; M. J. Pearce, Little, and Perez 2003; Smith 2003), stress levels (Ellison et al. 2001), cardiovascular health (Comstock 1971; Horne et al. 2008; Kobayashi et al. 2015; Lapane et al. 1997; Obisesan et al. 2006), cancer risk (Jim et al. 2015), mortality (Ellison et al. 2000; Hummer et al. 1999; Lutgendorf et al. 2004), and self-rated health (Doane and Elliott 2016; Ferraro and Albrecht-Jensen 1991; Krause and Hayward 2014; Levin 2015; McCullough and Laurenceau 2005; Mukerjee and Venugopal 2018; Stavrova 2015; Veenstra 2000; Zhang 2017). Significant associations between religiosity and health have been found in both male and female samples; across various racial and ethnic groups; in Western and non-Western samples; across various social classes; and across various life stages.
The first sociological study to explore the association between religiosity and health was the book Suicide (Durkheim 1897). The study explored the patterns of disparities in suicide rates between European countries as well as potential origin for these disparities. The most notable finding from Suicide was that suicide rates were lower in countries with majority-Catholic populations compared to countries with majority Protestant populations. Durkheim theorized that this disparity was due to greater levels of social control within Catholic countries, which leads to higher levels of social integration—and by extension—lower rates of suicide. However, there have been several scholars who have disputed this finding (see Selvin 1965; Van Poppel and Day 1996 as examples). Despite that, studies continue to find that religion plays a protective role against suicide (Wu, Wang, and Jia 2015).
Institutional religiosity and health
According to Suicide, variation in religious structures—rather than differences in religious beliefs—accounted for religion’s influence on suicide rates. Over the years, various other scholars have also cited involvement in religious institutions as being the primary driver of the connection between religion and health. In particular, religious involvement has been found to reduce mortality risk during subsequent years (Bruce et al. 2017; Ellison et al. 2000; Hummer et al. 1999; Li et al. 2016; Strawbridge et al. 1998). Attendance at religious services has also been found to be associated with lower levels of depression, lower blood pressure, improved immune functioning, enhanced physical functioning, and improved self-rated health (Koenig and Vaillant 2009).
In Suicide, Durkheim argued that religion improved the health and well-being of individuals by regulating their behaviors and integrating them into networks of social support. Over the years, various studies have provided evidence for this argument. For example, researchers have found that attendance at religious services influences health by encouraging healthy lifestyle habits such as regular exercise (Wallace 2008), reducing the likelihood of engaging in unhealthy behaviors such as substance use (Kelly et al. 2015), and improving overall life satisfaction (Headey et al. 2010).
Attendance at religious services has also been found to improve health by providing social support during stressful life events. It provides coping resources that reduce stress and improve overall mental and physical health (Bruce et al. 2017; Ellison and Henderson 2011; Ellison and Levin 1998). There is also evidence that attendance at religious services may reduce the likelihood of stressful life events ever occurring. Margarita Mooney and colleagues (2014) found that attendance at religious services reduced the likelihood that individuals experienced both “controllable” stressful life events (e.g., divorce) and “uncontrollable” stressful life events (e.g., death of a loved one). They also found that attendance at religious services by one’s parent also reduced an individual’s likelihood of experiencing controllable stressful life events.
Personal religiosity and health
In addition to institutional religiosity, some studies have found that personal religiosity—in particular prayer 1 and belief in a connection to a higher power—improves mental and physical health. For example, Peter A. Boelens and colleagues (2009) discovered that direct contact person-to-person prayer both reduced depression and anxiety and increased optimism. Studies have also shown that prayer is associated with lower pain scores after a C-section (Beiranvand et al. 2014) and improved the quality of life for women who are diagnosed with breast cancer (Jafari et al. 2013). In addition, a belief in a divine connection with a higher power (Ellison 1991; Ellison et al. 1989; Foley 1988; Holt and McClure 2006; Idler 1987; Roth et al. 2016) as well as a belief that one is forgiven of sins by a higher power (Ellison 1991; Lutjen, Silton, and Flannelly 2012) improves health by reducing stress, increasing self-efficacy, and alleviating the insalubrious effects of guilt.
Religious affiliation and denominational differences in health
Religious affiliation refers to identification with a specific religious group, but does not necessarily denote membership in the group. While used interchangeably with affiliation, religious denomination typically only refers to affiliation with a specific Protestant sect. A few studies have linked differences in religious affiliation and/or religious denomination with health, though most of these studies do not primarily focus on religious affiliation or denominational differences (Schlundt et al. 2008). One factor that may explain affiliation and denominational differences in health may be differences in the “strictness” of rules between religious groups. Churches with stricter rules (e.g., conservative Protestant Churches) may lead to improved health by restricting the behaviors of adherents as well as selecting out individuals who refuse to adhere to strong religious edicts (Iannaccone 1994).
Studies have found significant affiliation and/or denominational differences in a variety of measures of health such as body weight (Kim, Sobal, and Wethington 2003), use of preventive medical interventions (Benjamins and Brown 2004), life satisfaction (Cohen 2002), substance use (Ford and Kadushin 2002; Gillum 2005), and breast cancer survival (Van Ness, Kasl, and Jones 2003). David G. Schlundt and colleagues (2008), however, found no significant denominational or affiliation differences when controlling for demographic factors as well as an index of individual religious involvement made up of attendance at religious services, religious salience, and a measure of religion as a source of comfort.
Selection effects
Another potential reason for the apparent association between religiosity and health are selection effects. They occur when unobserved (and unmeasured) factors create an apparent association between two traits. In the case of religiosity and health, these unobserved factors may include age, race, gender, personality traits, psychological traits (e.g., impulsivity), or genetic disposition (e.g., behavioral disinhibition). Mark D. Regnerus and Christian Smith (2005) found that various factors including proclivity toward taking risk, temperament, and fearfulness at least partially account for the association between religiosity and self-rated health.
Concerning genetic disposition, numerous studies reveal nontrivial heritability estimates for both religiosity (Boomsma et al. 1999; Bradshaw and Ellison 2008; Button et al. 2011; D’Onofrio et al. 1999; Eaves et al. 2008; Koenig, McGue, and Iacono 2008; Koenig et al. 2005; Winter et al. 1999) and self-rated health (Mosing et al. 2010; Romeis et al. 2000; Svedberg et al. 2005). Pleiotropic effects may explain at least part of the covariance between religiosity and self-rated health. Pleiotropic effects occur when a common set of genetic factors influence one or more traits. In regard to religiosity and self-rated health, genetic factors associated with neuroticism, objective measures of health, and traits that mediate the association between religiosity and self-rated health (e.g., substance use behaviors) may at least partially explain the association between those two phenomena.
Deleterious effects of religiosity on health
While most of the literature on the association between religiosity and health reveals a significant positive association between these two phenomena, a few studies reveal deleterious effects of some dimensions of religiosity on health. For example, Randy Hebert and colleagues (2009) found that negative religious coping (e.g., feeling abandoned by or anger at God) among women with breast cancer predicted worse overall mental health, depressive symptoms, and lower life satisfaction. In addition, studies show that religious doubt (Ellison and Lee 2010; Krause and Wulff 2004) and strained relations with co-religionists (Krause and Ellison 2009) have a deleterious effect on health as well. Also, a few studies have examined whether religious fatalism, the belief that an individual’s outcomes are predetermined by a higher power and is therefore beyond their control, inhibits the use of health care services and health promotion programs (Franklin et al. 2007). Overall, studies have found that religious fatalism is associated with poorer health outcomes, in particular among black and Hispanic populations (Franklin et al. 2007; Nageeb et al. 2018).
Religiosity and health among adolescents
Despite the large body of research exploring the association between religiosity and health in the overall population, relatively few studies have specifically examined the association between religiosity and health among adolescents (Regnerus 2003; Wallace 2008). This is possibly because researchers who study adolescent health have traditionally failed to include religious measures in their studies (Regnerus 2003; Thomas and Carver 1990; Wallace 2008). Christian Smith (2003) argues that this puzzling omission may reflect reductionist tendencies among scholars who argue that any association between religiosity and health among adolescents is likely spurious.
The few studies that have examined the association between religiosity and health among adolescents typically find a significant positive association between the two phenomena (Benson, Donahue, and Erickson 1989; Cotton et al. 2006; Donahue and Benson 1995; Hyde 1990; Regnerus 2003; Thornton and Camburn 1989; Wallace and Forman 1998; Wallace and Williams 1997). Among adolescents, religiosity has been found to be protective against a variety of negative health outcomes and negative health-related behaviors including smoking (Sussman et al. 1993), drug use (Hodge, Cardenas, and Montoya 2001; Miller 2000), risky sexual behaviors (Regnerus 2007); suicide (Borowsky, Ireland, and Resnick 2001), depression (M. J. Pearce et al. 2003; Wright, Frost, and Wisecarver 1993), and injuries (Wallace 2008).
Religiosity has also been found to encourage some behaviors related to better health such as healthy eating, exercise, and getting an adequate amount of sleep each night (Wallace 2008; Wallace and Forman 1998). Moreover, like the association between religiosity and health in the general population, some dimensions of religiosity can have a negative impact on health, such as the negative health impacts of being a religious minority (Estrada et al. 2019).
Within the literature on the association between religiosity and health during adolescence, various theoretical mechanisms have been put forward to explain the association. The most common mechanism cited is religion as an agent of social control (Regnerus 2003; Wallace 2008). Social control theory posits that social order is based on conventional moral beliefs and values, which are internalized and upheld by society. Religious teachings are a key source of moral beliefs and values and are internalized through involvement with religious institutions such as religious congregations and religious youth groups (Caputo 2004; Hirschi and Stark 1969; Smith 2003). These internalized beliefs, such as the belief that suicide is a sin and that sex should only occur within marriage, may decrease the likelihood that an adolescent engages in behaviors that are deleterious to their health.
John M. Wallace and David R. Williams (1997) went beyond the social control explanation for the association between religiosity and health and argued that religion influences adolescent health by providing adolescents with a means of social integration and social support, helping them develop their identity and values. In other words, in addition to internalized values that adolescents receive from religious teachings, religious organizations also provide adolescents with co-religionist peers who model behaviors that have positive health effects, such as abstinence from smoking and avoidance of risky sexual behaviors. Religion also provides identities for adolescents that may require them to avoid behaviors that risk their health. For example, Seventh-Day Adventists have a holistic view of religion and emphasize that living a healthy lifestyle is an expression of their faith. This lifestyle often includes a largely (or strictly) vegetarian diet. Studies show Seventh-Day Adventists who adhere to such a diet have a lower mortality rate (Orlich et al. 2013) and lower rates of diabetes, cancer, hypertension, and arthritis (Fraser 1999) than the general population.
Smith (2003) took a more comprehensive view of the association between adolescent religiosity and health and argued that there are nine distinct, yet connected theoretical mechanisms linking adolescent religiosity and adolescent outcomes. These mechanisms include moral directives, spiritual experiences, role models, community and leadership skills, coping skills, cultural capital, social capital, network closure, and extra-community skills. Smith organized these nine mechanisms into three groups which are (1) moral order (moral directives, spiritual experiences, and role models); (2) learned competencies (community and leadership skills, coping skills, and cultural capital); and (3) social and organizational ties (social capital, networks closures, and extra-community skills). Unlike Wallace and Williams (1997), who argued that religion influences adolescent outcomes indirectly through social control, social support, and shaping identity/values, Smith argued that some of the mechanisms allowed religion to have a direct influence on adolescent outcomes. For example, moral directives that prohibit substance use (Chawla et al. 2007; Michalak, Trocki, and Bond 2007) and premarital sex (Lammers et al. 2000; Regnerus 2007; Thornton and Camburn 1989; Wallace 2008) directly lead to lower levels of substance use and sexual activity among adolescents, even controlling for other relevant facts. In other words, religiosity itself, and not just factors associated with religiosity, has a direct influence on adolescent health.
Overall, it is likely that religiosity influences adolescent health through multiple pathways, both directly and indirectly. The influence of internalized religious teachings and values on behavior (i.e., social control) is the most cited way in which adolescent religiosity influences adolescent health and health-related behaviors. However, other religious factors may influence adolescent health and health-related behaviors such as integration into religious organizations that regulate behaviors through rewards and sanctions, and religious identities that require strict adherence to rules governing diet and lifestyle choices.
Theoretical Framework: The Influence of Parental Religiosity on Adolescent Health?
While little is known about the association between adolescent religiosity and adolescent health, even less is known about the association between parental religiosity and adolescent health. Only a few studies have found a direct association between parental religiosity and adolescent health, and these studies suffer from the same significant methodological problem. For example, Richard K. Caputo (2004) found that parental religiosity was positively associated with a measure of self-rated health and inversely associated with substance abuse. While Caputo utilized a religious scale made up of six statements describing the way some people feel about religion and religious practices, Caputo failed to account for the adolescent’s own religious status within his models. In addition, Merrill, Folsom, and Christopherson (2005) found that within a sample of Latter-Day Saint (LDS) adolescents, parental religiosity showed an inverse association with substance use. However, like the Caputo study, this study did not control for adolescent religiosity. Based on the paucity of published studies showing a direct association between parental religiosity and adolescent health, coupled with the relative weakness of the literature, it is likely that parental religiosity does not have a direct influence on adolescent religiosity. This leads to the first hypothesis (H1) tested in this paper, which states that parental religiosity does not have a direct influence on adolescent self-rated health.
Despite the lack of studies finding a direct association between parental religiosity and the health of adolescent children, there is evidence that parental religiosity influences the health of their children indirectly via the adolescent child’s own religiosity. Studies indicate that there is a strong positive association between parental religiosity and adolescent religiosity (Francis and Brown 1991; Hayes and Pittelkow 1993; Myers 1996; Ozorak 1989; L. Pearce and Denton 2011:23). Parents socialize their children by both modeling religious behaviors (e.g., weekly attendance at religious services) and encouraging religious behaviors with various sanctions (e.g., ostracism, corporal punishment) and rewards (personal praise, increased personal autonomy). Studies show that the effectiveness of religious socialization depends on the level of conflict between the parent and child. When conflict is high, the association between parental religiosity and that of the child is weak or nonexistent (French et al. 2013; Kirkpatrick and Shaver 1990; Rafford 2011). This is probably because children are less likely to model their parent’s behaviors when there is conflict with the parent. Therefore, rewards and sanctions are less effective when there is parent-child conflict. Studies also show that the association between parental and childhood religiosity weakens as children age (Francis and Brown 1991; Myers 1996; Zhang 2017). This may be due to increased personal autonomy as an adolescent ages, which may lead to a disjuncture between the parent’s behaviors and that of the adolescent.
In addition to findings showing a significant positive association between parental religiosity and adolescent religiosity, studies also indicate that there is a strong positive association between adolescent religiosity and adolescent health (Benson et al. 1989; Cotton et al. 2006; Donahue and Benson 1995; Hyde 1990; Regnerus 2003; Thornton and Camburn 1989; Wallace and Forman 1998; Wallace and Williams 1997). Therefore, as parents socialize their children into a religion, they are also providing their children access to the health benefits associated with religion such as decreased likelihood of engaging in risky behaviors and increased likelihood of engaging in healthy behaviors. This leads to the second hypothesis (H2) tested within this paper, which is that parental religiosity influences adolescent self-rated health indirectly via adolescent religiosity.
Parental religiosity may also influence adolescent health by encouraging healthy behaviors and discouraging unhealthy behaviors. Religious individuals, including religious parents, are more likely to avoid unhealthy behaviors such as smoking, engaging in risky sexual behaviors, and suicidality. In addition, various groups such as Seventh-Day Adventists, LDS, and Jehovah’s Witnesses adhere to strict behavioral and dietary guidelines. Social learning theory posits that a child’s behavior is taught and maintained through social influences, such as parents, peers, and religious institutions (Akers 1985). Therefore, the children of religious parents are likely to avoid unhealthy behaviors and engage in a healthy lifestyle.
Parental religiosity may also influence adolescent health by rewards that encourage healthy behaviors and sanctions that discourage unhealthy behaviors. As previously stated, social control theory posits that that social order is based on conventional moral beliefs and values, which are internalized and upheld by society. Religious teachings are a key source of moral beliefs and values and are internalized through involvement with religious institutions such as religious congregations and religious youth groups (Caputo 2004; Hirschi and Stark 1969; Smith 2003). Religious parents may ostracize or punish children for unhealthy behaviors such as smoking, alcohol use, and risky sexual behaviors. Extreme examples of this are honor killings among some groups of Hindus and Muslims (Chesler and Bloom 2012) and shunning among groups such as the Amish (Hurst and McConnell 2010) and Jehovah’s Witnesses (Holden 2002). Religious parents may also encourage healthy behaviors through various rewards such as personal praise, increased status within the family, and increased personal autonomy. Therefore, highly religious parents may have healthier children because their children are afraid of being sanctioned by the parents (or religious community as a whole) or desire rewards associated with adherence to family or community norms. This leads to the third hypothesis (H3) tested in this paper which is that religious parents influence adolescent self-rated health by increasing the likelihood of engaging in healthy behaviors and reducing the likelihood of engaging in unhealthy behaviors.
Finally, parental religiosity may also indirectly influence adolescent health through increased marital stability. Studies have consistently shown that marital instability is associated with worse health outcomes for their children (Lee and McLanahan 2015; Waldfogel, Craigie, and Brooks-Gunn 2010). Children of divorce tend to show declines in cognitive development (Lee and McLanahan 2015; Magnuson and Berger 2009; Waldfogel et al. 2010), increases in behavioral problems (Cavanagh and Huston 2006; D’Onofrio and Emery 2019; Fomby and Cherlin 2007; Osborne and McLanahan 2007), and declines in physical health (Bzostek and Beck 2011). Studies also find that marital stability is positively associated with religiosity (Call and Heaton 1997; Kaslow and Robison 1996; Larson, Larson, and Gartner 1990; Robinson and Blainton 1993). This is likely because of the stigma associated with divorce and nonmarital sex among many religious groups. Therefore, parents who are highly religious are less likely to divorce than nonreligious parents. As a result, the children of highly religious parents are less likely to suffer the negative effects of martial instability. This leads to the fourth hypothesis tested in this paper (H4) which is that parental religiosity has an indirect association with adolescent self-rated health via marital stability.
Data and Measures
Sample
The data for these analyses come from the parent and adolescent samples taken during the first three waves 2 of the National Longitudinal Study of Adolescent to Adult Health (Add Health), a nationally representative longitudinal survey of adolescents and young adults obtained from an initial in-school survey of middle- and high school students conducted from September 1994 to April 1995. These samples are utilized because they include measures of parental and adolescent religiosity along with self-rated health. They also include measures of adolescent health-related behaviors (e.g., healthy eating, substance use) and parental marital stability. In total, 90,118 adolescents who attended 80 high schools and 54 feeder schools (both public and private) took part in the initial interview. During the months of April through December 1995, a sample of the in-school respondents (stratified by gender and grade) was selected to participate in an in-home face-to-face interview (wave I). This sample included 20,745 individuals. During Wave I, 17,670 parents (or guardians) were also interviewed. These interviews provided demographic and health-related information about the parent or guardian as well as general information about the adolescent respondents. The in-home sample adolescent respondents were re-interviewed in 1996 for wave II, in 2001–2002 for wave III; in 2008–2009 for wave IV; and the 2016–2018 timeframe for wave V.
Self-rated health
Self-rated health was assessed by asking “In general, how is your health?” The variable was reverse coded for the analyses and ranged from 5 indicating “excellent health” to 1 indicating “poor health.” To test mediation I utilized a lagged measure of self-rated health from wave III, which follows the measures of parental religiosity as well as the mediators in time-order. During wave III, individuals are between the ages of 18 and 26. This period of the life course has been described as late adolescence, early adulthood, and emerging adulthood (Arnett 2000). I refer to this period as late adolescence/early adulthood.
Religiosity
For this study, three measures of parental and adolescent religiosity are utilized: institutional religiosity, personal religiosity, and religious affiliation. To test mediation each measure of parental religiosity is from wave I and each measure of adolescent religiosity is from wave II.
Institutional religiosity is religiosity that occurs exclusively as part of a religious organization such as a church or religious youth group. Measures of institutional religiosity include attendance at religious services and participation in religious activities. Personal religiosity is religiosity that occurs on a personal level, completely independent of a religious organization. Examples of personal religiosity include beliefs about the importance of religion in one’s life as well as private prayer outside of a religious organization.
Marie Cornwall and colleagues (1986) were the first scholars to empirically verify the existence of institutional and personal religiosity. They described two modes of religious involvement: personal and institutional. The personal mode consists of beliefs, feelings, and behaviors that originate on the personal level. This includes accepted beliefs within a religious group (e.g., abstinence before marriage). The institutional mode consists of beliefs, feeling and behaviors, related to formal religious involvement. This includes participation in religious rituals (e.g., Holy Communion) and religious services. Utilizing principal components factor analysis, Cornwall and colleagues found evidence that the personal and institutional modes constituted independent dimensions of religiosity.
For the present study, parental institutional religiosity is measured by a single measure, parental attendance at religious services. This variable ranges from 0 to 3 with 0 indicating “no attendance at religious services” and 3 indicating “attendance at religious services at least on a weekly basis.” Parental personal religiosity is an index made up of a measure of religious salience and a measure of frequency of prayer. Religious salience was measured with the question: “How important is religion to you?” Responses to this question were coded into a variable that ranged from 0 to 3 with 0 indicating a response of “not important at all” and 3 indicating a response of “very important.” To measure daily prayer respondents were asked, “How often do you pray?” Responses ranged from 1 to 5 with 1 indicating “daily” and 5 indicating “never.” This variable was recoded into a four-category variable with 0 indicating “never”; 1 indicating “monthly or less”; 2 indicating “weekly”; and 3 indicating “daily.” Cronbach’s alpha for parental personal religiosity is .86.
Adolescent institutional religiosity is an index consisting of a measure of attendance at religious services and a measure of participation in religious activities. Responses range from 0 to 6 with 0 indicating “no attendance or participation” and 6 indicating “weekly attendance or participation.” Cronbach’s alpha for adolescent institutional religiosity is .74. Adolescent personal religiosity is an index made up of a measure of religious salience and a measure of frequency of prayer. Religious salience is measured by the question: ““How important is religion to you?” Responses to this question were coded into a variable that ranged from 0 to 3 with 0 indicating a response of “not important at all” and 3 indicating a response of “very important.” Daily prayer was measured with the question: “How often do you pray?” Responses ranged from 1 to 5 with 1 indicating “daily” and 5 indicating “never.” This variable was recoded into a 4-category variable with 0 indicating “never”; 1 indicating “monthly or less”; 2 indicating “weekly”; and 3 indicating “daily.” Cronbach’s alpha for adolescent personal religiosity is .47.
Parental religious affiliation and adolescent religious affiliation are modified versions of the RELTRAD religious classification scheme devised by Steensland and colleagues (2000). To avoid the potential for multicollinearity with the black racial category, black Protestant respondents were incorporated into theologically similar Conservative or Mainline Protestant categories. The religious affiliation variable consists of five categories: (1) Conservative Protestant, (2) Mainline Protestant, (3) Roman Catholic, (4) Other Religion (Jews, Muslims, Hindus, etc.), and (5) No Religion. Conservative Protestants is the omitted reference group.
Conflict
Parent-child conflict is measured by an index made up of five variables that describe the nature of the relationship between the residential parent and their adolescent children. The five variables used to create the index include a variable indicating the warmth of the relationship between the parent to the child, how caring the child feels the parent is, how close the adolescent child feels they are to their parent, how satisfied the adolescent child is with their communication with their parent, and overall how satisfied they are with their relationship with their parent. Each variable is measured using a Likert scale with 1 indicating “strongly disagree” and 5 indicating “strongly agree.” Cronbach’s alpha for parent-child conflict is .85.
Health-related behaviors
Eight measures of health-related behaviors—defined as behaviors that positively or negatively influence a respondent’s health—were used in my analyses. They include self-reported frequency of adolescent smoking, self-reported frequency of adolescent alcohol use, self-reported parental smoking, self-reported parental alcohol use, self-reported sleep problems, self-reported healthy eating, self-reported physical activity, and self-reported number of sexual partners. Self-reported adolescent smoking is measured as how many days in the past 30 days that a respondent indicated that he or she smoked. Self-reported adolescent alcohol use is measured as the number of days a respondent indicated that he or she drank alcohol during the past 12 months. Responses range from 0 indicating “never” and 6 indicating “every day or almost every day.” Self-reported parental smoking is measured by a dichotomous variable indicating whether a parent or guardian indicated that he or she smokes. Self-reported parental alcohol use is measured as how often a parent or guardian indicated he or she currently drinks alcohol. Reponses range from 0 indicating “never” to 5 indicating “nearly every day.”
Self-reported sleep problems is a measure of how often a respondent had trouble falling or staying asleep. Responses ranged from 0 indicating “never” to 4 indicating “every day.” Self-reported healthy eating is measured by an index made up of four variables that describe whether a respondent had eaten vegetables, dairy products, fruit, or grain-based foods (e.g., bread, rice, cereal) the previous day. According to the Centers for Disease Control and Prevention (CDC) and United States Department of Agriculture (USDA), individuals require nutrients provided by these groups of foods and lacking one or more is associated with poorer health. Each item of the index was coded a 1 indicating they had eaten a food from that food group the previous day and 0 indicating that they had not. Cronbach’s alpha for health-related behaviors is .32. Self-reported physical activity is measured as the number of times a respondent participated in physical activities (e.g., running, bicycling, weightlifting) in the past 7 days, and ranged from 0 indicating “no physical activity” to 3 indicating “greater than 3 physical activities.” Cronbach’s alpha for physical activity is .42. Self-reported number of sexual partners is measured as a respondent’s number of sexual partners in the months following their last Add health interview. These data are based on the question, “Since the month of the last interview, with how many people, in total, including romantic relationship partners, have you ever had a sexual relationship?” Responses range from 0 sexual partners since the month of the last interview to 20 or more sexual partners in that time.
Covariates
To avoid the confounding effects of excluded variables, covariates for age, gender, 3 race/ethnicity, household income, and region are included in each model. Age is calculated using the interview completion date and date of birth variables. Because only the month and year of birth are available, 15 is used as the day of birth when calculating age. Gender is determined by the interviewer. The interviewer was directed to ask the gender of the respondent if necessary. The omitted reference category for gender in the analyses is female. Household income was measured as the total household income from all sources before taxes and deductions. A log-transformed version of this variable was used in order to lessen the impact of extremely high incomes on statistical estimates. Most respondents reported their household income in dollars. A few preferred to report a range; the midpoints of the indicated ranges were used for these respondents. Race/ethnicity is a set of categorical variables that indicates if a respondent is Hispanic, non-Hispanic, white, black, or Other. To determine race/ethnicity, respondents were asked to indicate their racial status. If they chose more than one racial status, they were asked to indicate which racial status best describes them. Respondents were categorized into the racial group they felt best described them. Respondents were also asked if they were Hispanic. If a respondent indicated that he or she is Hispanic, they were placed in the Hispanic race/ethnic group. The omitted reference category for race/ethnicity in the analyses is the “Other” category. The state in which participants attended school at wave I was coded into regions consistent with the coding established by the U.S. Census Bureau. Regions include Northeast, Midwest, South, and West with West being the omitted reference category.
Analytic Strategy
I estimate structural equation models using Lavaan 0.6-5 to test each of my hypotheses. Each model is estimated using maximum likelihood (ML) estimation and includes covariates for age, race, gender, income, and region. To account for missing values, full information maximum likelihood (FIML) is utilized.
Each of the models test the association between all three measures of parental religiosity, a set of mediators, and a lagged measure of self-rated health. Each of the measures of parental religiosity is taken from wave I of the Add Health Study, while each of the mediators (with the exception of parental substance use and parental marital stability) is measured at wave II, and the lagged measure of self-rated health is measured at wave III. Figure 1 illustrates the mediation effect tested in each model. To test mediation, I utilize the following equation:
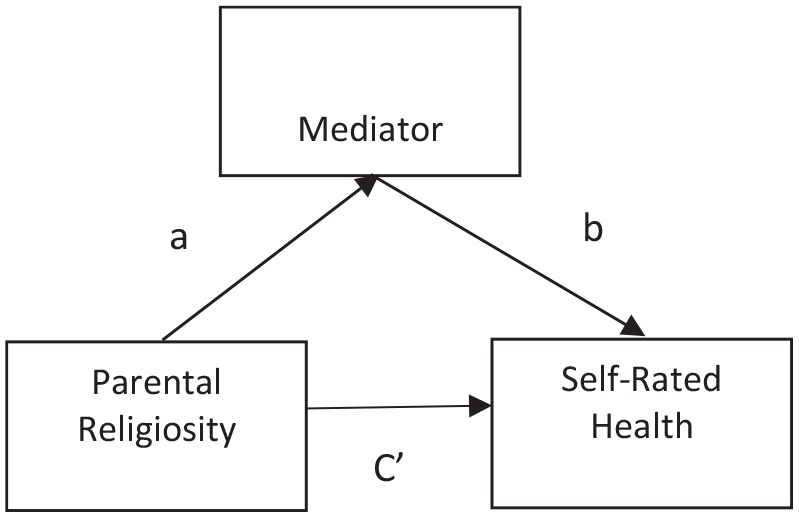
Mediation model.
Where c is the total effect of parental religiosity on lagged self-rated health, a is the influence of parental religiosity on each mediator, b is the influence of each mediator on lagged self-rated health, and c′ is the direct effect of parental religiosity on lagged self-rated health. Indirect effects are estimated as the product of the influence of parental religiosity on each mediator and the influence of each mediator on lagged self-rated health (ab). To test for the presence of mediation effects, p values and confidence intervals are estimated for each indirect effect. A significant p value (<.05) indicates evidence of mediation between parental religiosity, the mediator, and lagged self-rated health. Because the indirect effect (a*b) is not normally distributed, bootstrapping based on 1,000 draws is used to estimate standard errors for each indirect effect.
I test each of the hypotheses in a sequential order utilizing three models which I refer to as the religious socialization model, the health-related behaviors model, and the marital stability model. Figure 2 illustrates a conceptual model which combines each of my full models. I test H1 and H2 using the full religious socialization model. This model includes a mediation effect for adolescent religiosity on the association between parental religiosity and lagged measure of self-rated health. In addition, various studies show that parent-child conflict moderates the association between parental religiosity and adolescent religiosity (French et al. 2013; Kirkpatrick and Shaver 1990; Rafford 2011). Therefore, I fit a moderated mediation model in which parent-child conflict moderates the association between parental religiosity and adolescent religiosity. I use a multiple group approach (Miles et al. 2015) in which I model the mediation effect of adolescent religiosity on the association between parental religiosity and self-rated health during late adolescence/early adulthood for individuals experiencing “high” levels of parent-child conflict (one standard deviation above the mean level of parent-child conflict) and individuals experiencing “low” levels of parent-child conflict (one standard deviation below the mean level of parent-child conflict).
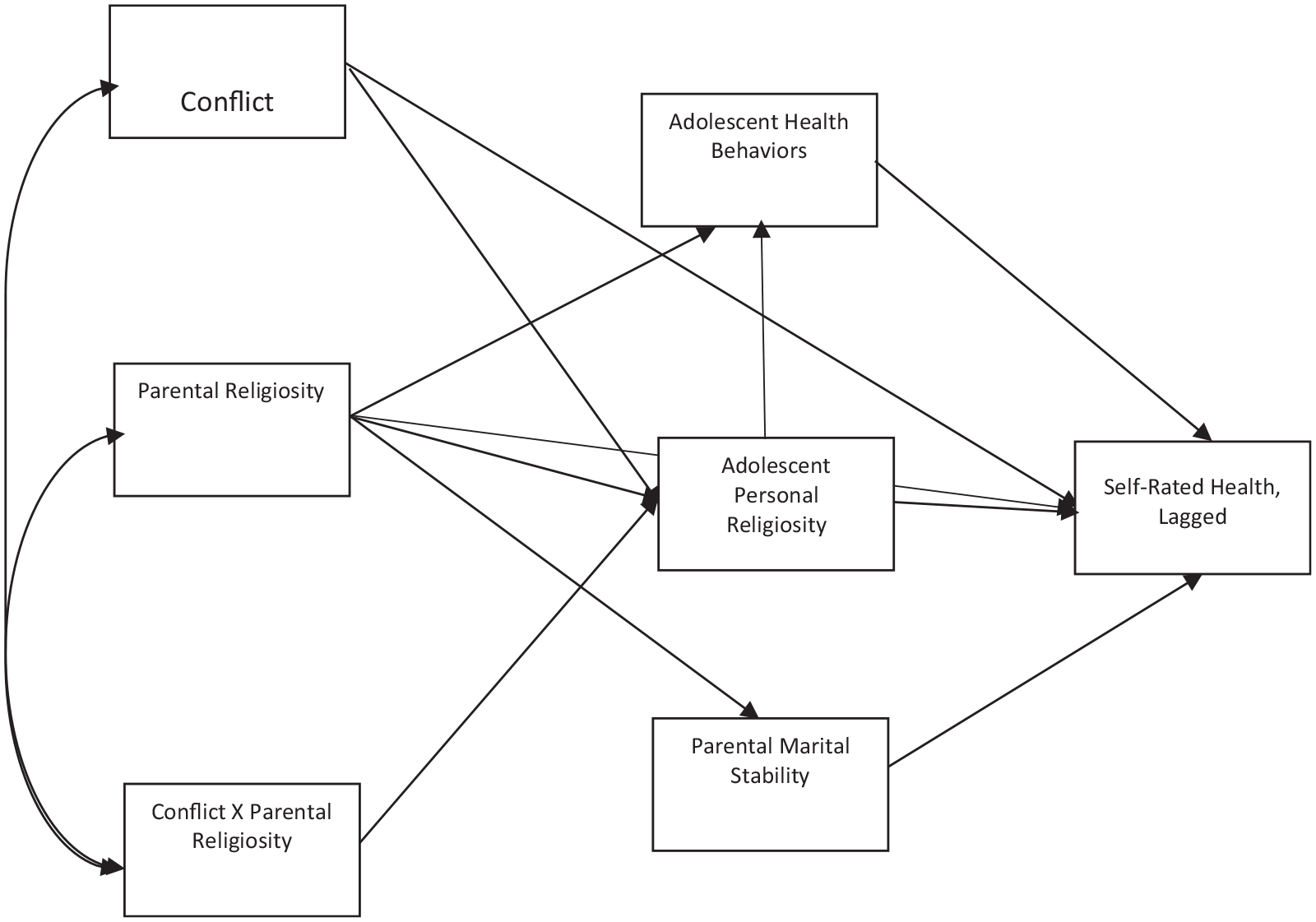
Combined full model.
After I test the religious socialization model, I fit a revised religious socialization model with only the significant direct and indirect effects from the full religious socialization model. Following the estimation of this revised religious socialization model, I estimate the full health-related behaviors model, which includes the significant direct and indirect effects from the revised religious socialization model as well as the measures of health-related behaviors. I test H3 utilizing the full health-related behaviors model. A revised health-related behaviors model will be estimated utilizing the significant direct and indirect effects from the full health-related behaviors model. To test H4, I estimate the full marital stability model consisting of the direct and indirect effects of the revised health-related behaviors model as well as the measures of marital stability. Finally, if there is evidence of marital stability mediating the association between parental religiosity and lagged self-rated health, a final revised marital stability model will be estimated with the significant direct and indirect effects from the full marital stability model.
Several measures are utilized to assess the “fit” of each of my models. I utilize a chi-square test to assess the difference between the implied covariance matrices of my models and the observed covariance matrix of the sample. A chi-square statistic that is close to zero and a nonsignificant p value indicate a better fit (a smaller difference between implied and observed covariance matrices). However, with large samples it is unlikely that a nonsignificant p value is obtained. Therefore, in addition to the chi-square test, I utilize three other measures of model fit that are less affected by sample size. The standardized root mean square residual (SRMR) is the square root of the difference between the observed covariance matrix and the implied covariance matrices. It ranges from 0 to 1 with an SRMR ≤ 0.08 indicating an acceptable fit. The root mean square error of approximation (RMSEA) compares my models to the saturated model. Like the SRMR, the RMSEA ranges from 0 to 1. According to Robert C. MacCallum, Michael W. Browne, and Hazuki M. Sugawara (1996), an RMSEA of 0.01, 0.05, and 0.08 indicates an excellent, good, and mediocre model fit, respectively. A p value can also be calculated for the RMSEA to test the null hypothesis that the RMSEA is < 0.05. Rejecting the null indicates that the model is not a good fitting model. Finally, the comparative fit index (CFI) compares the χ2 of each of my models and the null model. The CFI ranges from 0 to 1 with a CFI > 0.90 indicating an acceptable fit and a CFI > 0.95 indicating a good fit.
Results
Table 1 presents the means and standard deviations for each of my continuous variables, percentages for each of my categorical variables, as well as the results of bivariate analyses between each variable and self-rated health. Table 1 reveals that just under half of the sample (47%) is male and the majority of the sample is white (52%). It also reveals that conservative protestant is the modal religious affiliation for both parents during wave I (31%) and adolescents during wave II (27%). Finally, Table 1 reveals that most parents (72%) during wave I were married and 37 percent of respondents live in the South.
Descriptive Statistics by Wave (N = 15,195).

Note. 95% confidence intervals in brackets. Standard error in parentheses.
p < .05. **p < .01. ***p < .001, two-tailed test.
Most of the bivariate analyses presented in Table 1 support what has been previously found in the literature. Bivariate analyses reveal that (1) parental and adolescent institutional and personal religiosity are positively associated with self-rated health; (2) negative health behaviors such as smoking have a negative association with self-rated health; and (3) positive health behaviors such as eating a healthy diet has a positive association with self-rated health. However, two findings that contradict previous literature are a positive association between parental alcohol use and self-rated health (β = 0.022, p = .042) and a nonsignificant association between number of sexual partners and self-rated health (β < 0.001, p < .976).
Table 2 presents the direct and indirect effects for the full religious socialization model. Table 2 reveals that the direct effects for parental personal religiosity and each measure of parental religious affiliation are nonsignificant. This finding supports H1, which posits that parental religiosity does not directly influence self-rated health. However, Table 2 also reveals a significant positive association between parental institutional religiosity and self-rated health, which contradicts H1, but only in the case of parental institutional religiosity. In addition, the findings revealed in Table 2 contradict H2, which posits that parental religiosity influences self-rated health indirectly via adolescent religiosity. Finally, the model fit statistics for Table 2 indicates that the full religious socialization model is a poorly fitting model (p value for chi-square test < .001; CFI = 0.850; RMSEA = 0.254, p < .001; SRMR = 0.125).
The Influence of Parental Religiosity on Lagged Self-rated Health Mediated by Adolescent Religiosity and Moderated by Parent-Child Conflict (Full Model) (N = 15,195).
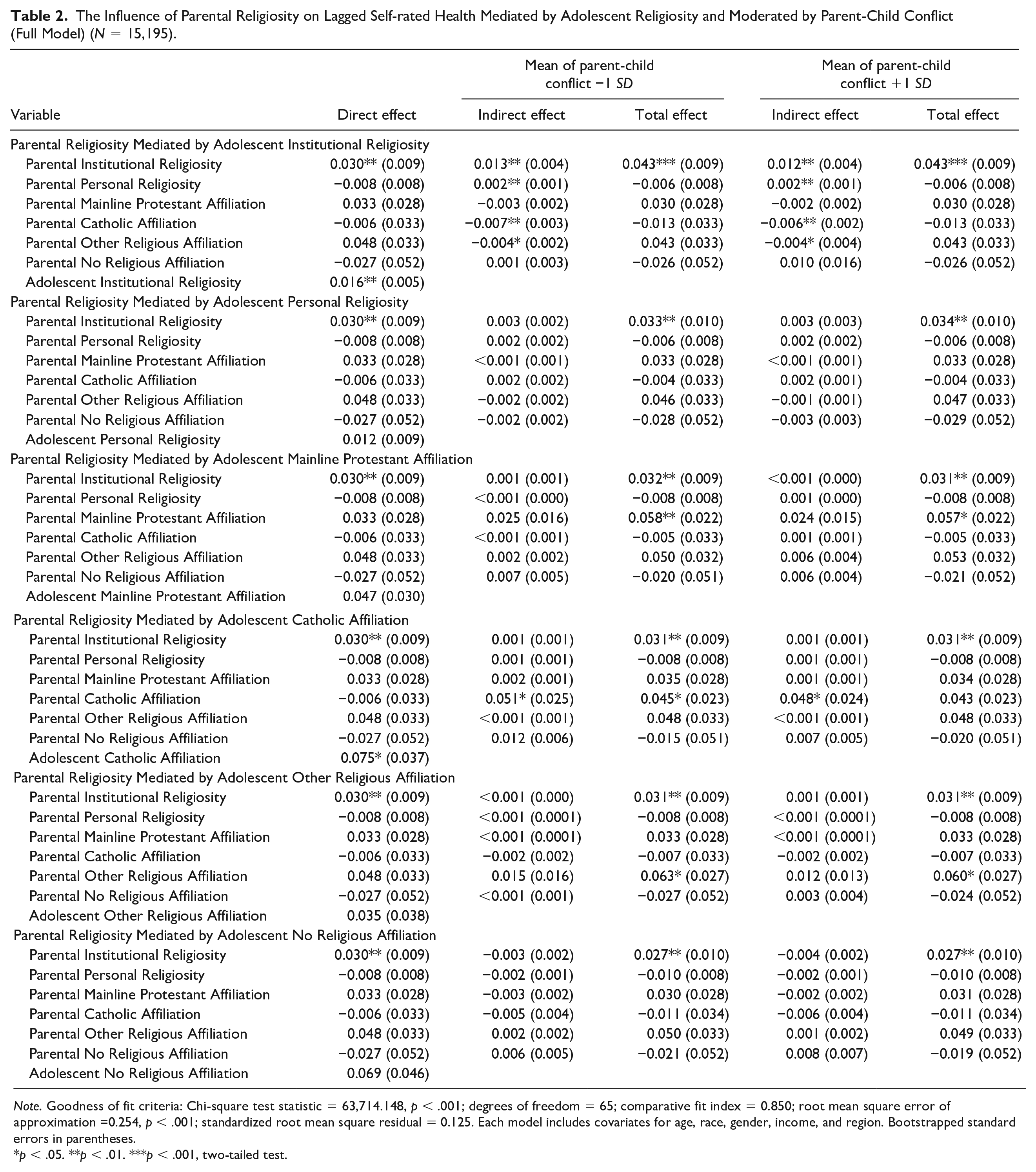
Note. Goodness of fit criteria: Chi-square test statistic = 63,714.148, p < .001; degrees of freedom = 65; comparative fit index = 0.850; root mean square error of approximation =0.254, p < .001; standardized root mean square residual = 0.125. Each model includes covariates for age, race, gender, income, and region. Bootstrapped standard errors in parentheses.
p < .05. **p < .01. ***p < .001, two-tailed test.
Table 3 presents the findings for the revised religious socialization model, which excludes nonsignificant associations from the full religious socialization models. This model is a slightly better fitting model than the full religious socialization model (p value for chi-square test < .001; CFI = 0.864; RMSEA = 0.158, p < .001; SRMR = 0.071), though it is also a poorly fitting model.
The Influence of Parental Religiosity on Lagged Self-rated Health Mediated by Adolescent Religiosity (Revised Model) (N = 15,195).
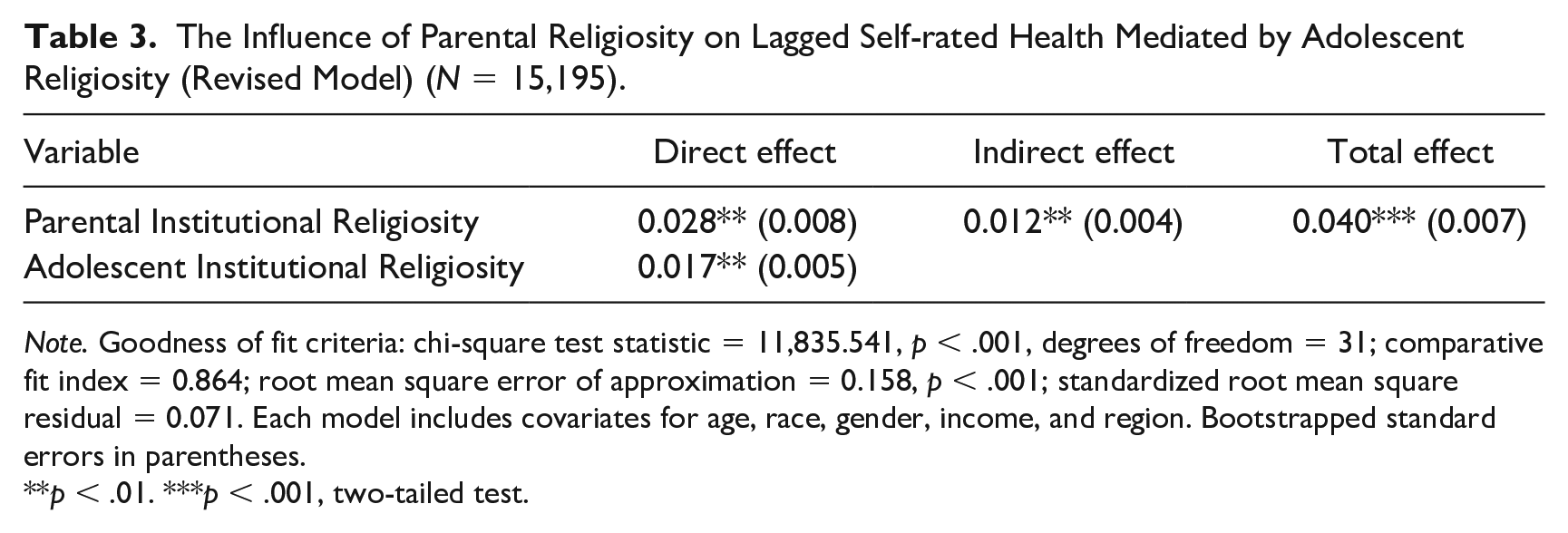
Note. Goodness of fit criteria: chi-square test statistic = 11,835.541, p < .001, degrees of freedom = 31; comparative fit index = 0.864; root mean square error of approximation = 0.158, p < .001; standardized root mean square residual = 0.071. Each model includes covariates for age, race, gender, income, and region. Bootstrapped standard errors in parentheses.
**p < .01. ***p < .001, two-tailed test.
Table 4 presents the direct and indirect effects for the full health-related behaviors model and reveals that the full health behaviors model has a much better model fit (p value for chi-square test < .001; CFI= 0.974; RMSEA = 0.051, p < .071; SRMR = 0.045) than the full and revised religious socialization model. Table 4 also reveals that parental institutional religiosity has both a positive and deleterious impact on lagged self-rated health. Specifically, parental institutional religiosity has a significant direct effect on lagged self-rated health (β = 0.019, p = .21) and significant indirect effects on lagged self-rated health via self-reported physical activity (β = −0.001, p = .025); self-reported adolescent smoking (β = 0.003, p = .005); self-reported parental smoking (β = 0.012, p < .001); and self-reported parental alcohol use (β = −0.003, p = .008).
The Influence of Parental Religiosity on Lagged Self-rated Health Mediated by Health-related Behaviors (Full Model) (N = 15,195).
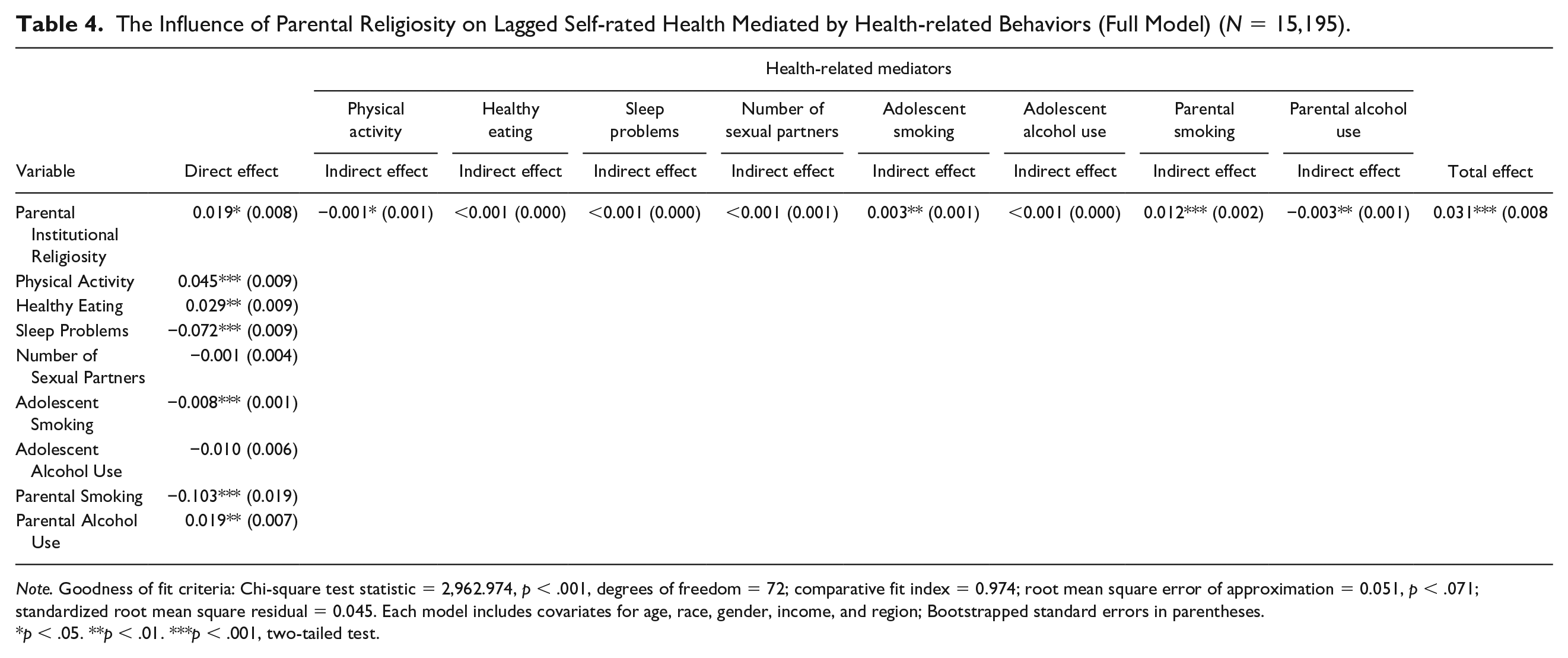
Note. Goodness of fit criteria: Chi-square test statistic = 2,962.974, p < .001, degrees of freedom = 72; comparative fit index = 0.974; root mean square error of approximation = 0.051, p < .071; standardized root mean square residual = 0.045. Each model includes covariates for age, race, gender, income, and region; Bootstrapped standard errors in parentheses.
p < .05. **p < .01. ***p < .001, two-tailed test.
Table 5 presents the findings for the revised health-related behaviors model, which excludes nonsignificant associations from the full health-related behaviors model. This model is also a good fitting model (p value for chi-square test < .001; CFI = 0.974; RMSEA = 0.044, p < 1.000; SRMR = 0.045), though it has the added advantage of being a more parsimonious model than the full health-related behaviors model.
The Influence of Parental Religiosity on Lagged Self-rated Health Mediated by Health-related Behaviors (Revised Model) (N = 15,195).
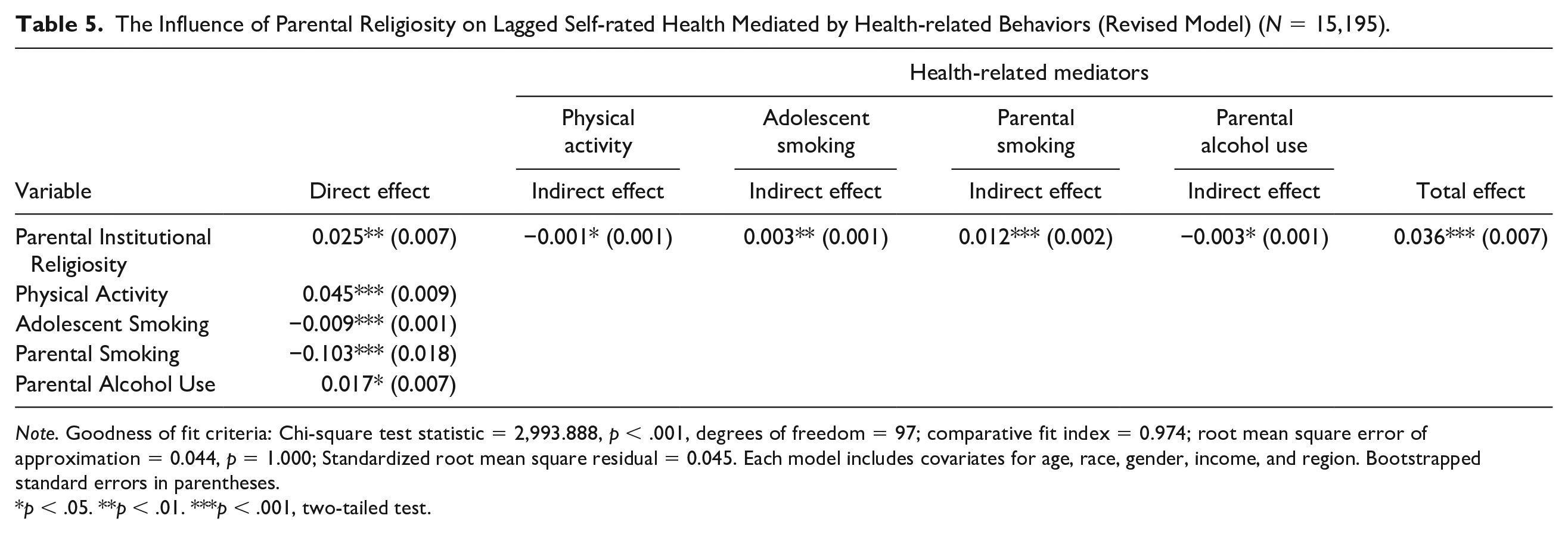
Note. Goodness of fit criteria: Chi-square test statistic = 2,993.888, p < .001, degrees of freedom = 97; comparative fit index = 0.974; root mean square error of approximation = 0.044, p = 1.000; Standardized root mean square residual = 0.045. Each model includes covariates for age, race, gender, income, and region. Bootstrapped standard errors in parentheses.
p < .05. **p < .01. ***p < .001, two-tailed test.
Finally, Table 6 reveals the direct and indirect effects of the full marital stability model. Table 6 reveals no evidence to support H4, which posits that parental religiosity has an indirect association with adolescent self-rated health via marital stability. All four of the measures of marital stability show a nonsignificant indirect effect. And while the martial stability model is technically the best fitting model (p value for chi-square test < .001; CFI = 0.975; RMSEA = 0.035, p = 1.000; SRMR = 0.040), the revised health-related behaviors model presented in Table 5 is a more parsimonious model and has model fit statistics that are very similar to the martial stability model. Therefore, the revised health-related behaviors is the best overall model to explain the association between parental religiosity and self-rated health during late adolescence/early adulthood.
The Influence of Parental Religiosity on Lagged Self-rated Health Mediated by Parental Marital Stability (Full Model) (N = 15,195).
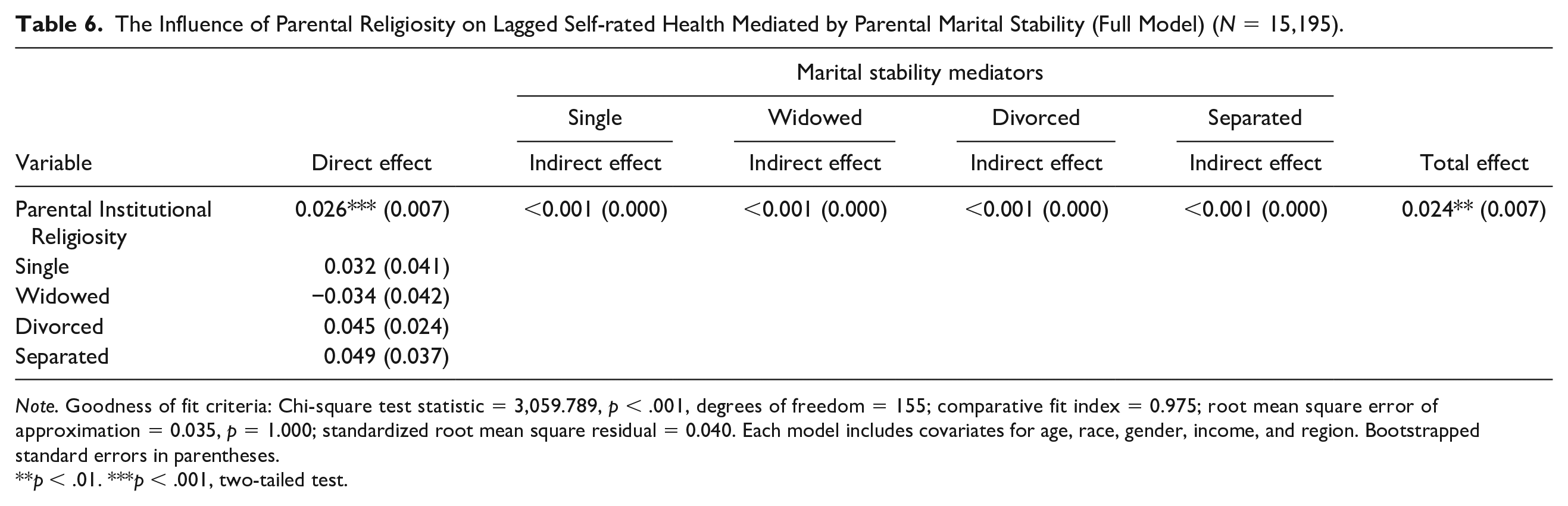
Note. Goodness of fit criteria: Chi-square test statistic = 3,059.789, p < .001, degrees of freedom = 155; comparative fit index = 0.975; root mean square error of approximation = 0.035, p = 1.000; standardized root mean square residual = 0.040. Each model includes covariates for age, race, gender, income, and region. Bootstrapped standard errors in parentheses.
**p < .01. ***p < .001, two-tailed test.
Figure 3 illustrates the revised health-related behaviors model. Figure 3 reveals that parental institutional religiosity improves self-rated health during late adolescence/early adulthood by reducing parental and adolescent smoking, while simultaneously diminishing self-rated health by decreasing physical activity and increasing parental alcohol use.
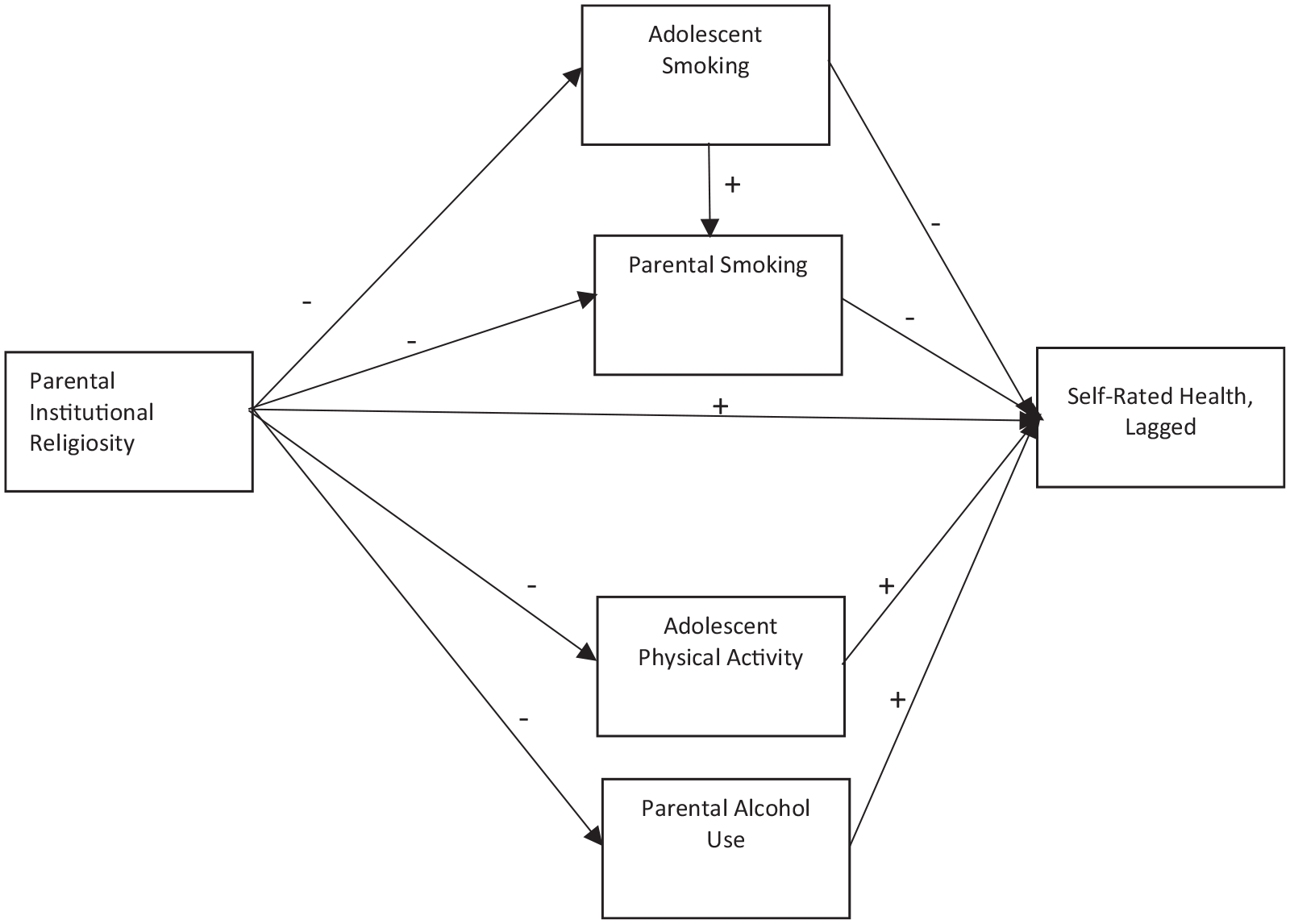
Revised health-related behaviors model.
Discussion
Despite a large body of research exploring the association between religiosity and health, only a few studies have explored whether parental religiosity can influence health of adolescent children. The present study explores whether three measures of parental religiosity (i.e., parental institutional religiosity, parental personal religiosity, and parental religious affiliation) indirectly influence the self-rated health of children during late adolescence/early adulthood via adolescent religiosity, adolescent health-related behaviors (e.g., healthy eating, substance use), and marital stability. I tested four hypotheses, which are parental religiosity does not have a direct influence on adolescent self-rated health (H1); parental religiosity influences adolescent self-rated health indirectly via adolescent religiosity (H2); religious parents influence adolescent self-rated health by increasing the likelihood of engaging in healthy behaviors and reducing the likelihood of engaging in unhealthy behaviors (H3); and parental religiosity has an indirect association with adolescent self-rated health via marital stability (H4). My finding partially supports H1, H2, and H3. However, support for the H2 disappears once health-related behaviors are included in the model.
In regard to H1, I found that parental institutional religiosity directly influences self-rated health during late adolescence/early adulthood, even when I control for adolescent religiosity (as well as health-related behaviors, martial stability, and covariates). This finding supports the findings of Merrill et al. (2005) and Caputo (2004) who found a direct influence of parental religiosity on health. This also supports the idea put forward by Smith (2003) that religiosity has a direct influence on individual outcomes. The direct influence of parental institutional religiosity may be due to internalized moral beliefs linked to parental religiosity. For example, religious parents may be more likely to espouse “traditional” norms that see unhealthy habits such as smoking as a sign of weak character. They may feel that unhealthy habits are not acceptable for the children of churchgoing parents. Alternatively, the influence of parental religiosity on self-rated health may be due to selection effects, where underlying traits (e.g., neuroticism, objective health measures, and genetic proclivity toward risk-taking behaviors) create the appearance of a positive association. Finally, the persistence of a direct influence of parental institutional religiosity on self-rated health during adolescence/early adulthood may also indicate the need for better theories to explain the association between parental religiosity and self-rated health during adolescence/early adulthood.
In regard to H2, I found a significant indirect effect of parental institutional religiosity on adolescent self-rated health via adolescent religiosity. However, the direct influence of adolescent religiosity on self-rated health disappears once health-related behaviors are included in the model. This indicates that the influence of adolescent religiosity on self-rated health is mediated by the influence of health-related behaviors.
In regard to H3, parental institutional religiosity improves self-rated health during late adolescence/early adulthood by reducing parental and adolescent smoking. This finding supports both social learning and social control theoretical explanations for the connection between parental religiosity and adolescent health. It is likely that religious parents reduce adolescent smoking by modeling lower rates of parental smoking or smoking abstinence, and also sanction adolescents for smoking, which leads to improved health during late adolescence/early adulthood.
In addition to parental institutional religiosity improving self-rated health during late adolescence/early adulthood, it also diminishes self-rated health by reducing physical activity during adolescence. The inverse association may be due to the fact that the amount of time utilized to participate in religious services reduces the amount of time available to engage in physical activities such as jogging or bike riding. One anomalous finding is that parental institutional religiosity has a deleterious influence on self-rated health during late adolescence/early adulthood by reducing parental alcohol use, which is positively associated with self-rated health. The positive association between parental alcohol use and self-rated health during late adolescence/early adulthood may be due to endogeneity—bias due to the influence of unobserved factors. One potential source of this endogeneity are genetic factors that influence both parental alcohol use and self-rated health. Studies find that both alcohol use (Verhulst, Neale, and Kendler 2015) and self-rated health (Romeis et al. 2000) are heritable—meaning that variation in these factors may at least partially be due to genetic factors. Genetic factors that increase alcohol use and improve self-rated health may create what appears to be a positive association between parental alcohol use and self-rated health. However, this is only speculation. Further study would be required to identify the specific unobserved factors that explain the positive association between parental alcohol use and self-rated health during late adolescence/early adulthood.
Finally, I found that parental institutional religiosity does not influence self-rated health during late adolescence/early adulthood via parental marital stability. Like adolescent religiosity, parental marital stability may influence self-rated health via health-related behaviors. For example, children of divorce are more likely to smoke than the children of intact families (Fuller-Thomson, Filippelli, and Lue-Crisostomo 2013). Therefore, including smoking behaviors in the models may account for much of the influence parental marital status has on self-rated health.
Limitations
While the present study fills a gap in the literature regarding the association between parental religiosity and health, several limitations should be noted. First, while adolescent institutional religiosity is measured as both attendance at religious services and participation in religious activities, parental institutional religiosity is measured only as attendance at religious services. While ideally, multiple measures of each dimension of religiosity should be used, I would argue that for adults the main interaction with religious institutions would be attendance at religious services. However, for adolescents religious youth groups may be a major source of interaction with religious institutions in addition to attendance at religious services.
A second weakness of this study is the low Cronbach’s alpha for adolescent personal religiosity, healthy eating, and physical activity measures. While Cronbach’s alpha for parental personal religiosity was rather high (α = .86), the low Cronbach’s alpha for adolescent personal religiosity may be a result of prayer being compulsory within some households. If prayer is not a choice, then an individual’s frequency of prayer may not be related to his or her level of religious salience. The low Cronbach’s alpha for the self-reported healthy eating measure may be due to the fact that unhealthy foods may be included among breads and cereals (e.g., pretzels) and dairy (e.g., ice cream), but this is less likely for fruits and vegetables. Similarly, the low Cronbach’s alpha for the self-reported physical activity measure may be due to the disparate types of physical activity (e.g., walking, football, jumping rope, gymnastics included in the measure) that are not typically correlated.
Directions for Future Research
The findings of the present study logically lead to several future directions for research on the association between parental religiosity and adolescent health. First, future studies should explore variation in the link between parental religiosity and adolescent health. While the present study shows a variety of linkages between parental religiosity and various measures of adolescent health, these linkages may vary across gender categories, social class, racial groups, or religious groups. For example, in groups where attendance at religious services is compulsory (e.g., the Amish), there may be very few (or no) individuals who do not attend religious services. In those circumstances, any connection between parental attendance at religious services and adolescent health may be due to some underlying factor such as significant disability of the adolescent preventing parents from regularly attending religious services, rather than the salubrious impact of attendance at religious services on health. Alternatively, among religious groups where attendance at religious services is not considered a major aspect of religious commitment, such as some Jewish groups, there may be little or no association between parents attending religious services and the health of their adolescent children.
Second, future studies should investigate potential variation in the paths linking parental religiosity and health. For example, parental religiosity may reduce risk of cardiovascular disease by reducing blood pressure. Concurrently, parental religiosity may reduce an individual’s cancer risk by improving immune function. However, the absence of an influence of parental religiosity on cardiovascular health does not necessarily negate the influence of parental religiosity on cancer risk.
Finally, future research should explore whether the religiosity of other “significant others” within the adolescent’s environment has influence on their health. The current study reveals that parental institutional religiosity influences an individual’s health by decreasing their likelihood to smoke. At least one other study has found that the religiosity of peers also decreased an individual’s likelihood to smoke (Bahr and Hoffmann 2008). Future research should explore whether the religiosity of other relatives (grandparents, aunts, siblings, etc.) and/or the role models an adolescent chooses to follow (e.g., movie stars, famous athletes) have a similar impact on adolescent health by reducing substance use.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.