
Abstract
Being identified with a learning disability makes students vulnerable to experiences of stigmatization, which can be associated with negative academic and emotional effects. Yet, research with other vulnerable populations demonstrates that individual perceptions of stigmatization, or stigma consciousness, are not uniform and that variability in stigma consciousness is more predictive of outcomes than assuming all members of the group are similarly affected. We present here a measure that enables consideration of such individual experiences of stigma consciousness specifically designed and tested with adolescents with learning disabilities (N = 42). We demonstrate that the Stigma Consciousness Questionnaire–Learning Disabilities (SCQ-LD) is reliable, valid, and usable with this population. Furthermore, we demonstrate that variability in stigma consciousness is present. Results support the use of this construct and measure to contribute to our understanding of the individual experiences of students in this population.
In a nationally representative public opinion poll, 50% of the general public agreed or strongly agreed with the statement that learning disabilities (LD) was a term often used to describe a condition that could really be called laziness (Roper Public Affairs & Corporate Communications, 2010). In the same poll, more than half of the public, a similar number of parents, 43% of teachers, and 31% of educational administrators believed LD were often caused by conditions at home. Furthermore, one in five members of the public did not believe that children with LD were “just as smart as you and me.” How do young people with LD experience these societal perceptions? To what degree do they experience stigmatization due to these negative views from the culture at large, and from parents, teachers, and administrators in their schools?
Prior research with large, national data sets has demonstrated that the presence of stigma associated with the LD label is likely to adversely affect educational expectations and academic outcomes, over and above the influence of specific academic deficits for this population as a whole (Crosnoe, Riegle-Crumb, & Muller, 2007; Shifrer, 2013). In addition, numerous, largely qualitative, studies have demonstrated negative emotional experiences associated with having a LD (Al-Yagon, 2015; Feurer & Andrews, 2009; Lackaye, Margalit, Ziv, & Ziman, 2006; Maag & Behrens, 1989; Margalit, 1991; Margalit & Raviv, 1984; Wiener & Daniels, 2016). In the set of articles to emerge from the landmark longitudinal Frostig Center study, stigma and awareness of “differentness” were found to play significant roles in the developmental experiences of many individuals with LD (Higgins, Raskind, Goldberg, & Herman, 2002). Although this research—from both the bird’s-eye and on-the-ground perspectives—makes clear the potential role of stigma in the academic and broader lived experiences of young people with LD, nuanced understanding of stigma’s influence has been hampered by lack of an appropriate construct and measurement approach to untangle individual experiences from trends in the population at large. Direct measurement of students’ experiences of stigma can provide a needed view of the dynamics of stigma from the perspective of the student (Shifrer, 2013).
Moving beyond considering stigmatized groups, and instead having a means to investigate individual experiences of stigma has been powerfully explanatory in reconciling discrepant findings about social, emotional, and academic effects of stigma with other stereotyped populations (Pinel & Bosson, 2013). The goal of the work we report here was to develop, pilot test, and validate such a measure to assess stigma consciousness among adolescents with LD. We view this as foundational work to advance the field’s capacity to investigate the role of stigma in students’ developmental and educational experiences and outcomes.
Stigmatization
For members of stigmatized groups, experiences with prejudice and discrimination are often pervasive and can range from acts of overt hostility and rejection to subtle insults and slights (Link & Phelan, 2006). Stigmatization occurs when perceived differences between an individual or group and other members of society lead to labeling, stereotyping, separation, loss of status, and discrimination (Link & Phelan, 2001).
As Shifrer (2013, 2016) has articulated and we revisit here, students with LD are vulnerable to each of the five elements of stigma. Labeling theory has made clear that formal labels, like those assigned through the diagnosis and special education identification process for LD, hold influence by changing one’s own and others’ perceptions of individuals assigned that label (Higgins et al., 2002; Link, Cullen, Struening, Shrout, & Dohrenwend, 1989; Mehan, Hertweck, & Meihls, 1986). Labeling has the unfortunate consequence of allowing for the creation of stereotypes. The term “learning disability” is associated with socially devalued traits including laziness, carelessness, or stupidity (Mackelprang & Salsgiver, 1996; Morrison & Cosden, 1997; Orenstein, 2000; Riddick, 2001). Students with LD often report feelings of shame or humiliation and actively conceal their disability among peers and teachers so as to avoid association with negative stereotypes (Miller & Kaiser, 2001; Smart & Wegner, 1999).
Furthermore, educational experiences of students with disabilities commonly involve separation from peers (Green, Davis, Karshmer, Marsh, & Straight, 2005) and loss of status. Studies in an array of contexts and from a variety of perspectives have made clear the challenges in social adjustment of young people with LD (for a review, see Al-Yagon & Margalit, 2013). Peer rejection and loneliness are likely (e.g., Al-Yagon, 2007; Estell et al., 2008; Feldman, Davidson, Ben-Naim, Maza, & Margalit, 2016; Margalit & Levin-Alyagon, 1994), and separation and loss of status may be particularly prone to co-occur in this population, with those in less inclusive educational settings experiencing more significant social challenges (Wiener & Tardif, 2004).
The final condition of stigmatization, discrimination, is similarly well documented among students with LD, with increased risk of overt discrimination like bullying (Mishna, 2003; Rose, Monda-Amaya, & Espelage, 2011) and the tendency for teachers to view students more negatively when told they have a LD (Fogel & Nelson, 1983; Meltzer, Katzir-Cohen, Miller, & Roditi, 2001). For example, elementary-aged students with LD perceive that their teachers are more rejecting, compared with perceptions of their typically developing peers (Al-Yagon & Mikulincer, 2004), and they are more likely than peers to believe other students in their schools are prejudiced against them (Svetaz, Ireland, & Blum, 2000).
Stigma Consciousness
Overall, the population of students identified with LD tends to satisfy these conditions for stigmatization; however, the experience of stigma is not uniform within a stereotyped group (Link & Phelan, 2014; Pinel, 1999; Pinel & Bosson, 2013). Instead, “individuals’ perceptions of the probability of being stereotyped” (Pinel, 1999, p. 114), their stigma consciousness, vary, and this variation is associated with differences in the degree to which stigma and stereotypes have a negative impact. Just as there has been a focus on understanding heterogeneity in the nature of learning and social-emotional challenges within the LD population (e.g., Backenson et al., 2015; Szűcs, 2016; Wolf & Bowers, 2000), experiences of stigma are similarly not uniform. This was apparent in a 20-year study by Higgins and colleagues (2002), in which many adult participants described lingering effects of discrimination and stigma from childhood, although others described early acceptance of their LD and lack of concern for others’ views. Enhancing understanding of this variability provides the greatest opportunity to identify aspects of the educational environment that are most likely to create stigma, to inform reform and effective intervention for individuals.
Stigma consciousness focuses on the belief that others see you in light of the stereotype about your group, regardless of actual behavior. In the case of students with LD, this consciousness would reflect an expectation that others primarily think of you in light of the negative attributes of all students with LD, even if you have not internalized those attributes. A ninth grader with LD might believe that others see students with LD (including himself) as lazy, even if he does not consider himself lazy.
Studies with other populations for which the conditions of stigmatization are evident demonstrate variability in impact of stigma based on stigma consciousness (Brown & Lee, 2005; Brown & Pinel, 2003; Link & Phelan, 2001). Individual differences in stigma consciousness are associated with poorer academic performance among women and racial minorities, particularly in academic situations that are likely to be threatening due to stereotypes (Brown & Lee, 2005; Brown & Pinel, 2003). Combined with other measures like sense of belonging, stigma consciousness is likely to predict outcomes like staying in a discipline (Good, Rattan, & Dweck, 2012), and individuals high in stigma consciousness may be less confident that any academic success truly represents potential, and more likely to expect others to view all of their behaviors in terms of the stereotype for their group (Cokley et al., 2015).
Measuring Stigma Consciousness: The Stigma Consciousness Questionnaire (SCQ)
Stigma consciousness has been studied in more than 200 previous projects, primarily using and adapting a self-report measure developed by Pinel in 1999: the SCQ. In the original work to develop and validate the SCQ, Pinel began with a version designed to measure stigma consciousness among women and adapted it to be used to assess stigma consciousness related to homosexuality and race (e.g., Bazemore, Janda, Derlega, & Paulson, 2010; Bean, Covarrubias, & Stone, 2014; Brown & Lee, 2005). The measure includes 10 items that ask respondents to indicate level of agreement with statements about how much they expect to be stereotyped. The statements can be adapted by changing target phrases. For example, Pinel (1999) adapted an item that originally read, “When interacting with men, I feel like they interpret all my behaviors in terms of the fact that I am a woman,” to “When interacting with heterosexuals who know of my sexual preference, I feel like they interpret all my behaviors in terms of the fact that I am a homosexual.” This type of simple modification was not expected to be sufficient for use with our target population, but the SCQ would serve as a strong foundation for measure development.
Several qualities make the SCQ a useful starting point for developing a measure to assess stigma consciousness among adolescents with LD: (a) The SCQ demonstrates strong internal consistency and evidence that stigma consciousness is a single, unique construct. In the initial development study (Pinel, 1999), Cronbach’s alpha was between .64 and .84 for the measures with different groups, with most above .75, and items consistently loaded on a single factor. This consistency has held up across subsequent studies. (b) The measure demonstrates stability across time, with test–retest reliability of r(42) = .76, p < .001 (Pinel, 1999). This suggests that stigma consciousness reflects a relatively consistent perception of the likelihood of being stereotyped, regardless of intermittent fluctuations or group membership–related events. (c) External validity is demonstrated through strong positive correlation with overall self-consciousness. Individuals who are more generally self-conscious also tend to have higher levels of stigma consciousness (Pinel, 1999), indicating a consistent tendency to be concerned with and aware of the views of others. (d) External validity is further demonstrated through negative correlation with measures of self-concept or self-perception (Pinel, 2004; Pinel & Bosson, 2013; Pinel, Warner, & Chua, 2005). We sought to develop a measure with these core properties that could be effectively administered to participants with a wide array of reading levels and with different understandings of their LD.
The Present Study
It is clear that the population of students with LD, overall, is vulnerable to the negative effects of stigmatization. What has been lacking is a means for directly investigating individual differences in the experiences of stigma within the population; such variation has proven critical in understanding the effects of stigma in other stereotyped populations. We present here a study to develop and validate a measure of stigma consciousness called the Stigma Consciousness Questionnaire–Learning Disabilities (SCQ-LD), particularly for adolescents with LD.
The focus on adolescents is purposeful. Younger students are less vulnerable to the stresses associated with membership in a stereotyped group (Good, Aronson, & Inzlicht, 2003), and school climate becomes a more potent influence in middle school and beyond (Anderman, 2003). Comparatively less research has focused on the social-emotional experience of students with LD in adolescence versus at younger ages despite cause for concern about the emotional health of this population (Al-Yagon, 2015, 2016). Developing a measure appropriate for this age range was considered most critical and aligns with the age-group focus in prior studies of stigma consciousness.
In pursuing the validation process to demonstrate the standards described above, we hypothesized the following:
In addition, we considered it critical that our measure incorporate the input of our target population, both in regard to its ability to accurately capture their lived experiences and ease of understanding and administration. The development of the measure was the target of an initial study, and this measure was then formally pilot tested to consider our hypotheses in a second study. This work focuses on four research questions, with the first being addressed in Study 1, and Questions 2 to 4 in Study 2:
Method
The SCQ-LD was developed through a process of progressive refinement and testing. Initial development of the measure involved adapting questions from the SCQ (Pinel, 1999), and two phases of pilot testing. After revisions, we then conducted a more robust study to determine reliability and validity of the SCQ-LD.
Site and Participants
In Table 1, we summarize the characteristics of participants in all three phases of research: two initial phases of iterative development (Study 1) and the full piloting of the new measure (Study 2). All participants were from urban and suburban areas in the northeastern United States. The first phase of development in Study 1 included six students (two boys and four girls) identified by their schools as having a specific LD, per the categories in federal special education legislation. Participants included two students in each of ninth, 10th and 11th grades at a single public comprehensive high school. LD status was determined based on review of each student’s individualized education program (IEPs), with confirmation from parent report. The second phase of Study 1 focused on testing a revised version of the SCQ-LD and the other measures to be used in Study 2. Ten students (four boys and six girls) who were identified by school administrators as having a specific LD were recruited from a second large high school.
Demographic Characteristics of Participants in Each Study Phase.
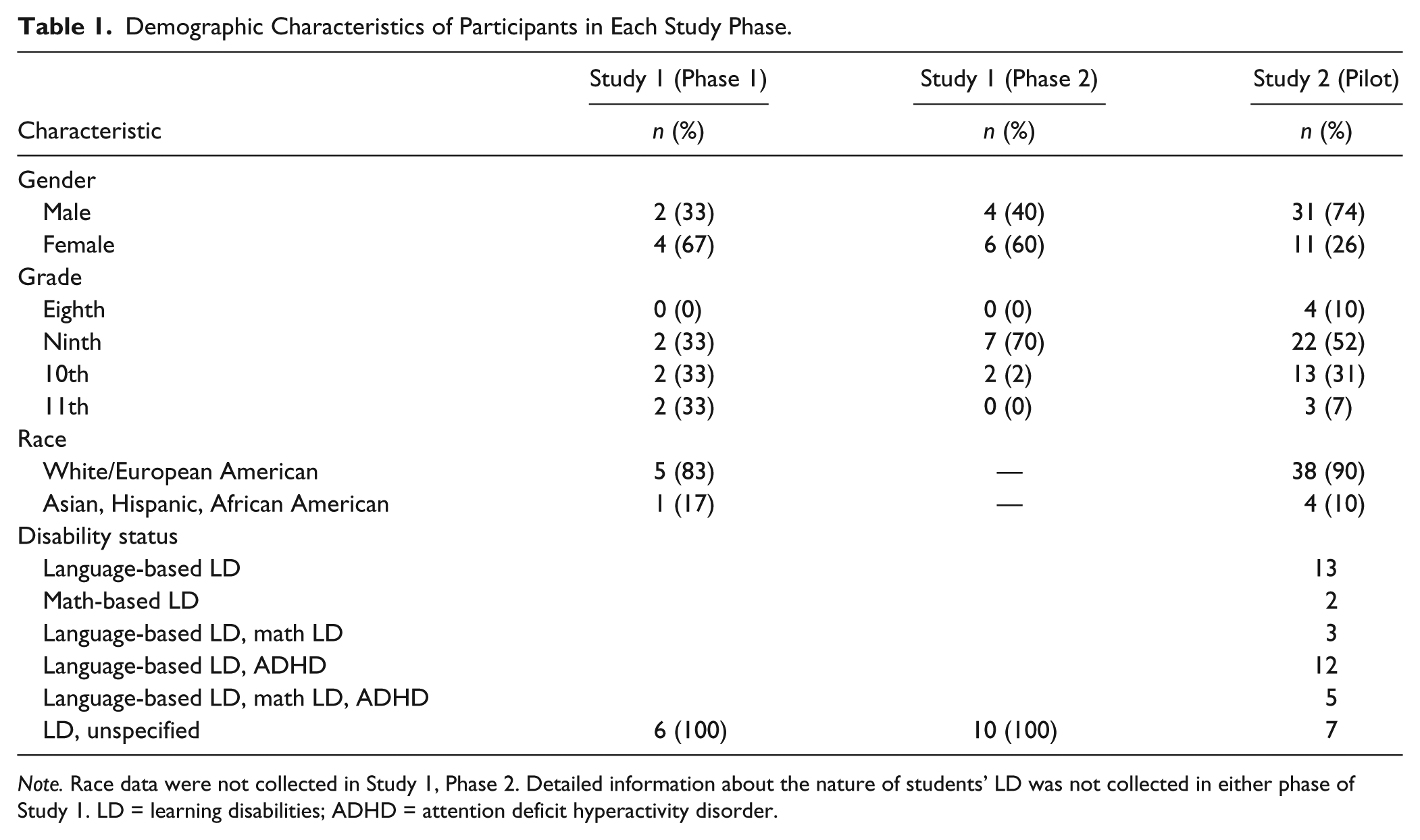
Note. Race data were not collected in Study 1, Phase 2. Detailed information about the nature of students’ LD was not collected in either phase of Study 1. LD = learning disabilities; ADHD = attention deficit hyperactivity disorder.
Study 2, the more formal pilot testing, included 42 eighth- through 11th-grade students (31 male, 11 female). As in Study 1, students were identified by their schools as having a specific LD, per the categories in federal special education legislation. Most of the students in the sample (35 of 42 participants) were enrolled at private schools that restrict admission to students with this diagnosis. Including such a large proportion of specialized school students poses limitations in terms of the generalizability of the findings regarding prevalence of stigma consciousness, as described more fully in the “Discussion” section, but the stringent requirements for enrollment in these schools that serve only students with language-based LD indicate that students reliably meet the criteria for the diagnosis of specific LD.
As described in Table 1, the sample was predominantly White (90%), and all students in the sample were native English speaking. Seventy-four percent of participating students (n = 31) provided access to psychoeducational testing histories. Among this portion of the sample, all had average or above-average full scale intelligence quotient (M = 100, SD = 11.5). The specific nature of the learning challenges varied, with language-based deficits being most prevalent, as is the case in the population. Twenty-seven students were specifically identified by their schools as having dyslexia. Seventeen students had diagnoses of both LD and attention deficit hyperactivity disorder (ADHD), but students with other disabilities were excluded from the study. No students in the sample had diagnoses related to social or emotional challenges. This narrowed the sample to those students for whom experiences of stigma related to a LD were not likely clouded by other stigmatizing disability-related conditions. The specific nature of the LD was expected to be less critical in this research than in other LD-focused work because it is the label that was expected to be salient in the experience of stigma rather than the specific academic challenges. This is similar to the Higgins et al. (2002) findings in which the social and emotional effects of the LD were unrelated to the nature or severity of the difficulty.
Measures
The primary measure was the SCQ-LD, the development and final version of which is described in the “Results” section below. To address Research Question 3 about the relationship between this new measure and existing validated measures, we also administered the Self-Consciousness Scale for Children (SCS-C; Higa, Phillips, Chorpita, & Daleiden, 2008) and the widely used Self-Perception Profile for Learning Disabled Students (Harter, 2012). The SCS-C was used to test the hypothesized positive relationship between stigma consciousness and concern about self, relative to the thoughts and feelings of other people. The SCS-C is a 19-item self-report measure requiring respondents to rate on a 5-point scale (1 = strongly disagree; 5 = strongly agree) aspects of their personality (e.g., “I care about the way others think I look”). It has strong internal consistency (Cronbach’s α = .86) and was purposefully developed for use with this age group. The Self-Perception Profile for Learning Disabled Students (Harter, 2012) was used to measure self-perception, which was expected to be negatively associated with stigma consciousness on the SCQ-LD. This 15-item self-report measure asks students to indicate perceptions of themselves along several dimensions: global self-worth, intellectual ability, and social competence. Responses indicate how “true for me” descriptions of teens are (e.g., “Some teens are sure they are pretty smart in school. But other teens are not so sure they are all that smart in school.”). Reliability, reported via Cronbach’s alpha, is strong across subscales (global self-worth = .83; intellectual ability = .81; and social acceptance = .81).
Procedure
Study 1
To develop the SCQ-LD, we adopted a process of progressive refinement that leveraged both expertise from the field and input from students with LD. To begin adapting the SCQ, we first used the simplest approach of replacing key phrases about the population. For example, the original phrase “woman” is replaced with a phrase describing the group under investigation (e.g., “person with a learning disability”). After this first step, we leveraged formative feedback from our advisory board. The four-member group included one leader in research in LD who is a past president of the Division for Learning Disabilities and past chairperson of the National Center for Learning Disabilities’s professional advisory board, one pediatrician who directs a clinic that assesses and supports students with LD, one expert in emotional development of adolescents in marginalized populations, and one leading researcher in stigma and stereotype threat. Together, we noted several challenges around readability, understanding, and accessibility using this simple method.
Further revision of the SCQ-LD resulted in a version that we tested with the six students described in Phase 1 above. For this initial work, researchers met participants at their school in a private room. Student participants were asked to complete the SCQ-LD through an online survey program that read items aloud through headphones, while the researcher sat nearby. This procedure was selected to mitigate concerns about reading challenges affecting understanding of the items and to provide a private means of responding to items without having to voice responses to the researcher. This procedure was deemed effective and was used in all subsequent phases of the research. Researchers then engaged participants in a semi-structured, qualitative interview addressing readability, understanding, accessibility, and usability.
The SCQ-LD was revised again to incorporate feedback and address challenges. In the second phase of Study 1, 10 students met individually with researchers to complete the revised SCQ-LD, administered in a similar fashion as in the first phase, and also completed the SCS-C and Self-Perception Profile for Learning Disabled Students. Because the SCS-C and Self-Perception Profile for Learning Disabled Students were not validated for use with a computer interface, we administered these measures in paper-and-pencil form and read the questions aloud to all participants. This phase enabled us to again evaluate the study procedure and focus on internal consistency of the measure before the larger testing described in Study 2. Our advisory board again reviewed the revised version, and final changes were made based on their feedback to produce the version of the SCQ-LD used in Study 2.
Study 2
Data collection for the more substantial validation study took place over the course of two individually administered 45-min sessions, scheduled 4 to 6 weeks apart. Researchers met one-on-one with participants in a private room at their school. 1 All measures were administered in the first session. To assess test–retest reliability, the SCQ-LD was administered a second time (4 to 6 weeks after the first administration) under like conditions.
Results
Research Question 1: Is the Method for Revising the SCQ That Has Been Used in Previous Adaptations of This Measure Appropriate for a Focus on Adolescents With LD (Readability, Understanding, Accessibility)?
The first round of adaptation of the SCQ for students with LD revealed several critical challenges with the typical approach to adapting the SCQ. As described above, we adopted the simple replacement approach and sought to maintain person-first language. This approach was problematic for two reasons. First, the language of the survey became syntactically cumbersome. For example, the reverse-scored item “I almost never think about the fact that I am female when I interact with men” would become “I almost never think about the fact that I am a person with a learning disability when I interact with people without learning disabilities.” Similarly, a simple term to describe people who are prejudiced against individuals with LD does not exist. The item “I often think that men are unfairly accused of being sexist” had no straightforward translation for our target population. To respond to these challenges, each item was adjusted to maintain the intent of the original but to use more appropriate language and syntax. This resulted, for example, in changing “Most men have a lot more sexist thoughts than they actually express” to “Most people have negative views about kids with learning disabilities even though they don’t say them out loud.” The original item “I never worry that my behaviors will be viewed as stereotypically female” became “I never worry that people think I act like someone with a learning disability.”
After pilot testing, we identified two other challenges that required revision to the survey. First, we observed that all of the participants struggled with the usability of the survey. In particular, the number of response choices was unnecessarily complex, significantly slowing participants as they recorded their responses. To address this challenge, we revised the SCQ-LD to provide only four response options (strongly disagree, disagree, agree, strongly agree), removing the midpoint option and simplifying the scale from the original SCQ.
Second, we found that many students were unfamiliar with key terms on the SCQ-LD. Most notably, they were not consistently able to explain the word “stereotypes,” which was essential to understanding two of the items. We adjusted the language of these items to convey the intent of the original without relying on this vocabulary. In addition, we found substantial variation in students’ definitions of the term “learning disability.” We ultimately decided to keep this as the focal term (instead of “learning difference,” or “learning difficulty”) because of a desire to focus on the potential stigma associated with the label itself, but we sought a means to capture differences in interpretation. This led to the addition of two open-ended questions at the beginning of the measure: “What does having a ‘learning disability’ mean to you?” and “In your experience, what do you think most people think about kids with learning disabilities?” This gave respondents an opportunity to voice their understandings and experiences and added contextual depth to future findings.
The final SCQ-LD used in Study 2 (see Table 2 for SCQ-LD items) consisted of 17 self-report items, administered via computer with consistent read-alouds. This version included two open-response items and 15 statements describing concerns about judgments other people may make about individuals with LD; respondents indicated their level of agreement with each statement, from 1 (strongly disagree) to 4 (strongly agree).
The SCQ-LD Items, Their Means and Standard Deviations, and Factor Loadings for Exploratory Factor Analysis With Varimax Rotation.
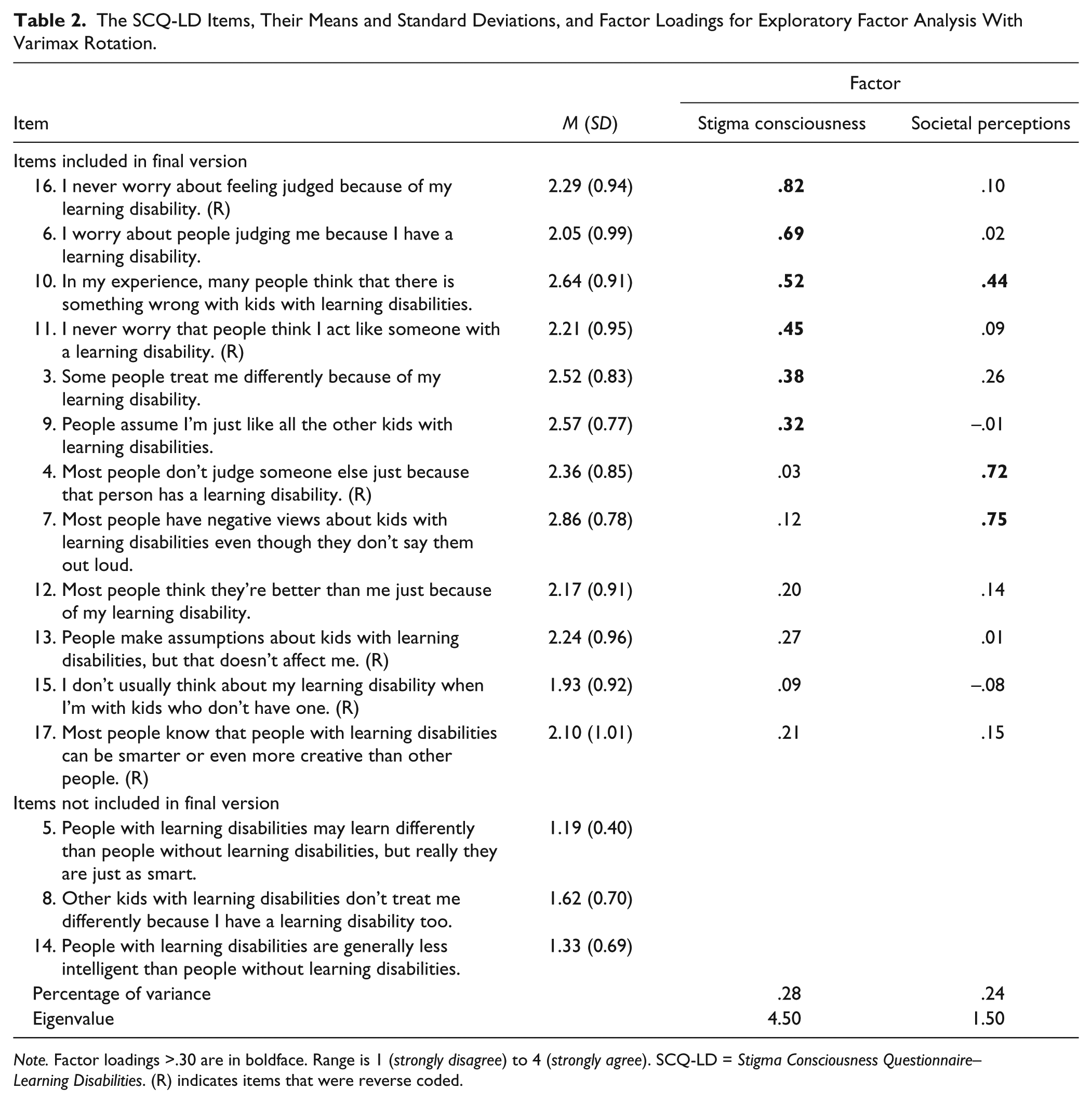
Note. Factor loadings >.30 are in boldface. Range is 1 (strongly disagree) to 4 (strongly agree). SCQ-LD = Stigma Consciousness Questionnaire–Learning Disabilities. (R) indicates items that were reverse coded.
Research Question 2: Do Tests of Reliability of the SCQ-LD (Internal Consistency, Factor Analysis, and Test–Retest) Indicate a Single, Stable Construct of Stigma Consciousness?
Initial analysis of the psychometric properties of the SCQ-LD focused on calculating Cronbach’s alpha with the 15 quantitative items. Three items (five, eight, and 14; see Table 2) were notably discrepant from the others. Correlations between each of these items and the rest were negative or zero. After removing these items, Cronbach’s alpha was excellent at both Time 1 and Time 2 (.82 and .84, respectively), indicating high internal consistency.
We next conducted an exploratory factor analysis of the remaining 12 items, using the first administration for all participants. An exploratory factor analysis is appropriate to verify unidimensionality beyond Cronbach’s alpha because reliability can be high even when several dimensions are assessed by a given measure (Fabrigar & Wegener, 2012). We note that the sample size (N = 42) could be considered small for factor analysis. Guidelines around sample size in factor analysis typically do not consider the specific conditions, including the number of factors, how correlated they are with each other, and the method of rotation (Fabrigar & Wegener, 2012; MacCallum, Widaman, Zhang, & Hong, 1999). When these characteristics are considered, sample sizes for effective factor analysis can vary dramatically; with 12 items, our sample-to-item ratio is 3.5, within the range of 3 to 6 as recommended values (MacCallum et al., 1999). A relatively low ratio was considered appropriate here because we expected a single factor that would be overdetermined, and we expected high communality between items. High communality was indeed found in the analysis we describe next, with the final main factor demonstrating an average communality of .59, approximating the recommended guideline of .60 for small samples (Worthington & Whittaker, 2006).
Using varimax rotation and an orthogonal solution, as recommended to facilitate future replication of this initial validation study (Henson & Roberts, 2006), we hypothesized a single factor reflecting students’ overall level of stigma consciousness related to have a LD. Kaiser’s criterion instead suggested the presence of two factors (eigenvalues = 3.69 and 1.30). A scree test similarly suggested two factors. Both factors were conceptually interpretable, leading us to retain two factors that combined to explain 55% of the variance.
As described in Table 2, Factor 1, which was dominant, loaded to .30 or higher on six of the 12 items, with Item 16 (“I never worry about feeling judged because of my learning disability”) and Item 6 (“I worry about people judging me because I have a learning disability”) contributing the highest loadings. We consider this factor the expected measure of stigma consciousness. Factor 2 loaded to .30 or higher on only three items (Item 7: “Most people have negative views about kids with learning disabilities even though they don’t say them out loud”; Item 4: “Most people don’t judge someone else just because that person has a learning disability” [reverse coded]; Item 10: “In my experience, many people think that there is something wrong with kids with learning disabilities.”). All relate not to one’s personal experiences or concerns about stigmatization, but to society’s views of learning disability, leading us to name this factor “societal perceptions.” As confirmation, a parallel factor analysis was conducted with the same 12 items from the second administration. These again loaded on two factors. 2
Subsequent analysis focused on the first factor, which is most central to the focus of this validation work. Rather than limiting the stigma consciousness score to the items with high factor loadings, we calculated stigma consciousness scores for each student by averaging across the 12-item scale. Higher scores indicate greater stigma consciousness. Scores ranged from 1.33 to 3.33 (M = 2.32, SD = 0.51) on a 4-point scale. We chose to maintain all items because we recognize the relatively small sample size and exploratory nature of this work; we expect future studies to confirm whether deletion of items is warranted. Sensitivity analyses with only the high-loading items suggest results below were unaffected by retaining all items.
To assess the test–retest reliability of the SCQ-LD, we calculated a correlation between stigma consciousness on our first and second assessments, 4 to 6 weeks apart. The coefficient was r(30) = .80, p < .01, indicating good stability over time.
Research Question 3: Does the SCQ-LD Correlate in Expected Ways to Previously Validated Measures of Self-Perception and Self-Consciousness?
We next examined the relationships between stigma consciousness and other measures to determine construct validity. We found significant correlations consistent with hypothesized directions, indicating validity of the stigma consciousness construct. Specifically, stigma consciousness was positively correlated with students’ overall self-consciousness, r(42) = .33, p < .05, and negatively correlated with each of the three subscales of the Self-Perception Profile for Learning Disabled Students: intellectual ability, r(42) = –.37, p < .05; social competence, r(42) = –.33, p < .05; global self-worth, r(42) = –.35, p < .05. All are moderately correlated, as would be expected for related but not identical constructs. Descriptive statistics for these measures are provided in Table 3.
Summary of Measures.
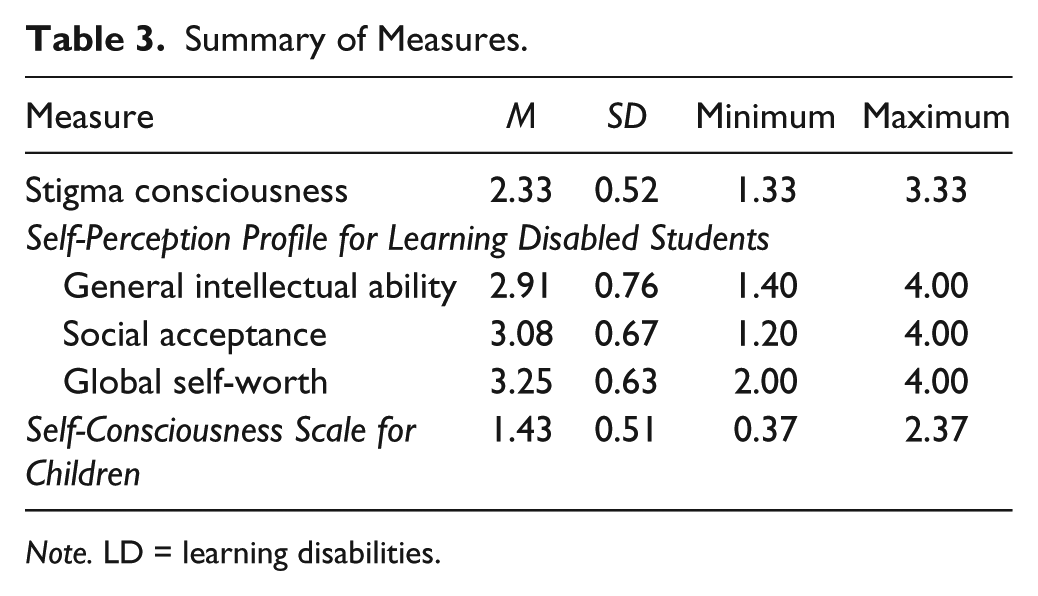
Note. LD = learning disabilities.
Research Question 4: Do Students With LD Report Stigma Consciousness Related to the LD Label, and to What Degree?
Thirty-eight percent of participants’ average stigma consciousness scores fell in the “agree” to “strongly agree,” range indicating they were conscious of stigma related to their LD. In addition, 67% of respondents either agreed or strongly agreed with at least four items on the scale, indicating that a significant majority had some consciousness of stigma related to their LD. Stigma consciousness did not differ by gender, grade, or school.
In addition to the quantitative findings, we were able to qualitatively explore student responses to the two open-response questions about definition of “learning disability” and perceptions of others’ views of LD. As with the earlier qualitative analysis during measure development, we systematically reviewed student statements using constant comparison and typological analysis (LeCompte, Preissle, & Tesch, 1993). Our analysis revealed great variability in both how students view and understand their LD, and how they perceive others’ views and understanding of LD. When asked what having a LD means to them personally, many students responded that it means learning differently than other people and that certain tasks may be difficult or require extra time or help: “It means I need to learn differently than my peers and struggle a bit more to get the same amount of progress.” Many students expressed that although they learn differently, they are just as capable of achieving what others can: “It means that it will be harder to learn but not impossible and if you persevere you can do anything.” However, one student responded that having a LD means “that you are going to have a hard time in school and in real life.” Several students described a LD as a gift or advantage: “I see a learning disability more as an advantage, I think we think differently than everyone else, but it’s a gift. I think it can be very difficult to handle it sometimes, because it makes certain things more difficult.” When asked what other people think about kids with LD, most students responded that other people think kids with LD are less smart, stupid, or dumb: “Most people think that they are just plain out dumb and will never be as smart as people without them.” In contrast, some students said that other people do not see or treat them any differently: “I don’t think that they think anything different of them.”
Discussion
The purpose of this study was to develop and validate a measure of stigma consciousness for adolescents with LD that enables consideration of individual differences in the experience of stigmatization in this population. The newly developed SCQ-LD shows variability in a construct not previously examined among adolescents with LD and it demonstrates expected qualities of an effective measure. That a roughly normal distribution in stigma consciousness existed even among the small, demographically homogeneous group of participants confirms the potential of this construct to move beyond the view of students with LD as, by default, a stigmatized population. As Link and Phelan (2001) suggested in their landmark work on stigma, there will be individual differences in experiences and outcomes within any stigmatized group, just as in any other segment of the population: “no one is fully trapped in a uniform disadvantaged position” (p. 380).
Results indicate that stigma consciousness is a stable construct in this population and that it relates as would be expected to other constructs like self-perception and self-consciousness. Because it is related to and yet distinct from other constructs, stigma consciousness may contribute understanding beyond what has previously been studied. Furthermore, the finding that two factors best represent the data leads to consideration of the potential distinction between personal experiences of stigma and perceptions of society’s views of LD. Qualitative responses are consistent with this potential distinction, as students’ explanations of LD and others’ perceptions suggest that some students distinguish between a personal view of the LD as not substantially negative and yet still perceive prejudice from others; they are conscious of stigma yet resilient in self-concept.
Although the finding that many participants do not report substantial stigmatization provides promise for the potential of identifying contextual and individual factors that may be protective, it is also clear that many adolescents with LD do perceive themselves to be stereotyped due to membership in this group. Just more than one-third of participants indicated across items a consistent perception that they are likely to be stereotyped because of their LD, and two thirds indicate such a perception on four or more items. Such perceptions can have critical impact on academic skills and emotional health. One effect of stigma consciousness is particularly relevant for students with LD. Inzlicht, McKay, and Aronson (2006) demonstrated that wrestling with and being conscious of stigma can result in lower levels of self-control and self-regulation. Given the likelihood that students with LD already face challenges in executive function and self-regulation (e.g., Cutting, Materek, Cole, Levine, & Mahone, 2009), assessing and attending to stigma consciousness may be particularly salient for this population. Furthermore, chronic experiences of stigmatization have long-term effects on disengagement as a student (Woodcock, Hernandez, Estrada, & Schultz, 2012) and concealable stigmas come with particular risk for depression and anxiety (Quinn & Chaudoir, 2009).
In addition to the learning to be gained from use of the measure, the iterative process of its development also highlights important findings. This process demonstrated both the complexity of the LD identity and the need for substantial input from students with LD themselves. Measuring stigma consciousness when focusing on a concealable stigma with varying labels and self-perceptions presented a unique challenge. This work provides an example of how to adapt an existing measure such that it maintains the structure and goals of a previously used instrument, but reflects the particular needs of this unique population. Purposefully working with both experts and students for understanding and usability resulted in a substantially different measure from where we started, with a unique approach to administration.
Limitations
This study provides an initial step and useful tool for the field to pursue stigma consciousness as a new direction for understanding students’ experiences, but we recognize the limitations of this work and the need for continued research. A primary limitation is clearly the nature of the sample, which was small, demographically homogeneous, and primarily from private school settings. This presents a serious challenge, particularly in determining the prevalence of stigma consciousness, but we suggest that it does not invalidate the development and validation work; the SCQ-LD is reliable, valid, and usable. We hope that it will be used for research in other contexts with many more students so that the field can continue to understand both the most effective measure design and the nature of stigma consciousness in the population of adolescents with LD as a whole. The factor analysis was exploratory and on a small sample; as such, the solution is our current understanding about how the scale organizes, but it could be that with a larger, more diverse sample, a more complex factor structure will emerge. This initial work follows in the same vein as the Frostig Center study (Goldberg, Higgins, Raskind, & Herman, 2003; Higgins et al., 2002) in which all participants had attended the private school for students with LD; the field benefited from understanding their experiences and outcomes to then investigate similar trends with a broader population.
In addition, we did not investigate what contributed to students’ reported experiences of stigmatization. Future work needs to consider the role of, for example, societal-level influences like those presented in the media, relationships with key individuals such as parents, teachers, and peers, and instructional or school-related contextual factors. A developmental perspective would additionally contribute to understanding the dynamics of stigma experiences, perhaps particularly in relation to time of diagnosis and types of academic experiences at different grade levels. When focusing on students in high school, investigation of the relative contribution to perceptions of stigma from childhood experiences compared with those during adolescence would contribute to the body of life-course perspectives (McNulty, 2003). This would more effectively inform the identification of high-leverage opportunities for intervention.
Implications for Practice
This work has potential implications for practice, as future work could investigate the potential to use the SCQ-LD as a component of assessing school climate. Although the measure has not yet been used in partnership with educators, administrators with whom we partnered expressed concern about the stigma experiences of their students with LD and a desire for support in this regard. Overall, the prevalence of high levels of stigma consciousness supports previous calls for a focus on supporting the social and emotional health of students with LD, including for adolescents (Al-Yagon, 2016).
Addressing stigma consciousness is complex. Interventions with other populations have taken different perspectives. One approach would be to encourage a group identity. Stronger identification with a group may be associated with high levels of stigma consciousness, and also provide benefits through increased likelihood of fighting against stereotyping and discrimination (Pinel, 1999). Recent campaigns like “say dyslexia” (http://www.saydyslexia.org/) and Project Eye-to-Eye’s work on “owning the label” (http://eyetoeyenational.org) suggest that some in the LD field have embraced this identity salience strategy. Students with LD are encouraged to recognize, embrace, and appreciate their LD as a core part of themselves and a reason for pride rather than concern. Recent intervention work to address the negative effects of stigma consciousness and stereotype threat with other vulnerable populations take a different perspective, suggesting that harm from awareness and experience of stigma manifest primarily when stigmatization becomes a critical aspect of one’s identity (Cohen, Garcia, Purdie-Vaughns, Apfel, & Brzustoski, 2009; Pinel & Bosson, 2013). These instead focus on strengthening self-perception regarding other aspects of identity. For example, interventions emphasize strengths and values without attention to group membership. Understanding more richly the experiences of individual students may be able to inform the design of interventions that effectively leverage a group identity and avoid some of the psychological risks associated with it.
Conclusion
Experiences of stigmatization play a critical role in the developmental and academic experiences of individuals who perceive their group memberships to be reason for stereotyping and prejudice. As many educators, parents, and individuals are aware, adolescents with LD may be vulnerable to such perceptions. But, the lack of uniformity in experiences presents great opportunity to understand the dynamics at play. Continuing the tradition in the field of avoiding consideration of the population as a whole but instead looking at variability within can move beyond assumptions of stigmatization to understand and intervene in a more responsive way.
Footnotes
Acknowledgements
The authors wish to acknowledge the research assistance of Miriam Evans, Graham Gardner, Elysa Greenberger, and Kristin Robinson.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This material is based upon work supported by the National Science Foundation under Grant No. HRD #1251819.