
Abstract
The objective of this study was to identify contextual factors influencing the degree of integration of the ecological approach in disease prevention and health promotion (DPHP) programming initiatives for older adults in two public health organizations in Québec, Canada. A case study design was used and two organizations presenting contrasting profiles in the degree of integration of the approach in their DPHP programming for older adults were selected. Face-to-face interviews with professionals and managers and archival analysis were conducted. Several factors emerged as constraining the integration of the approach in both organizations, including the lack of data showing the effectiveness of DPHP interventions for older adults and the presence of macro-contextual political factors at odds with the ideology of DPHP. Resources and partnerships with academic milieus emerged as key factors distinguishing the two organizations. These results provide increased understanding of conditions required for planning DPHP programs for older adults.
Introduction
Over the past 20 years, a great deal of enthusiasm has been directed toward the ecological approach, which is now regarded as a key component of the new public health and of the health promotion movement (Green, Poland, & Rootman, 2000; Schwab & Syme, 1997). The ecological approach offers a framework for research and intervention centered on a broadened perspective of the determinants of health and emphasizing the complex transactions among individuals, groups, and their environment (Green, Richard, & Potvin, 1996; McLaren & Hawe, 2005; Sallis, Owen, & Fisher, 2008). In line with such a perspective, there is growing recognition that the most effective programs are those based on a comprehensive approach that includes multiple intervention strategies aimed not only at the individual-level determinants of health (e.g., behavior, knowledge, skills) but also, and more importantly, at the various environmental-level determinants (i.e., social networks and organizational, community, and political environments) across a variety of settings (Green et al., 1996; Jackson et al., 2007; Sallis et al., 2006; Whitehead, 2007). In light of this potential, it is not surprising that bodies such as the WHO, the Institute of Medicine, and Ministries of Health have made the ecological approach the framework underpinning their thinking and initiatives in the field of the health of populations (Smedley & Syme, 2000; U.S. Department of Health and Human Services, 2000; World Health Organization & Health and Welfare Canada and the Canadian Public Health Association, 1986). Despite this emerging consensus, it is surprising to note that the ecological approach is still poorly integrated into professional practice (Beaglehole & Bonita, 2004; Trickett, 2009). The resolution of this paradox demands more extensive research. Aside from knowledge transfer and methodological developments (Kok, Gottlieb, Commers, & Smerecnik, 2008; Richard, Potvin, Kishchuk, Prlic, & Green, 1996; Stokols, 1996), one avenue has been to investigate factors associated with the integration of the ecological approach in public health organizations to identify potential levers to stimulate implementation.
Initial studies revealed the pivotal role played by the cognitive attributes and personal traits linked to the training and experience of the professionals involved in programs. Programming practices are more likely to be ecological when practitioners have more extensive academic training, are familiar with health promotion interventions, and harbor beliefs that are consistent with the ecological approach (e.g., recognize the importance of macro-social determinants of health; Holden, Strazza Moore, & Holliday, 1998; Lévesque, Richard, & Potvin, 2000; Richard, Gauvin, Potvin, Denis, & Kishchuk, 2002; Richard et al., 2004). Moreover, results show that ecological programs are more likely to be adopted by multidisciplinary teams who have access to more substantial resources and among professionals who have frequent contacts and collaborations with external partners (Richard et al., 2002, 2004; Riley, Taylor, & Elliott, 2001; Robinson, Driedger, Elliott, & Eyles, 2006). Finally, Richard et al. (2004) underscore the marked influence of ministerial orientations and policies.
With regard to health policies, recent studies have shed light on macro-level factors likely to heighten support of an approach centered on the determinants of health. For example, Raphael and Bryant (2006) conducted a case study of public health policies in Sweden, Canada, USA, and UK. Their results showed that political ideology and public health traditions lead to unique configurations of public policies. For example, Sweden, with its tradition of maintaining a welfare state, has been a very fertile ground for the implementation of the determinants of health discourse and associated policies (Petersson, 2007). Similarly, reflecting over the experience of large-scale innovative public health initiatives including a broad vision of determinants of health in the United Kingdom (e.g., Health Actions Zones, Healthy Cities), Berkeley and Springett (2006b) identified cultural constraints and political barriers impeding the transition from public health policy “rhetoric to [public policy] reality” including the dominance of the biomedical paradigm with its emphasis on quantification and short-term targets of performance, differing organizational cultures and practices of partners, differing professional/experiential culture among professionals, and political imperatives at odds with a health promotion perspective.
It is noteworthy, although not surprising, to note that none of the existing studies have been conducted within the context of policies and programs devoted to aging and older adults. Even though disease prevention and health promotion (DPHP) offer excellent potential in terms of preventing disabilities and improving quality of life during the later years of life (Goetzel et al., 2007), in comparison to other age groups, older adults are least often targeted by DPHP efforts (Bennett & Flaherty-Robb, 2003). Even when such programs are developed, they more often than not adopt a traditional approach aimed at modifying individual characteristics to the detriment of innovative approaches involving action on environmental conditions (Richard et al., 2008; Runciman, Watson, McIntosh, & Tolson, 2006; Satariano & McAuley, 2003). Issues of ageism in public health may explain the lack of attention devoted to this clientele (Ory, Hoffman, Hawkins, Sanner, & Mockenhaupt, 2003). Bennett and Flaherty-Robb (2003) also suggest that beliefs grounded in the notion that physical health is the main determinant of quality of life among older adults could limit the potential for adopting a more inclusive, ecological approach with this population.
In light of these considerations, the purpose of this study was to identify the contextual factors associated with greater integration of the ecological approach in DPHP programming offered to older adults in organizations entrusted with the mandate of delivering public health programs and services at the regional level. Toward this end, a case study approach was adopted and the organizations examined were regional public health departments in the province of Québec, Canada. Conceptually, the study was couched in Scheirer’s model of program implementation (Roberts-Gray & Scheirer, 1988; Scheirer, 1981, 1994). In keeping with Scheirer’s model and recent theoretical developments on program implementation (Durlak & DuPre, 2008), three categories of contextual factors were examined: environmental, organizational, and professional (see Table 1).
Contextual Factors Hypothesized to Influence the Degree of Integration of the Ecological Approach According to Scheirer

Note: DPHP = disease prevention and health promotion.
Method
Context
In Canada, health care services come under provincial jurisdiction. Most provincial governments, including Québec, have assigned the decision making process (planning, resource management, and budget allocation) to authorities working in regional establishments. Although the regionalization process had been underway for some time in Québec, an additional reform occurred in 2004 wherein service delivery was restructured around local service networks. In each region, agencies are responsible for coordinating and setting up local services/programs on their territory. At the local level, the Centres de santé et des services sociaux (CSSS; Local Health and Social Services Centers) now act as the headquarters for this new mode of service/program delivery and have the mandate of organizing, in collaboration with partners, the delivery of health and social services on their territory to meet population needs (Ministère de la santé et des services sociaux, 2004). In public health, this method implies that regional agencies, through their Directions de santé publique (DSP; Public Health Departments), organize and carry out public health functions (e.g., disease prevention, health promotion, protection) and implement the regional public health action plan, in compliance with the Public Health Act and the Quebec National Health Program (Ministère de la santé et des services sociaux, 2003) taking into account the unique characteristics of the population in their territory. The CSSSs are now being given the responsibility of delivering “frontline” public health services to local populations: Actions that are aimed at health promotion, disease prevention, and health protection in accordance with the regional and local public health action plans (Ministère de la santé et des services sociaux, 2004). It should be recognized that as a result of this hierarchical organization of service delivery, the DSP does not directly deliver services to the population. Rather, services to the population are offered by the CSSSs.
Design and Case Selection
We adopted a case study design using the DSP and its DPHP programming for older adults as the unit of analysis. Programming was conceived as the DSP’s entire ensemble of DPHP initiatives (programs, interventions, etc.), offered to achieve objectives related to the health of older adults. Two cases (referred to as DSP A & B) representing contrasting profiles in regard to the degree of integration of the ecological approach in DPHP programming for older adults (i.e., extensive vs. limited integration as shown by number and types of strategies deployed and of intervention settings as well as the number of initiatives) were identified. Data collected during a previous study examining DPHP programming in DSPs (Richard et al., 2008) were used to identify an initial set of contrasting DSPs. Other criteria were also taken into account. That is, to limit sources of variability, only DSPs whose headquarters were located in urban or peri-urban environments and that were servicing populations similar in size and proportion of older adults were included. Finally, for practical purposes, organizations located more than 200 km from Montreal were excluded as were two organizations that had recently participated in another study by our team.
DSP A (extensive integration of the ecological approach) serviced a population of 302,161 residents which included 15% older adults (age ≥ 65years). Its territorial catchment area was about 10,000 km2 and included urban, peri-urban, and rural subareas. DSP B (limited integration of the ecological approach) serviced a population of 376,845 residents which included 14% older adults. The catchment area was somewhat smaller at 246 km2 and characterized by urban subareas with predominantly suburban-type housing.
Procedure and Measures
Once agreement to participate had been received from the directors of DSPs, the profile of each organization in regard to integration of the ecological dimension into DPHP programming for older adults was updated. That is, the list of programming initiatives identified in the previous study (Richard et al., 2008) was reviewed and a detailed description of new and modified initiatives was drawn up to enumerate intervention strategies and settings. In line with Richard et al. (2008), an intervention strategy refers to the intervention pathway from where the intervention initiative is instigated to where it reaches individuals whose health we wish to promote. The analysis chart includes five targets: the individual client and their interpersonal, organizational, community, and political environments. For example, a healthy nutrition initiative may include two strategies, one involving action on diabetic seniors (individual target) and another involving action on their spouses (interpersonal target). The intervention setting is defined as the context or social system in which individuals ultimately targeted by the DPHP strategy are reached. Four categories of settings are used: organizations, community, society (e.g., province), and supranational systems (e.g., European Economic Community). To continue with our example, the healthy nutrition initiative may reach individuals when they visit their physician (health organization setting); alternatively, individuals might be reached through a community media campaign (community setting).
Data related to environmental, organizational, and professional factors hypothesized to be associated with the degree of integration of the ecological approach (see Table 1) were collected by means of semidirected interviews with professionals identified as resource persons (n = 9) for specific initiatives in each DSP. Interviews lasting about 90 min were also conducted with members of middle and upper management (n = 5) in both DSPs. Archival data were examined and included action plans and portraits of the health of local populations. Data were collected in 2006; shorter follow-up interviews were carried out in 2007. The Health Sciences Human Research Ethics Committee of the Université de Montréal approved the project.
Analysis
Information pertaining to the updated list of programming initiatives was reviewed by two analysts (MT, LR) to identify intervention settings and strategies. All differences in coding were resolved by consensus.
Data from interviews and archival documents were content analyzed. The first step involved coding of interview materials in terms of themes falling into each category of contextual factors derived from the Scheirer model (see Table 1) by one of the team members (MT). Coding was then thoroughly reviewed by a second team member (LR) and differences were resolved by consensus. Next, summary statements were produced for all themes identified and used to establish a portrait of each DSP. The final step involved examining the two portraits and writing a comparative analysis. Toward this end, the analyst responsible for these last two steps (LR) built a chain of evidence which involved careful specification of each step in the reasoning process and inclusion of detailed references to the data set at each step. A third member (MEL) validated the analysis. For penultimate validation purposes, results and interpretation were presented to and discussed with interview respondents at each DSP during two separate, 75-min consensus meetings.
Results
Degree of Integration of the Ecological Approach in Contrasting DSPs
In line with the profile established a few years prior (Richard et al., 2008), the analysis carried out on the updated initiatives allowed for corroboration of contrasting profiles and recognition of some commonalities. In both sites, the programming initiatives addressed a variety of health issues with physical health issues being the focus most often (see Table 2). As shown in Table 3 though, a greater number of programming initiatives was implemented in DSP A (12 vs. 9) and overall initiatives encompassing a much greater number of intervention strategies (23 vs. 11). Furthermore, a detailed analysis revealed a marked difference in terms of the diversity of these strategies. Only two types of strategies were observed in DSP B, namely actions on individual and organizational targets. By contrast, a more diversified profile emerged in DSP A where six different types of strategies were identified, including various networking strategies. Such networking strategies, which were conspicuously absent from DSP B’s programming and which consist of getting actors to work collaboratively on a health issue of common concern, is very much in line with the tenets of the health promotion movement and the implementation of innovative and more ecological community-based approaches (Stith et al., 2006; Zakocs & Edwards, 2006). With regard to intervention settings, the analysis showed seven different types of settings in both DSPs (data not presented). Health organizations of various types (hospitals, clinics and physicians’ offices, long-term care facilities, and local public health organizations) were frequently found in DSPs A and B, but DSP A clearly showed a very distinct profile with higher frequencies of other types of settings, including the community setting. Community settings are, of course, of critical relevance for the implementation of large-scale ecological programs. Overall, these analyses support the notion that the two DSPs were indeed contrasting organizations with DSP A showing extensive integration of the ecological approach whereas DSP B showed very limited integration.
Health Issues Targeted Through Programming Initiatives
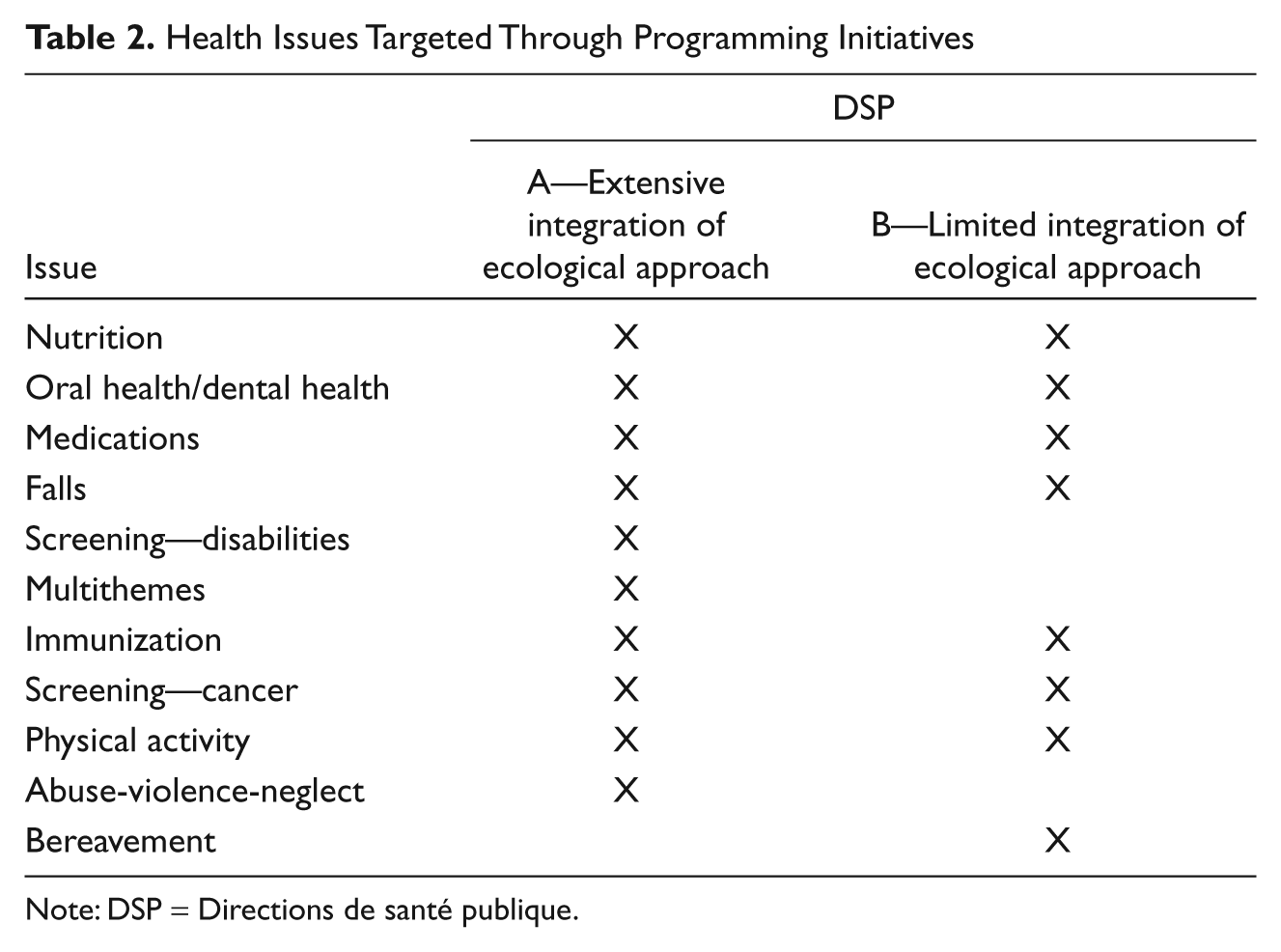
Note: DSP = Directions de santé publique.
Ecological Analysis of Programming Across Contrasting Organizations
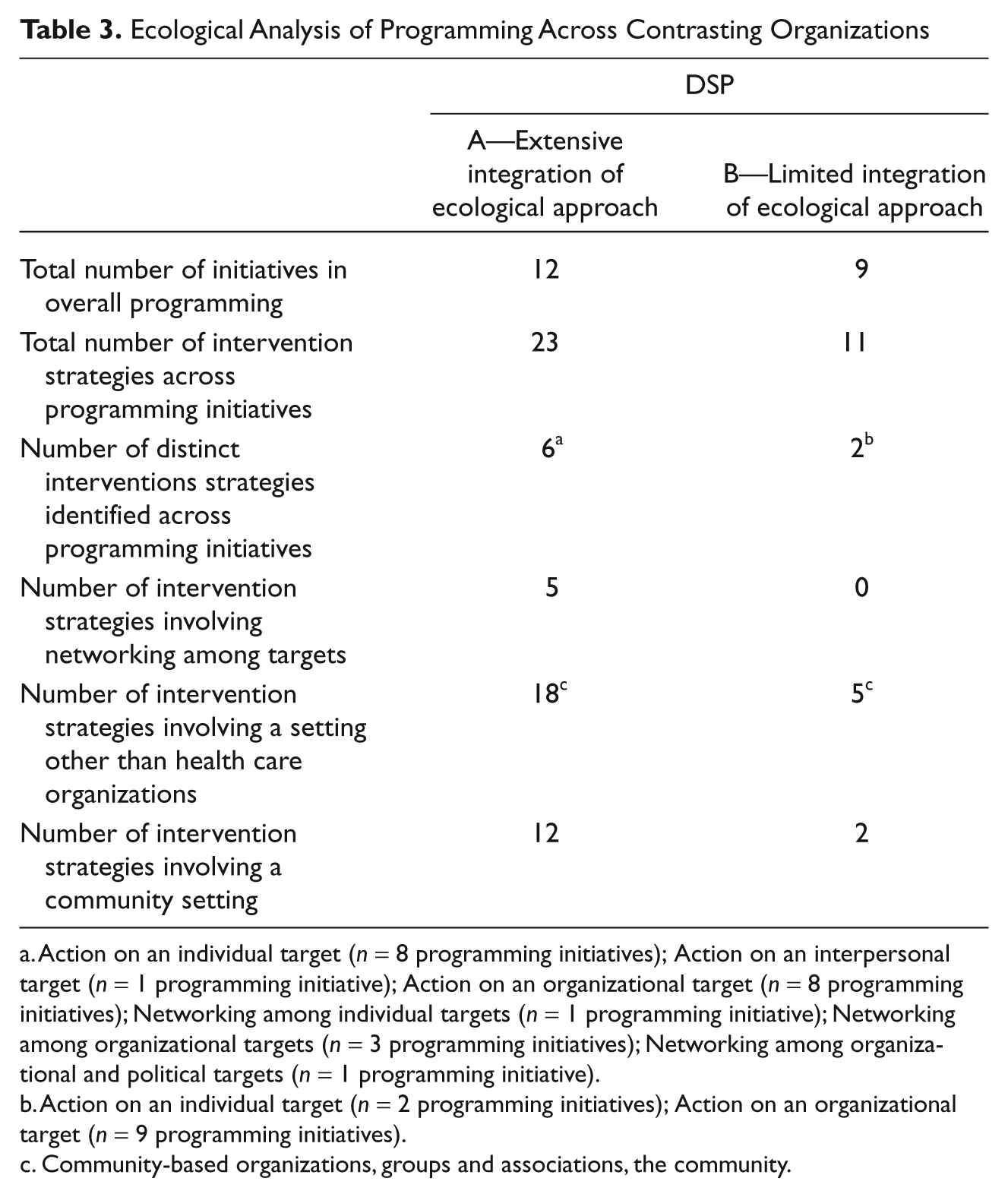
Action on an individual target (n = 8 programming initiatives); Action on an interpersonal target (n = 1 programming initiative); Action on an organizational target (n = 8 programming initiatives); Networking among individual targets (n = 1 programming initiative); Networking among organizational targets (n = 3 programming initiatives); Networking among organizational and political targets (n = 1 programming initiative).
Action on an individual target (n = 2 programming initiatives); Action on an organizational target (n = 9 programming initiatives).
Community-based organizations, groups and associations, the community.
Contextual Factors Associated With Implementation of DPHP Programming Initiatives
Environmental Factors
Although the inclusion criteria allowed for the selection of DSPs that were similar on various predefined characteristics, selected DSPs differed in terms of population densities. DSP A serviced a population living over a large territory and which was more scattered than at DSP B. Even though this situation presented challenges to practitioners because of the distances, it also appeared to engender advantages including a more “human dimension” and the capacity of having informal interactions with intervention partners: “Around here, we can speak directly with the Mayor” (DSP A-03). The region was described by DSP respondents as dynamic with, among other establishments, a university campus that included a research centre on aging. DSP B was located on a more compact territory and close to a major urban area. Respondents in this DSP viewed this situation as both advantageous (e.g., higher access to resources) and disadvantageous (e.g., difficulty in eliciting interest from the media for local issues). Administratively, the territory was also unique having only one administrative office, one CSSS, one school board, and so forth.
Respondents from the two DSPs reported the presence of numerous organizations that they qualified as partners in regard to developing and contributing to DPHP programming initiatives. The data collected at DSP A showed a favorable history of collaboration, with several statements pertaining, among others, to the presence of boards and working groups, to a “culture of dialogue,” to the presence of partners valuing the DPHP function of public health: “Our bosses have established good relationships with the network of establishments . . . this is a strength compared to other regions” (DSP A-03). Moreover, one respondent mentioned and commented favorably on the collaborative links created by university researchers and his or her public health department. At DSP B, given the administrative profile described earlier, the number of organizations and personnel addressing public health issues was more limited. Dialogue was viewed as effortless: “It’s easy to seat everyone around the table” (DSP B-01); “You keep meeting the same people, you meet them on different boards, thus they have a connection” (DSP B-04). Partnerships, particularly boards and working groups, have been in place for a long time.
Despite this positive portrait of the community context across the two DSPs, respondents mentioned certain constraints. Lack of resources among community partners and within the public health and social services network as well as the context created by the current health care system reform were identified in both DSPs : “The changeover is very draining on our network” (DSP B-06) so that “The time is not really right for DPHP” (DSP A-06). Finally, one informant identified the fact that “There is no pressure from the population to do these activities (DPHP)” (DSP A-08) as a constraint.
Organizational Factors
Team Structure
The two DSPs showed substantial similarity in terms of organizational structure. Professionals dedicated to the older adult clientele were located within a DPHP team within a structure that included other teams devoted to other public health domains (e.g., surveillance, occupational health). At both DSPs, the DPHP team had 12 to 15 professionals. These professionals worked on several projects at the same time and certain groupings may have been created around themed priorities, for example, “Healthy Schools”. However, there wasn’t any grouping around the older adult clientele at either DSP.
Planning of Programming Initiatives
Ministerial orientations
Informants placed the implementation of the Québec National Health Program at the centre of the DSP’s mission, thereby providing substantial orientation for their DPHP work. This program is the principal instrument in the Public Health Act for orientating programming initiatives at the provincial, regional, and local levels. As such, it outlines priorities and activities for maintaining and improving the health of the population. Based on a broad vision of the determinants of health, the program enumerates social and health objectives and outlines sets of activities to be implemented. Older adults are targeted implicitly in all activities addressing the general population and are also identified as a specific clientele for selected activities related to a small number of health issues including medications, abuse-violence-neglect, screening for and coping with chronic illnesses, and falls prevention. Several respondents observed that the older adult clientele was not given priority in the Québec National Health Program. One informant referred to much tension, within the health care system, between curative and preventive services, particularly in regard to services for older adults: “The huge amount of curative needs among older adults, takes up a lot, a lot of room” (DSP B-06).
Criteria for identifying priorities
The criteria governing the identification of priorities in planning DPHP programming initiatives at the regional level emerged as a major influence. A first criterion pertains to ministerial announcements and attached budgets. Programming initiatives directly in line with the expectations of the ministry, and for which funding is available, had greater likelihood of occurrence. A second important criterion pertains to the existence of data supporting the effectiveness of a given programming initiative. Several respondents underscored that this criterion was detrimental to the cause of DPHP interventions overall and more specifically to DPHP for older adults: “. . . there is not a lot of literature that demonstrates by a + b the effectiveness of health promotion programs in general, and even less for those for older adults” (DSP B-01). Respondents indicated that, as a consequence, programming initiatives were set almost in advance:
it is very, very clear that when we adopt such a stance then programming initiatives are necessarily orientated towards approaches that are slightly more clinical, for example, an individual approach rather than a population-based approach, because the outcomes of approaches that are more clinical and individually focused can be measured better.” (DSP A-03)
Similarly, “. . . interventions based on risk factors appear to me to be easier than working on the fundamental determinants of health” (DSP A-01).
Work procedures
At both sites, the “unfolding of the Québec National Health Program at the regional level” included several iterative steps involving management, public health professionals, and community organizations. It also left a lot of room for consultation with partners. Collaboration with researchers from outside the organization in the form of knowledge transfer and consultation was mentioned in Site A. Once adopted, the regional action plan provided direction for the planning of programming initiatives. The next step involved implementation, which was done by community organizations (e.g., CSSS, community organizations) but supported by DSP professionals.
Partners outside the DSP
At both DSPs, the CSSS emerged as major partners in the DPHP planning process. The DSP, now “once-removed” from action, acts as a support for these local organizations which are responsible for deployment of programming initiatives locally, directly to the population.
We at the regional level set the fundamental objectives, the main parameters, but afterwards, how is the program implemented at the local level? This is actually done with the CSSSs . . . Our intervention is a lot of planning, training, tools, support, evaluation, etc.” (DSP A-01)
Community associations and organizations also appeared to be partners, while selected ones were supported, particularly in terms of budgets, by the DSP to implement specific projects. Finally, the partnerships with university milieus was quite markedly apparent at DSP A, and three informants referred very favorably to collaborations with researchers and students: “We had the best experts very close by, within a couple of blocks, so we went to the research centre and we worked with them” (DSP A-08).
Resources Devoted to DPHP
Respondents at both DSPs stressed the lack of resources devoted to DPHP for older adults: “Public health has never had money for older adults” (DSP A-08). This context of scarcity seems to have contributed to generating a strategy for maximizing resources. This involves the initiation of close ties between professionals dedicated to the older adult clientele in the DSPs and colleagues from the services organization department. Such partnerships create opportunities for developing DPHP programming initiatives as part of the services developed by this parallel department which addresses the needs of older adults who are losing their independence. One comment from DSP B illustrates this point: “Some of our DPHP activities are very closely related to the organization of services, among others, those targeted towards older adults losing their independence, so that we can look for funding within these budgets” (DSP B-06). This partnership was also mentioned at DSP A, in a more significant way, for a long time, where staff exchanges between the two departments involved, and formalized agreements in regard to budget transfers, have maximized the size of the budgetary allowances actually available for developing DPHP activities for older adults. “They [Service Organization Department] previously gave money, an amount indexed each year and which went towards our services. But we did DPHP with that” (DSP A-02).
Normative Environment and Support From Management
With regard to the ecological approach, respondents harbored favorable standards and perceptions: “Everyone involved in public health services knows that if we don’t have a multi-factorial approach and what’s more, multi-sectorial, we don’t see how we can go anywhere with DPHP” (DSP A-08). However, according to respondents, complete implementation seemed to present a challenge, particularly because of the difficulties posed by action on the political front: “When it’s political, once you touch on politics or on citizen groups, it’s very, very touchy” (DSP A-08).
Certain aspects specific to the clientele were also noteworthy. First, respondents indicated that older adults are not perceived as a priority clientele in the Québec National Health Program. Next, several informants at both DSPs perceived unfavorable prejudice regarding DPHP programming initiatives for older adults, compared with younger clienteles:
I think there’s a bias towards youth in public health. (DSP A-04)
. . . the premise of DPHP is . . . to attack early, thus before the problem arises. So, already the fact that we’re talking about older adults, perhaps there’s a small intellectual bug in certain people . . . (DSP B-03)
One informant clearly referred to the ageism present in public health, a feature of the results that inspired lively debate when the preliminary results were presented at each DSP. The word was deemed to be “too strong.”
Respondents at both DSPs reported being supported by their management and their colleagues, particularly in regard to DPHP for older adults. This support seems crucial given the long-term horizon for this type of intervention: “. . . this takes policy-makers who know they’re going to have to wait 20 years for results, and politics really doesn’t like that very much and it takes someone who has a lot of faith in these things” (DSP A-04).
Other Features
One final question led respondents to identify other factors that could help or limit integration of the ecological approach. Two main issues arose. First, training for the approach should be more user-friendly: “. . . those of us in public health, we have a lot of work to do to make things simple, concrete” (DSP B-01). At DSP A, one informant clearly made a connection between the richness of the programming in his or her DSP and “important links that we have with the academic and university milieu”; “[with] this closeness, we don’t have any choice but going in the direction that seems to be pertinent for the future” (DSP A-08). Close ties among DSP A staff members and the service organization department were again identified as having facilitated the provision of resources for DPHP for older adults.
Professional Factors
At DSP A, the public health professionals directly involved in DPHP for older adults had vast experience within the DSP (all more than 10 years), sometimes coupled with other experiences within the public health system. The fields in which they were originally trained were diverse (e.g., gerontology, kinesiology) and two people had postgraduate degrees. At DSP B, a few people also had had involvement in older adult dossiers. In total, however, the number of years of experience was lower than at DSP A. The background disciplines were varied at the postgraduate level.
Informants were questioned as to their personal definition of the ecological approach (a definition was classified as “correct” when the response included references to varied intervention settings, targets, and/or intervention strategies). In DSP A, three respondents provided a correct definition, whereas only one person at DSP B responded correctly (at DSP A, a fourth informant was not asked about his or her definition; however, in the analysis, all of his or her remarks reflected an excellent knowledge of the approach). As for perceptions about the ecological approach, more positive elements (especially in connection with relevance and effectiveness) than negative (especially in relation to the complexity of the approach, its long-term impact, and the costs involved) were observed at both sites.
Comparative Analysis
The between-case analysis revealed two groups of factors distinguishing the two DSPs. Human and financial resources constituted the first group. The professionals at DSP A had been working on older adult issues for much longer than those at DSP B; they also seemed more familiar with the ecological approach. The validation stage provided confirmation of the importance of human resources with the stability of staff in DSP A and, in contrast, the turnover of staff in DSP B. In addition, the budgetary resources appeared significant such as the presence of a strategy for maximizing budgets through collaboration with another department that organizes services which clearly emerged as a key factor in DSP A. Finally, the establishment of close links between the team at DSP A and its partners in the university milieu dedicated to the study of aging appeared to play a crucial role in allowing for the integration of the ecological approach, a finding that was strongly endorsed during the consensus meetings. Aside from these differences, the analysis revealed many commonalities in terms of factors of influences. Table 4 outlines common factors and key differences across the two DSPs.
Commonalities and Key Differences in Factors Influencing the Integration of the Ecological Approach in DSP A (Extensive Integration) and DSP B (Limited Integration)
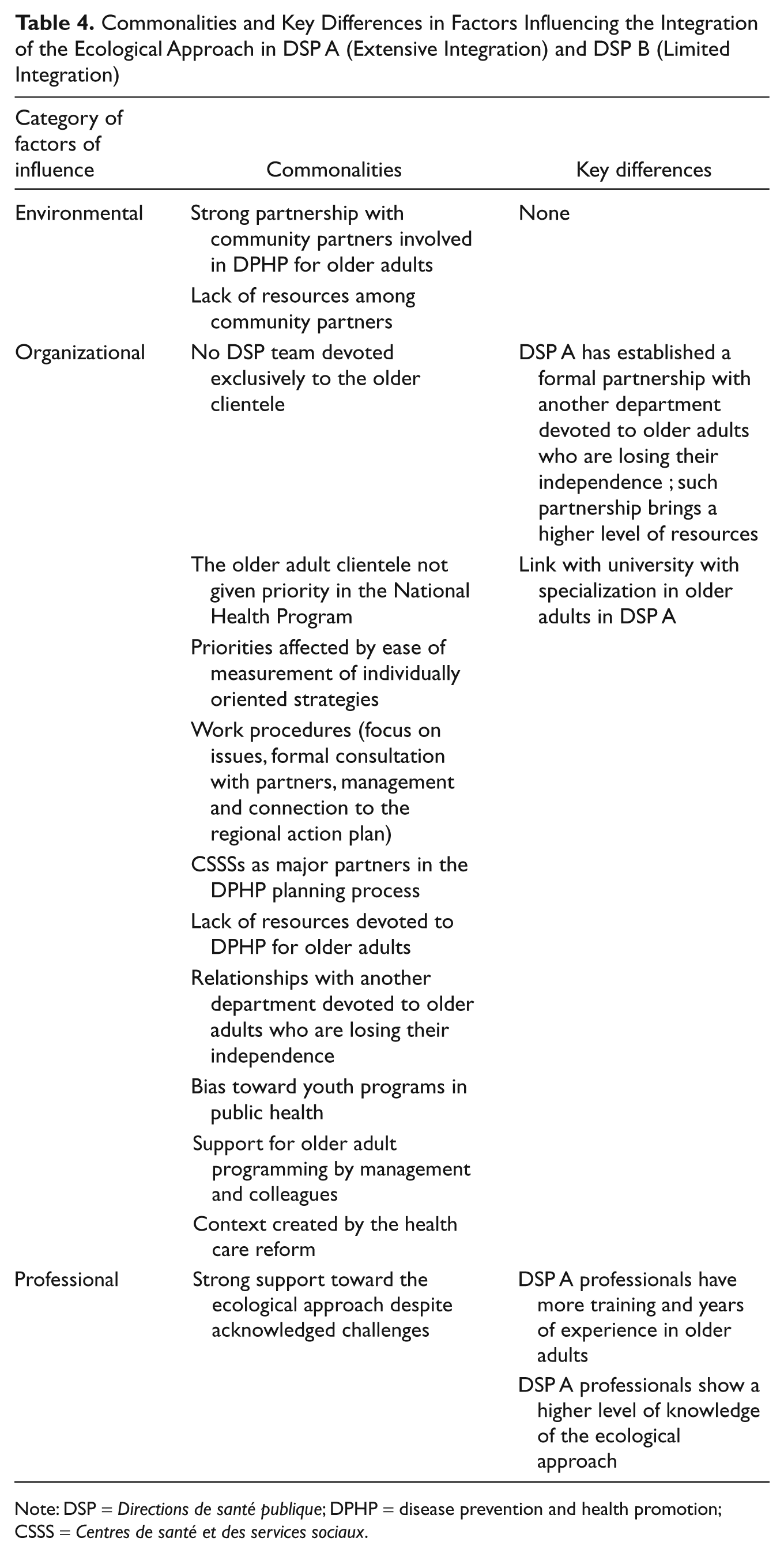
Note: DSP = Directions de santé publique; DPHP = disease prevention and health promotion; CSSS = Centres de santé et des services sociaux.
Discussion
This study allowed for a detailed examination of two DSPs’ DPHP programming for older adults. Although it is clear that one DSP had a better performance than the other in terms of integrating the ecological approach, both sets of programming showed areas for improvement given, for example, the predominance of initiatives aimed at physical health and the relative lack of interventions aimed at community and political targets. This portrait is in line with previous research (Richard et al., 2008; Wallace & Levin, 2000) and is consistent with gaps identified in this area (Satariano & McAuley, 2003). Identifying levers for action to offer DPHP programs more attuned with innovative approaches and thus better able to address population aging are required. Using a case study design, this study identified contextual factors associated with greater integration of the ecological approach in DPHP programming offered to older adults in regional public health organizations.
Shared Factors Impeding Implementation of the Ecological Approach
Respondents at both sites elaborated at length on a series of macro-contextual elements they identified as major influence on their limited capacity to adopt innovative DPHP approaches for their older adult clientele. Of initial interest is the lack of data supporting the effectiveness of specific DPHP interventions for older adults, as a factor likely to delay inclusion of ecological programming initiatives. The heavy reliance on efficacy as a criterion for choosing an intervention resulted in a greater focus on individual initiatives which were often clinical and for which evaluation findings are more readily available. In summarizing data on effectiveness of DPHP interventions, Anderson et al. (2005) wrote that, “Public health is still short of the material base for comprehensive evidence-based decision-making” (p. 228). This would be the case particularly for interventions concerning emerging issues, implemented more widely, involving socioenvironmental determinants and where complex processes of social changes are at work. Elaborating on this, Berkeley and Springett (2006b) stress the absence of consensus on appropriate evaluation frameworks to assess the impact of complex social programs like health promotion programs. These authors suggest that the armamentarium used in public health, which is still based mainly on the biomedical model, is not well suited to the more social approach of health promotion.
Closely associated to the evidence-based rhetoric are a series of political barriers identified by the respondents as constraining the adoption of innovative DPHP approaches. In this respect, consistent with the analyses of the policy directions being taken by liberal political economies such as Canada (Raphael, Curry-Stevens, & Bryant, 2008), lack of support for long-term intervention and resistance to political action, notably on structural determinants, was reported. Respondents indeed stressed the expectations of management in terms of quantifiable and short-term results, these being at the heart of evaluative practices brought by successive health care reforms, largely triggered by a context of public funding crisis. The detrimental effect of such practices on health promotion initiatives in United Kingdom, yet in the context of governmental policy positions supporting action on health determinants, have been exposed by Berkeley and Springett (2006a, 2006b). Originating from a province that has a reputation for being a leader in innovative public health approaches, these results are reminiscent of the British experience and clearly establish a relationship between political macro dimensions and the prioritization of clinical, individual preventive approaches to the detriment of programs targeting the environment.
Finally, another potentially important political barrier emerged in that respondents often referred to the lack of room given to the older adult clientele in ministerial orientations, more specifically in the Québec National Health Program, where this clientele appears to be considered as a lower priority in comparison with other population subgroups. With the exception of abuse-violence-neglect, the objectives devoted to older adults in the program were all related to physical health issues, giving credence to Bennett and Flaherty-Robb’s (2003) impression of a possibly truncated vision of the determinants of quality of life among older adults. The possibility that this situation is a reflection of ageism was not retained during consensus validation. The issue of ageism in public health has already been raised (Ory et al., 2003; Runciman et al., 2006). This study results show that this is a sensitive issue which would need to be investigated from a research perspective.
Factors Associated With Greater Integration of the Ecological Approach
Despite these constraints, one of the organizations studied had begun to implement programming initiatives that included significant diversity in regard to intervention settings and strategies. Resources and partnerships emerged as two factors contributing to success. In regard to resources, the results are certainly consistent with previous studies that show their marked influence both on the development of DPHP programming initiatives (Stith et al., 2006) and on implementation of ecological programming initiatives (Richard et al., 2004). In addition, the favorable impact of establishing partnerships with research and teaching milieus is certainly in line with numerous studies that have demonstrated the key role played by involvement of professionals with organizations and players outside their organization (Richard et al., 2002; Riley et al., 2001). For several decades, organizational research has shown a link between organizational innovation and maintaining contacts and collaboration with the external environment (Aiken & Hage, 1971; Monge, Cozzens, & Contractor, 1992). Two mechanisms could certainly be at play here: the links and exchanges that ensure the influx of innovative programming approaches and practices that provide solutions to issues arising from implementing a demanding and complex programming approach.
Limitations and Future Research
Despite its noteworthy features, this study has some limitations. First, although the use of a conceptual framework orientating the research toward a comprehensive set of factors presents an obvious advantage in terms of interpreting evidence, it also limits the depth of key elements emerging from interviews. A more focused investigation of the question of partnerships with the external environment would, for example, allow for the emergence of information regarding mechanisms favoring the establishment of such partnerships. Such an approach would also make possible an in-depth analysis of the interactions between the environmental, organizational, and professional factors of the Scheirer model, thus potentially allowing for the identification of additional dynamics. Second, the retrospective character of the analysis may have complicated the task for respondents. Longitudinal studies examining the capacity of teams to implement ecological programming initiatives in a context of change are promising. Third, although a case study design certainly allows for a rich, in-depth investigation of DPHP programming, it shows a limited potential in terms of generalizing results to other organizations in Québec or elsewhere. Replication with a larger number of cases and extensions to new organizational and geographical contexts are needed. Finally, it would be advantageous to integrate managers and interventionists more extensively into the research team. This participatory action research strategy is more attuned with the “ecological spirit” (Ryerson Espino & Trickett, 2008) and would maximize the potential for initiating a change agenda aimed at political and organizational environments that are more receptive to health promotion approaches.
Conclusion and Recommendations
Despite its limitations, this study identified factors influencing the integration of the ecological approach in DPHP program planning for older adults and thus provides orientation for policy makers and practitioners interested in implementing this approach. Including a more comprehensive set of priorities aimed at older adults within ministerial orientations and programming is certainly one of the first objectives to pursue. A second priority would be to insure that DSP team stability and budgetary resources required for implementing complex approaches are present. In this respect, establishing teams of professionals devoted to the older adult clientele and offering ongoing training on the ecological approach are promising strategies. Another important action lever involves developing partnerships across programming teams and external organizations including university milieus.
Footnotes
The author(s) declared no potential conflicts of interest with respect to the authorship and/or publication of this article.
The author(s) disclosed receipt of the following financial support for the research and/or authorship of this article: This work was supported by the Canadian Institutes for Health Research [CIHR #MOP-84549].