
Abstract
Depression frequently co-occurs in heart failure (HF) patients, causing significant interference and negative health outcomes. This case-controlled study explored the construct of illness intrusiveness and examined its relationship to HF severity and depression. Older veterans (n = 104) with an HF diagnosis completed a one-time assessment that included demographics, depressive symptoms (Geriatric Depression Scale), the Illness Intrusiveness Rating Scale (IIRS), and HF quality of life and functional abilities (Kansas City Cardiomyopathy Questionnaire [KCCQ]). Analyses included exploratory correlations between IIRS and KCCQ items, a confirmatory factor analysis (IIRS), and formal mediational analyses. Results indicated that the IIRS had adequate internal consistency and concurrent validity, with support for its established three-factor model. Regression analyses indicated that illness intrusiveness mediated HF illness severity and depression. In conclusion, illness intrusiveness may be a better indicator of depression than illness severity (HF symptoms); thus research methods and interventions targeted at reducing illness intrusiveness merit further investigation.
More than 85% of older adults report having a chronic medical condition, and of those afflicted almost 70% face two or more chronic illnesses (Hoffman, Rice & Sung, 1996). Heart disease is the leading cause of death in the United States (Kung, Hoyert, Xu, & Murphy, 2008), and heart failure (HF), one of the most chronic and debilitating cardiac conditions, is estimated to affect approximately 5 million Americans (American Heart Association, 2008). Rates of depression in HF are approximately two to three times the rate of community-based samples (Rutledge, Reis, Linke, Greenberg, & Mills, 2006). HF patients with depression differ from nondepressed patients by using significantly more health care services, experiencing greater functional declines, and being at increased risk of mortality (Cully, Johnson, Moffett, Khan & Deswal, 2009; Jiang et al., 2007; Rumsfeld et al., 2003; Rutledge et al., 2006; Vaccarino, Kasl, Abramson, & Krumholz, 2001). In addition, researchers have found that depression in HF patients is associated with poor quality of life (QoL; Cully, Phillips, Kunik, Stanley, & Deswal, 2010), reduced feelings of self-efficacy (Tsay & Chao, 2002), greater social conflict, and less active coping responses (Carels, 2004; Park, Fenster, Suresh, & Bliss, 2006). In contrast, perceived control has been found to be associated with less depression in HF patients (Dracup et al., 2003; Moser & Dracup, 1995). Medical illnesses often disrupt daily living activities, which can lead to a negative impact on emotional well-being. These perceived disruptions in daily activities (attributed to a chronic illness) have been labeled as illness intrusiveness (Devins et al., 1983). In noncardiac chronic conditions, the concept of illness intrusiveness (Devins et al., 1983) is significantly related to quality of life, subjective well-being, and emotional adjustment (Dancey, Hutton-Young, Moye, & Devins, 2002; Mullins et al., 2001; Schimmer et al., 2001). Illness intrusiveness differs from quality of life, which is defined as a broad concept that integrates physical, social, mental, and/or environmental factors. Illness intrusiveness specifically measures the self-perceived lifestyle disruptions that are attributed to illness symptoms and treatment.
Illness intrusiveness has been investigated in chronic illnesses such as end-stage renal disease, diabetes, and multiple sclerosis (Devins, Beanlands, Mandin, & Leendert, 1997; Mullins et al., 2001; Talbot, Nouwen, Gingras, Belanger, & Audet, 1999). Prior studies suggest that illness intrusiveness mediates the effects of illness and disease-related factors (Devins, Bezjak, Mah, Loblaw, & Gotoweic, 2006). Unfortunately, only one known study has examined illness intrusiveness in cardiac and/or HF patient populations (Paukert, LeMaire, & Cully, 2009). Paukert et al. (2009) found that perceived intrusiveness of HF symptoms and treatment was a significant predictor of depressive symptoms after controlling for physical limitations but did not examine the specific relationships between depression, HF severity, and illness intrusiveness.
The current study sought to expand the investigation by Paukert et al. (2009) by focusing on the use and impact of illness-intrusiveness ratings in older HF patients. The first aim of the study sought to test the statistical fit of the established three-factor structure of the IIRS ( Devins et al., 2001). The second aim sought to determine whether illness intrusiveness mediated the relationship between the severity of HF and depression.
Method
Participants
This case-control study enlisted participants from a large VA hospital using administrative databases. Medical records of veterans 60 years of age or older with a documented diagnosis of HF (n = 4,129) were extracted using a database search. Charts without critical information (e.g. contact data, insufficient medical record documentation)were excluded (n = 2,834). Of the remaining 1,295 participants, 304 participants were contacted by telephone and agreed to complete a telephone assessment to establish intial study inclusion criteria. Overall, 177 participants were excluded, including 11 for cognitive impairment (three or more errors on a brief cognitive screen; Callahan, Unverzagt, Hui, Perkins, & Hendrie, 2002), 67 for no HF functional impairment (New York Heart Association [NYHA] class I), and 23 for substance, thought, or bipolar disorder (Mini International Neuropsychiatric Inventory; [MINI; Sheehan et al., 1998]). Because the study recruited patients using a case-control approach, based on the presence or absence of depression and/or anxiety symptoms, 77 patients without significant levels of anxiety and/or depression (Geriatric Depression Scale [GDS] < 6; Yesavage et al., 1983; Geriatric Anxiety Inventory [GAI] <9; Pachana et al., 2007) were not enrolled. One hundred and twenty-seven patients were invited for an in-person assessment appointment, completed within 2 weeks of the telephone appointment. Twenty-three patients did not attend this appointment. The final sample consisted of 104 HF participants, half (52) of whom had significant levels of anxiety and/or depression.
Primary Study Measures
Geriatric Depression Scale (GDS)
The GDS Short Form is a 15-item self-report measure of depression (Sheikh & Yesavage, 1986) with good reliability and validity in older adult populations (Friedman, Heisel, & Delavan, 2005; Weeks, McGann, Michaels, & Penninx, 2003). The GDS has been used specifically in HF populations (Vaccarino et al., 2001) and can be administered effectively by telephone (Burke, Roccaforte, Wengel, Conley, & Potter, 1995). For this study, a cutoff of > 5 was used to determine the presence of clinically significant depressive symptoms.
The Kansas City Cardiomyopathy Questionnaire (KCCQ)–Physical Limitations Subscale (PLS)
The PLS is a subscale of the KCCQ, a well-validated, self-administered, disease-specific QoL inventory for HF patients (Green, Porter, Bresnahan, & Spertus, 2000). The PLS represents the physical deficits associated with HF and its symptoms of fatigue and shortness of breath. It has convergent validity with NYHA classifications and the 6-min walk test (Green et al., 2000). Given this convergent validity, the current study defines HF severity using the KCCQ PLS. The PLS includes six questions asking about activity limitations related to HF symptoms (e.g., dressing oneself) over the previous 2 weeks. Items are rated on a Likert-type scale and are consistent with semistructured interviews used to determine NYHA classification. Scores range from 0 to 100, with higher scores indicating better function.
Heart Failure Illness Intrusiveness Rating Scale (HF IIRS)
The IIRS is a 13-item instrument designed to measure perceived lifestyle disruptions (beyond physical limitations) resulting from the symptoms and treatment of a chronic illness (Devins et al., 1983). For example, the questionnaire asks, “How much does your HF and/or its treatment interfere with” important areas of life (e.g., work, social/family life). Each item is rated on a Likert-type scale with the total score reflecting perceived overall level of intrusiveness.
The IIRS scale has demonstrated good reliability and validity with a variety of chronic illness populations (Devins et al., 1990, 2006; Schimmer et al., 2001). Devins et al. (2006) found three underlying IIRS factors, labeled as Relationships and Personal Development, Intimacy, and Instrumental Life Domains.
Notably, the HF IIRS and the KCCQ PLS represent different constructs. The HF IIRS is a measure of the perceived global disruption of physical health difficulties on lifestyle factors, and the PLS is a subjective measure of the actual physical health difficulties associated with HF symptoms and closely resembles concepts in the NYHA classification system.
Analyses
A confirmatory factor analysis (CFA) using LISREL, version 8.80 (Scientific Software International, Lincolnswood, IL) was applied to the IIRS data to determine the consistency of the previously identified three-factor structure of the IIRS (Devins et al., 2001) with an older HF population. CFA is a theory-testing procedure that specifies how many factors there are, which factors the variables will load, and the relative importance of each item within the factor (Stevens, 2002).
To test the hypothesis that illness intrusiveness partially mediates the relationship between HF severity and depression, we used Barron and Kenny’s (1986) classic four-step regression method. The first regression equation (i.e., Step 1) required the predictor (HF severity) and outcome variable (depression) to be significantly related. The second regression equation required the predictor (HF severity) and mediator variable (illness intrusiveness) to be significantly related, and the third regression equation required the mediator (illness intrusiveness) and predictor (HF severity) to be significantly related to the outcome variable (depression). The fourth regression equation tested whether the strength of the relationship between the predictor (HF severity) and outcome (depression) remained significant when the mediating variable (illness intrusiveness) was added to the model.
Results
Ninety-nine percent of the participants in the sample were men (mean age = 71.1; SD = 7.7). Most participants were White (n = 75, 72%) and married (n = 60, 58%); had more than a high school education (n = 60, 59%); earned than less than US$20,000 per year (n = 58, 56%); and lived with a spouse, family member, or friend (n = 76, 73%).
To evaluate the concurrent validity of the IIRS, correlations were examined between IIRS total and subscale scores and KCCQ items that correspond to the IIRS domains of interest. Specific items selected from the KCCQ included Item No. 5, fatigue; Item No. 7, shortness of breath; Item No. 12, how HF limited enjoyment of life; Item No. 15a, HF interference with hobbies/recreation; Item No. 15b, HF interference with working/household chores; Item No. 15c, HF interference with visiting family/friends; and Item No. 15d, HF interference with intimate relationships. All correlations between the IIRS and KCCQ items were moderate-to-large negative correlations, indicating strong inverse relationships. Lower scores on the KCCQ indicate greater reported impairment/interference; and the reverse is true for the IIRS (see Table 1).
Pearson Correlations Between IIRS Total and Subscale Scores and KCCQ Items
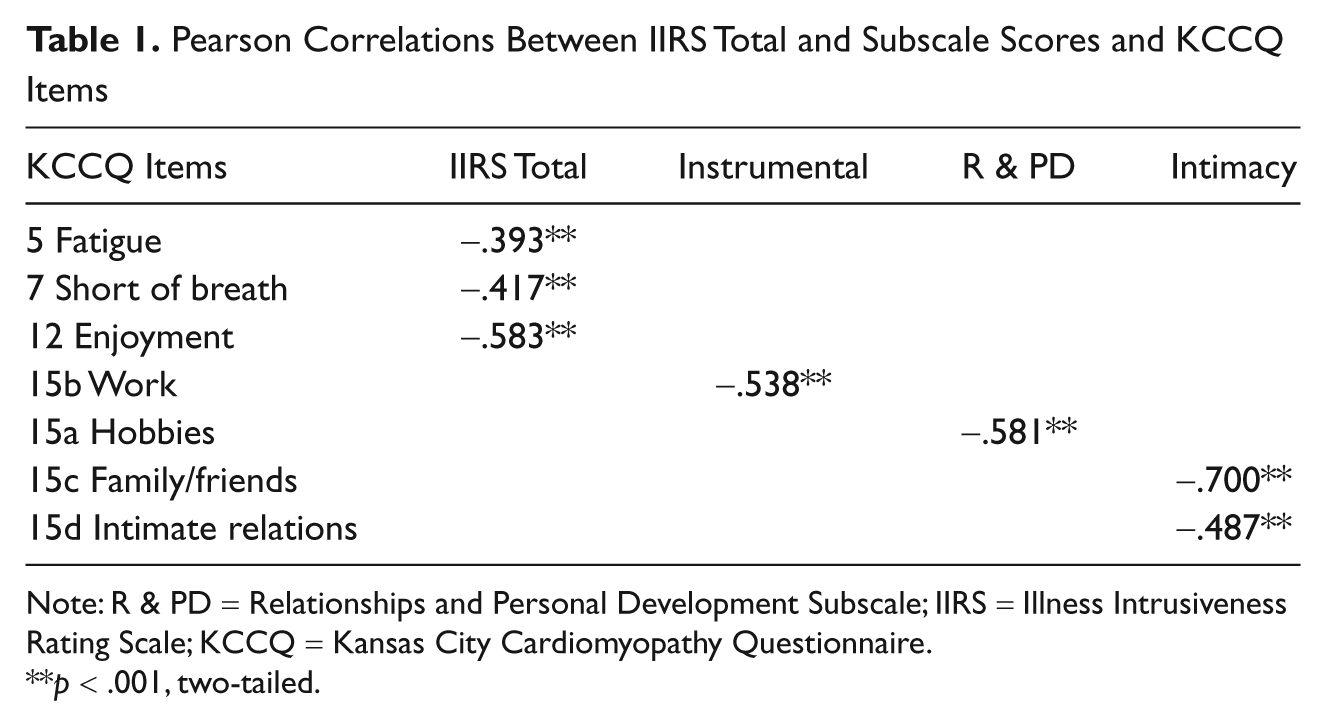
Note: R & PD = Relationships and Personal Development Subscale; IIRS = Illness Intrusiveness Rating Scale; KCCQ = Kansas City Cardiomyopathy Questionnaire.
p < .001, two-tailed.
Confirmatory Factor Analysis
Table 2 displays the factor loadings obtained from the CFA. The adjusted goodness-of-fit index (Joreskog & Sorbom, 1993) was used to test the overall model fit of the three-factor model (adjusted fit index = 0.82), the normed fit index (Bentler & Bonnett, 1980) was used to compare the hypothesized model to that of a null model (normed-fit index = 0.93), and the root mean square error of approximation (Steiger, 1990) was used to measure lack of model fit (root approximation = 0.08). All items had significant loadings (>.40; Stevens, 2002) on the factors they were intended to measure. The largest factor correlation for the model was between Instrumental and Intimacy (r = .91), followed by Relationships and Personal Development and Intimacy (r = .86), and then Instrumental and Relationships and Personal Development (r = .84). All correlations were greater than .60, indicating a strong relationship between factors.
Factor Loadings
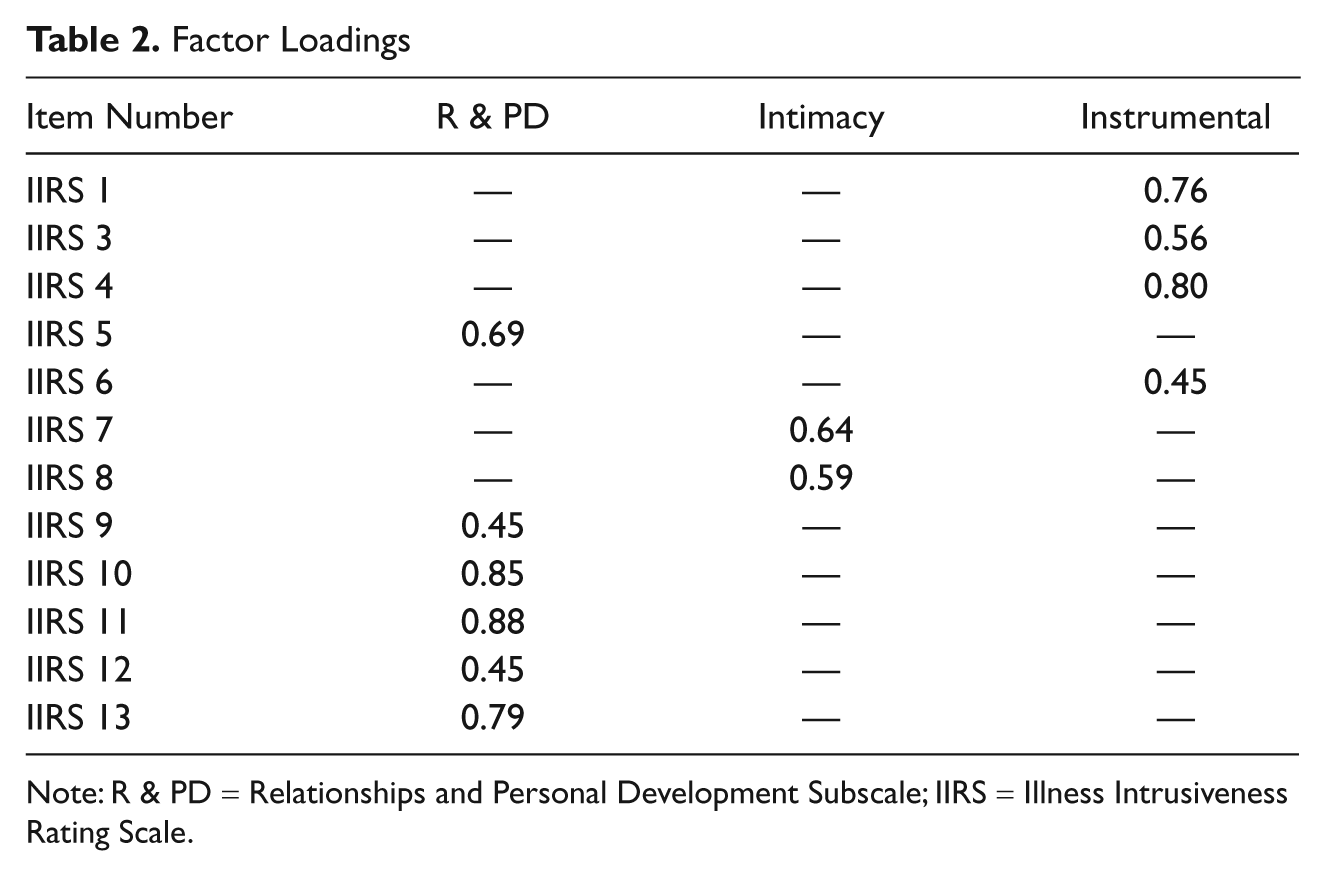
Note: R & PD = Relationships and Personal Development Subscale; IIRS = Illness Intrusiveness Rating Scale.
Mediational Results
Results from the CFA indicated a strong relationship between factors (e.g., Instrumental, Relationships and Personal Development, and Intimacy), suggesting that one rather than three distinct factors may be most appropriate for this sample. As a result, the total IIRS score was used as the mediator representing illness intrusiveness. HF severity (KCCQ PLS) was used as the independent variable, and depression (GDS)_was used as the dependent variable.
Significant effects were found for relationships between HF severity and depression, Figure 1; R2 = .11, F(1, 102) = 12.38, p < .001. When entered as full meditational model, significant effects were found for HF severity and illness intrusiveness, R2 = .33, F(1, 102) = 44.45, p < .000, and illness intrusiveness and depression, Figure 2; R2 = .13, F(1, 102) = 15.12, p < .000. When illness intrusiveness was accounted for in the full model, the direct effect between HF severity and depression became nonsignificant (Figure 2; t = −1.65, p > .05), suggesting that illness intrusiveness mediated the relationship between HF severity and depression.
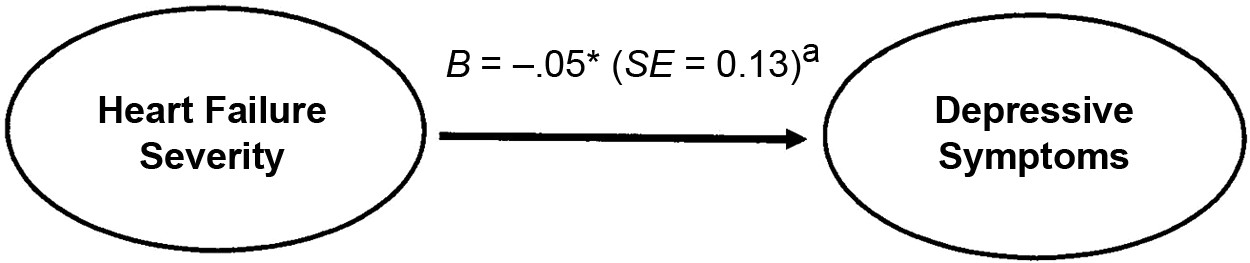
Path diagram without mediator

Path diagram with mediator
Discussion
The current study found that illness intrusiveness mediated the relationship between illness severity and depressive symptoms in HF patients. As noted in other studies (Dancey et al., 2002; Devins et al., 1990; Mullins et al., 2001), illness severity is not the best indicator of depression in chronic illness populations. Rather, the perceived disruptions to the patient’s life, as a result of illness symptoms and treatment, appear more significant. These findings support the claim that illness severity (an often unchangeable factor) may be of secondary importance to illness intrusiveness (a potentially modifiable factor).
These results further highlight the need for frontline providers to assess the functional and emotional impact of physical health difficulties in addition to physical health markers. Overreliance on physical examination or laboratory report may misrepresent the actual impairment or difficulties experienced by the individual patient. For example, certain patients with strong social support and/or higher levels of resiliency may experience few limitations from a severe chronic illness such as HF; other patients with milder forms of the illness may face greater perceived impairment, not indicated by the severity of the physical disease. Therefore, the use of an illness-intrusiveness framework may provide clinicians with a more accurate picture of patient functioning and provide valuable information to address the unique physical and emotional health needs of the patient.
Another goal of the present study was to evaluate the psychometric properties of the IIRS with HF patients. Within this HF sample, the total IIRS scale and two of the subscales showed good internal consistency and concurrent validity (with a measure of HF-related QoL). Previous findings by Devins et al. (2001) identified a three-factor underlying structure of the IIRS, which was supported in this sample of HF patients. However, the high correlations between the three factors suggest that the IIRS may be best interpreted as a total score.
Collectively, results from this study support the general use of the IIRS within a HF patient population. Importantly, HF patients in this sample had higher total illness-intrusiveness levels than most previously studied chronic illness populations, such as transplant (Schimmer et al., 2001), end-stage renal disease (Devins et al., 1990), and rheumatoid arthritis (Devins et al., 1993), suggesting that HF patients may experience some of the most intense levels of intrusiveness from their physical illness.
Limitations of this study include the cross-sectional (rather than longitudinal) design and the modest sample size, given the sophisticated statistical methods used. As such, causal inferences cannot be made but only suggested. Additional observational and interventional research is needed to evaluate the role of illness intrusiveness in medically ill patient populations.
Summary
This study illustrates the importance of illness intrusiveness in mediating the relationship between severity of HF and depression and the potential utility of assessment tools such as the IIRS to provide a richer understanding of HF patients who might be at risk for depression.
Footnotes
Authors’ Note
When they worked on this project, Ashley LeMaire, Amit Shahane and Tam Dao were affiliated with the Michael E. DeBakey Veterans Affairs Medical Center, and Ashley LeMaire was also affiliated with Baylor College of Medicine. Tam Dao was also affiliated with the Veterans Affairs South Central Mental Illness Research, Education and Clinical Center.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interests with respect to the authorship and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research and/or authorship of this article:This work was supported in part by a VA HSR&D Career Development Award (JAC; CDA-2 05-288), the Veterans Affairs South Central MIRECC Pilot Study Program, and the Houston Veterans Affairs HSR&D Center of Excellence (Houston Center for Quality of Care & Utilization Studies, HFP90-020). The views expressed represent those of the authors and not necessarily the Department of Veterans Affairs (Baylor College of Medicine).