
Abstract
Local Long-Term Care Ombudsman Programs (LLTCOPs) protect the health, safety, welfare, and rights of residents in long-term care (LTC) facilities. This study examines the (a) existing resources available to LLTCOPs in Georgia, California, and New York, (b) relationship of resources to LLTCOP’s reported effectiveness in meeting its federal mandates, and (c) state-specific mediating factors influencing LLTCOPs’ resources and reported effectiveness. Quantitative and qualitative data from the National Ombudsman Reporting System (NORS) and a telephone survey of LLTCOPs in Georgia, California, and New York were collected and analyzed. Resource adequacy, as measured by beds per full-time equivalent staff (beds/FTE), is inconsistently associated with effectiveness in meeting federal mandates across and within the states studied. Analysis of alternate resource measures suggests a threshold of LLTCOP size, under which program effectiveness may be lower. LLTCOPs report the changing LTC environment and additional state mandates as factors influencing resource adequacy.
Long-term care (LTC) ombudsmen are advocates for residents of LTC facilities, serving some of the most vulnerable individuals in our society. Mandated in 1978 under the Older Americans Act (OAA), the Long-Term Care Ombudsman Program (LTCOP) is designed as a resource to provide independent and effective oversight over the quality of care and life of residents in LTC facilities by advocating for their health, safety, welfare, and rights. Although most states have local LTCOPs (LLTCOPs) in addition to the mandated Office of the State LTC ombudsman, some states operate with only a state office. In states with both, the state LTCOP office provides oversight and guidance to LLTCOPs, as well as program representation with state agencies, departments, and administration.
Nationwide, LTCOPs serve more than 2.8 million residents in over 62,000 LTC facilities (nursing homes and board and care facilities, Administration on Aging, 2009). Recent data indicate that more than 1,300 paid and 8,700 certified volunteer staff investigate more than 271,000 complaints nationally each year, provide information to more than 327,000 consumers, work with more than 21,000 resident councils and 4,900 family councils, and conduct trainings for other ombudsmen (more than 7,257), facility staff (more than 7,600), and the local community (more than 10,000, National Long-Term Care Ombudsman Resource Center, 2010). The LTCOP’s federally mandated activities include complaint investigation; community education; resident and family education; monitoring federal, state, and local laws and regulations, and other government policies and actions; and systems advocacy, including legislative and administrative policy advocacy.
Purpose of the Study
This research investigates the (a) existing resources available to LLTCOPs in three states: Georgia, California, and New York, (b) effects of resources on LLTCOP reported effectiveness in meeting mandates, and (c) state-specific mediating factors that shape LLTCOP resource adequacy and that are associated with reported effectiveness. Comparison of LLTCOP resources, within and among different states, may contribute to an understanding of the common and diverse challenges, best practices, and potential policy solutions for LLTCOPs.
Background
In 1995 the Institute of Medicine (IOM) commissioned a report evaluating the LTCOP and its work in representing residents of LTC facilities. The IOM study identified insufficient resources as a factor associated with the effectiveness of state LTCOPs. This study was to be followed by a 50 state study funded by the Kaiser Family Foundation (KFF; Estes, Zulman, Goldberg, & Ogawa, 2004) and 4 separate statewide studies of LLTCOPs in California, New York (Estes, Goldberg, Lohrer, Nelson, & Hollister, 2006; Estes et al., 2010), Illinois (Hughes, 2007), Ohio (Wellin & Kart, 2008 ), and Georgia (Estes, Hollister, & Goldberg, 2007). All of the aforementioned studies, the IOM national study, the 50 state KFF funded study, and the 5 individual state studies’ (funded by private foundations and public funds) illustrate the continued interest of those concerned with long-term care policy in evaluating and strengthening the LTCOP. Previous studies have recommended that resources be increased to allow state and LLTCOPs to more effectively meet the needs of residents and fulfill their state and federally mandated activities (Estes et al., 2004; Estes et al., 2006; Estes et al., 2007; Estes et al., 2010; Harris-Whehling, Feasley, & Estes, 1995; Hollister, 2008; O’Shaughnessy, 2009).
Although recommendations and best practices have been developed based on past studies, the variability of LLTCOPs identified both within and across states makes the adoption and implementation of best practices models difficult. Nevertheless, the 1995 IOM report recommended LTCOP staffing ratios of no less than one paid (full-time equivalent staff) FTE staff for every 2,000 licensed LTC beds within any state. Since the IOM study, the ratio of beds per full-time equivalent staff (beds/FTE) has most commonly been used as a LTCOP resource measure in research and as a tool to advocate for additional program resources. The present study calls attention to the fact that the bed ratio only captures the resources needed to conduct complaint investigation and, to a certain extent, resident and family education. The researchers contend that the IOM ratio lacks the complexity to measure the resources needed for LTCOPs to provide community education; monitor federal, state, and local laws and regulations; and conduct systems advocacy. Continued evaluation of the LTCOP has allowed for a closer look at the responsibilities of LTCOPs and their resources, leading to a more nuanced understanding of resource adequacy. The study data collected provide the first step toward assessing and creating an improved set of LTCOP resource measures.
Types of Resources
To meet their state and federally mandated activities, LLTCOPs rely on several types of resources including funding, staff, and volunteers.
Funding
LLTCOP’s primary federal funding source is through the Older American’s Act (Title III and VII). Some programs apply for and receive additional funding through federal grants, private foundations, and state government. These sources of funding are often attached to additional mandated activities. Funding resources are used for personnel, office space, educational materials, and other operating expenses (transportation, internet access, phones, and faxes). Sufficient funding resources are needed to sustain the level of staff and volunteers (which require training and supervision) to perform their five federally mandated activities.
Staffing
Paid LLTCOP staff may include a program coordinator, administrative staff, paid ombudsmen, and a volunteer coordinator. The yearly full-time salary ranges for local ombudsmen vary greatly both across and within states (MacInnes & Hedt, 1999) and the salaries are generally modest at best, making the recruitment and retention of educated, experienced, dedicated, and resourceful staff difficult.
Volunteers
The LTCOP was initially conceptualized as a program relying heavily on volunteer resources. However, the use of volunteers and beliefs about their roles within the LLTCOP vary widely in practice (Nelson, Netting, Huber, & Borders, 2004; Netting & Hinds, 1989). Volunteers and paid FTE staff often assume different responsibilities, resulting in a triaging of the work of the LTCOP (Netting, Huber, Borders, Kautz, & Nelson, 2000).
Research Design and Method
A collaborative, community-based, participatory research design is used for this research. This research was conducted in collaboration with the local Ombudsman Associations and the state LTCOPs in Georgia, California, and New York. The research was designed to be action oriented, with the goal of producing knowledge and outcomes that are relevant to stakeholders and that are likely to facilitate positive change (Israel et al., 2003).
The comparison of issues confronting LLTCOPs within and across three geographically, demographically, economically, and politically diverse states (Georgia, California, and New York) seeks to produce information regarding program strengths and weaknesses. California and New York ranked first and third, respectively, in the number of people aged 85 and over in the United States (U.S. Census Bureau, 2011). The Georgia state LTCOP and LLTCOPs are often referred to as exemplary; presenting best practices on a variety of challenges with local and state policies and procedures replicated nationwide. 1
This research uses quantitative and qualitative data from the UCSF/IHA LLTCOP telephone survey and the quantitative National Ombudsman Reporting System (NORS) maintained by the Administration on Aging. Data were examined both within and across states to examine the relationships between the independent variables (resource measures, including bed/FTE) and dependent variables (self-rated effectiveness in meeting mandated activities).
The study hypothesizes that LLTCOPs serving fewer beds/FTE will report higher effectiveness in meeting their mandated activities. A second research hypothesis is that additional dimensions of resources will be associated with the reported effectiveness of LLTCOPs. Third, it is hypothesized that mediating factors, such as the changing LTC environment and additional unfunded state mandates, will be associated with the reported effectiveness of LLTCOPs.
Study Participants
All LLTCOP coordinators in Georgia (15) and California (35; 100% response rate), and 39 of New York’s 50 LLTCOP coordinators (78% response rate) participated in the research. Analysis of potential bias determined that nonrespondents in New York did not differ significantly from respondents, as measured by available NORS data (Hollister, 2008). The Georgia interviews were conducted between April 2007 and August 2007. Interviews were conducted in California and New York between March and July of 2004.
Instruments
Survey questions were generated based on a thorough review of prior research and data collected, issues raised and recommendations set forth by the 1995 IOM report, a 50 state Kaiser Family Foundation study (Estes et al., 2004), and recommendations of the project advisory committee members and consultants. The survey for LLTCOP coordinators contains both closed and open-ended items. Instrument measures include yes/no questions and 4-point Likert-type scales of effectiveness, agreement, and ability.
Data Collection
Researchers contacted LLTCOP coordinators by mail to request participation in the survey interview. A few weeks later a project researcher contacted each of the potential subjects (15 in GA, 35 in CA, and 50 in NY) to obtain consent and schedule an interview. The secondary NORS data 2 collected is the only source of national data about LLTCOPs. The time period of NORS data collected and when interviews were conducted are proximate but not identical.
Data Analysis
All quantitative data from LLTCOP survey interviews and NORS data were entered into a data file and analyzed using SPSS. Quantitative data analysis focused on program resources and their relationship to LLTCOP coordinators’ reported effectiveness in meeting their federally mandated activities. Quantitative analysis consisted of basic associations determined through comparisons of means, medians, proportions, and summary measures. Because the data collected are for the universe of LLTCOPs in each state, statistical tests are not used to evidence the generalizability of the data to any larger population of LLTCOPs. The median is used rather than the mean because of the skewed nature of the data and to better compare the measures across states. When informative for specific measures, range is presented to highlight within-state variation.
Qualitative data were analyzed using ATLAS.ti coding software. Qualitative analysis uses a general inductive analytical approach, allowing research findings to emerge from the frequent, dominant or significant themes found in the data (Ezzy, 2002). Content was examined for the following themes: (a) resource adequacy, (b) program effectiveness, and (c) factors influencing resource adequacy.
Program Effectiveness Measures (Dependent Variable)
LLTCOP coordinators provided ratings of their program’s efficacy in each of the five federally mandated activities: (a) complaint investigation; (b) community education; (c) resident and family education; (d) monitoring federal, state, and local laws and regulations, and other government policies and actions; and (e) systems advocacy. Effectiveness ratings were provided on 4-point Likert-type scales (0 = very ineffective to 3 = very effective). Although not providing an absolute criterion of program performance, self-rated efficacy measures have been used in prior research efforts in this topic area (Estes et al., 2004; Estes et al., 2006; Estes et al., 2007; Estes et al., 2010; Harris-Whehling et al., 1995; Hughes, 2007).
Resource Adequacy Measures (Independent Variable)
Twelve measures are included under the category of resource adequacy. From the NORS data, measures include the number of (a) paid FTE staff, (b) volunteers, (c) LTC beds served (both nursing home and board and care beds), (d) LTC facilities served (both nursing home and board and care facilities), and (e) program budget dollars. NORS data were also used to calculate a series of six ratios: (f) beds/FTE, (g) facilities/FTE, (h) volunteers/FTE, (i) budgeted dollar/bed, and (j) budgeted dollar/facility. The remaining measures of resources were based on survey responses to two questions: (k) “Does your local LTCOP have a sufficient amount of funding to carry out all of its state and federal Mandates, would you say, ‘Yes’ or ‘No’?” and (l) “In your best estimate, how much additional funding, if any, would be necessary on an annual basis, in order to enable your local LTCOP to meet all mandated state and federal requirements?”
Findings
LLTCOP coordinators report a lack of resources (time, money, and personnel) and the need to prioritize some mandates (e.g., complaint investigation) over others (e.g., systems advocacy). Wide variation characterized most of the descriptive characteristics of LLTCOPs, evidenced by large standard deviations and widely differing mean and median scores.
Facilities and Beds
Georgia and California LLTCOPs serve a similar median number of beds (3,615 and 3,566, respectively) and facilities (114 and 97, respectively). New York LLTCOPs’ much lower median number of beds (742) and facilities (12) reflect the large number of very rural areas in New York State. New York LLTCOPs also report a larger range of beds served across the state than Georgia and California, reflecting New York City’s size in comparison with the remainder of New York State. New York LLTCOPs serve larger facilities with a median of 76 beds/facility compared with Georgia (32) and California (35) LLTCOPs.
LLTCOPs in each state serve more board and care homes than nursing homes, with California and Georgia serving a much higher proportion of board and care homes than nursing homes (CA: 84% of facilities served are board and care homes, GA: 71%) than New York LLTCOPs (52%).
Although all LLTCOPs serve a larger proportion of board and care homes than nursing homes, in Georgia and New York the majority of beds served are located in nursing homes (GA: 59% nursing homes, NY: 76%). In contrast, a majority of beds served by California LLTCOPs reside in board and care homes (57%). New York LLTCOPs serve the largest proportion of nursing home facilities and beds out of the three states. These findings suggest that although Georgia and California’s LTC systems have become less institutionalized (i.e., more board and care homes than nursing homes), a majority of LTC residents in New York still reside in nursing homes.
Funding
LLTCOP funding (from all sources) varies widely. New York LLTCOPs report the lowest median budget (US$14,127) compared with Georgia (US$114,345) and California (US$141,719). New York LLTCOPs also report the widest budget range (US$842,000) compared with Georgia (US$650,432) and California (US$672,251). This range reflects the existence of one large and many very small programs within New York. However, if program size was taken into account, one would expect the ratio of budget/bed to be similar across states. Although this is evident in Georgia (US$39) and California (US$40), New York LLTCOPs receive about half of the budget/bed of these states (US$19).
California LLTCOPs are most likely to report that they do not have adequate funding (78%), compared with Georgia (60%), and New York (51%). Budget uncertainty also appears to be a major concern.
The program is always in danger of losing money . . . We’re never sure exactly what we are going to get . . . The Older American’s Act is in danger of losing over a million dollars . . . If there are changes in the budget for my program, I would be in danger of losing the only staff person I have. (GA)
When LLTCOPs reporting inadequate funding were asked how much additional funding was needed, New York LLTCOPs report needing a median 100% increase, Georgia a median 28% increase, and California a median 38% increase.
Staff and Volunteers
Georgia LLTCOPs report the highest median number of paid FTE staff (3.00), followed closely by California (2.75), and distantly by New York (.36). Only 15% of New York LLTCOPs report a full-time coordinator, compared with 91% in California and 93% in Georgia.
Despite reporting the smallest number of paid FTE staff, New York LLTCOPs report a median of eight certified volunteers per LLTCOP. California has the highest median number of volunteers (24) and Georgia the lowest (7 statewide).
The 1995 IOM study recommended a ratio of one paid FTE staff to 20-40 volunteers. On average, New York LLTCOPs report the most volunteers/FTE (21.56), followed by California (8.03) and Georgia (0.15). The training and certification requirements for volunteers vary across states, which may alter the numbers reported. There are differences in opinion regarding the value of volunteers across LLTCOPs: I am a small program. We deal with three facilities and I have four volunteers—It’s a total of 289 beds—so . . . we have more resources to do things. (CA) Ombudsman need to be perceived more as professionals and funded as such. This takes a lot of training and skill and we are dealing with very complex issues. We need to be recognized as professionals, which is not reflected in the federal and state funding and legislation. Everyone talks about it as a volunteer program, but very professional staff is needed to do what we do. (CA)
Without adequate paid FTE staff, one coordinator fears that “the program will become a paper tiger” (CA) with poorly trained volunteers acting as friendly visitors rather than advocates.
Workload
The 1995 IOM report recommended that LLTCOP workload not exceed 2,000 beds/ FTE. Georgia and California LLTCOPs report similar median beds/FTE (1,407 and 1,503, respectively) compared with the median 2,137 beds/FTE served by New York LLTCOPs.
Two Georgia (13%), 10 California (30%), and 22 New York (55%) LLTCOPs report serving more beds/FTE than the IOM standard. The heaviest workload among New York LLTCOPs is 7,163 beds/FTE compared with 4,476 beds/FTE in California and 2,169 beds/FTE in Georgia.
Although New York LLTCOPs serve the highest median number of beds/FTE, they also serve the lowest median number of facilities/FTE (29). Georgia and California LLTCOPs serve a similar median number of facilities/FTE (45 and 47, respectively). The need to visit more facilities, each housing fewer residents, places stress on LLTCOP staff and transportation funding.
LLTCOP Effectiveness
Figure 1 illustrates the aggregated state-level differences in reported effectiveness for each of the five federally mandated activities. Although there are similarities in the general pattern of responses across Georgia, California, and New York, a higher proportion of Georgia LLTCOPs report being very effective in meeting all five mandates, than LLTCOPs in California and New York. LLTCOPs in California and Georgia are least likely to rate their program as very effective in monitoring federal, state, and local laws and regulations and systems advocacy. Less than one third of LLTCOPs in New York rate their program as very effective in meeting any mandate other than complaint investigation.

Proportion of Georgia, California, and New York LLTCOP coordinators that rate their programs as very effective in meeting specific federally mandated requirements
To examine the relationship between resources and LLTCOP effectiveness, a dichotomous workload variable was created by separating programs with workloads heavier than the bed/FTE median from those with workloads lighter than the beds/FTE median. State-specific bed/FTE medians are used to capture within-state variation and across-state differences.
Bed/FTE Resource Measure and LLTCOP Effectiveness
Georgia LLTCOPs with heavier workloads (more beds/FTE) are less likely than those with lighter workloads to report being very effective in meeting all five of the federally mandated activities (Table 1).
Effect of Resources on the Proportion of Georgia, California, and New York LLTCOP Coordinators That Rate Their Programs as Very Effective in Meeting Federally Mandated Requirements.
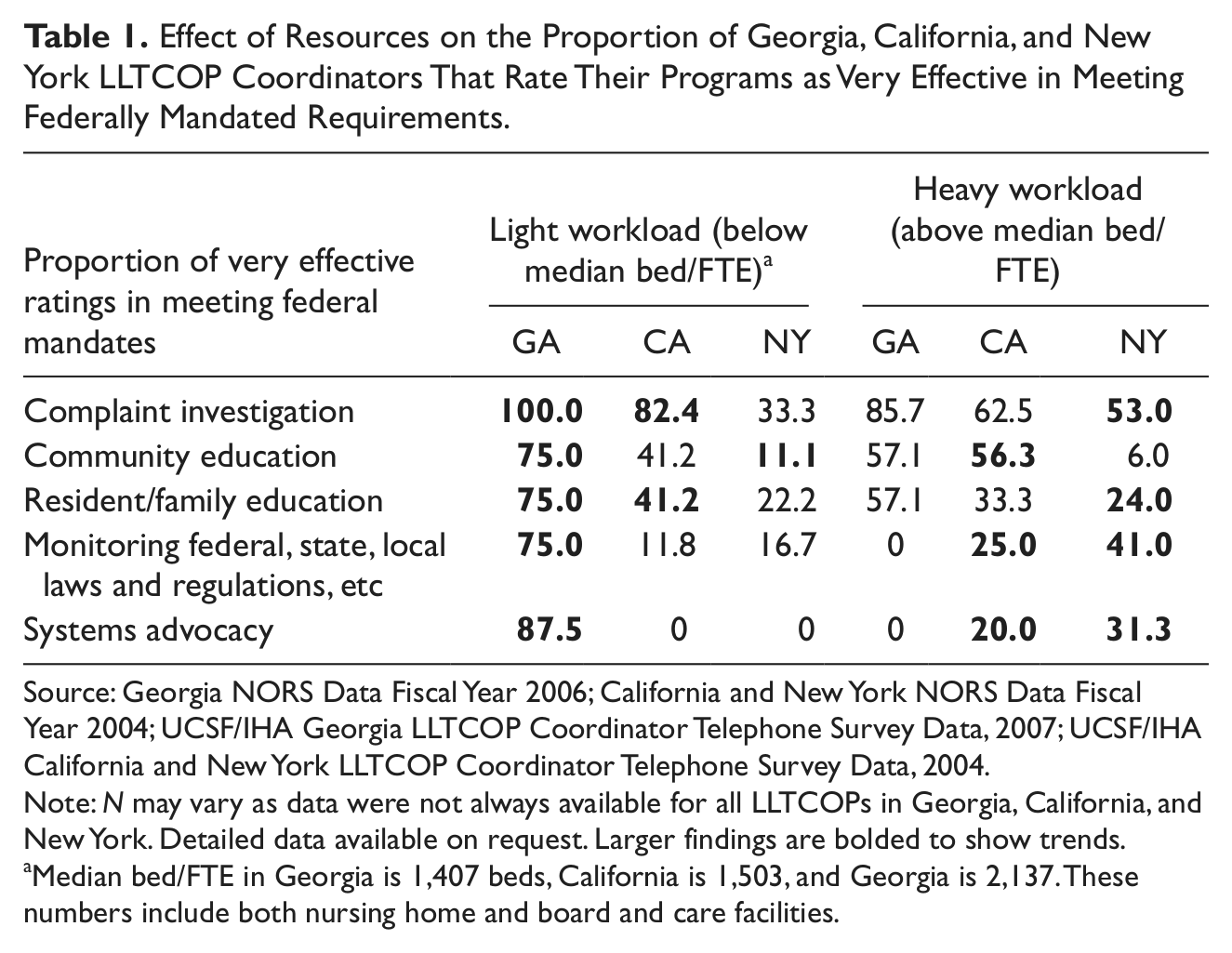
Source: Georgia NORS Data Fiscal Year 2006; California and New York NORS Data Fiscal Year 2004; UCSF/IHA Georgia LLTCOP Coordinator Telephone Survey Data, 2007; UCSF/IHA California and New York LLTCOP Coordinator Telephone Survey Data, 2004.
Note: N may vary as data were not always available for all LLTCOPs in Georgia, California, and New York. Detailed data available on request. Larger findings are bolded to show trends.
Median bed/FTE in Georgia is 1,407 beds, California is 1,503, and Georgia is 2,137. These numbers include both nursing home and board and care facilities.
California and New York LLTCOPs report varying associations between workload and effectiveness in complaint investigation, community education, and resident and family education. In California, LLTCOPs with heavier workloads are more likely to report being very effective in community education; monitoring federal, state, and local laws and regulations; and systems advocacy. New York LLTCOPs with heavier workloads are more likely than those with lighter workloads to rate their programs as very effective in all activities except community education.
In summary, resource adequacy as measured by workload (beds/FTE) is positively associated with all measures of effectiveness in Georgia. However, there is less consistency in both California and New York. Study results suggest that the simple IOM resource measure of beds/FTE either (a) lacks the complexity needed as a measure of LLTCOP resource adequacy or (b) resources, as measured by beds/FTE, do not have the same effects on California and New York LLTCOP effectiveness as they do on Georgia LLTCOPs.
Conceptually, the beds/FTE measure of resource has several limitations. The beds/FTE measure does not take into account (a) systems-level work required of LLTCOPs that is not captured in bed ratios (community education; monitoring federal, state, and local laws and regulations; and systems advocacy); (b) additional state mandates such as California’s abuse reporting mandate, and Georgia’s mandate to serve additional types of facilities as well as diverse populations of residents; (c) volunteer resources that may alleviate (or exacerbate) the workload of FTE staff; (d) the geographic distributions, number of facilities served, and travel reimbursements that may limit access to facilities; (e) the qualifications of LLTCOP staff that likely reflect the salaries offered; and (f) interorganizational relationships that may facilitate (or impede) the LLTCOP’s work. For these reasons, this research examines alternate measures of resources and potential mediating factors related to resources and effectiveness such as the changing LTC environment and additional unfunded state mandates.
Alternate Resource Measures and LLTCOP Effectiveness
Alternate measures of resources (FTEs, volunteers, beds, facilities, budget) were analyzed by splitting each measure into a dichotomous variable by their median (state-specific) and comparing the reported effectiveness of each group (Tables 2, 3, and 4). In Georgia, volunteer resources are measured by comparing the three LLTCOPs with volunteers to those with none. Large programs are those that report higher numbers of paid FTE staff, volunteers, beds, facilities, and a larger budget in each state.
Effect of Different Measures of Resources on the Proportion of Georgia LLTCOP Coordinators That Rate Their Program as Very Effective in Meeting Mandates and Serving Facilities.
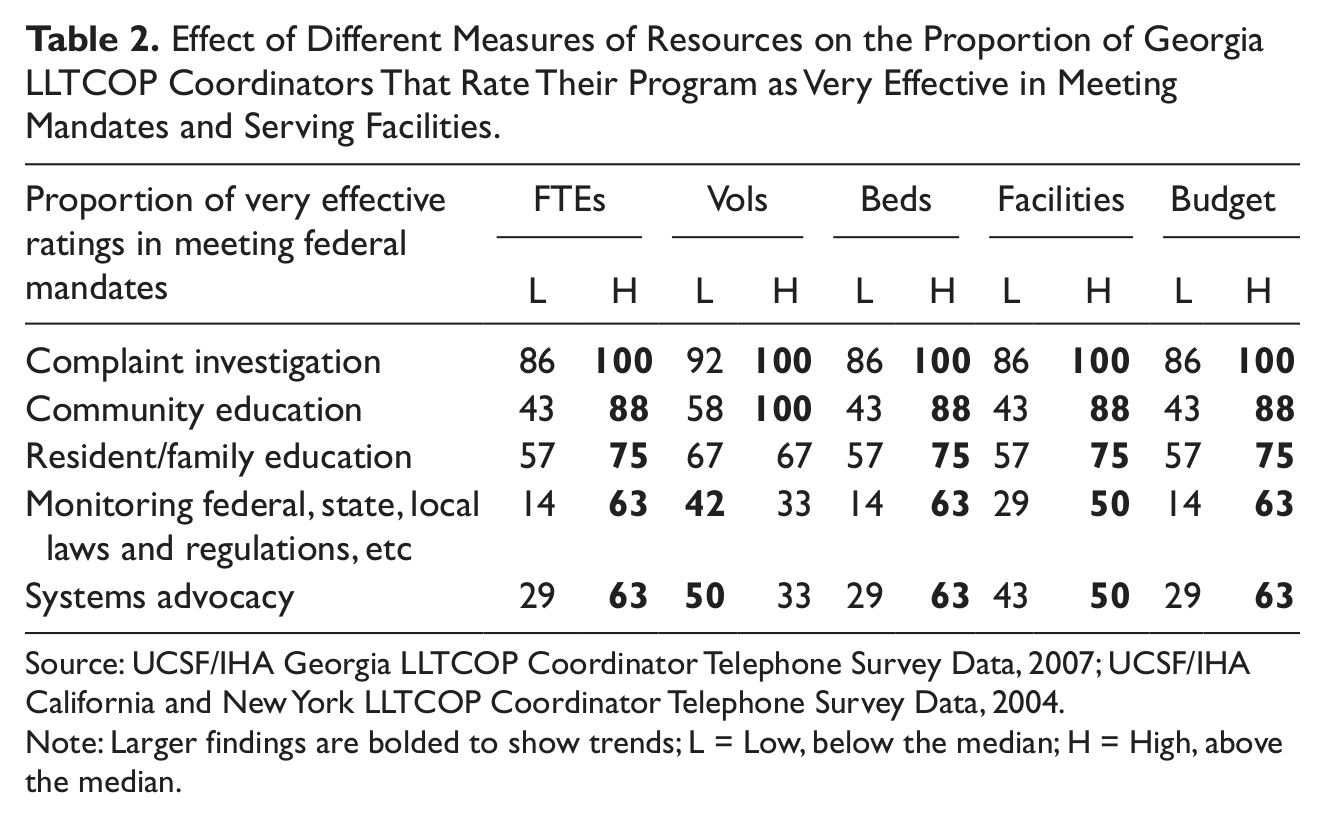
Source: UCSF/IHA Georgia LLTCOP Coordinator Telephone Survey Data, 2007; UCSF/IHA California and New York LLTCOP Coordinator Telephone Survey Data, 2004.
Note: Larger findings are bolded to show trends; L = Low, below the median; H = High, above the median.
Effect of Different Measures of Resources on the Proportion of New York LLTCOP Coordinators That Rate Their Program as Very Effective in Meeting Mandates and Serving Facilities.
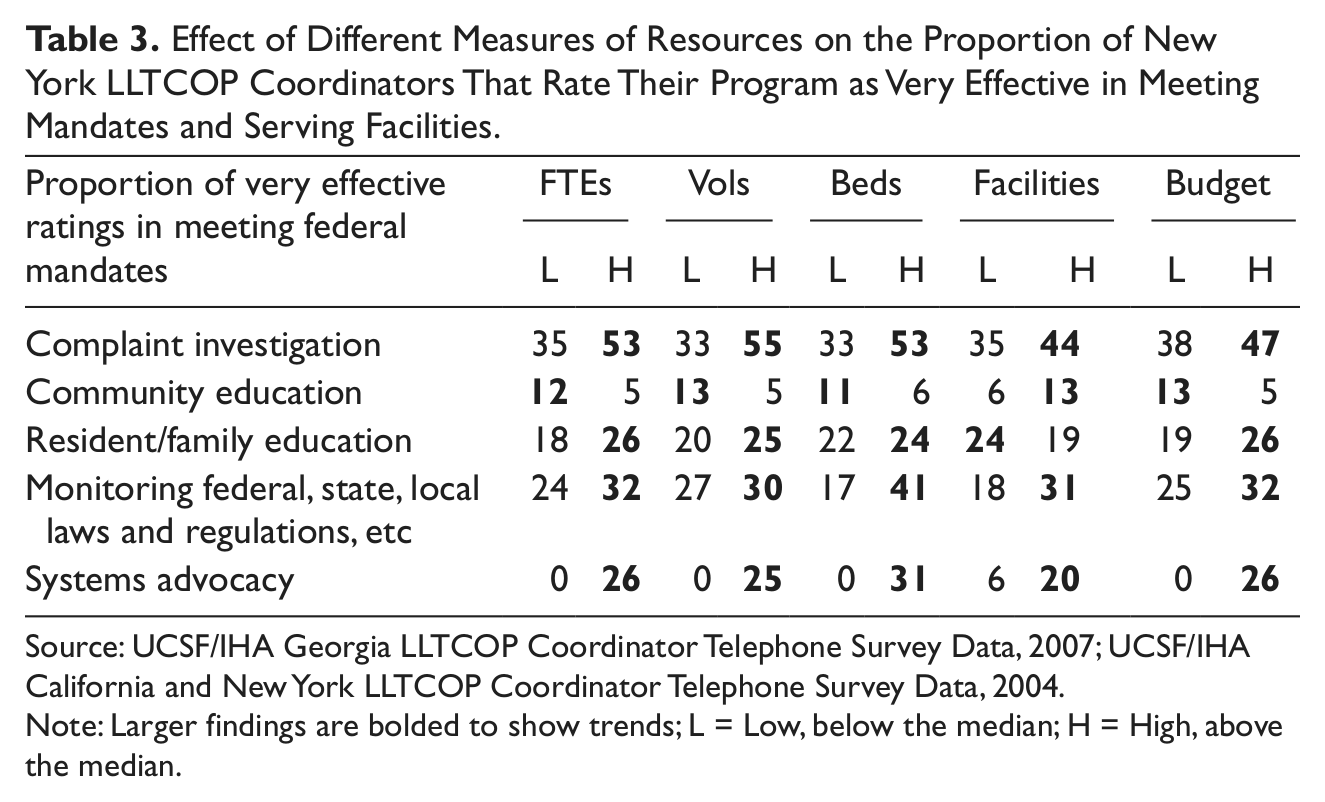
Source: UCSF/IHA Georgia LLTCOP Coordinator Telephone Survey Data, 2007; UCSF/IHA California and New York LLTCOP Coordinator Telephone Survey Data, 2004.
Note: Larger findings are bolded to show trends; L = Low, below the median; H = High, above the median.
Effect of Different Measures of Resources on the Proportion of California LLTCOP Coordinators That Rated Their Program as Very Effective in Meeting Mandates and Serving Facilities.

Source: UCSF/IHA Georgia LLTCOP Coordinator Telephone Survey Data, 2007; UCSF/IHA California and New York LLTCOP Coordinator Telephone Survey Data, 2004.
Note: Larger findings are bolded to show trends; L = Low, below the median; H = High, above the median.
Larger LLTCOPs in Georgia (Table 2) and New York (Table 3) are generally more likely to report being very effective in meeting most mandates. However, smaller New York LLTCOPs report higher effectiveness in community education than larger programs, which may reflect the difficulty of providing community education in urban environments.
LLTCOPs in Georgia with fewer volunteers also report higher effectiveness in monitoring federal, state, local laws and regulations, and systems advocacy. This result suggests that volunteers in Georgia LLTCOPs are not a significant contributing factor in effectively meeting these mandates. However, LLTCOPs in California with more volunteers are more likely to report being effective in these same systems-level mandates (Table 4), suggesting that volunteers are likely a very different resource in California and Georgia. In contrast to LLTCOPs in Georgia and New York, smaller California programs are generally more likely to report being very effective in most mandates than larger programs.
The exception to this is the association between larger California LLTCOPs and higher effectiveness in meeting their systems advocacy mandate. In fact, larger programs in all three states are more likely to rate their programs as very effective in systems advocacy, with the exception of Georgia who reports higher effectiveness with fewer volunteers.
The association found between alternate measures of resources and effectiveness suggests the significance of program size (as measured by more FTEs, volunteers, beds, facilities, and higher budget), particularly to effectiveness in systems advocacy. The tendency for larger programs to be more effective suggests that there may be a critical threshold of program size, under which effectiveness, particularly in systems advocacy activities, is (or will be) lower.
Changing LTC Environment
The LTC environment has changed significantly since the inception of the LTCOP in 1972. As seen in the number of board and care beds and facilities served by LLTCOPs in California and Georgia, LTC is becoming less institutionalized. In all three states, LLTCOPs are more likely to report being effective in serving residents in nursing homes than in board and care facilities. Nursing home settings are more highly regulated than when the LTCOP was created, while less institutionalized board and care type facilities remain less (and variously) regulated. The presence of regulations to cite and guide their investigations is important for LLTCOPs to be able to effectively advocate for residents (Nelson, Netting, Huber, & Borders, 2001).
Additional State Mandates
The problem of additional responsibilities and state mandates is that many are imposed without any additional funding. California LLTCOPs are designated as both investigators and mandatory reporters of elder abuse. Some California LLTCOPs contend these conflicts with their federal mandate to act on behalf and with consent of the resident. LLTCOPs in California cite mandatory abuse reporting and investigation, the witnessing of advanced directives, and monitoring residential care facilities for persons with mental illness, mental retardation or developmental disabilities as state mandates that add to the workload of their program. Many California LLTCOPs report that funding allocated to these additional mandates, if available at all, is insufficient. In Georgia, LLTCOPs are also required to serve additional facilities housing residents with mental retardation and mental illness. 3
We cannot meet personal care home and community living arrangement mandates because of the number of facilities in our county area. With intermediate care facilities for people with mental retardation and community living arrangements, the population is much less able to communicate with us and there is less involvement of family. (GA)
Such additional state mandated responsibilities influence the adequacy of program resources, the training needed for staff and volunteers, and the agencies with which the LLTCOPs coordinate
Discussion
The inconsistent relationships found between beds/FTE and LLTCOP effectiveness both within and across states lead to the rejection of our first hypothesis that LLTCOPs with heavier workloads (more beds/FTE) will report lower effectiveness in meeting all mandates. The findings related to other measures of resources and their association to the reported effectiveness also leads to the rejection of our second hypothesis. However, this study uncovered the factor of a critical threshold for program size that needs to be further conceptualized and investigated. Lastly, the finding that LLTCOPs report strained resources as a result of changing LTC environments and additional unfunded state mandates supports the third hypothesis that mediating factors influence the adequacy of LLTCOP resources. Although the findings did not confirm all study hypotheses, they do show that the IOM measure of beds/FTE is not sufficient to reflect the complexity of LTCOP resource adequacy or to fully account for the necessity (or lack thereof) for increased program resources. The addition of unfunded state mandates requires a serious discussion of organizational boundaries and potential mission creep.
Critical Threshold of Program Size
Although neither the beds/FTE workload measure nor individual alternate measures of program size are consistently predictive of LLTCOP effectiveness across states, there is a tendency for larger programs in Georgia and New York to report higher effectiveness. In addition, the association between larger programs and higher effectiveness in systems advocacy in all three states suggests that there is a critical threshold of program size especially for systems-level mandates. Organizational sociologists have studied the role that size plays in organizations, Organizations that are large have more power and leverage over their environments. They are more able to resist immediate pressures for change and, moreover, have more time in which to recognize external threats and adapt to meet them. Growth enhances the organization’s survival value, then, by providing a cushion or slack against organizational failure.
Thus, it may be argued that larger LLTCOPs are afforded nonmonetary resource “slack” through the division of labor, and diversity of informational, experiential, and strategic human capital of more staff and volunteers. These assets of larger programs may enable them to more effectively meet their systems-level mandates, such as monitoring federal, state, and local laws and regulations, and systems advocacy. Another plausible explanation is that smaller programs’ efforts are directed toward essential administrative tasks (i.e., paperwork, reporting, paying bills, answering the phone).
Organizational Boundaries and Mission Creep
Especially in challenging economic environments, organizational boundaries are likely to become weaker with pressure to secure additional funding, resulting in an expansion of the organization’s mission. Many LLTCOPs have been required to expand their mission to include investigating elder abuse, witnessing advanced directives, and serving additional populations and facility types. According to this study, such role expansion often does not come with additional resources. In additional, reliance on variable and uncertain funding is likely to generate instability in the organization as well as among its staff and volunteers.
Research Limitations
Limitations of this research result from with the data and methods used. Given the small data set, the 100% participation of Georgia and California LLTCOP coordinators, and the defensible representativeness of the 78% of New York LLTCOP coordinators and data; the analyses were limited to simple associations between dichotomous variables, median characteristics, and the proportion of specific responses. Although the data collected from the universe of LLTCOPs in the states studied did not require statistical tests of correlations or regressions, this minimizes the researcher’s ability to control for variables to eliminate collinearity and confounded associations.
The 3-year gap between the California and New York data-collection period and the Georgia data-collection period may also limit the validity of study findings, although the researchers found no empirical evidence of variability as a result of different periods of data collection. No federal or state laws, regulations, and/or funding changed dramatically during this period that would render the comparative analysis of these data across this time period inappropriate.
Finally, with a total of 89 LLTCOPs reporting from three states, the findings are not generalizable to the national universe of all LLTCOPs. Additional analyses of LLTCOPs are needed to extend the findings and the generalizability of the results to other states and LLTCOPs.
Implications for Future Research
The replication of this research in additional states is needed to identify and test more complete and accurate measures of resources. Larger data sets and the participation of additional LLTCOPs in other states will provide the statistical power needed to allow for the application of more technical analytical methods. To address reliable and valid measures of resources, it is recommended that future research focus on the development of measures that reflect actual workloads of LLTCOPs and variations in additional mandates within and across states. Measures of program resources need to be tested for their predictive power in relation to program effectiveness, program viability, and the continued health, safety, welfare, and rights of LTC residents.
Policy Implications
Although this research provides a critique of the resource measure and standards developed in the 1995 IOM study, this standard has been instrumental in allowing local and state LTCOPs, scholars, and others to advocate for adequate funding. The aim of this research is not to discredit the IOM measure or the advances stemming from it, but to examine the empirical case for a more nuanced measure of resource adequacy. This effort is particularly timely given the nascent state of data collection and the development of indicators of quality of care on the new Long-Term Services and Supports Scorecard (Reinhard, Kassner, Houser, & Mollica, 2011). As advocates for residents of LTC facilities, it is essential that the LTCOP is included in this current effort to improve the measurement and analysis of quality of care and quality of life among older adults.
Three policy implications arise concerning the ability of LLTCOPs to effectively perform their federal mandates. The research findings are consistent with and suggestive of two recommendations contained in the 1995 IOM study. First, it is recommended that the organizational boundaries of LLTCOPs be strengthened “to the effect that, before expanding the LLTCOP into new roles with other populations, the capacity of LLTCOPs to effectively meet their existing federally mandated services for beneficiaries of the Older Americans Act needs to be ensured” (p. 22). Second, “if Congress mandates additional responsibilities for the ombudsman programs then Congress should also provide adequate additional appropriations to the ombudsman program” (p. 21).
Lastly, further research and evaluation are needed to advance the development, testing, and validation of state-specific resource adequacy measures that take into account a number of factors including within- and across-state differences, additional state and local mandates, and the existence of a critical threshold of program size. Other potentially relevant factors that must be incorporated in future research include the LTC policy and fiscal environment of the different states and communities in which these LLTCOPs operate. It is suggested that the Administration on Aging or other appropriate agencies or foundations undertake such research.
Conclusion
The effectiveness of LLTCOPs is integral to the quality of care and quality of life of residents in LTC facilities. Without LLTCOPs, regulatory agencies will likely be required to conduct more visits; legal services agencies will receive fewer referrals; law enforcement may not have the evidence they need; the LTC system will have reduced sources of quality control; and state governments will have to find other efficient ways to meet the needs of residents and the public. Leaving these programs without adequate resources, whatever those might be, strains the larger LTC system and may leave LTC residents vulnerable to abuse and neglect. Additional research and the development of more nuanced measures of the adequacy of LLTCOP resources are imperative to assess the capacity of the LTCOP to effectively advocate for the health, safety, welfare, and rights of LTC residents.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The researchers acknowledge the generous support of five foundations and key staff: The Commonwealth Fund (Dr. Mary Jane Koren and Karen Davis, President), The Archstone Foundation (Mary Ellen Courtright, Vice President), The Jacob & Valeria Langeloth Foundation (Scott Moyer, President), The New York Community Trust (Len McNally) and The California Endowment (Dianne Yamashiro-Omi). This collaborative community-based research is particularly indebted to the CA Long Term Care (LTC) Ombudsman Association, the NY State Ombudsman Association, and to the Project Advisory Committee including representatives of the National Association of Local LTC Ombudsmen (NALLTCO) and the National Association of State Ombudsman Programs (NASOP). Invaluable assistance was provided by the local ombudsman in California, Georgia, and New York as well as the State LTC Ombudsmen and their respective state units on aging; Sue Wheaton of the Administration on Aging and consultants, especially Sara Hunt and Bill Benson. The views presented here are those of the authors and should not be attributed to the granting organizations, their directors, officers, or staff.