
Abstract
This pilot study examines the associations between structural characteristics and the adoption and subsequent use of electronic health records (EHR; resident demographics, clinical notes, medication lists, problem lists, discharge summaries, and advance directives) as a process characteristic in assisted living facilities (ALFs). The study is guided conceptually by Donabedian’s Structure-Process-Outcome (SPO) model. Primary survey data were collected from a randomly selected sample (N = 76) in Florida during 2009-2010. Analysis included descriptive and bivariate statistics. Descriptive results indicated that ALFs most frequently used an EHR to record medication lists. Characteristics, including size, profit status, resident case mix, and staffing, were associated at the bivariate level with the use of one or more functional domains of an EHR. Thus, the use of EHRs in ALFs is correlated with facility characteristics.
Introduction
The 2009 federal Health Information Technology for Economic and Clinical Health (HITECH) Act allocated US$27 billion to doctors and hospitals to promote the use of electronic health records (EHR). Although EHRs have the potential to improve the quality and safety of health care, eliminate inefficiencies, reduce costs, and encourage greater patient engagement (Kramer, Richard, Epstein, Winn, & May, 2009; Shekelle, Morton, & Keeler, 2006), adopting meaningful use of this technology has proven difficult (Black et al., 2011). Currently, qualified health centers, rural clinics, hospitals, and physicians’ offices are eligible to receive Medicare and Medicaid incentives to adopt EHRs; however, long-term care providers (nursing homes, assisted living facilities [ALFs], home health, rehabilitation centers, and adult day care) are ineligible.
Despite the growing numbers of older adults who require coordination of care across multiple long-term care settings, the adoption of EHRs is not as ubiquitous within these domains as compared to acute care settings (Ferris, 2005). Prior studies examining EHR use in nursing homes (NH) suggest that those facilities that are members of a chain, as well as larger, nonprofit facilities with a greater number of services and longer tenure of the administrator, were more likely to use EHRs for clinical care and administrative domains (Chan, 2008; Davis, Brannon, & Whitman, 2009; Resnick, Manard, Stone, & Alwan, 2009). Across home health and hospice agencies, nonprofit or government providers, providers that were members of a chain, and those with a larger patient census were more likely to use EHRs (Bercovitz, Sengupta, & Jamison, 2010).
One growing long-term care setting that has not been studied in regards to EHR utilization is ALFs. Approximately 1 million older adults reside in 31,100 ALFs nationwide (Park-Lee et al., 2011) and that number is expected to reach 1.9 million by 2030 (Mollica, Sims-Kastelein, & O’Keefe, 2008). Since the past decade, ALFs have evolved into a viable alternative to NH placement (Ball et al., 2000; Chapin & Dobbs-Kepper, 2001; Spillman & McGillard, 2002) as most ALF residents tend to be frail older adults with multiple comorbidities and deteriorating physical health (Kane & Mach, 2007; Street, Burge, & Quadagno, 2009). Although ALF residents are similar to NH residents with respect to depressive symptoms, physical impairments, behavioral problems, and changes in morbidity (Sloane et al., 2004), ALFs are not health care facilities, which leaves residents vulnerable to hospitalizations (Becker, Boaz, Andel, & DeMuth, 2011) and medications mismanagement (Briesacher, Limcangco, Simoni-Wastila, Doshi, & Gurwitz, 2005; Sloane et al., 2004). Consequently, EHR integration into ALFs may improve residents’ health outcomes and reduce unnecessary health care expenditures.
Conceptual Framework
The Structure-Process-Outcome (SPO) model (Donabedian, 1996) has been widely used to conceptualize and study quality of care in long-term care. According to this model, quality is composed of three related domains: structure (characteristics of the physical/organizational setting), process (the technical processes of care), and resident outcomes (Donabedian, Wheeler, & Wyszewianski, 1982). Donabedian’s model provides a framework to examine how structure and process of care have the potential to cause injury or harm to residents.
Purpose
Using the SPO theoretical model, this pilot study examines the associations between structural characteristics and the use of EHRs in ALFs. To our knowledge, this is the first study to provide insight into the use of EHRs in ALFs.
Method
Sample
The sample (n = 741) was selected from the 2,768 Florida licensed ALFs and 490 adult family care homes (AFCH) in 2009. AFCHs were also included because they represent residential care settings in Florida that provide very similar long-term care services as ALFs and are only differentiated in licensure by their bed capacity. Florida is an ideal site for examining ALFs since it has a diverse industry and accounts for 33% of facilities nationwide (Mollica, Johnson-LaMarche, & O’Keefe, 2005). The sample was stratified based on three facility-size categories (high: >15 beds, medium: 7-15 beds, and low: <7 beds), which have been used in previous studies in Florida and nationally (Hawes, Rose, & Phillips, 1999; Salmon, Hyer, Hedgecock, Zayac, & Engh, 2004)
Between May 2009 and April 2010 surveys were mailed, along with an informational study letter about how to complete the survey (paid postage return envelope, Qualtrics online survey, or telephone interview). Several strategies were used to increase the response rate. Within 2 weeks of the initial mailing a follow-up phone call was made to the AL administrators and subsequently the survey was resent, or a time to conduct a phone interview was scheduled. Two additional strategies included support letters and emails sent from a number of the AL corporate headquarters to their participating facilities in the study and announcements about the study in the statewide AL organization’s monthly newsletter. Despite these recruitment efforts, a total of 76 ALFs completed the survey (10.6% response rate). The University of South Florida Institutional Review Board approved this pilot study.
Findings from chi-square and t-test statistical tests for differences between respondents and nonrespondents found no significant differences with respect to facility size, licensure type, and profit status. Sample strata only differed significantly between respondents and nonrespondents for the low category with fewer small facilities responding to the survey.
Measures
ALF administrators were surveyed about whether they provided a computerized system for seven different EHR domains. The survey asked, “Does your ALF have a computerized system for (1) resident demographics, (2) physician notes, (3) nursing assessments, (4) problem lists, (5) medication lists, (6) discharge summaries, and (7) advance directives. These seven EHR domains were identified from published surveys (Centers for Disease Control and Prevention/National Center for Health Statistics, 2009; Jha et al., 2009). Because of the limited medical care provided by ALFs, physician notes and nursing assessments were combined into a clinical notes category yielding six final EHR domains.
The survey included structural characteristics of the facility based on the SPO model (Donabedian, 1996). Facility size was defined according to the total number of beds. Proprietary status was defined as for-profit, publicly traded company. ALF licensure type was categorized according to Florida statutes as extended congregate care (ECC), limited mental health (LMH), and limited nursing service (LNS). Staffing measures included the number of full-time equivalent (FTE) registered nurses (RN), licensed practical nurses (LPN), and personal care aides (PCA).
Resident case mix and payer source (percent private pay or Medicaid) were included as factors associated with process characteristics, similar to other analyses guided by the SPO model (Castle, 2000; Luo, Fang, Liao, Elliott, & Zhang, 2010; Williams et al., 2005). Resident case mix was described by the percentage of females, Caucasians, those with a diagnosis of dementia or Alzheimer’s disease, those requiring assistance with 3 or more activities of daily living (ADL), and primary payment source as either Medicaid or private funding.
Statistical Analysis
Descriptive statistics were used to examine the frequency of EHR use in ALFs. To study the relationship between structural, resident case mix, and payer source characteristics of ALFs and EHR use, point-biserial (r pb ) correlations were used. Descriptive and bivariate analyses were appropriate for this evaluation considering the small sample and the novelty of this research. There were no missing data for the variables of interest. All analyses were performed using IBM SPSS version 19.
Results
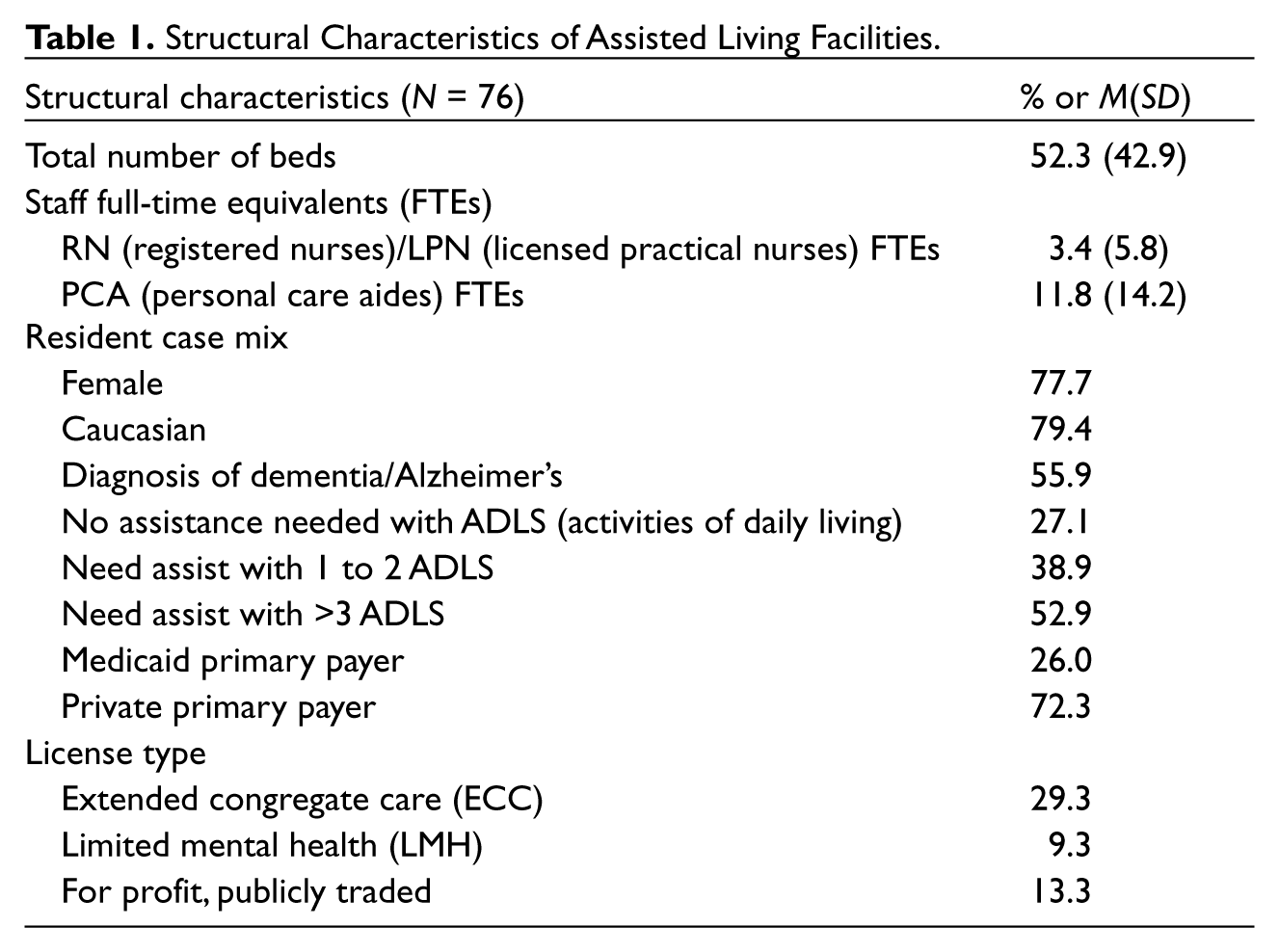
Descriptive statistics for the final sample are presented in Table 1. On average, the facilities had 52 beds and staffed slightly more than 3 nursing FTE (RN/LPN) and 11 PCA FTEs, respectively. Approximately 13% were for profit. Twenty-nine percent had a license for extended congregate care and only 9% were licensed as limited mental health. The majority of residents were female (77%), Caucasian (79%), and private pay (72%). About half of residents had dementia and significant ADL limitations.
Structural Characteristics of Assisted Living Facilities.
Approximately 53.9% of ALFs surveyed reported using at least one or more of the EHR domains. A comparison between those using EHRs (n = 41) and those not using the technology (n = 35) suggested that users differ significantly from nonusers based on profit status, as users were more likely to be for-profit, publicly traded facilities (χ2 = 6.22, p = .013).
Among these facilities using EHRs (n = 41), there was considerable variation in the reported use of each EHR component (Figure 1). Of those facilities with EHR capabilities, the most commonly reported functions were the ability to record medication lists (87.8%) and the documentation of resident demographics (73.2%), whereas EHR use for discharge summaries (39%) and advance directives (34.1%) was less common.
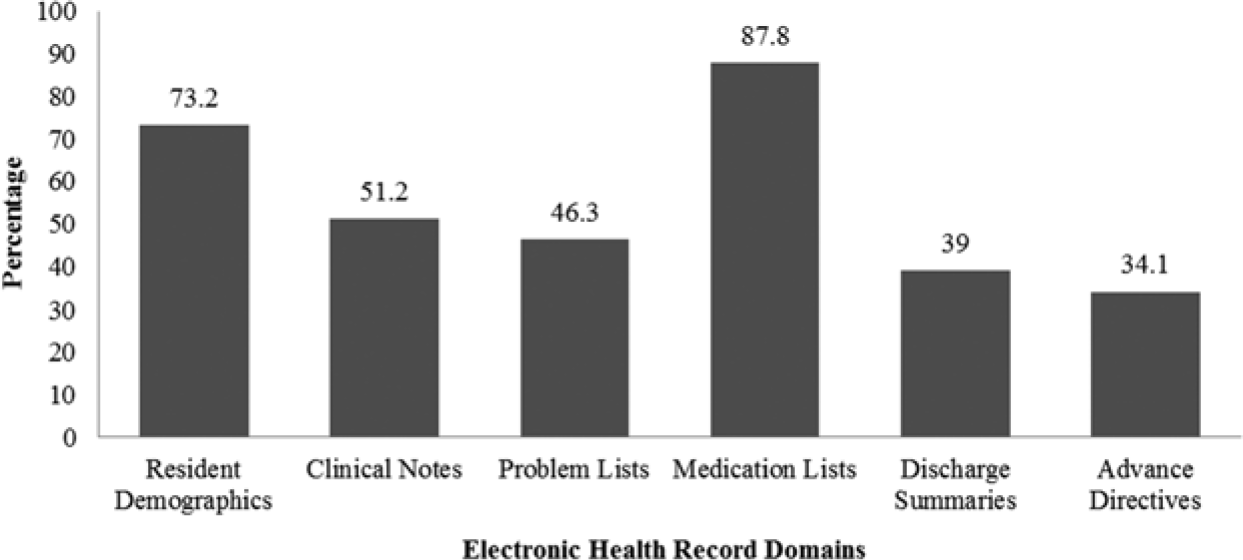
The use of specific electronic health record (EHR) domains in assisted living facilities currently using EHRs (n = 41).aThese percentages include those facilities that used at least one of the six EHR domains.
Correlation analysis indicated that several ALF characteristics, including size, profit status, resident case mix factors, and staffing, were significantly associated with the subsequent use of EHR to record resident demographics, clinical notes, medication lists, and resident problems (Table 2). Using an EHR to document resident demographics was correlated with larger, for-profit facilities that employed a higher number of PCAs, RNs, and/or LPNs. These facilities also had a higher percentage of Caucasian and female residents as well as residents with a diagnosis of dementia. EHRs used to record clinical notes were positively correlated with larger, for-profit facilities that had a higher percentage of female and Caucasian residents. Status as a for-profit, publicly traded facility was correlated with the use of EHRs to document resident problems and medication. No facility characteristics were correlated with the use of EHRs for discharge summaries or advance directives.
Correlations Between the Characteristics of Assisted Living Facilities and Specific Domains of Electronic Health Record Use.
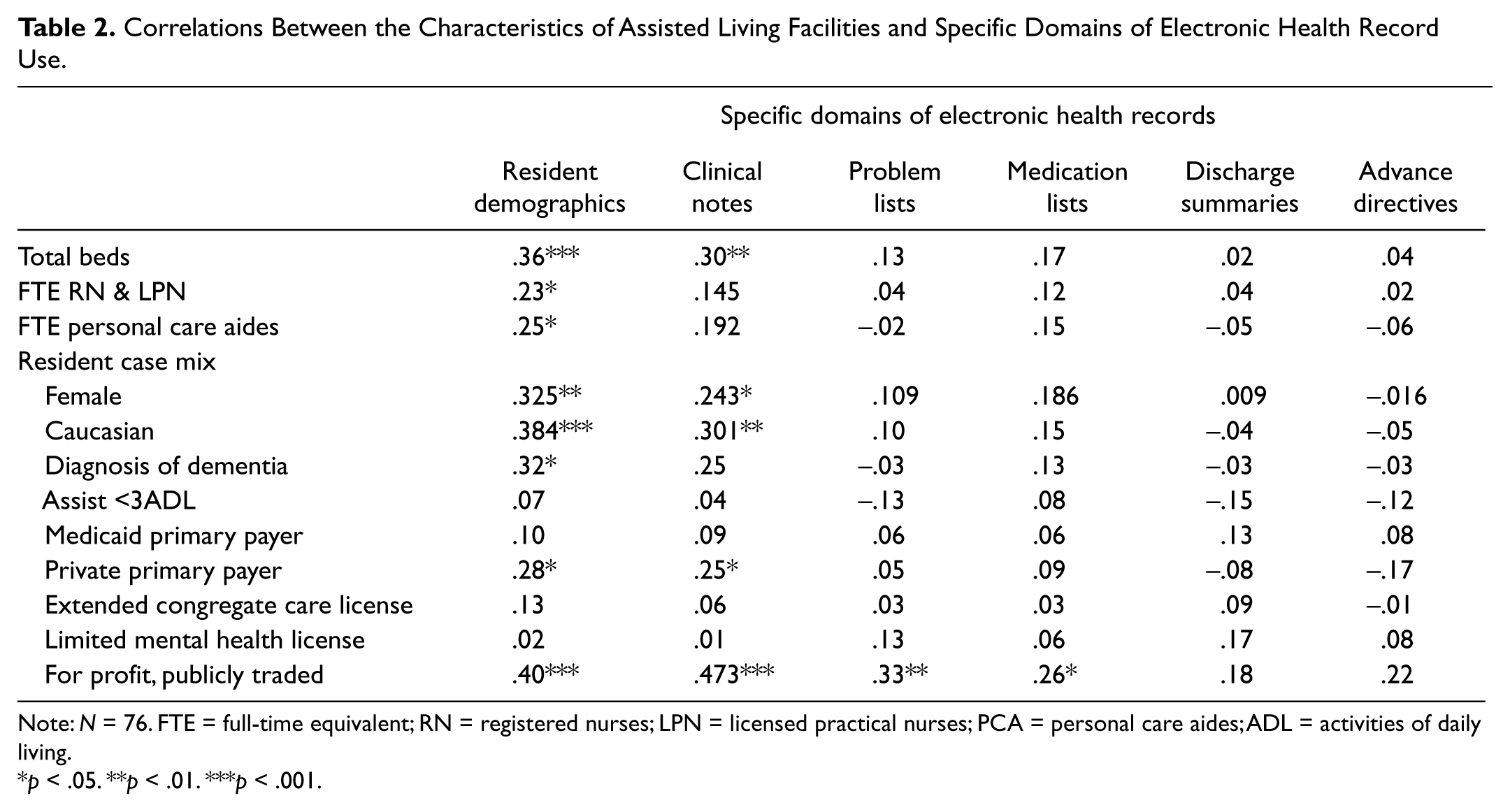
Note: N = 76. FTE = full-time equivalent; RN = registered nurses; LPN = licensed practical nurses; PCA = personal care aides; ADL = activities of daily living.
p < .05. **p < .01. ***p < .001.
Discussion
The findings of this pilot study provide initial evidence that ALFs are currently utilizing EHRs and serve as a preliminary step toward analyzing EHR use in ALFs. Based on these findings, the most commonly reported functions of EHRs are the ability to record medication lists and resident demographics. Although, considerable variability exists in the proportion of ALFs using EHR components, our prevalence findings are consistent with research examining these trends in home health and hospice agencies (Resnick & Alwan, 2010).
Although the finding that status as a for-profit, publicly traded facility is correlated with EHR use for several domains did not follow the direction suggested by existing research in NHs (Davis et al., 2009), several studies have suggested that for-profit NHs value efficiency more than nonprofits (Anderson, Weeks, Hobbs, & Webb, 2003; Knox, Blankmeyer, & Stutzman, 2001). Considering the costly initial investment for establishing and maintaining this technology, for-profit communities may also have the financial infrastructure and capital available to adopt an EHR earlier than other facilities. In addition, since ALFs opt to implement specific components with others being used less often, EHR may be implemented in stages with the use of this technology best modeled by a continuum of applicability instead of the current dichotomy.
Several important limitations of this pilot study should be considered. First, this is a pilot study in one state with a small sample and, despite the aggressive recruiting efforts, a low response rate; therefore, our findings are not generalizable beyond the sample that is represented. The small sample used in this study may also explain the small to moderate correlations between ALF structural characteristics and the domains of EHR use. Another key limitation rests in the fact that this study only examined the use of EHR components in ALFs and not the duration of use or the availability of the technology. This is an important distinction considering that the low proportion of EHR use in ALFs may be due to limited availability, stepped implementation, or a slowed acceptance of the technology. Last, this study presents only descriptive and bivariate analyses. Therefore, although the data support our conclusions, studies using predictive models with a larger sample to increase power are required to confirm these findings and provide further insight into EHR use in ALFs.
In discussions about electronic health information systems, our study provides benchmark findings regarding the use of EHRs in ALFs. However, studies that examine the availability and barriers to adopting EHRs across these settings will be necessary to advise the development of policies and improve the quality of care delivered across the healthcare system.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.